
Access to all articles, new health classes, discounts in our store, and more!
The Experimental Basis for a New Theory of Dental Caries, with Chemical Procedures for Determining Immunity and Susceptibility
Read before the Dental Society of the State of New York, Albany, May 11, 1932. Published in Dental Cosmos, December 1932.
* * *
Introduction
The control of dental caries has been one of the most difficult of the major health problems of the past half century. This has been due primarily to absence of knowledge as to its etiology. This is the most important problem confronting the dental profession today, both because of the evidence that caries is on the increase in many districts and because of the metastatic involvements arising from dental focal infections made possible by dental caries.
The theories as to the etiology of dental caries that have been propounded as a result of past investigations can be divided into two distinct groups: most of the theories have been related directly to the external environment of the tooth; some of the later theories have been related to the internal environment of the tooth. Little or no evidence has been presented associating these two. The studies herewith presented provide an important connecting link.
Miller’s outstanding work presented strong evidence of a bacterial origin of dental caries. Black1 has presented data indicating that dental caries is not related to the structure of the tooth; that so-called soft teeth are no more susceptible than so-called hard teeth; that the active cause of caries is a thing apart from the teeth themselves acting upon them from without; that caries of the teeth is not dependent upon any tissues of the teeth but on conditions of their environment. He further states, “There is no basis for the treatment of pregnant women medicinally with the view of furnishing lime salts to prevent the softening of their teeth, or with the view of producing better calcified teeth in their offspring.”
The slogan of oral prophylaxis for the last two decades has been largely built around the concept that dental caries is primarily dependent upon cleanliness of the surfaces of the tooth. Williams has supported this view, which finds its expression in a phrase which he advises as he coined; namely, “a clean tooth will not decay.” Clinical results have not supported this view. Williams’ intensified studies placed him in accord with Black’s fundamental concept that the cause is to be found in the external environment rather than in the structure of the tooth.
During the past decade much work has been done on the relation of the acidophilic bacteria of the month to dental caries. These studies have been largely presented by Rodriguez,2 Bunting and his associates3 in this country, and James4 and his associates in England. Their studies have not indicated that dental caries can be controlled by the use of bactericides, notwithstanding the fact that the acidophilous group of organisms has tended to be less abundant in mouths without active caries than in those with active caries.
The importance of the texture of the food has been emphasized by many workers. An important recent contribution dealing with this phase has been presented by Hoppert5 and his associates. They have interpreted their studies to indicate that dental caries developed much more readily when rats were eating coarse particles of cracked corn than when eating fine particles.
A new approach to nutritional problems has been provided in the last two decades by knowledge of organic catalysts, some of which have been identified as vitamins. These would seem to have a direct relationship to the internal environment. Evidence has been presented indicating the importance of vitamin C, not only in soft tissues as scurvy but in the formative processes of hard tissues, particularly the teeth. Howe6 and Hanke7 have emphasized the importance of vitamin C in the etiology and control of dental caries.
The use of synthetic vitamin D as activated ergosterol has been recommended, and data presented to support this view by May Mellanby.8
A series of clinical and laboratory studies covering several years, with several progress reports, have been conducted by Price,9,10,11,12,13,14,15,16 indicating that the addition to almost any average diet on which dental caries was developing of fat-soluble activators coming from butter and cod-liver oil, with a reinforcement of minerals in milk and the entire mineral content of selected cereals, is competent to control dental caries to 90 per cent efficiency in even the worst cases.
McCollum and Klein17 have emphasized the importance of an adequate mineral ratio and content of calcium and phosphorus, which for the rat might he obtained largely from inorganic sources.
The controlling influence of the pulp and of an internal circulation in the dentin from the pulp has been postulated, and is stressed by Bödecker at this meeting.
We have accordingly today supporters of a variety of viewpoints. There are those who say that caries is of bacterial origin; others consider it to be all or partly nutritional; and there are others who would say food has little or nothing to do with it. Some would expect to accomplish control of caries by prophylactic procedures; others believe that prophylaxis cannot prevent dental caries or at least that it is not adequate alone. Some would persuade the public that particular brands of washes and dentifrices can accomplish the desired results. Others would put primary emphasis upon the mechanical phases, such as the method of using the brush, the coarseness or hardness of foods eaten, etc.
As in all health problems, we get our standards from Nature. When we study Nature we find that animals throughout the passing periods have been largely immune to dental caries, that many races of humans have been immune, and that limited groups are today immune. These immune peoples, whether of the past or present, have had very little knowledge of the toothbrush, mouthwashes and dentifrices.
From the above it is suggested that progress, when it is made, must be through a better understanding of the natural laws as involved in nutrition and as physically expressed in the internal and external environments of the teeth, as these vary with susceptibility and immunity to dental caries.
The investigations herein reported have been directed to throw further light on this phase of the problem.
Experimental
Since our problem of the etiology and control of dental caries involves the behavior of the calcified tooth tissues in the presence of biologic fluids, internal and external, it has seemed fundamental that we should know more about the chemical and physical characteristics of these fluids, and that studies should be made as to the behavior of calcified tissues of other parts of the body in the presence of changing conditions of the fluids involved. As a part of this study and the general one of the nature of the vital processes involved in health and disease, with particular emphasis on dental disease, the writer has been accumulating data from blood chemical analyses of the patients under his observation for twelve years, and on saliva for six years. These include at this time over 2000 blood chemical analyses and over 400 saliva analyses. These have been progressively more detailed and at present the chemical and microscopic studies on the blood, saliva and urine total approximately 150 different determinations on each case. In the last 800 of these blood studies, over a period of about six years, there have been included determinations of data on the variations in the behavior of bloods in the presence of calcified material, usually powdered bone. These studies have thrown very important light on the physico-chemical factors involved in the presence of biologic fluids when in contact with calcified tissues.
In general, it has been found that when finely powdered bone dried at room temperature in ordinary atmosphere is placed in normal blood serum, the serum will give up from 30 to 50 per cent of its calcium and nearly as much of its inorganic phosphorus. Further, this transfer of calcium and phosphorus from the blood serum to the bone chips or in opposite direction has a very direct relationship to the constitutional well-being and to the general health of the individual. It has, indeed, been found that frequently with phosphorus, and occasionally with calcium, the transfer will be in the opposite direction, showing that there is an avidity on the part of the blood serum for calcium and phosphorus, such that it will take these from calcified bones, even though in normal blood the movement is always in the opposite direction; namely, from the serum to the bone chips. A comparison of the physical state of the individuals with regard to the structure of the bone can be splendidly illustrated in relation to these phenomena.
In Fig. 1 will be seen two groups of individuals, the first group including fifty and the second, ten individuals. The physical characteristics of the fifty are those of miscellaneous cases presenting with dental problems and not generally seriously ill. From their history and from the roentgenograms of the teeth and supporting structures and of other bones of the body, it was apparent that these individuals are not in a marked state of tissue decalcification. In this group the average percentage of transfer of calcium from blood serum to bone chips is 27 per cent and for inorganic phosphorus, 18 per cent. While this is not as much as normal, it will be seen that they are all in this general phase. The fifty cases were selected from a group of sixty consecutive cases. Ten were considered separately because they had marked evidence of calcification disturbances; some had had spontaneous fractures. In this group of ten it will be seen that the average calcium transfer from the blood serum to the bone chips was 24 per cent of the total calcium contained in the blood serum. Not only did inorganic phosphorus fail to be transferred from the blood serum to the bone chips, as in the other group, but, on the contrary, an amount of inorganic phosphorus was removed from the bone chips and taken up by the blood serum equal to an average of 28 per cent of the total serum inorganic phosphorns. These phases are shown in this figure by the rise or fall above or below the base line crossing the center of the chart. The calcium is shown by a single line and the phosphorus by a double line.
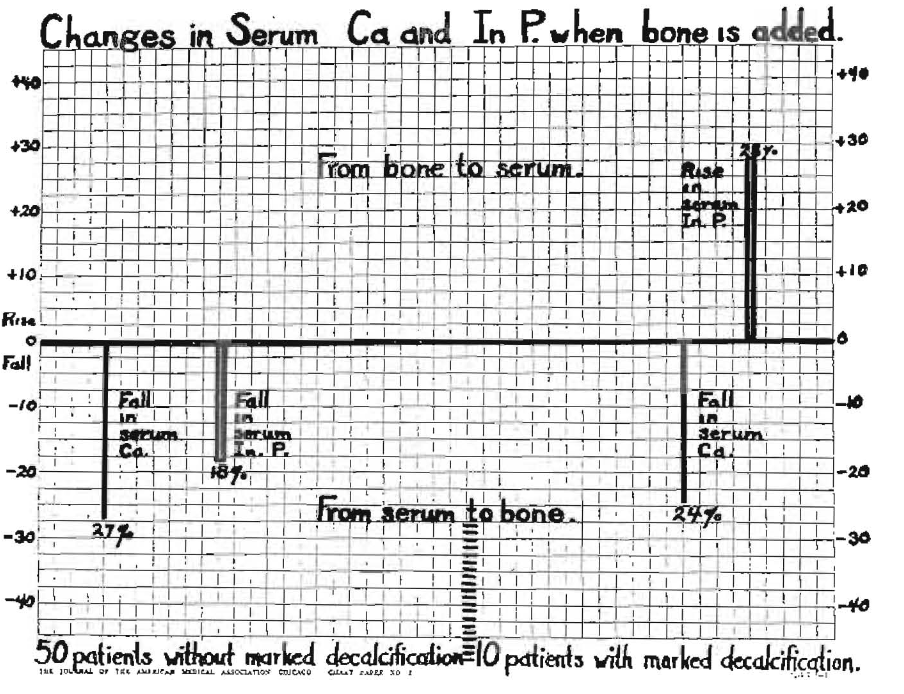
Fig. 1
It is particularly important that we observe the effect of treatment on these apparent imbalances. This is shown graphically in Fig. 2. The first patient is one with a spontaneous fracture. It will be observed that before treatment the calcium behaved about normal. The inorganic phosphorus, however, was in opposite phase, an amount equal to 35 per cent of the total being taken from the bone chips and transferred to the blood serum. After two months of nutritional treatment, the fracture showed splendid callus formation, with progressive calcification of all the bones and a marked improvement in general health. The phosphorus changed with treatment to a reverse phase, approaching but not yet reaching normal. Forty per cent of the calcium now passed from the serum to the bone and 15 per cent of the inorganic phosphorus moved in this direction.
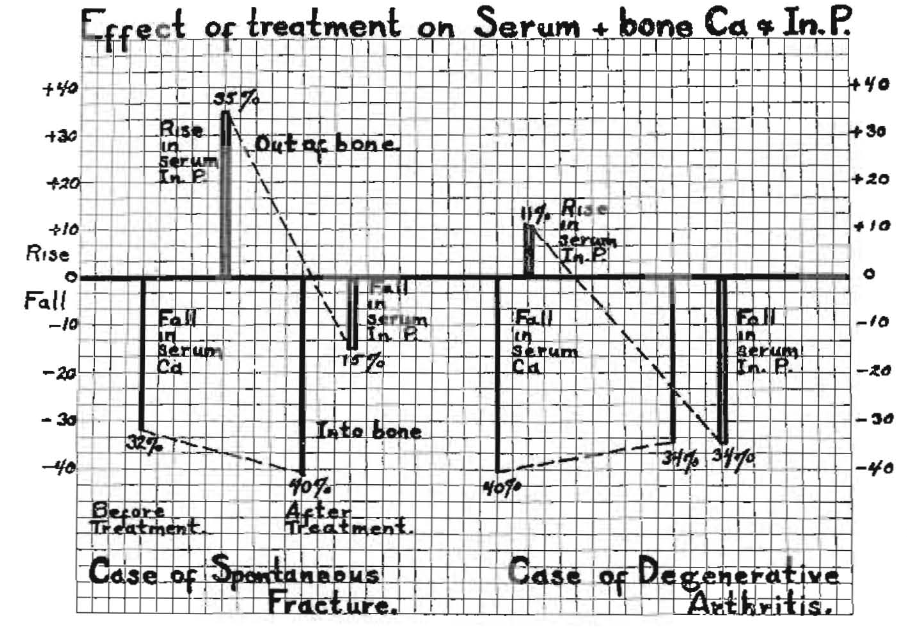
Fig. 2
In the second case shown in Fig. 2 is illustrated a case of the degenerative type of arthritis with extreme decalcification of all the bones. Again the calcium factor will be seen to behave practically as normal both before and after treatment. There is a marked change, however, in the inorganic phosphorus. Before treatment an amount equal to 11 per cent of the total in the serum passed from the bone chips to the serum, but after twenty-four days on the dietary program specially designed to meet this emergency, the phosphorus factor changed to practically normal; namely, 34 per cent of the total inorganic phosphorus of the serum now passed to the bone chips.
This phase is so important that it is desirable to observe another and even more extreme case which is shown in Fig. 3. This young woman has suffered so many spontaneous fractures that she can scarcely count them. She has had nineteen in one year. It will be seen from the structure of the bones that they were not able to even resist the normal pull of the muscles and had curved. The decalcification has extended nearly to the cortex of all the bones. Her father told me that at two different times he had seen her with both legs and one arm in a cast at the same time. She has spent many years of her life in casts.
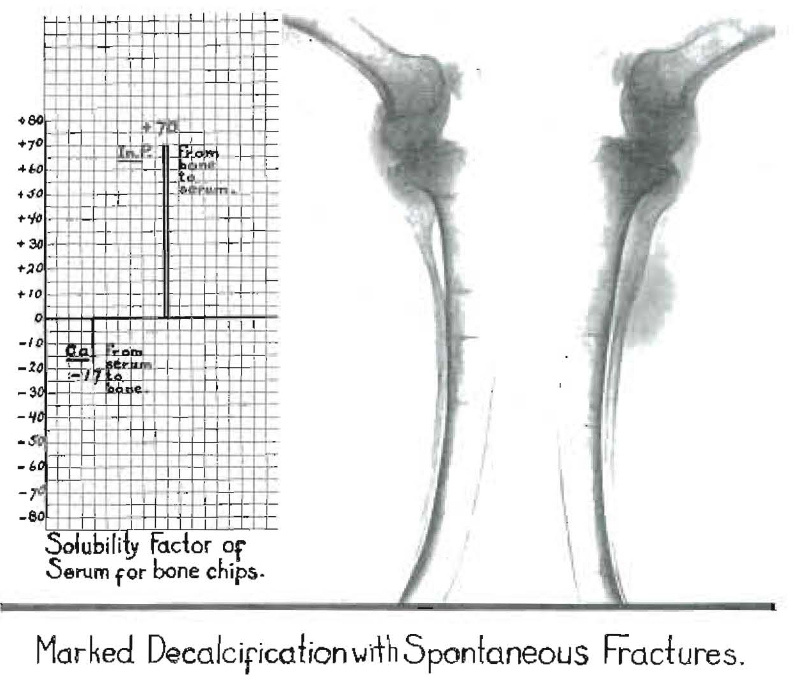
Fig. 3. The marked decalcification shown in the bones is accompanied by a movement of phosphorus from bone chips to blood serum in amount equal to 70 per cent of total inorganic phosphorus of scrum. Calcium moved in the normal direction, though in reduced amount from normal of 17 per cent.
We are here primarily concerned with the behavior of the blood serum in relation to bone, which is shown graphically in the same figure. The extent to which calcium moved from the serum to the bone is much less than normal, the reduction being 17 per cent of the total. However, the phosphorus moved rapidly from the bone chips to the serum of this patient to an amount equal to 70 per cent of the total inorganic phosphorus of the serum. It will readily be seen that, to the extent that this process was operative in the body, there would be marked demineralization of the phosphorus. It is of interest that the history of this case showed a nearly normal early childhood, with progressive development of disturbed growth and easily produced fractures following childhood sicknesses. This individual has never used dairy products, at least not since childhood, and but little then.
These data suggest that the forces within the body must be very strong which would prevent bones from weakening or dissolution if the plasma in circulation had such an avidity for phosphorus as this patient’s serum does in the presence of bone chips. Second determinations following treatment are not yet available.
Since the chemical content of tooth structure and of bone is so similar, differing largely in organic matter, it has seemed probable that a similar relationship would be found between tooth structure and circulating blood within the tooth and the saliva and the external tooth surface. Accordingly, this program has involved the routine study of the behavior of the saliva of the individual with regard to the direction of the movement of minerals from saliva to calcified structure or in the opposite direction. The saliva study has been associated with the blood studies in about the last 400 cases, besides being applied directly to salivas in a large number of cases where the blood chemical analyses were not included. The importance and significance of the findings revealed in these studies can be evaluated by data relating to particular individuals and by groups, there being a distinct advantage in the latter.
It has continually been observed that even the blood picture with regard to the amount of calcium and phosphorus that will leave the serum and go into bone had a direct bearing upon not only the physical welfare of the individual, as presented in Figs. 1 and 2, but often appeared to have a direct relationship to a tendency to dental caries; and, further, that with improvement in general physical condition as a result of an improved nutritional program, there was not only an improvement in the solubility factor of the blood serum but also in the saliva as a result of treatment. It has also been observed that when the factor of safety is low in the blood serum, it is low in the saliva.
The application of this method of study to practical cases has now been applied to several hundred cases. It has been deemed exceedingly important that controlling factors should not be allowed to mask the interpretation of the data. The principles involved are fundamental, and they should obtain in severe cases of dental caries, regardless of geographic location and racial characteristics. I therefore endeavored to establish data obtained from patients in distinctly different environments. My clinical cases furnish several hundred different types provided in a variety of families and types of homes and home life as found in a large city.
It is important to know whether similar conditions would be found in average families from city life in other parts of the world. This I have undertaken to provide and at the same time obtain helpful criticism of the procedure by having a group of coöperating dentists, usually five, in each of about a dozen cities distributed throughout the United States, Canada and Switzerland. Under this arrangement these dentists have been requested to send roentgenograms of the teeth, history of the case on a questionnaire furnished, and also a sample of saliva and culture from the mouth. We furnish the containers for that purpose. The saliva tests are repeated at the end of one month and again at the end of three months. Each dentist is requested to select a typical severe case of dental caries, preferably of the “teen” age, or a case of pregnancy. I have undertaken, with the patient’s cooperation, to provide additional vitamins and directions for reinforcing the diet where found necessary. Notwithstanding the disadvantage of absence of personal contact, the evidence indicates a splendid degree of success, as will be shown, and splendidly comparable to data obtained directly from patients with whom I have personal contact for examination and instruction. This has furnished two groups differing primarily in geographic location, both, however, having the ordinary severe conditions of dental caries found in homes with average nutritional programs.
It has been desirable to have still another in which the individuals load, group it possible, a more rampant type of dental caries and associated with a more extreme systemic disturbance. For this, a group of children has been selected from a district of a city that has been seriously handicapped by the industrial depression. This district is in the vicinity of the steel mills, which have been closed down for a year or two. The same type of data has been obtained for these children; namely, roentgenograms, saliva chemical analysis, and the placing of fillings in open cavities in most cases. In the first two groups all that was deemed necessary was to provide additional activators, to be described, and some reinforcement of the dietary program. In this last group there was no possibility of the parents providing an adequate nutritional program.
Through the kind and efficient cooperation of Reverend Edwin A. Brown, of the Broadway Methodist Episcopal Church, which is in the vicinity of these homes, and working in complete cooperation with his staff, arrangements were made for providing one reinforced meal a day to the most serious of these cases. In all, about three dozen have been on this program. The content of the meal provided will be described. The examination of the mouths of these children revealed many very large open cavities in first and second permanent molars, many of which apparently involved the pulp, but with pulps still vital. Some of these will be shown in roentgenograms.
In Fig. 4 will be seen data being obtained from each of these three groups. The first group is called Broadway Mission Group; the second, Other Cities Group, and the third, Office Clinic Group. The severity of the dental caries, as demonstrated by the roentgenograms, all of which are in my files, was clearly much greater in the Broadway Mission Group children than in those of the other two groups. This was to be expected. However, this is a matter of degree only, for many areas of decalcification, chiefly on occlusal and proximal surfaces, are found in practically all of these cases of all three groups.
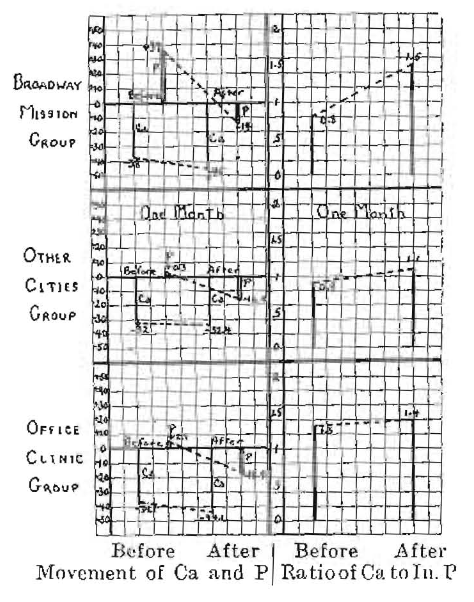
Fig. 4. Behavior of In. P of saliva of three groups of patients with dental caries before and after treatment.
The routine chemical analysis of the saliva for all of these cases includes the following: pH or hydrogen-ion concentration, potassium, sodium, total calcium, diffusible calcium, non-diffusible calcium, per cent diffusible, saliva plus bone calcium, change from same, percentage change, total phosphorus, inorganic phosphorus, percentage of total phosphorus, that is, inorganic, diffusible phosphorus, non-diffusible phosphorus, percentage of inorganic phosphorus, saliva plus bone phosphorus, change produced by bone, percentage change, product of calcium and inorganic phosphorus, ratio of inorganic phosphorus to calcium, ratio of diffusible phosphorus to diffusible calcium.
In the chart only two factors are shown before and after treatment. In the first square for each group the movement of the calcium and inorganic phosphorus of the saliva as a result of adding bone chips to the saliva is illustrated. It will be seen that the line representing calcium, reading down, represents an average reduction by calcium going from the saliva to the bone chips, of 38 per cent. The phosphorus is graphically shown by the double lines and will be seen to read above the base or zero line to almost the same extent that the calcium is shown below the line; namely, an increase in an amount equal to 37 per cent of the total inorganic phosphorus of the saliva. We will keep in mind that in normal saliva both phosphorus and calcium have been found to move in the directions that the calcium has moved here.
When we compare the calcium and phosphorus movement in the saliva of the Broadway group, with its very severe dental caries, with that which obtained in the two other groups, we note that the essential and striking difference is one of degree in the movement of the phosphorus. The average showed some movement of phosphorus from the bone chips to the saliva in the members of these last two groups. The calcium factor in all three groups was quite similar.
The addition to the daily intake of food of fat-soluble activators, to be described, with some improvement in mineral-carrying foods, made a remarkable change, in that the phosphorus ceased to move from the bone chips to the saliva but now moved from the saliva to the bone chips. The rapidity with which this change can be brought about will presently be shown.
The individuals in the Broadway group received as a reinforcement one specially prepared meal reinforced in activators and minerals. Many of the children received at home little but plain unsweetened coffee and white bread, and often little of either of these. A special meal was designed to furnish nearly the amount of the body’s daily requirements in calcium and phosphorus and activators. After six weeks’ treatment the calcium is seen to be in the same phase as before, with a slight increase in the movement of the percentage of calcium from the saliva to the bone chips. The inorganic phosphorus in the time covered in this graph changed in the same direction for the Broadway Mission group to an amount equal to 14 per cent of the total saliva inorganic phosphorus; in the Other Cities group, to 16 per cent and in the Office Clinic group, 18 per cent. The time covered by the treatment in these cases was six weeks for the Broadway group, one month for the Other Cities group and an average of four months in the Office Clinic group. At the time of this writing, which allows the Broadway group twelve weeks’ time, the phosphorus movement has increased in the same direction, averaging 39 per cent of the total saliva inorganic phosphorus. The third monthly salivas for the Other Cities group are not available.
The ratio of inorganic phosphorus to calcium was 0.8 for the Broadway Mission group; 0.9 for the Other Cities group and 1.3 for the Office Clinic group. These factors changed after treatment to 1.5, 1.1, and 1.4, respectively. The increase in weight in the Broadway Mission group was from an average of 73.8 per cent to 77.6 per cent in twelve weeks’ time. These data are not yet available for the other groups.
It is important to note that this dietary program does not necessarily increase weight. It does tend to bring individuals more nearly to normal, which often means a loss in weight. However, for growing children it generally does mean a gain in weight.
For those who wish to read the data as oxids of the minerals, the correction factor would be obtained by multiplying the amount of the element shown as follows: calcium by 1.4, phosphorus by 2.29, potassium by 1.2, sodium by 1.35, magnesium by 1.66.*
A chemical analysis of one of the test meals showed calcium in grams as CaO at 1.48 grams, phosphorus as P2O5 at 1.28, magnesium as MgO at 1.06, fats at 10.7 grams, proteins at 8.89 grams. This included one helping only of the various elements of the meal, whereas many of the children took a second helping of several courses. Two children of five years each took four bowls of thick soup the first two days (about two quarts). This meal was begun by each child marching up in a line and taking half a glass of thick tomato juice or citrus fruit and a teaspoonful of half and half of a high vitamin cod-liver oil and high vitamin butter concentrate mixture provided by the writer. They then proceeded to the tables and had as their first course a large bowl of vegetable and meat soup containing a large assortment of vegetables and chopped meat prepared as a stew. Many of the children took a second liberal helping of soup. For the next course they had sliced canned peaches and delicious rolls made of freshly ground whole wheat, to which had been added an additional quantity of fresh wheat germ. The whole wheat was ground in a motor-driven coffee mill set up in the kitchen, and freshly prepared from day to day. These rolls were spread liberally with an extra high vitamin butter provided by the writer, which had been produced by cows while pasturing on green wheat. Unfortunately, as yet this has to be shipped long distances and most of it provided by special arrangement for feeding the dairy cows. Each child had also one or two glasses of milk. This meal is varied from day to day but so designed as to maintain these high levels of fat-soluble activators (minerals and grain embryo). These children receive six meals a week. The source of vitamin C was varied. Carotene was reinforced by adding to the vegetable soup finely ground small carrots of deep yellow color. These and the wheat germ were added to the vegetable soup after it was removed from the stove, but still hot, to avoid the high temperature and long cooking, which would injure the activator content.
Individuals in the Other Cities group and the Office Clinic group received the same fat-soluble preparation placed in 0 size capsules containing six-tenths of a gram. Three of these capsules were taken with each meal. An arrangement was made for providing freshly ground whole wheat and a freshly prepared wheat germ for all the patients of the Other Cities and Office Clinic groups. Instructions were given for the preparation of this cereal by cooking the crushed wheat in a double boiler from two to four hours and, before removing from the fire, adding an amount of wheat germ, according to the percentage of embryo contained, sufficient to provide ten per cent pure embryo, which gets only the cooking of the cooling-down process. Enough can be prepared for several days and the portion desired warmed up each day. It can be varied and the appetizing factors, which are very high, can be enhanced by adding pieces of fresh or dried fruits and nuts.
The method of preparing the activator mixture is as follows: A natural high vitamin cod-liver oil is selected by chemical tests, using the Lovibond Tintometer method of reading antimony trichloride colorations for vitamin A as suggested by Carr and Price18 and Drummond aud Hilditch.19 The vitamin D content is determined by a modification of the Yoder20 hydriodic acid test. The high-vitamin butter is selected by the same procedure. I have discussed these factors in detail in earlier communications.
When I have located a sample of butter–and a very small percentage of available butter samples will be considered sufficiently high in vitamins for this use–the low-melting sterols are separated by chilling and centrifuging while in a proper physical state. The oil thus produced remains liquid at room temperature, is completely miscible with the cod liver oil, has a surface tension that does not leak in the capsules.
These studies are including observations on the relations of acidophilic bacteria and dental caries and the change in incidence and number of these organisms under these nutritional programs.
An important phase of these nutritional studies in relation to the control of dental caries has been the rapid change in the development of the dentin about the pulps of the teeth, together with a marked increase of density of tooth roots as well as of crowns when a patient is under treatment. In Fig. 5 will be seen a striking illustration of this phenomenon. In A, the first view, caries had decalcified apparently through to the pulp from a distal cavity in the bicuspid and underneath a leaking alloy filling. The dentin was partially disinfected and a protective capping placed over it. The removal of the involved dentin was delayed until the pulp could build in a new protecting wall. The second view, B, shows the wall of dentin being built beneath the area of approaching caries underneath the dressing and temporary filling. The third view, c, shows a splendid protecting wall of dentin over the area which originally constituted the virtual exposure. The involved dentin has been removed.
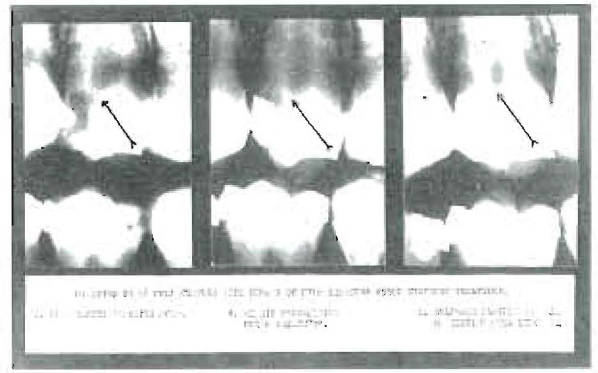
Fig. 5
This nutritional program has made possible a new prognosis for teeth with virtual exposures. This principle has been applied in a number of cases. The children constituting the Broadway Mission group presented many teeth with conditions of this type. Several of these are shown in Fig. 6. This is of great significance in that the dental caries had decalcified the tooth through to the pulp so that there clearly would have been exposure had the decalcified dentin all been removed. These pulps are progressively building in new walls, which are readily disclosed by the Roentgen rays in even eight weeks’ time. The upper or left hand picture in each case shows the condition at the time treatment was begun; in many cases temporary treatment fillings are shown in place. The lower pictures show the same teeth six or eight weeks later, as indicated. Only two cases gave trouble and they had considerable apical involvement. To save space only six of these cases are shown here.
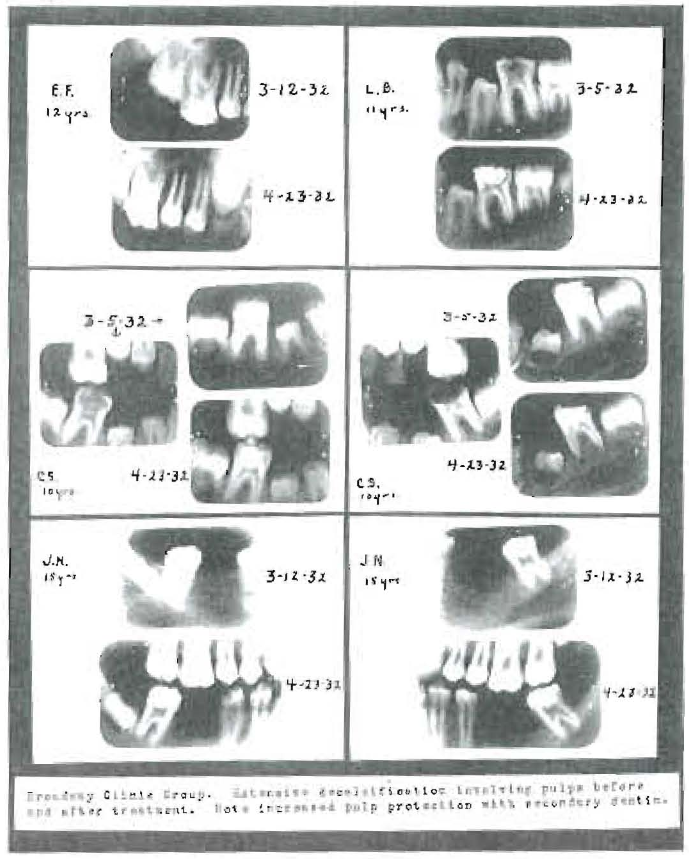
Fig. 6
One of the cases of excessive caries, which had destroyed all of the occlusal surface of the crown and the dentin with apparent decalcification to the pulp chamber, did not receive a temporary filling due to an oversight, and a large area of dentin was left freely exposed to the saliva. When this girl was sent for to have this tooth taken care of, it was found that the dentin had become very tough and dark in color, with evidence that the active caries had ceased even without filling. It is my experience that, where decalcification has not extended through the enamel to the dentin while on this nutritional program, dental caries ceases to be active even in the small proximal contact cavities.
During the years that this nutritional program has been under development as a practical procedure for the control of dental caries, results have been reported from time to time indicating the percentage of control exceeding 90 per cent for even difficult and rampant cases. Many individuals have been put on this program who had been referred by other dentists because of exceedingly rampant dental caries. These cases frequently had even two and three dozen open cavities.
A typical case is shown in Fig. 7. This boy presented with thirty-eight open cavities and with the report that the dentist could not keep up with the caries even with one appointment a week. The two upper bite-wing roentgenograms show the condition at the beginning, and it will be noted that the crowns of nearly all the molars and bicuspids have been greatly injured by dental caries. There are almost two years between the upper and lower pair of roentgenograms, and during this time few if any new cavities developed. Some old amalgam margins broke down and needed repair. This case is of particular interest because this control has been maintained notwithstanding the fact that the young man was out of the country for approximately a year of this time, living under conditions where it was very difficult to control the basic diet. The vitamin capsules were sent to him in Europe. Note particularly the reduction in the size of pulp chambers, particularly the lower left second molar, and note that the carious cavity shown in the upper view of this tooth apparently originally exposed the horn of the pulp. Similarly note the reduction in the size of the pulp chamber in the lower right first molar.
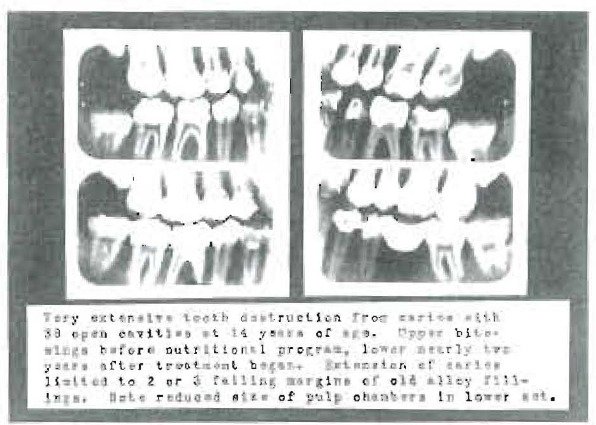
Fig. 7
Several groups of studies have been put into chart form comparing individuals with and without this defensive treatment. A summary of some of these is shown in Fig. 8, which shows in graphic form the results of five separate studies made at different times for the comparison of individuals who are treated with those who are not treated in regard to the matter of prevalence in carious cavities. “A” compares the same individuals in two different groups, neither of which received treatment in 1928 and one of which, including 38 patients, received treatment in 1929. This second group included individuals who in 1928 had excessively active dental caries; namely, an average of 8 cavities per person. In 1929, after these individuals had been put on the defensive treatment, the number of cavities dropped in this very susceptible group to 1.4 cavities per person, whereas in the other group not receiving treatment either year there were in 1928 an average of 4.85 cavities per person, and in 1929, about the same, 4.73.
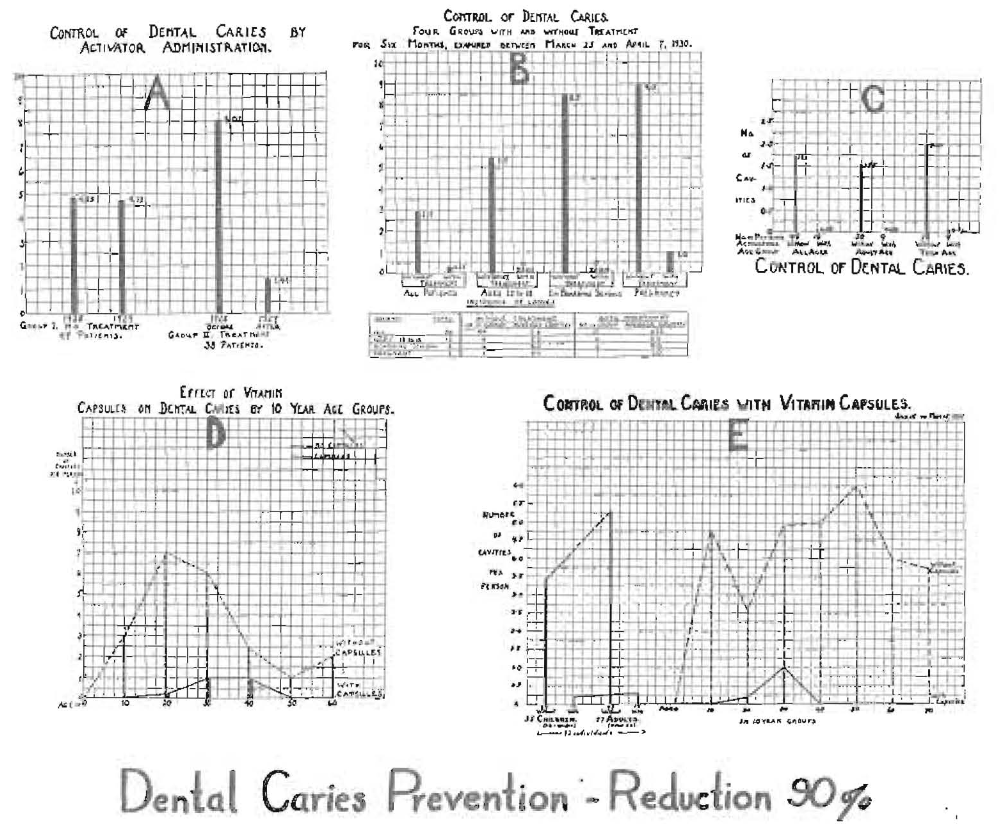
Fig. 8
In B will be seen results of the examination of individuals presenting in a two weeks’ period for their regular check-up at spring vacation in 1930. Of fifty-six patients, 44 had not received treatment and since their last examination, approximately six months previously, they had an average of 2.9 cavities per person. Twelve had received treatment and the number of cavities was 0.25 per individual. In the age group twelve to eighteen there were nine without treatment, with an average of 5.5 cavities per individual, while the six with treatment had no cavities. In the boarding school group, four without treatment had an average of 8.5 cavities, while four with treatment had no cavities. There were two cases of pregnancy; one without treatment had nine cavities and the one with treatment had one cavity.
In series C, there were sixty-six patients in which forty-eight were without treatment and for the period of study had 1.73 cavities per person. Eighteen with treatment had 0.05 cavities per person. When the adults and young people are separated, there were thirty adults without treatment; they had 1.55 cavities per person, and the nine with treatment had no cavities. In the young group there were eighteen without treatment, with an average of two cavities per person, and the nine with treatment had 0.11 cavities per individual.
In series D (1930) a group of 200 individuals, including 100 with treatment and 100 without treatment, are shown in ten-year age groups up to sixty years. The lower solid line with its upright column represents those with treatment, and the upper dotted line with upright broken columns represents the number of cavities for those without treatment. It is of interest that in the age group ten to twenty there were forty times as many cavities in those not receiving treatment as in those receiving treatment. For all the groups of this series an average difference of tenfold was found.
In series E is shown the result of another series of ten-year age groups covering the period from January 15 to May 15, 1931. In this series there were ninety-two individuals, of which number fifty-seven were adults and thirty-five were children. In this graph again, as in the last one, the lower solid line represents those receiving treatment, and the upper broken line those without treatment. It will be noted that in the twenty-four children without treatment there were 3.4 cavities per person, whereas the eleven with treatment had only 0.24 cavities per child. Of the fifty-seven adults, there were forty-three without treatment and they had 5.3 cavities per individual; of the fourteen receiving treatment there was an average of 0.3 cavities per individual. There were seventeen times as many cavities in the group of children not receiving treatment as in the group receiving it. There was a slightly larger difference in the group of adults. When divided into ten-year age groups the caries was practically controlled except in the twenty to thirty age group, which averaged one cavity per person under treatment, while those of this age not receiving treatment had 4.9 cavities per person. For the entire series as expressed in Fig. 8,A, B, C, D and E, there is an average of 5.2 cavities per person in the groups without treatment as compared with 0.55 cavities per person in the groups receiving treatment, or 9.25 times as many cavities per person in the individuals not receiving treatment as in those receiving it.
Discussion
In the light of these new data it is possible to explain some of the conflicting theories relative to dental caries. When an unerupted tooth is extracted, the surface will be permeable to dyes or silver nitrate for a conspicuous distance into the enamel. After normal eruption has taken place and the tooth is exposed to saliva for some months or years, the surface under normal conditions progressively becomes more dense, in which state dyes will not penetrate the surface. In rampant caries the change in tooth structure is often sufficient to impress operators that it is more readily cut with chisel or bur. This has frequently been noted in cases of pregnancy, and yet these teeth readily, after the patient has returned to normal condition, recover their original hardness.
An explanation is provided for these phenomena in this reverse phase, in which minerals pass out of the surface of the tooth into the saliva under conditions of stress. Normally, the minerals go in the other direction. An interpretation of the data here presented leads immediately to the mineral and activator content of the ingested foods, and the emphasis is placed on the phosphorus content. The animal life of the world has developed by adaptation to the normal balances of minerals in growing green plant structures and their seeds. It is of great significance that the plants store phosphorus in high percentage in their reproductive units, such as seeds and grains. Lactating animals similarly provide milk carrying calcium and phosphorus in liberal amounts approximating ten times the level of calcium and inorganic phosphorus in the blood per volume. Milk also provides activators or vitamins. Per volume of ingested food, cereals furnish phosphorus both in liberal quantity and high ratio to other minerals. It is of interest that the inorganic phosphorus of the saliva is from half again to twice that of the blood, whereas the calcium is usually less than that of the blood, often about one-half. This clearly indicates a special function of the salivary glands if these levels are to be maintained for establishing the environment of the teeth. This is an important provision of Nature, and can only be provided by the blood maintaining an adequately high inorganic phosphorus level.
If, as there are indications, saliva normally contains tricalcium phosphate, Ca3 (PO4), in saturated solution, which for water would be 2.7 milligrams per 100 cc., using 0.54 milligrams of phosphorus and 1.05 milligrams of calcium, this amount of water also could carry in saturated solution twenty milligrams of dicalcium phosphate, CaHPO4 ᐧ 2H2O, providing 3.6 milligrams of phosphorus and 4.7 milligrams of calcium. If the saliva were saturated with these two salts of calcium and phosphorus, they would together provide 1.14 milligrams of phosphorus and 5.71 milligrams of calcium. If, in addition to providing saturated solutions of tricalcium phosphate and dicalcium phosphate, a monocalcium phosphate, CaH4(PO4), H₂O, was formed, 100 ce. of water could carry in solution as high as 1800 milligrams of monocalcium phosphate, providing 285.71 milligrams of calcium and 442.86 milligrams of phosphorus. However, since the saliva contains other strong bases, sodium and potassium, phosphates of these would also be formed, so that all the phosphorus that would be present in the saliva would not be available for forming phosphates of calcium. Even if all of the phosphorus available and all the calcium available in the saliva were first used to produce solutions of tricalcium and dicalcium phosphate, there would not be enough total calcium and total inorganic phosphorus present to provide saturated solutions in some salivas. Salivas are being studied to throw further light on this phase of the problem.
The clinical observations of a marked increase in the density of decalcified dentin when the individual has changed from a state of susceptibility to one of immunity would seem to be related to this condition. In a previous paper we have discussed the role of vitamin A in increasing the function of the salivary glands and thus directly affecting the chemical content of the saliva.
A comparison has been made of the action of enamel, dentin and bone in regard to the movement of phosphorus and calcium to or from the saliva and blood serum. These data will be discussed in another communication.
In a previous communication16 we have reviewed data dealing with the action of fat-soluble activators in the releasing of phosphorus from phospholipids, which seem to be an important function of vitamin D, the amount of calcium phosphate that can be formed being in part provided by the release of phosphorus with the formation in tissues of tricalcium phosphate in precipitated form where the calcium is already available in the tissues when and where the phosphorus is released. An important contribution to this phase has been made by McGowan and associates. This may throw light upon the action that takes place within the tooth structure where phosphorus has been removed, leaving an excess of calcium.
We have previously reported an important phase of this problem15,22,23,24 which deals with the behavior of calcium and phosphorus in solution in various media, including biologic fluids, when these fluids are exposed to direct irradiation or placed in contact with certain substances like butter and cod-liver oil; also these when they have been exposed to irradiation. These studies have indicated that the diffusibility of calcium can be greatly modified by this procedure, there being a very marked release of the calcium from its organic bond. These phenomena also affect the phosphorus, though not to so great an extent, there being often a marked increase in the organic phosphorus in the case of blood, saliva or milk. These effects were produced by many procedures, for example, to a limited extent by direct irradiation of the animal’s or individual’s body, by the irradiation of some foods and by taking into the stomach even small doses of irradiated cod-liver oil or butter, and also to a very marked degree by rubbing these substances on the surface of the body, with the result that the phosphorus and calcium content of the blood serum has been raised by rubbing the material onto the human body or the body of experimental animals. The serum calcium of chicks with rickets was nearly doubled by rubbing the activated oil on their necks. This has developed a procedure for the management of ununited fractures and the management of arthritic processes which often produces most gratifying results.25
We have shown that blood serum shaken with irradiated cod-liver oil not only greatly changes diffusibility of calcium, but was able to increase the inorganic phosphorus of the serum from 2.9 to 4.1 milligrams, which amounts to 41.3 per cent, where an irradiation of the blood serum increased it from 2.9 to 3.75. an increase of 29.3 per cent. I have demonstrated that similar effects are produced in saliva when shaken with high vitamin butter and high vitamin cod liver oil, or when these are ingested, this being one of the routine factors being estimated as a result of administration of activators in connection with control of dental caries.
This has been an essential phase of our successful treatment of large clinical groups of dental caries patients by the two procedures of adding more activators to the food and increasing the high phosphorus-carrying foods. We do not now administer internally the activated cod-liver oil. We are obtaining best results with a mixture of high vitamin butter and high vitamin cod-liver oil.
Our extensive blood chemical studies before and after treatment demonstrate that we modify these and other factors in the blood, and our saliva chemical analyses demonstrate that we have distinctly modified both the chemical content and mineral ratios and changed the environment of the tooth by changing the direction of movement of the phosphorus.
Forbes,26 in discussing “Dental Caries from a Biochemical Standpoint,” has detailed the processes by which the solid phase tricalcium phosphate passes into solution and becomes dissociated as calcium and phosphorus ions according to known laws of ionization, and he has also illustrated the influence of changes in concentration of either of these ions on the phosphate buffer system of the saliva.
It is at this point that the activators can, by modifying the saliva, modify the ion concentration by releasing the bond of the phosphorus with organic compounds, and probably by some such mechanism as this it enhances the immunizing effect of the saliva. This very important point has not, to my knowledge, been brought to our attention as a part of the consideration in any previous discussion of the phenomena of dental caries. There are, however, other phases of this vital aspect of saliva as a controlling factor in maintaining immunity to dental caries than its buffer action which have to do with the modification of the culture medium which influences the growth of acidophilic bacteria. These data augment those presented by Klein and McCollum¹ on dental caries in rats.
If we review the theories that have been propounded and the evidence in their support, we find that most of the data can now be correlated.
Miller stressed the importance of the role of acidophilic bacteria, which theory still has a place, but the organisms cannot produce caries except where the factor of safety has gone down both generally and locally to a sufficiently low point, thus explaining also why immunity may prevail in spite of abundant bacterial growth.
Black’s evidence, indicating that both hard and soft teeth may be attacked by dental caries, immediately becomes clear since we are able to change an individual from a state of susceptibility to one of immunity in a few days’ time. The so-called dense teeth may have their surface factor of safety changed in a short period of nutritional disturbance. Similarly, while age may have a varying influence on the structure of the teeth, it will not in itself prove a protection.
The relation of prophylaxis to the prevention of dental caries seems to have a very important place, though not a controlling one, in the presence of dental caries. In those conditions which have a low factor of safety in the saliva of the mouth, though not sufficiently low to constitute a loss of immunity to caries, bacterial growth in protected areas can reduce the low local immunity to a positive susceptibility. Adequate prophylactic procedures, as so strongly emphasized by Williams and others, may make the difference in this often narrow margin of safety of the presence or absence of active caries. This also explains why in open cavities, where the saliva has free access, after the patient has been changed from a state of susceptibility to one of immunity, active caries has been checked even though no fillings are placed, while caries in protected places, for example, in the dentin beneath an adjoining proximal contact where there is a small opening through the enamel, or beneath overhanging fillings and crowns that have a physical condition which, by preventing the neutralizing effect of the saliva, provide a local susceptibility. This stresses the role of the acidophilic bacteria as a factor in the production of dental caries. While it is probable that dental caries cannot take place without their assistance, they are not able to function with the production of dental caries in any location where the phosphorns protective factors are adequate. Apparently the factor of safety of every part of the mouth will be established by the level primarily of the phosphorus factor of the saliva, and this in turn will be established through the blood stream by the nutrition, which takes us immediately to the activator and mineral content of the food, especially its phosphorus content.
Summary and Conclusions
- Based on these new data, a new theory of dental caries may be formulated as follows: Both the external and internal environments of the tooth as provided by the saliva and blood are different in individuals who are immune to dental caries from those who are susceptible. There will be included in the variations physico-chemical differences, particularly in the saliva, with regard to phosphorus and to a lesser degree with regard to calcium, so that in the immune individuals these elements will tend to be deposited into the tooth structure from the saliva, and in those individuals who are susceptible to dental caries the movement of phosphorus and, in extreme conditions, of calcium, this factor will be reduced to zero or even to a reversal of direction of movement, particularly of phosphorus. While these factors have been shown to have a relationship in many cases to the level of the total phosphorus and calcium and to the ratio of phosphorus to calcium, these relationships have not been constant. Nature seems to have provided the salivary glands with the function and capacity to increase the inorganic phosphorus content of saliva well above that of the blood in normal individuals.
- Data are presented indicating that these physico-chemical factors of blood and saliva are controlled by the presence in the food of activating substances, chiefly fat-soluble, together with adequate minerals in suitable chemical form. The fat-soluble activators are normally present in dairy products produced from very favorable plant tissues, the best of which has been found being green, young, rapidly growing wheat. Helpful activators are also found in varying amounts in cod-liver oils. A combination of the two is especially effective. Immunity to dental caries is associated with a normal or increasing density of tooth structure. These changes in direction of movement of phosphorus and calcium, particularly the former, control the factors of safety of all surfaces of the teeth with which saliva is in contact with regard to attack from fermentation processes, and account for the limiting of attack in most instances to protected areas such as sulci and proximal contacts. Bacterial proliferations of acidophilic organisms can only progress in proportion with the degree of disturbance of the activator and phosphorus factor of safety and the degree of physical protection of the areas involved.
- Means are indicated whereby the factor of safety of most available diets can be reinforced sufficiently to control dental caries by the simple means of adding a small but proper kind and amount of fat-soluble activators and a cereal providing the normal minerals of a freshly ground whole wheat, rye or oats, often reinforced to advantage with an additional amount of wheat embryo, together with a liberal supply of milk, cheese and butter. Any food combination providing the proper mineral balances and activators and other essential chemicals will provide immunity.
- A comparison of three groups of individuals with dental caries, living under various and different conditions and in different geographic locations, has shown them to respond similarly to the stress of their environment and nutrition as expressed in typical dental caries and they respond similarly to the effect of nutritional reinforcement of the same general type regardless of location.
- A saliva chemical procedure has been presented which reveals degrees of immunity and susceptibility to dental caries and indicates that individuals can be changed from a state of susceptibility to one of immunity quite rapidly and effectively.
- Many obscure phenomena, such as variations in density of tooth structure, are provided with an explanation in accordance with the clinical, physical and chemical data.
- In the light of these new data it is possible to harmonize much of the evidence that has been presented by various workers who have attacked the dental caries problem from different approaches, and also to account for the clinical experiences of workers in different countries, as well as provide an explanation for individual and group immunity and susceptibility both of the past and present for all animal species, including humans.
- The phenomena that have been emphasized in their relation to dental caries as those of behavior of calcium and phosphorus, particularly the latter, in the presence of calcified tissues, apply with evident importance in all building up and tearing down processes occurring in other parts of the skeleton, and have a constant relation and universal expression in the bones of the body as associated and correlated factors with the phenomena of immunity and susceptibility to dental caries, and offer important suggested procedures for the prevention and management of disturbed mineral metabolism, including disease affecting the skeleton.
*The assay methods used for determinations were, for Ca, the Cramer-Tisdall (Journ. Biol. Chem., 1921, 47, 475), and, for P, the Stannous Chloride method of Kutler and Cohen (Journ. Biol., LXXV, Nov. 1927, No. 2, 517) adapted to saliva.
References Cited:
- Black: Dental Cosmos, 74:231, March, 1932. Quoted from article by J. Leon Williams.
- Rodriguez, F. E.: “Studies on Specific Bacteriology of Dental Caries.” Mil. Dent. Journ. 5:199, December 1922.
- Bunting, Hadley, Jay and Hard: “Problem of Dental Caries.” Amer. Journ. Dis. Child. 40:536, September 1030.
- McIntosh, James and Barlow: “Investigation into Etiology of Dental Caries.” Brit. Dent. Journ., 43:728, August 1, 1922.
- Hoppert, Webber and Canniff: “The Production of Dental Caries in Rats Fed an Adequate Diet.” Journ. of Dent. Research, X11:161, February 1932.
- Howe, Percy R.: “Dental Caries.” Dental Cosmos, 62:921, August 1920.
- Hanke, M. T.: “The Relation of Diet to Caries and Other Dental Disorders.” Journ. A. D. A., 16:2263, December 1929.
- Mellanby, M.. and C. L. Pattison: “Action of Vitamin D in Preventing Spread and Promoting Arrest of Caries in Children.” Brit. Med. Journ., 2:1079, December 15, 1928.
- Price, Weston A.: “Control of Dental Caries and Some Associated Degenerative Processes through Reinforcement of the Diet with Special Activators.” Journ. A. D. A., 19:1339, August 1932.
- Idem: “New Light on the Cause and Prevention of Dental Caries and Some Other Degenerative Diseases.” Proceedings of VIlI Int. Dentl. Congress, August 1931; Abstracted in Dental Survey, August, September, October 1932.
- Idem: “Some Means for Improving Life by Increasing the Vitamin Content of Milk and Its Products.” The Assn. Bull. of Int. Milk Dealers, January 29, 1931.
- Idem: “A New Light on the Control of Dental Caries and the Degenerative Diseases.” Journ. of A. D. A., 18: 1189, July 1931.
- Idem: “Some Contributing Factors to the Degenerative Diseases, with Special Consideration of the Role of Dental Focal Infections and Seasonal Tides in Defensive Vitamins.” Dental Cosmos, 72:1049, 1119, October and November 1930.
- Idem: “Seasonal Variations in Butter-fat Vitamins and their Relation to Seasonal Morbidity, including Dental Caries and Disturbed Calcification.” Journ. A. D. A., 17: 550, May 1930.
- Idem: “Calcium Metabolism Studies on the Nature and Role of the Activators: Researches on Fundamentals for the Prevention of Dental Caries.” Journ. A. D. A., 16:265, February 1929.
- Idem: “New Light on Some Relationships between Soil Mineral Deficiencies, Low Vitamin Foods and Some Degenerative Diseases, including Dental Caries, with Practical Progress in Their Control.” March 1932; Indiana State Dental Bulletin, September 1932; Oral Health, August and September 1932.
- Klein and McCollum: Science, 74:662, December 25, 1932.
- Carr and Price: “Colour Reactions Attributed to Vitamin A.” Biochemical Journ., 20:497, 1926.
- Drummond, J. C., and T. P. Hilditor: The Relative Values of Cod-Liver Oils from Various Sources. December 1930, London, England.
- Yoder, J.: “Relation between Peroxidation and Antirachitic Vitamin.” Biological Chem., 70:297, October 1926.
- McGowan, J., and associates: “On the Fundamental Nature of Vitamin D Action.” Biochem. Journ., 25:1295, 1931.
- Price, Weston A.: “Calcium, Its Activation, Utilization and Metabolism.” Journ. of A. D. A., 15:601, April 1928.
- Idem: “Calcium Metabolism Studies. (A) The Raising of Serum Calcium by Topical Applications of Raw and Activated Cod-liver Oil. (B) Disturbances Associated with the Active Dental Caries of Childhood and Pregnancy.” Amer. Journ. Dis. of Children, 33:78, January 1927.
- Idem: “Some New Fundamentals for the Prevention of Dental Disease, with Special Consideration of Calcification and Decalcification Processes.” Dental Cosmos, 71:145, February 1929.
- Idem: “New Light on Some Relationships between Soil Mineral Deficiencies, Low Vitamin Foods and Some Degenerative Diseases, including Dental Caries, with Practical Progress in Their Control.” Oral Health, August and September 1932; Bulletin of Ind. State Dental Assn., September 1932.
- Forbes, J. C.: “Dental Caries from a Biochemical Standpoint.” Journ. of Dental Research, 11:591, August 1931.