
Access to all articles, new health classes, discounts in our store, and more!
The Role of the Dental Hygienist in a Research Program
Presented at the Annual Meeting of the American Dental Hygienists’ Association, October 30, 1967, Washington, D.C. Published in Hygienists’ Association, Second Quarter 1968.
* * *
Introduction
“You would be surprised at the number of years it took me to see clearly what some of the problems were which had to be solved…Looking back, I think it was more difficult to see what the problems were than to solve them.” – Charles Darwin
The charge here is to elucidate the nature of oral disease. The hope is that such an appraisal will clarify the form and direction which stomatologic research must take and the niche of the dental hygienist in the coming years.
The Clinical Problem
The clinical problem is that chronic disorders in general, and dental caries and periodontal pathosis as the number one chronic diseases in particular, begin early in life. With advancing age, progressively more people develop progressively more dental caries and periodontal disease. Figure 1 pictorially portrays the sequence of events. One parameter (gingival inflammation) of periodontal pathosis is described on the ordinate. Time is expressed as age on the abscissa. The widening band suggests that variability also increases with advancing age. Hence, some individuals show more and others less gingival involvement at any given age. The fact that some persons display no gingival pathosis in the later years is reasonable evidence that the process, while common, is not necessarily a physiologic one.
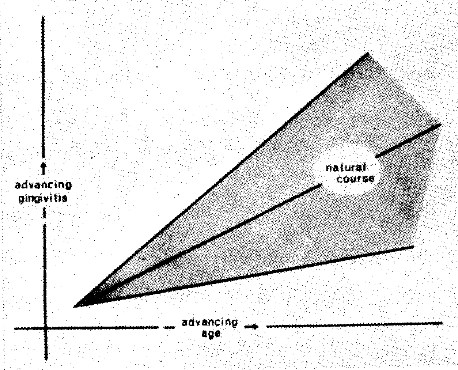
Figure 1. The common sequence of events is that, with time [advancing age], progressively more people show progressively more gingival inflammation. Also shown by the diverging gray zone is that there is greater variability in the later years.
To translate the validity of this observation for purposes of this report, one hundred 27 to 55 year-old policemen and firemen underwent oral examination. This group was chosen because it is fairly representative of the middle-class blue-collar worker who regularly visits a private dental office. Additionally, the group was selected because of its relatively good health status. A person who is obviously ill cannot meet the rigorous standards for employment in such hazardous professions. Lastly, these individuals were utilized because they presented themselves only for simple scaling and polishing of the teeth.
The gingiva of each anterior tooth was graded with a four-point scale to provide a gingivitis score. From these values, mean scores were derived for each of the 100 subjects. For purposes of subgroup analysis, the 100 subjects were divided into three near-equal subgroups. Figure 2 plots the mean gingival scores (on the y-axis) in terms of the youngest, intermediate, and oldest age groups shown on the x-axis. Two points deserve special mention. First, with advancing age gingival pathosis increases. Secondly, the findings in this group are quite in keeping with the general body of clinical fact. This is underlined by noting that the actual scores for this group neatly fall within the gray area.
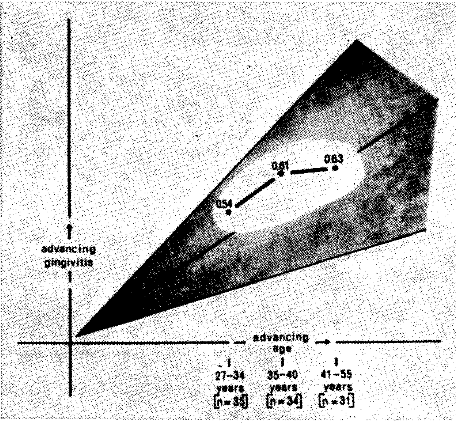
Figure 2. The increasing mean gingival scores with age in 100 policemen and firemen underscores the general observation of increasing pathosis with time.
The Etiologic Problem
Present therapeutic armamentaria are designed either to slow the disease process, stop it completely, reverse the problem, or if at all possible, to prevent it. The various possibilities just mentioned are graphically summarized in Figure 3.
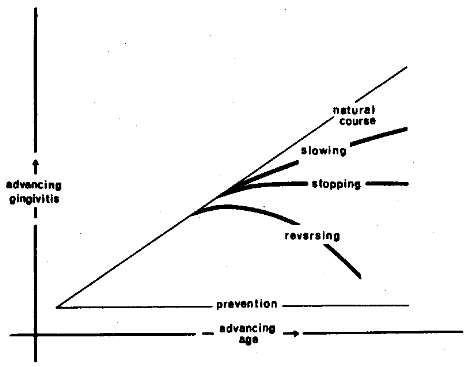
Figure 3. The present therapeutic armamentaria are designed to change the natural course of events. The evidence suggests that the major effects result in either slowing, arresting, or possibly reversing the pathologic process. The ultimate goal is to subtend an angle of zero through prevention.
There is enough convincing evidence to indicate that the frequency of toothbrushing is one effective therapeutic measure. In order to relate it to the report at hand, the one hundred policemen and firemen were subdivided into two groups based upon their toothbrushing habits. For simplicity, one subgroup included those brushing once or twice daily; the other group incorporated the individuals brushing three or more times per day. Figure 4 summarizes the effects upon gingival inflammation by virtue of different toothbrushing habits. It will be observed that the subjects brushing three or more times per day have, with increasing age, essentially no change in gingival inflammation. Thus, in terms of the earlier discussion (Figure 3), it is fair to say that toothbrushing under these conditions is helping to arrest the gingival problem. Additional confirmation can be derived by observing the increase in gingival pathosis in the subjects who brush their teeth only once or twice per day. It would seem, within the limits of this study and consistent with clinical experience, that the frequency of toothbrushing is indeed an effective therapeutic device. However, it should be pointed out that it does not accomplish the goal of reversing or preventing the problem.
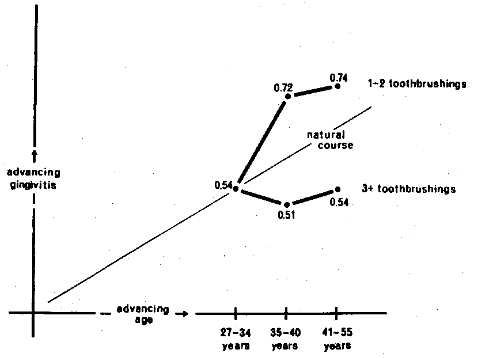
Figure 4. The common course of gingival pathosis can be altered by the frequency of toothbrushing. The subjects brushing three or more times per day show distinctly less gingival pathosis with time than the subjects with less toothbrushing.
There is abundant evidence that disease causality is a multifactorial problem.1-55 Leading authorities in the field of stomatology agree with this concept. For example, Dr. Henry Goldman,6 addressing the subject of the etiology of periodontal pathosis, supports the ecologic thesis.
It seems probable at this time that periodontal lesions are not the result of a direct cause-and-effect relationship to a single causative agent, as often cited, but are the result of many variable and interrelated influences.
Utilizing a more selective term, Dr. Irving Glickman has also underscored the interplay of host and environment.7
The ‘bone factor’ concept differs from the traditional division of periodontal disease into ‘local’ and ‘systemic’ types. It envisages a systemic component in all cases of periodontal disease.
On the basis of such statements, an attempt has been made to reexamine the policemen and firemen in terms of local and systemic factors. For example, the importance of vitamin C in oral and general health is well known.8-10 Accordingly, the subjects were graded in terms of vitamin C status. According to the Interdepartmental Committee on Nutrition for National Defense [ICNND],11 a plasma ascorbic acid level of less than 0.2 mg. per cent is regarded as unsatisfactory. Numerous studies of dental populations have demonstrated that approximately one third of the routine dental patients possess such plasma ascorbic acid levels.12 In the group of 100 policemen and firemen, 38 showed plasma ascorbic acid levels of 0.2 mg. per cent or less.
The 38 individuals were randomly divided so that 19 received scaling and polishing on the right side of the mouth and the other half on the left side. Additionally, one half of the sample was randomly administered a routine multivitamin-trace mineral supplement for one month; the remaining subjects were given an indistinguishable placebo. The gingiva was graded initially and one month later. Hence, it was possible at the end of the experimental period to examine the relative merits of: (1) no therapy (placebo and no scaling), (2) scaling with placebo supplementation, (3) vitamin supplementation with no scaling, and (4) scaling plus vitamin support. Figure 5 summarizes the results. Age is expressed on the abscissa and gingival pathosis on the ordinate. The natural course of increasing gingival inflammation is once again shown. It will be noted that, in the group receiving no therapy, namely placebo plus no scaling, there was an increase of 13 per cent in the gingival score. This may be likened to the natural course of gingival pathosis. Those individuals subjected to the vitamin therapy and no scaling showed no change. To relate back to Figure 3, the problem has been arrested with only vitamin support. It will be observed in Figure 5 that the group receiving scaling without vitamin therapy, the usual sequence of events in the dental office, improved 29 per cent. Relating this to Figure 3, there is a reversal of the process. Special attention should be called to the fact that there was an even greater improvement (39 per cent) when vitamin supplementation was added to the scaling. Thus, in this instance, there is even greater reversal by both local and systemic therapy.
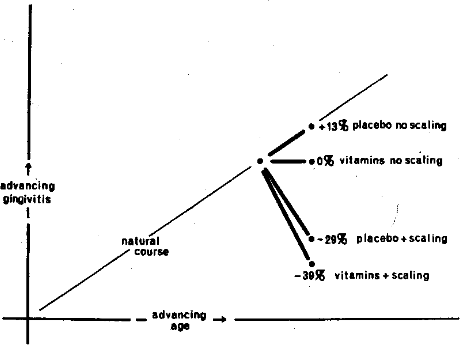
Figure 5. The relative effects upon gingival pathosis of local and systemic therapy singly and in combination. The evidence suggests the greatest improvement with combined treatment.
The Ecologic Problem
Many great thinkers have written extensively on the subject of the interplay of host state and environment in the genesis of disease.1-5 None has described the problem more eloquently than Dr. Jacques May when he said:13
It is as though I had on a table three dolls, one of glass, another of celluloid, and a third of steel, and I chose to hit the three dolls with a hammer, using equal strength. The first doll would break, the second would scar, and the third would emit a pleasant musical sound.
The published record shows that prime concern in stomatology has been directed to the effect of environmental influences, the hammer in Dr. May’s citation. It also reveals that this approach has been incomplete. The limited experimental data presented in this report is consistent with Dr. May’s fabric of the doll. These data suggest that viewing oral disease in an ecosystem (host and environment) is a more realistic model and should yield better results.
Summary
- In order to establish the rightful role of the dental hygienist in stomatologic research, it is first necessary to identify the research problem.
- The evidence suggests that, by and large, dental caries and periodontal pathosis are presently viewed as largely, if not exclusively, the result of environmental factors.
- There is valid reason to believe that a more accurate formula pictures oral health and disease as the end result of the interplay of host and environmental influences.
- Granting that an ecologic model offers a more tenable hypothesis, this provides an excellent niche for the dental hygienist in the area of stomatologic research.
References Cited:
- Dubos, R., Mirage of Health, p. 86, Harper and Brothers, New York, 1959.
- Rogers, E. S., Human Ecology and Health, p. 174, The Macmillan Company, New York, 1960.
- Bronte-Stewart, B. and Krut, L. H., “The interdependence of prospective and retrospective studies in research on ischaemic heart disease,” Atheroscl. Res. 2:317-331, 1962.
- Haggerty, R. J., “Host and environmental factors in infections,” Louisiana S. Med. S. 116:309-317, Sept. 1964.
- May, J. M., The Ecology of Human Disease, p. 3, MD Publications, Inc., New York, 1958.
- Goldman, H. M., Schluger, S., Fox, L., and Cohen, D. W., Periodontal Therapy, 3rd ed; p. 231, The C. V. Mosby Company, St. Louis, 1964.
- Glickman, L. Clinical Periodontology, 3rd ed; p. 387, W. B. Saunders Company, Philadelphia, 1964.
- Bicknell, F. and Prescott, F., The Vitamins in Medicine, 3rd ed. pp. 390-516, Grune and Stratton, New York, 1955.
- Wagner, A. F. and Folkers, L., “Vitamins and Co-Enzymes,” pp. 308-329, Interscience Publishers, New York, 1964.
- Sebrell, W. H. and Harris, R. S., The Vitamins: Chemistry, Physiology, Pathology, I. pp. 172-393, Academic Press, New York, 1954.
- Interdepartmental Committee on Nutrition for National Defense, Manual for nutrition surveys, United States Government Printing Office, Washington, D.C., 1957.
- Cheraskin, E. and Ringsdorf, W. M., Jr., “Vitamin C state in a dental school patient population,” South Calif. S. Dent. A. J. 32:375-387, Oct. 1964.
- May, J. M., “The ecology of human disease,” N. Y. Acad. Sc. 84: 789-794, Dec. 8, 1960.