
Access to all articles, new health classes, discounts in our store, and more!
The Name of the Game is the Name Revisited
Published in Journal of Orthomolecular Medicine, Vol. 8, No. 2, pp. 73-76, Second Quarter 1993.
* * *
Introduction
The following statement by Mr. Thomas J. Watson, Jr., Chairman of the Executive Committee of the International Business Machine Corporation (IBM), speaking at the Mayo Clinic in Rochester approximately 25 years ago, serves as an excellent prelude to and justification for this report:1
Let me start by asking a question that this great medical center brings to mind. How would you like to live in a country which, according to the figures available…has dropped from 7th in the world to 16th in the prevention of infant mortality; from 6th to 8th in female life expectancy; from 10th to 24th in male life expectancy; and which has brought itself this unenviable trend by spending more of its gross national product for medical care ($1 out of every $14) than any other country on the face of the earth? You know the country I am talking about…Our own USA–the home of the free, the home of the brave, and the home of a decrepit, inefficient, high-priced system of medical care. Just look for a moment at what some of the figures mean. They mean that in infant mortality, we have been overtaken by France, the UK, and Japan; that in male life expectancy we have been overtaken by France, Japan, West Germany and Italy…The evidence overwhelmingly indicates that we are falling down on the job, heading in the wrong direction, and becoming as a nation a massive medical disgrace…
The numbers have obviously changed since 1970. The trend is worsening and the conclusion that America is demonstrating a national medical disgrace is more true today than it was a quarter of a century ago when Dr. Watson addressed this major medical center.
The plethora of such pronouncements makes it now abundantly clear that health is the fastest growing failing business in these United States.2 While the problem is without argument, there is no paucity of debate with regard to its causes and solutions. Some experts contend that the major, if not sole, ingredient is a lack of doctors; other equally-credentialled authorities claim that it is not the number but the uneven distribution on a rural/urban basis or specialty/general practice ratio. There are some authorities who plead for more fundamental research; others for additional applied investigation; many for better communication between basic and clinical studies.
Quite probably, the so-called health delivery disaster is a multi-factorial issue and the explanations offered above and others all play a role. It is the purpose of this report to bring into focus one item which has received practically no attention. In traditional medicine today, the name of the game is the name. In other words, contemporary medicine is hung up on labels. We have examined this issue for many years and for numerous reasons.3,4 We shall once again be exploring evidence of Medical Ignorance: Myths and Magics in Modern Medicine.
How Does One Usually “Make” a Diagnosis?
From a practical standpoint, all disease is preceded by an incubation period. In the instance of acute mechanical trauma (e.g. an automobile wreck), the latency is obviously brief and inconsequential from a diagnostic and therapeutic point of view. In the case of the acute infectious disorders like the measles, the developing time is somewhat longer, approximately ten days, and more significant from a diagnostic and treatment standpoint. With the chronic disorders (e.g. myocardial infarction, diabetes mellitus, rheumatoid arthritis, periodontal disease), the incubation time extends over months and frequently years or decades. Clearly, the longer the prodromal time, the greater the opportunity to anticipate the end-problem and, hopefully, abort the process.
Initially, for example, the patient notes only feelings of fatigue (by this name or others such as exhaustion or tiredness). When one checks this symptom in our most contemporary and definitive diagnostic encyclopedia, the International Classification of Diseases, 9th Revision, 4th Edition, Clinical Modification (ICD-9-CM, p. 472)5 one finds a list of 18 classifiable items. However, this particular symptom does not fit any single disease. Hence, the complaint may either be ignored or assigned a meaningless label, or regarded as a minor emotional problem. In any case, because the clinical problem cannot be given a name, it follows that the treatment is purely symptomatic. At this stage, the story is expressed in the box on the left in Figure 1 (below).
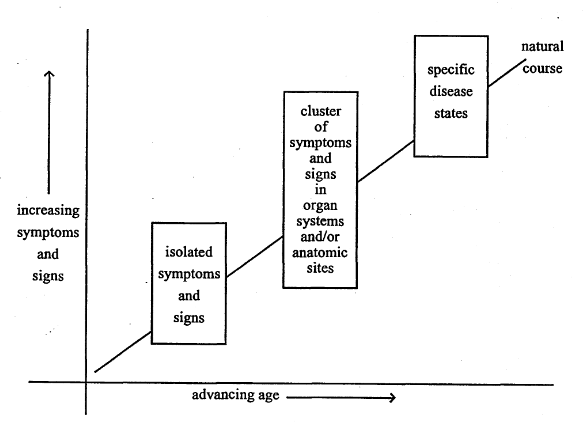
Figure 1. The clinical sequence of events in chronic disease. At first, there are few and diverse symptoms and signs (box on the left). With time, the findings become more numerous and localized in a system or site (center box). Finally, the clinical evidence fits the textbook picture of a particular disease or syndrome (box on the right).
More often than not, the situation just described continues and also other symptomatology appears. Sooner or later, the findings begin to cluster in systems, organs, or in localized sites. For example, the patient now also finds himself with several gastrointestinal complaints (i.e. indigestion, anorexia, constipation, and hemorrhoids). At this stage, the constellation is still not classifiable with textbook terminology. Hence, symptomatic treatment continues. An alternative is the recommendation for further observation. If many organ systems or anatomic sites are involved, the syndrome might, by exclusion, be assigned a psychologic/psychiatric etiology. This is the pattern pictured in the middle box of Figure 1.
Finally, when the syndrome is clearly identifiable in terms of a classical textbook description (i.e. available in the ICD-9-CM), a “diagnosis” is pronounced. This is the situation pictorially portrayed on the right in Figure 1.
In other words, in the traditional practice of medicine, disease does not really exist until a diagnosis is established. A diagnosis is only possible when a set number and constellation of findings ripen. Hence, for practical purposes, the long and tortuous incubation period clinically, biochemically, enzymatically frequently goes unlabelled or meaninglessly tagged. And so, in orthodoxy, the name of the game is the name!
The New and Now Medical Grail
Since the beginning of time, there have been efforts to pigeonhole disease. Doctor William Farr, in the latter part of the nineteenth century, initiated the first international classification of diseases. Throughout these years, there have been obvious disagreements, dissatisfactions, and debates. The present authority is expressed in a text originally published in 1979.5 This classification has the blessing of most, if not all, officiating agencies. The impressive Steering Committee consisted of the American Association of Health Data Systems, American Hospital Association, American Medical Record Association, Association for Health Records, Council on Clinical Classification, WHO Center for Classification of Disease for North America, sponsored by the National Center for Health Statistics, DHEW.
The publication of ICD-9-CM constitutes both a national and global landmark. It means that one categorization of diseases, injuries, impairments, symptoms, and causes of death will supplant the two, or even three or four present systems that have confounded and confused clinical and statistical comparisons in the United States for decades. The providers and users of the information based on this encyclopedia will also have the assurance that this volume represents the best contemporary thinking of clinicians, nosologists and statisticians. In other words, if you want to hang a label on, or actually give a number to, a medical problem so that you understand the disorder, its etiology, and solution, this international volume should provide the needed information.
Does it really do this? The implications of this name-calling game are profound and none-the-less ludicrous. Medical concern with thiamine and niacin is because of beriberi and pellagra (in their classical form, both are rare and unlikely syndromes). The value of vitamin E is still suspect in many medical circles since a deficiency of this vitamin has not been linked with a particular disease (even though the substance may be important in a host of vital metabolic processes). It is jokingly referred to as the vitamin in search of a disease.
There is nothing in the ICD-9-CM that describes the score or more functions of the ascorbates and its connection with hundreds of different clinical problems (e.g. myocardial infarction, cancer, cataracts, diabetes or even infertility).6 All that we really learn from the ICD is that there is classical scurvy and it has a number (267)!
A Case in Point
The present alleged health delivery system only recognizes a disease when a set of findings can be identified as consistent with a textbook description. By switching the emphasis from the classical disease syndrome (Figure 1, box on right) to the earliest stages of pathosis in terms of mistakes in living (Figure 1, box on left), new, productive and truly diagnostic vistas open.
We have been conducting a study of the health of health professionals for a number of years. More precisely, this includes a multiphasic testing program of doctors and their spouses. It is safe to conclude that no classical scurvy was identified in this group. In other words, there is no evidence to suggest pathosis which would fit the box on the right in Figure 1 and the ICD-9-CM specifications for scurvy (#267). Since vitamin C deficiency is presumed to be the sole factor in scurvy, the assumption follows in traditional circles that the ascorbate intake in this subset must therefore be optimal. The distribution of reported daily ascorbic acid consumption in a group of doctors and their spouses was made. Three points warrant particular mention. First, the average daily intake of vitamin C in these subjects is 327 mg which is approximately fivefold the present recommendation of 60 mg announced in the most recent edition of the Recommended Dietary Allowances (RDAs).7 Second, it is noteworthy that the group range is considerable (from 15 to 1120 mg). Finally, according to the cut-off point of 60 mg now set, about one in six or seven subjects displayed suboptimal, if not scorbutic, intake.
No one will argue with the fact that with advancing age, there is an overall increase in symptomatology. Older subjects have more problems than younger people. This is confirmed in this study of the health of health professionals. The question now to be resolved is whether there exist connections between this nonspecific clinical picture and daily vitamin C consumption in nonscorbutic subjects. Figure 2 depicts the relationship between clinical symptoms and signs (as shown on the ordinate) and age (as described on the abscissa) in relationship to daily vitamin C intake. It is clear that the group characterized by the lowest (but still generally acceptable RDA) ascorbic acid consumption (less than 100 mg per day) shows, that at all ages, there are the greatest number of nonspecific and usually unclassified clinical symptoms and signs (16.6, 18.2, and 18.9). The subset representing the highest vitamin C intake (200+ mg daily) is associated with the least clinical pathosis at all ages (12.7, 13.9, and 17.1). Finally, it comes as no surprise that the subjects occupying the inbetween position in terms of daily C intake (100-199 mg) occupy intermediate clinical places (13.7, 16.8 and 17.9). Lo and behold…the 50+ year old subjects consuming the greatest amount of vitamin C are clinically like the 40 year olds with the least intake of ascorbic acid. Here is an excellent demonstration of the well-known observation that some people can be 70 going on 40!
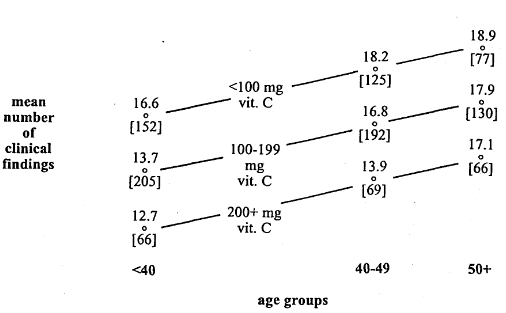
Figure 2. The mean number of clinical findings (Cornell Medical Index Health Questionnaire) in terms of daily vitamin C consumption. With advancing age, pictured on the horizontal axis, there is an increase in the number of clinical symptoms and signs. However, those consuming the largest amount of vitamin C (200+ mg daily) tend to report at all ages the fewest clinical findings.
Summary and Conclusions
The point of the story, as underlined in these pages, is that health/disease patterns become more meaningful when one de-emphasizes traditional nosologic classifications (e.g. scurvy) in favor of attention to the earliest evidence of pathology (the nonspecific matrix of pathosis), which basically reflects our lifestyles and our mistakes in living.
Here is a superb demonstration of one of the many myths and magics which contribute so vividly to modern medical ignorance.
References Cited:
- Watson TJ: “Remarks on Health Care.” Presentation before Mayo Clinic, Rochester, Minnesota, 19 November 1970. Reprinted in Journal of the American Society of Preventive Dentistry, January-February 1973.
- Schorr D: Don’t Get Sick in America. 1970. Nashville, Aurora Publishers, Inc.
- Cheraskin E: “The Name of the Game is the Name.” Proceedings of the San Diego Biomedical Symposium, 13:31-39, February 1974.
- Cheraskin E: “The Name of the Game is the Name: A Second and Harder Look.” Journal of Holistic Health, 6:73-79, 1981.
- International Classification of Diseases, 9th Revision, 4th Edition, Clinical Modification (ICD-9-CM). 1992. Los Angeles, Price Management Information Corporation.
- Cheraskin E: “Vitamin C…Who Needs It?” Health and Nutrition Update, 1992/1993.
- Food and Nutrition Board/Commission of Life Sciences/National Research Council: Recommended Dietary Allowances, Tenth Edition. 1989. Washington, D.C., National Academy Press.