
Access to all articles, new health classes, discounts in our store, and more!
To the Editor: What Is Normalization of Blood Glucose? Also, Reply by V. K. Piziak, MD, PhD
Letter to the Editor, published in Southern Medical Journal, Vol. 89, No. 2, February 1996.
* * *
What Is “Normalization” of Blood Glucose?
To the Editor: A recent editorial in the Southern Medical Journal raised the question, “Does normalization of blood glucose reduce the risk of complications of diabetes?”1 The conclusions were based on the recently published results of the Diabetes Control and Complications Trial (DCCT).2 Two groups of patients had long-term followup while one group was treated conventionally and the other intensively. Normalization of blood glucose was not attained in either group. However, it was only 40% above the suggested “normal” in the intensive treatment group. Nonetheless, over the study period, which averaged 7 years, there was at least a 60% reduction in risk between the intensive and standard treatment group in diabetic retinopathy, nephropathy, and neuropathy.
The unanswered question is, “Can the complications be even more dramatically reduced if we can really answer the question, how normal is normal blood glucose?” There are, according to Murphy, seven definitions of “normal.”3 Most represent average or statistical, and sometimes suggest physiologic or healthy. But the least studied definition is the “ideal.”
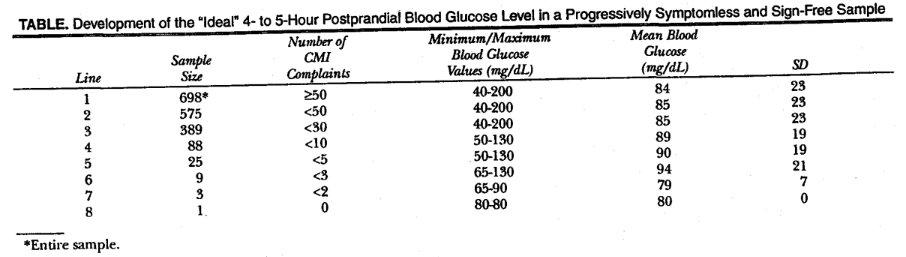
To derive blood glucose ideality, progressively symptomless and sign-free individuals were used. The time-tested self-administered Cornell Medical Index Health Questionnaire (CMI) was used. The Table summarizes the findings for the blood glucose levels of 698 presumably healthy subjects who consumed food or drink approximately 4 to 5 hours before having blood drawn.4 The mean blood glucose value was 84 mg/dL, with a standard deviation of 23. What is most noteworthy is the blood glucose range. It extends from a nadir of 40 to a zenith of 200 mg/dL. (The nonlethal range of blood glucose is 20 to 1,500 mg/dL.5) As one moves downward in the Table, the sample size understandably shrinks in a logical order as health requirements are stiffened. What is exciting is that with perfect regularity the lowest and the highest values are progressively eliminated. The point to be emphasized is that, with increasing health, there is systematically greater glucose homogeneity and the “ideal” nonfasting blood glucose value appears to be 80 mg/dL (hemoglobin A1c value, 4.4 mmol/L) (Figure). Obviously, there is always a problem with sample size, since no one is perfectly healthy. Also, there is always the experimental error in performing the test.
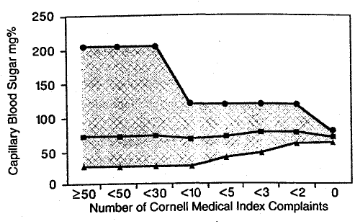
Blood glucose mean a nd range 4 to 5 hours postprandially in subgroups of patients reporting progressively fewer symptoms and signs, using Cornell Medical Index Health Questionnaire.
Is it possible to approach such ideality without running the risk of hypoglycemia and/or an increase in body weight if one were to add supplements such as chromium, vitamin C, and nicotinamide? The final question is with even greater normalization of blood glucose, can we reach even greater decreases in diabetic complications?
References Cited:
- Vajdos MA, Gilliland PF: “Does normalization of blood glucose reduce the complications of diabetes?” South Med J 1995; 88:372-375.
- American Diabetes Association: “Implications of the Diabetes Control and Complications Trial.” Diabetes 1993; 42:1555-1558.
- Murphy EA: “The normal and the perils of the sylleptic argument.” Perspect Biol Med 1972; 15:566-582.
- Cheraskin E: “The ‘ideal’ blood sugar: its bigger meaning.” J Appl Nutr 1994; 46:45-59.
- Guyton AC: Textbook of Medical Physiology. Philadelphia, WB Saunders Co, 1991.
Reply from V. K. Piziak, M.D., Ph.D.
To the Editor: The point that Dr. Cheraskin makes is an interesting one. Lowering blood glucose to within a percentage point of a normal hemoglobin A1c dramatically reduces the complications of insulin-dependent diabetes. The question of whether it is possible to achieve a greater decrease in diabetic complications or perhaps their total prevention by normalization of glucose will finally be answered when greater strides are made in pancreatic transplantation and islet cell implantation research. With exogenous insulin, the degree of hypoglycemia occurring in patients with diabetes who achieve near normal levels of glucose makes the goal of absolutely normal blood glucose levels unachievable for the vast majority of insulin-dependent diabetic patients.
It is also interesting to speculate on whether lowering the average blood glucose value in the population without diabetes will help promote better health and a greater sense of well-being. If we lower blood glucose in the general population, can we prevent the complications of aging, for example? We know that hemoglobin A1c is a glycosylation product formed by a nonenzymatic reaction when glucose binds to a fraction of hemoglobin. There are many glycosylation products formed spontaneously on tissue proteins. These advanced glycosylation products have been implicated in the pathogenesis of aging and may also be involved in atherogenesis and renal disease.1 Patients with higher glucose levels develop these products more rapidly. In addition, there are studies suggesting that rates of accumulation of glycosylation products may be accelerated in populations of diabetic subjects at high risk for complications.2 Thus, these glycosylation products, which now can be assayed, may be markers for patients in whom we should emphasize more stringent control of diabetes to prevent these complications. Might they also be markers in patients without diabetes for accelerated aging? Recently, glycosylation inhibitors such as aminoguanidine have been used to decrease advanced glycosylation products with the hope of decreasing some of the complications of diabetes and perhaps some of the age-related complications of glycosylation as well.3
As yet, however, there is no compelling scientific evidence to suggest that lowering blood glucose levels in the normal population will prolong life or promote a greater sense of well-being. The article by Murphy,4 cited by Dr. Cheraskin, looks at the number of complaints patients have, which does not necessarily correlate with either disease or outcome. There is, however, considerable evidence that a regular exercise program and the achievement of a normal body weight on a diet low in fat will diminish the probability of developing diabetes and atherosclerotic cardiovascular disease.5 Therefore at present we should aggressively advise our patients on a prudent diet. We hope that further research will allow us to inhibit glycosylation and thereby diminish the complications of diabetes and aging.
References Cited:
- Sensi M, Pricci F, Andreani D, et al: “Advanced non enzymatic glycation end products (AGE): their relevance to aging and the pathogenesis of late diabetic complications.” Diabetes Res 1991; 16:1-9.
- Wu JT: “Advanced glycosylation end products: a new disease marker for diabetes and aging.” J Clin Lab Anal 1993; 7:252-255.
- Makita Z, Vlassara H, Rayfield E, et al: “Hemoglobin-AGE: a circulating marker of advanced glycosylation.” Science 1992; 258:651-653.
- Murphy EA: “The normal and the perils of the sylleptic argument.” Perspect Biol Med 1972; 15:566-582.
- DeFronzo RA, Ferrannini E: “Insurance resistance. a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease.” Diabetes Care 1991; 14:173.