
Access to all articles, new health classes, discounts in our store, and more!
The “Ideal” Daily Protein Intake
Published in the Journal of the Medical Association of the State of Alabama, Vol. 47, No. 5, November 1977.
* * *
Introduction
The adult RDA (Recommended Dietary Allowance) for total protein has been set at 56 and 46 gms. per day for the male and female respectively.1 The Food and Nutrition Board grants the RDA is designed to protect only against classical protein deficiency states. There is no claim that this dosage is intended as the “ideal” daily intake for the maintenance of optimal health.
A series of studies2-11 has attempted to develop a truly “ideal” daily consumption based on the hypothesis that relatively symptomless and sign-free persons are healthier than those with clinical symptoms and signs. Therefore, the intake of such groups might well provide a basis for designating the “ideal” daily total protein consumption.
Method of Investigation
One thousand forty dentists and their wives were evaluated in terms of daily reported total protein consumption as judged from a food frequency questionnaire. Clinical state was graded by the Cornell Medical Index Health Questionnaire (CMI). The CMI is a self-administered health questionnaire consisting of 195 questions. Each question is answered by circling the word “yes” or “no.” The questions are phrased so that the affirmative answers indicate pathology. The clinical findings in this report are the total number of affirmative CMI responses (CMI score).
Results
Table 1 shows (line 1) the daily total protein consumption of the entire group of doctors and their wives. In this sample of 1,040, the CMI ranged from 0 to 125 with a mean and one standard deviation of 15.9 ± 12.4. The daily reported total protein intake ranged from 25 to 257 gms. with a mean and standard deviation of 103 ± 36 per diem.
Table 1–relationship of reported daily total protein intake (food frequency questionnaire) and reported total clinical findings (Cornell Medical Index Health Questionnaire) in a presumably healthy male and female sample

This is approximately two-fold more than the RDA. Parenthetic mention must be made that both the American Medical Association12 and the American Dental Association13 have indicated that the type of doctor interested in his own health is already above average in health. Hence, in the usual context, these values in line 1 of Table 1 would be viewed as “ideal” when in fact, they are only normal (average).
Deleting all subjects with 50+ symptoms and signs leaves a sample size of 1018 (line 2), a mean and standard deviation for the CMI of 14.8 ± 9.9, a total protein range of 25 to 257 gms. and a mean and standard deviation of 103-36. Exclusion of all subjects with 40+ symptoms and signs (line 3) nets a sample whose daily total protein consumption is 103 ± 36. Proceeding through the eleven lines of this table, the daily total protein intake slowly rises as the number of allowable clinical symptoms and signs (CMI score) is reduced.
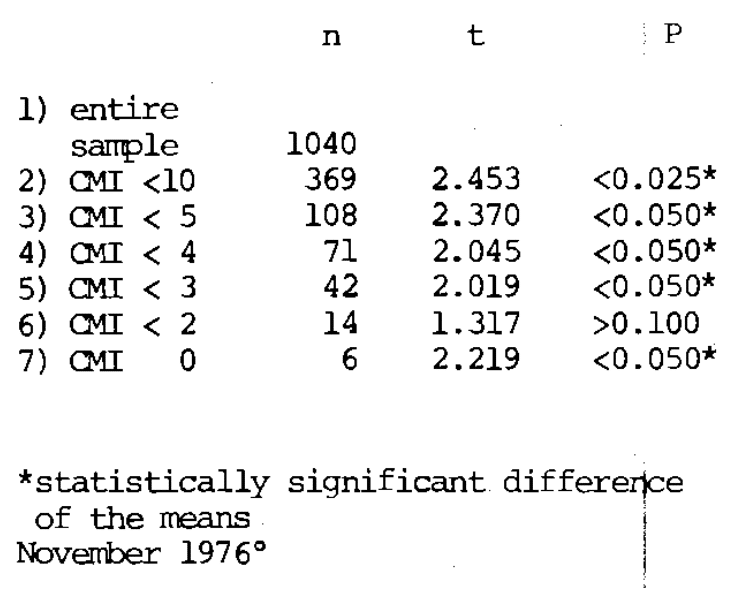
The significance of the progressive increase in the mean total protein intake by groups with progressively fewer symptoms and signs of disease is tabulated in Table 2. Compared with the entire sample, there is a statistically significant increase in mean protein intake in the subjects with less than ten, five, four, three, and zero CMI findings.
Table 2–statistical significance of the relationship of total protein and reported clinical findings (CMI)
This approach indicates that the healthier the sample, the greater the daily total protein intake. Under the conditions of this experiment, approximately 125 gms. of total protein may be designated as the “ideal” daily allowance. This is approximately two and one-half times the RDA.
It is recognized that the “ideal” is nonexistent as a theoretic endpoint since there is biochemical individuality and because the state of the measurement art leaves much to be desired. Nonetheless, the technique utilized here provides a goal not previously considered.
Summary
To determine the optimal total protein intake, 1040 dentists and their wives were evaluated in terms of their clinical symptomatology and total protein consumption.
In a progressive selection of healthier subgroups (those with fewer and fewer symptoms and signs), the total protein intake increased to over twice the RDA.
References Cited:
- Food and Nutrition Board, United States National Research Council-National Academy of Sciences. Recommended dietary allowances. 1974. Washington, D. C., National Academy of Sciences.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F. H. “The ‘ideal’ daily lysine intake.” IRCS Med. Sci. 5: 390, 1977.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F. H. “The ‘ideal’ daily vitamin C intake.” J. Med. Assn. St. Alabama 46: No. 12, 39-40, June 1977.
- Cheraskin, E. Ringsdorf, W. M., Jr., Medford, F. H., and Hicks, B. S. “The ‘ideal’ unrefined carbohydrate intake.” J. Am. Soc. Prevent. Dent. 7: No. 1, 6-7, January-February 1977.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F. H. “The ‘ideal’ daily niacin intake.” Int. J. Vit. Nutr. Res. 46: No. 1, 58-60, 1976.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F. H. “The ‘ideal’ daily vitamin A intake.” Int. J. Vit. Nutr. Res. 46: No. 1, 11-13, 1976.
- Cheraskin, E. and Ringsdorf, W. M., Jr. “How much refined carbohydrate should we eat?” Amer. Lab. 6: No. 7, 31-35, July 1974.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F. H. “The ‘ideal’ daily vitamin B1 consumption.” J. Oral Med. (in press)
- Cheraskin, E., Ringsdorf, W. M., Jr. and Medford, F. H. “The ‘ideal’ daily threonine intake.” (pending publication)
- Cheraskin, E. “The name of the game is the name.” Proc. San Diego Biomed. Sympos. 1974, 13: 31-39, 6-8 February 1974.
- Cheraskin, E. “The name of the game is the name.” In Williams, R. J. and Kalita, D. K. A physician’s handbook on orthomolecular medicine, 1977, New York, Pergamon Press. pp. 40-44.
- Editorial, “You may be sicker than you think.” J.A.M.A. 181: No. 2, 27, 22 September 1962.
- “ADA health screening program for dentists.” J.A.D.A. 79: No. 2, 235, August 1969.