
Access to all articles, new health classes, discounts in our store, and more!
The Concentration Factor in Local Anesthetic Solutions
Presented as part of the symposium, “Local Anesthesia,” at the Centennial Session, American Dental Association, New York, September 16, 1959. Published in Journal of Oral Surgery, Anesthesia and Hospital Dental Service, Vol. 18, pp. 275-290, July 1960.
* * *
An increase in the concentration of a local anesthetic drug or its accompanying vasoconstrictor up to a certain level will influence favorably the rate of onset, depth, spread, and duration of anesthesia. A given dose of drug is more effective in a smaller total volume of injected fluid.
Despite the numerous articles which have appeared in the literature regarding local anesthesia, relatively little consideration has been directed specifically to the problem of the concentration of the injected solution.
This report will attempt to review the available information on the subject of the concentration factor. The criteria for incorporation of material in this report include: (1) the data must deal specifically with the concentration factor, (2) the observations have been made on human subjects, and (3) the presented data are quantitatable.
In order to analyze the concentration factor, it is necessary first to review the conventional criteria used for the evaluation of local anesthetic agents.
Criteria for Acceptable Local Anesthesia
The two most important physiologic ingredients of local anesthetic agents are: (1) the local anesthetic solution itself, and (2) the vasoconstrictor substance.
Local Anesthetic Solutions–Sherman and co-workers,1 as well as other investigative groups, have outlined the criteria for an acceptable anesthetic solution. Eight specifications generally are listed. First, a local anesthetic agent must be as free as possible from toxicity. Second, the agent must be relatively free of properties which will irritate the tissues into which it is to be injected. Third, the material must possess a degree of stability necessary for storage. Fourth, the effects of an acceptable solution must be reversible so that physiologic sensation is restored within a reasonable interval of time after injection.
The remaining four criteria are of greater interest to the practitioner because: (1) they determine the course in clinical use, and (2) the clinician has more direct control over them. The first criterion, in this regard, is the induction time. With all other factors constant, it is highly desirable that anesthesia develop quickly. The second criterion is the depth of anesthesia. It is realized that desired depth will vary with the type of patient and nature of the operation. The third criterion is that an acceptable anesthetic solution must have a duration period that is satisfactory. Here again, different procedures for different operators make satisfactory duration different. The final criterion is that the ideal solution must be free of idiosyncratic effects.
Vasoconstrictor Agents–Criteria are also available for the ideal vasoconstrictor solution.2 Consideration is usually given to four items. First, the effect of the vasoconstrictor substance on duration of anesthesia; second, the vasoconstrictor substance should serve to minimize the toxicity of the local anesthetic solution; third, the potential hemostatic effect of a vasoconstrictor substance is judged; finally, systemic effects customarily are considered.
Analysis of Local Anesthetic Agents
An attempt will be made in this section to analyze the presently available data regarding local anesthetic solutions in terms of: (1) induction time, (2) depth of anesthesia, (3) extent (spread) of anesthetic effect, and (4) duration of anesthesia.
Induction Time–Huldt3 performed a series of experiments on 32 human subjects. One of the factors which he considered was the speed of onset of anesthesia (induction time). In all instances, the solution was injected supraperiosteally over the maxillary lateral incisor. Anesthesia was determined by the lack of response to a maximal electrical stimulus (Bjorn technic4). Figure 1 shows the results of his studies. It can be observed that, under conditions of constant volume (1 ml.) and constant vasoconstrictor (in every instance 1:40,000 epinephrine), the induction time decreased with an increase in the concentration of the local anesthetic solution. A ten minute latency can be observed with a 0.5 per cent procaine hydrochloride solution and an almost 50 per cent decrease in induction time when a 1 per cent procaine solution is injected. The curve begins to level off as the concentration is increased beyond 2 per cent. It is also interesting to note the shorter induction times with lidocaine (Xylocaine) as compared with procaine.
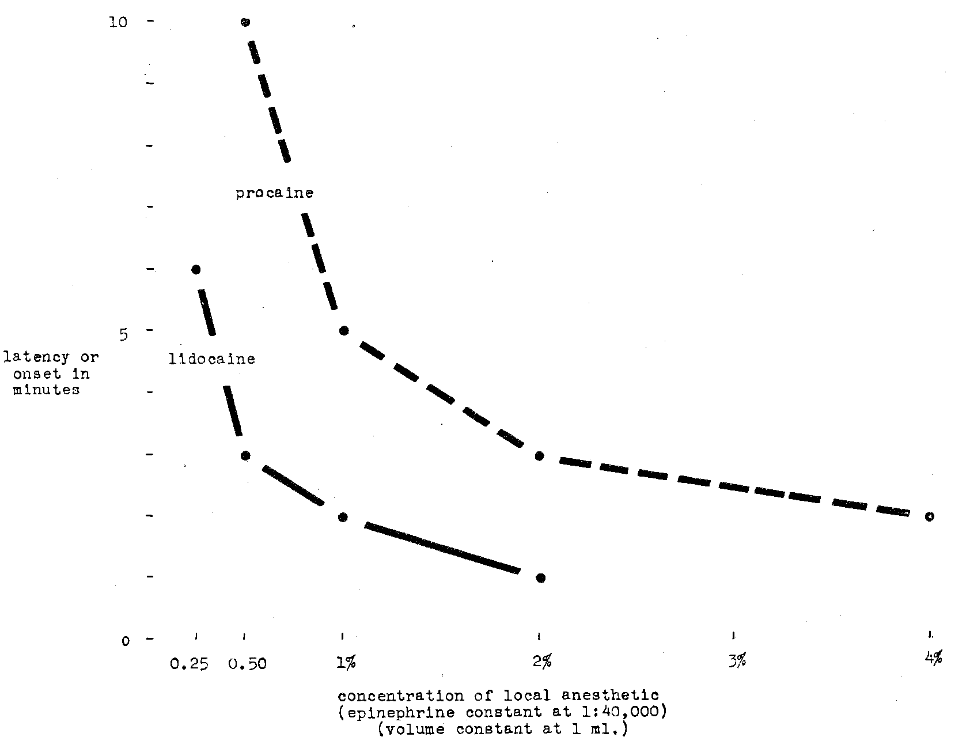
Fig. 1–Comparison of procaine hydrochloride and lidocaine hydrochloride in terms of latency or onset of anesthesia
Dobbs and co-workers5 compared 0.5 and 0.75 per cent propoxycaine (Ravocaine) with 1:30,000 levarterenol with respect to induction time. The time from the withdrawal of the needle until the patient perceived numbness in the anesthetized region was regarded as the induction time. The conclusion was drawn that the onset of anesthesia is much more rapid with the 0.75 per cent solution of propoxycaine as compared with the 0.5 per cent agent.
Depth of Anesthesia–Huldt, in the series of experiments previously quoted,3 also analyzed the depth of anesthesia. This was charted by recording the percentage of persons who did not respond to electrical stimulation.4 Figure 2 shows that increase in procaine concentration is associated with greater percentage of subjects with no response to electrical excitation. It appears, from this chart, that a limit is reached at 2 per cent and further increase in procaine concentration does not significantly alter the findings. It is noteworthy that concentrations of lidocaine, at lower than procaine concentrations, yield greater effectiveness (Fig. 2).
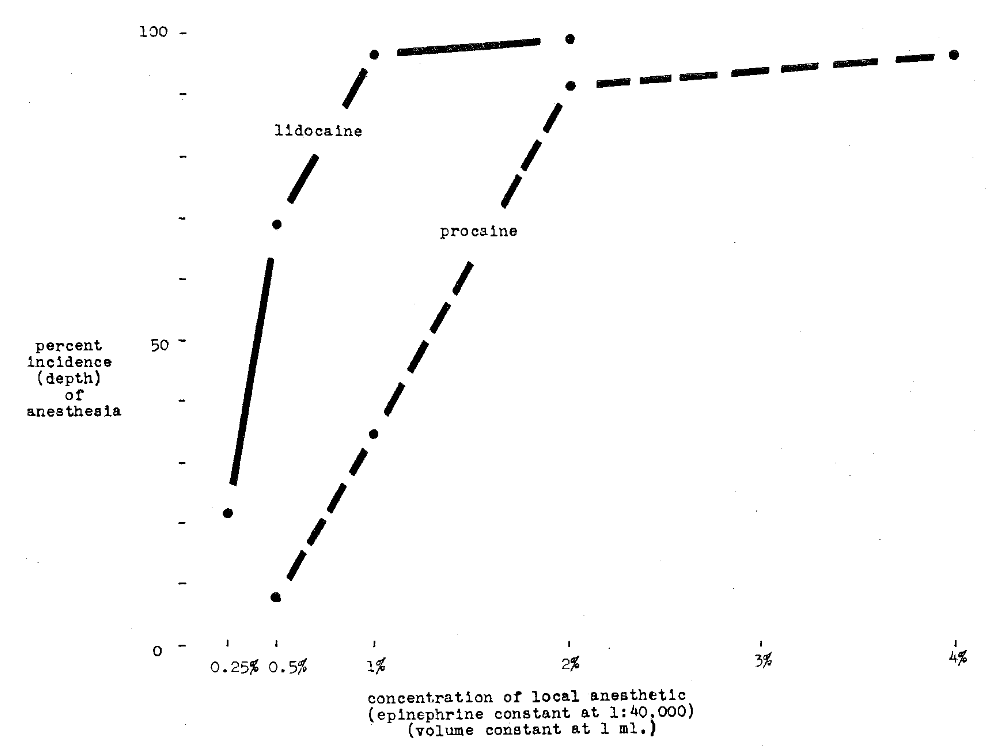
Fig. 2–Comparison of procaine hydrochloride and lidocaine hydrochloride in terms of per cent incidence (depth) of anesthesia
Huldt3 also studied the effect of total volume of solution on depth of anesthesia. It can be observed (Fig. 3) that the same amount of lidocaine (20 mg.) in decreasing total volume of injected fluid yielded greater anesthetic depth. This same relationship is underlined in other studies by the same author demonstrating that 4 per cent lidocaine (in 1 ml.) induced complete anesthesia in three out of every four subjects. In contrast, similar results were obtained in only 60 per cent of the patients with the same amount of lidocaine in greater volume (2 ml. 2 per cent).
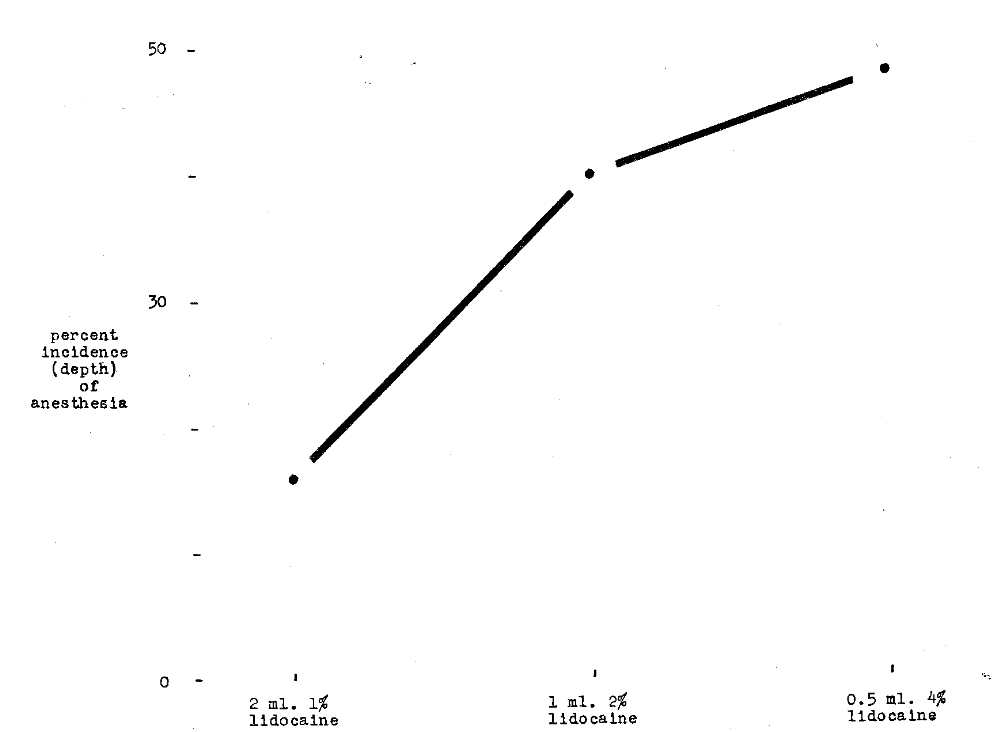
Fig. 3–Comparison of per cent incidence (depth) of anesthesia versus concentration of lidocaine hydrochloride when drug dose is constant at 20 mg.
Dobbs and co-workers5 compared propoxycaine 0.5 and 0.75 per cent with 1:30,000 levarterenol with respect to anesthetic depth. Anesthesia was graded as follows: (1) grade A indicated absolute freedom from pain during the operation, (2) grade B represented pain experienced during the operation but additional anesthetic solution was not needed, and (3) grade C designated pain experienced that required injection of more anesthetic solution. The conclusion was drawn that there is a slight advantage in the 0.75 per cent propoxycaine solution.
Extent of Anesthesia–The extent of local anesthesia is defined as the degree to which adjacent teeth show loss of sensation. In other words, the percentage of individuals with anesthesia about the central incisor and cuspid when local anesthetic solution is injected into the region of the lateral incisor has been utilized as an index of spread of the anesthetic effect.
Huldt3 investigated the spread of anesthesia after the injection of the substance in the region of the maxillary lateral incisor. Thirty-two subjects received 1 ml. of anesthetic solution with the same concentration of vasoconstrictor agent. Figure 4 shows that spread increases with increase in procaine concentration. Figure 4 also demonstrates the greater spread after the use of lidocaine.
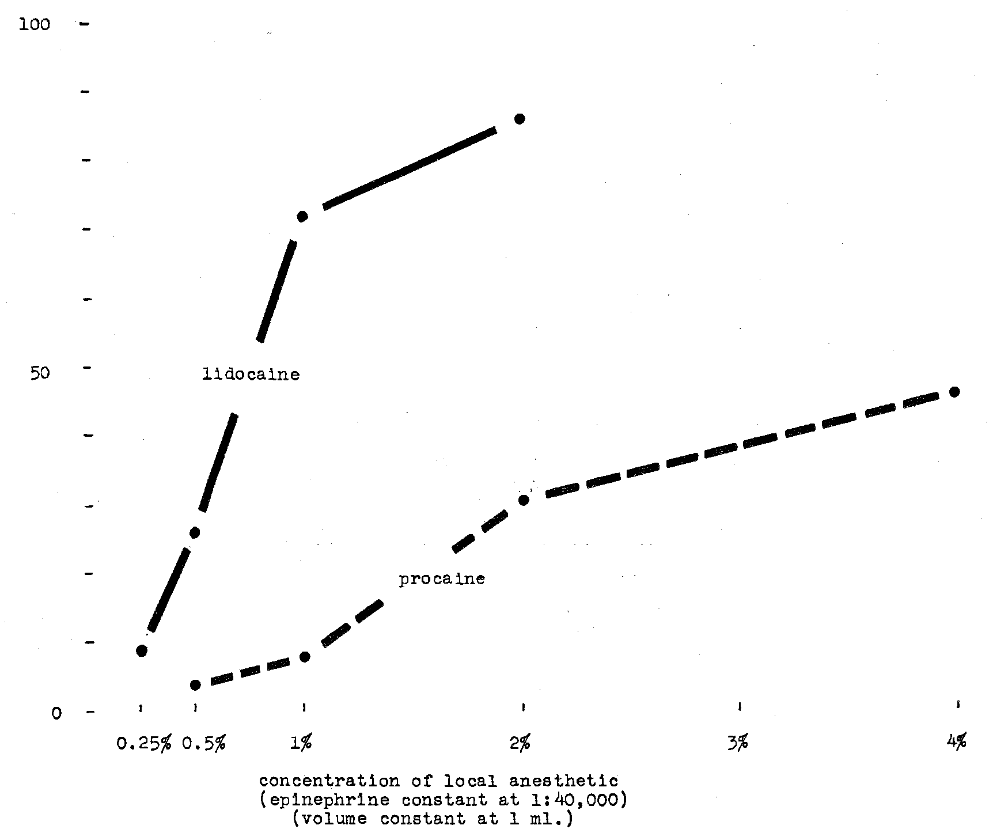
Fig. 4–Comparison of procaine hydrochloride and lidocaine hydrochloride in terms of per cent extent of anesthesia
Twenty-five subjects were injected with the same amount of vasoconstrictor-free lidocaine (20 mg.).3 It was found that anesthetic spread paralleled decrease in total volume of injected solution. This observation is consistent with conclusions previously drawn with regard to decreasing volume and anesthetic depth.
This same observation is, in part, confirmed in another experiment.3 Figure 5 shows there is greater spread with 1 ml. 2 per cent than with 2 ml. 1 per cent lidocaine.
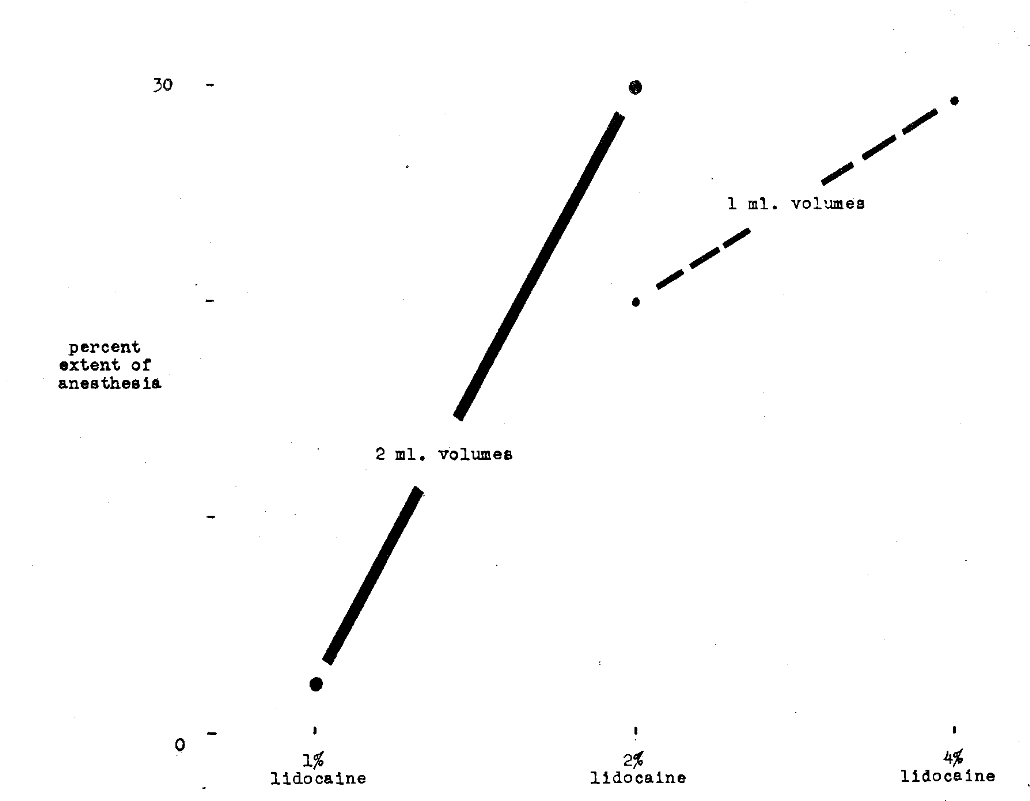
Fig. 5–Comparison of per cent incidence of anesthesia with I per cent, 2 per cent and 4 per cent lidocaine hydrochloride in varying volumes
Duration of Anesthesia–Huldt3 also studied the duration of local anesthesia after the supraperiosteal injection of substances over the maxillary lateral incisor. In one study of 32 subjects, the volume of solution was kept constant at 1 ml. and the epinephrine concentration was maintained at 1:40,000. Figure 6 shows duration increases with increase in concentration of local anesthetic agent.
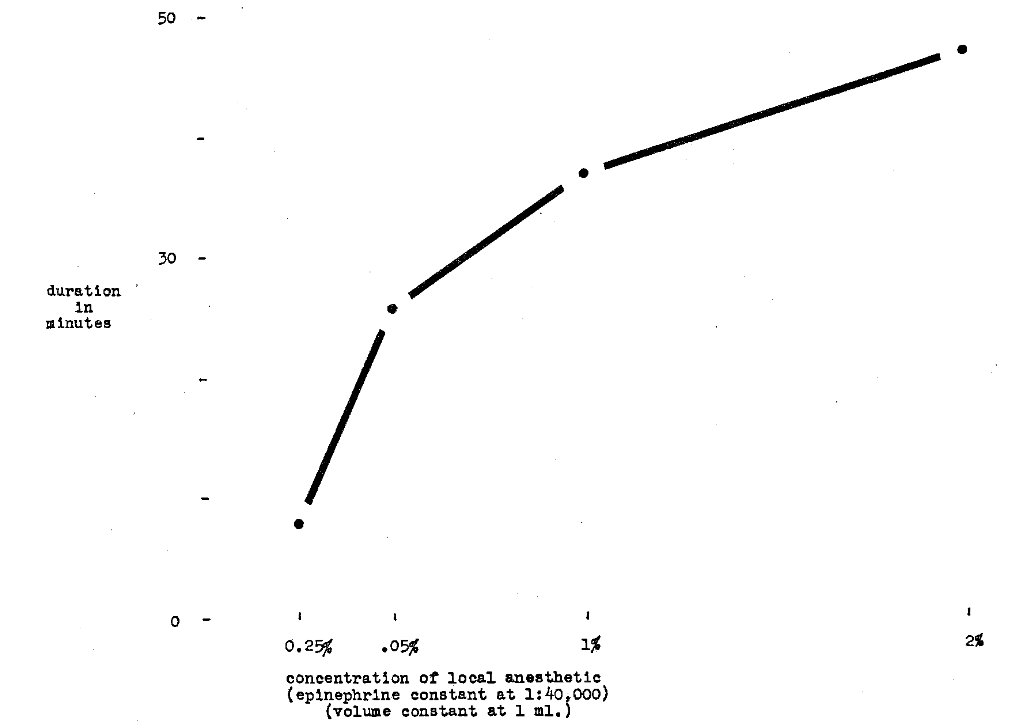
Fig. 6–Comparison of varying concentrations of lidocaine hydrochloride and duration of anesthesia
Dobbs and co-workers5 compared propoxycaine 0.5 and 0.75 per cent, both with levarterenol 1:30,000, with respect to duration of anesthesia and working time. The duration of anesthesia was the time from needle withdrawal until the last evidence of numbness vanished. Working time was considered to be the interval from withdrawal of the needle until pain caused by instrumentation returned or until operation was terminated. It was shown that the working time when 0.75 per cent propoxycaine was used was longer than that for the 0.5 per cent solution whereas there was only a small difference in the duration of anesthesia.
In a different series of 25 subjects3 injected with 20 mg. lidocaine in varying amounts of solution, it was found that there was little difference in duration after the injection of 2 ml. 1 per cent as against 1 ml. 2 per cent lidocaine. However, anesthetic duration was increased when 0.5 ml. 4 per cent solution was injected.
Finally, in another study,3 an attempt was made to analyze duration against volume of solution. It can be observed (Fig. 7) that 1 ml. 2 per cent is more effective than 2 ml. 1 per cent. However, these relationships do not obtain with the higher concentration solutions (that is, 1 ml. 4 per cent as against 2 ml. 2 per cent).
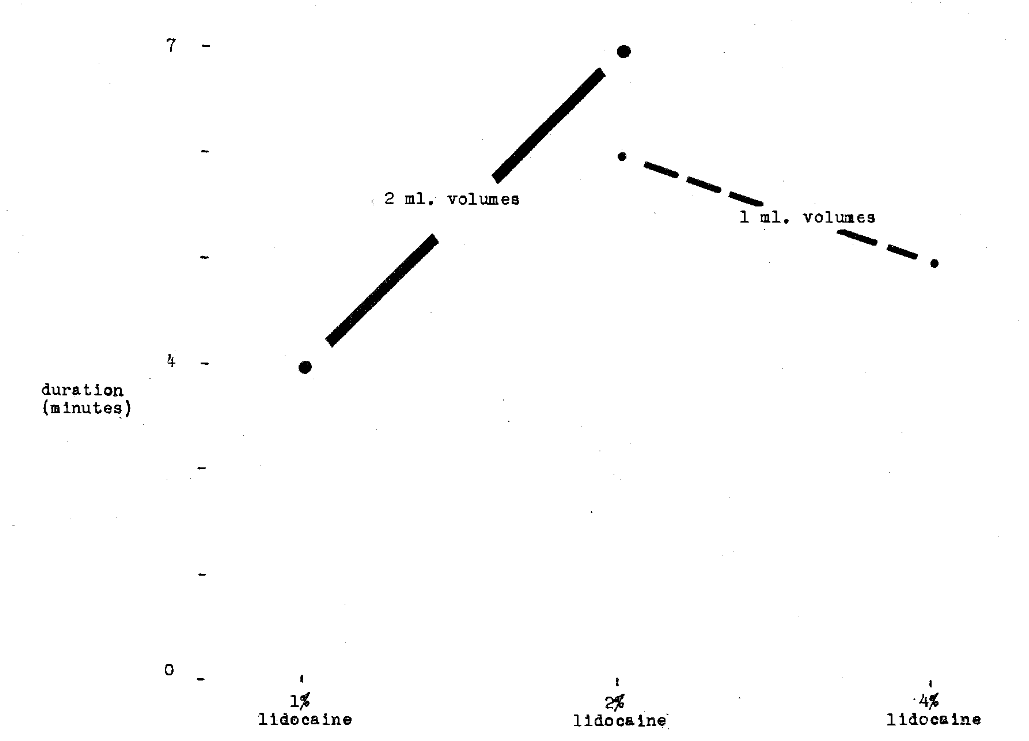
Fig. 7–Comparison of duration of anesthesia with 1 per cent, 2 per cent and 4 per cent lidocaine hydrochloride in varying volume
Analysis of Vasoconstrictor Agents
An attempt will be made in this section to analyze the presently available data regarding vasoconstrictor substances in terms of: (1) induction time, (2) anesthetic depth, (3) extent (spread) of anesthesia, (4) anesthetic duration, and (5) side-effects.
Induction Time–Kramer6 studied the speed of onset of anesthesia under conditions in which the concentration of the local anesthetic solution remained the same. Specifically, he compared 2 per cent lidocaine 1:50,000 epinephrine with lidocaine 1:100,000 epinephrine. He also investigated 1.5 per cent metabutoxycaine (Primacaine) with 1:60,000 epinephrine and with 1:125,000 epinephrine. The lack of response to the rotation of a bur in the dentin was used as the index of anesthetic efficiency. Figure 8 shows his findings. It appears, in the case of lidocaine, that greater amounts of epinephrine produce faster induction. However, the converse is shown with metabutoxycaine.
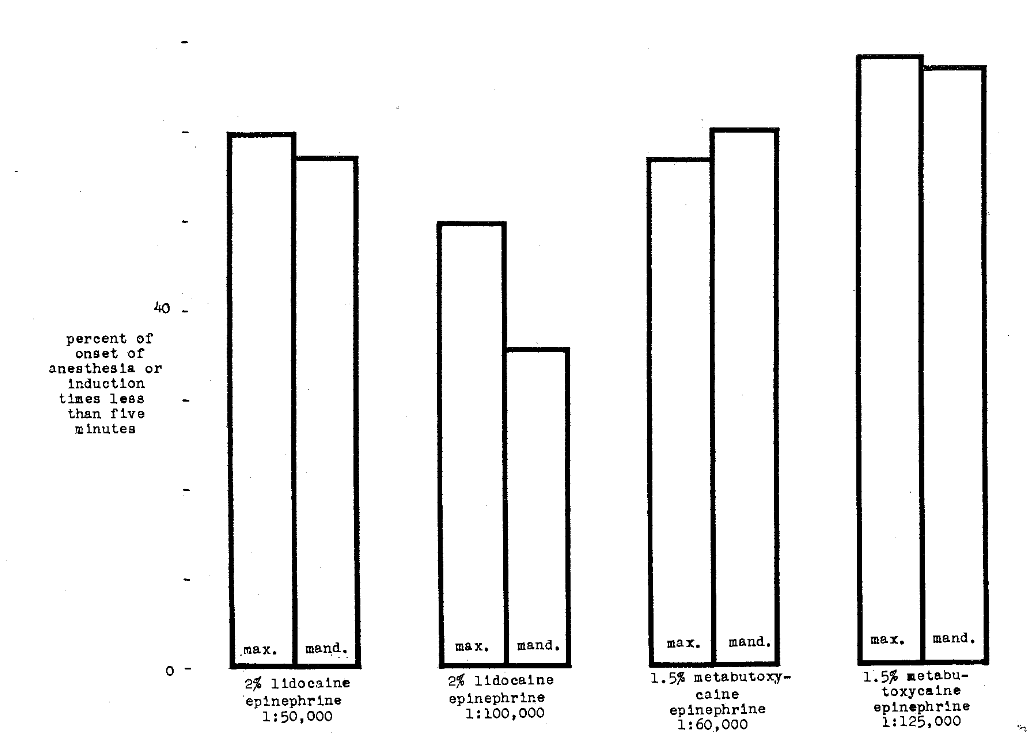
Fig. 8–Comparison of onset of anesthesia or induction time of lidocaine hydrochloride and metabutoxycaine hydrochloride with different concentrations of epinephrine
Costich7 studied the relative induction time of 2 per cent procaine and 2 per cent procaine with 1:50,000 epinephrine in a series of patients in whom inferior alveolar block anesthesia was utilized. He observed more rapid induction with the epinephrine-free anesthetic solution.
Depth of Anesthesia–Huldt3 studied the depth of anesthesia in 37 subjects after the supraperiosteal injection of a constant amount of lidocaine with different concentrations of epinephrine. Figure 9 shows the rapid increase in depth up to a point after which the curve levels off.
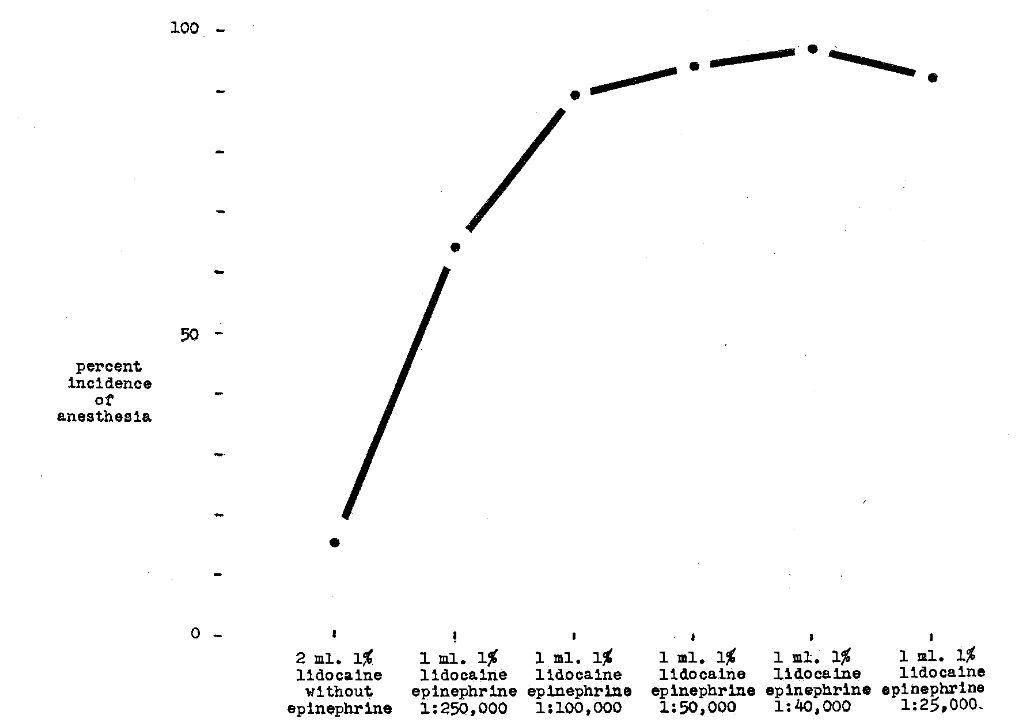
Fig. 9–Comparison of per cent incidence of anesthesia versus 1 per cent lidocaine hydrochloride with varying concentrations of epinephrine and without epinephrine
Huldt3 injected supraperiosteally 1 ml. 2 per cent procaine without epinephrine over the region of the maxillary lateral incisor in ten test subjects. In no instance was there an absence of response to a maximum electrical stimulus.4 This can be interpreted to mean that satisfactory anesthetic depth was not obtained. The solution, nevertheless, was not wholly without effect on the sensitivity of the teeth. A near maximum threshold value was obtained in two out of the ten subjects. The addition of epinephrine 1:40,000 to the same procaine solution resulted in a radical change in the activity of the anesthetic, giving a 78 per cent incidence of anesthesia.
Kramer6 compared the depth of anesthesia during the clinical use of 2 per cent lidocaine with 1:50,000 and with 1: 100,000 epinephrine. He also analyzed the relative effectiveness of 1:60,000 and 1: 125,000 epinephrine with 1.5 per cent metabutoxycaine. Depth was scored on a three-point system. Grade A consisted of complete elimination of pain. Grade B indicated pain but not sufficient to warrant reinjection. Finally, Grade C anesthesia was regarded as the type requiring additional local anesthesia. It appeared to him that depth was slightly greater when stronger epinephrine solutions were added to lidocaine. However, this relation was not observed in the metabutoxycaine experiments.
Harris and Worley8 compared 1.5 per cent metabutoxycaine 1:50,000 epinephrine as against 1:100,000 epinephrine. Infiltration injections were made with 0.5 cc. of the solution. The pain threshold was recorded as the mean quantity of electricity used to elicit pain when applied to a dental metallic occlusal (Class I) restoration. It appears from Figure 10 that anesthetic depth is slightly greater with the 1:50,000 epinephrine solution than with the 1:100,000 solution. Figure 11 shows the results of a similar study with 2 per cent lidocaine and 1:50,000 and 1:100,000 epinephrine. Once again, the more concentrated epinephrine solution produces greater depth.
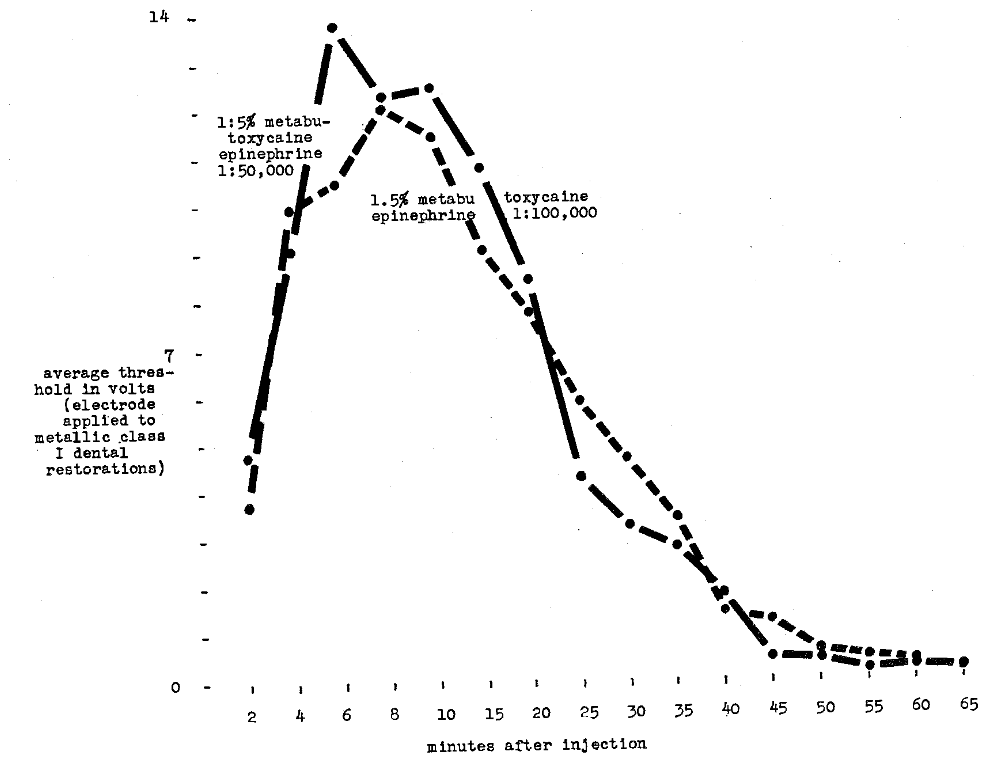
Fig. 10–Comparison of depth and duration of anesthesia using metabutoxycaine hydrochloride with epinephrine 1:50,000 and 1:100,000
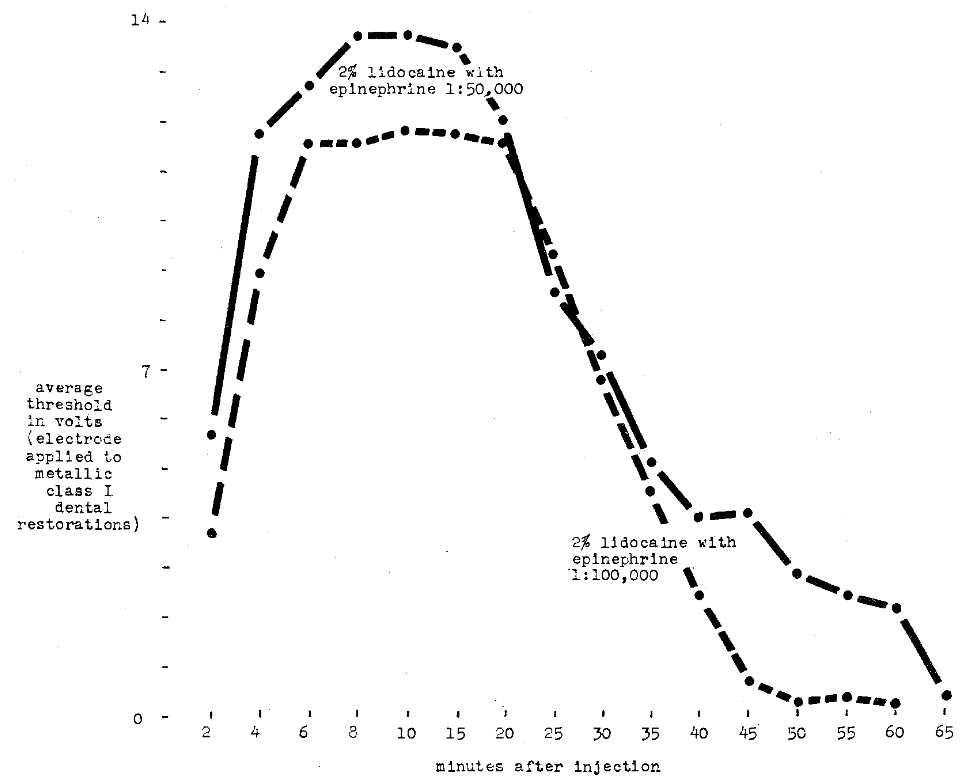
Fig. 11–Comparison of depth and duration of anesthesia using lidocaine hydrochloride with epinephrine 1:50,000 and 1:100,000
Extent of Anesthesia–Huldt3 studied the spread of anesthesia under conditions in which only the amount of epinephrine injected varied. It is clear from Figure 12 that spread increases with increase in epinephrine up to a point.
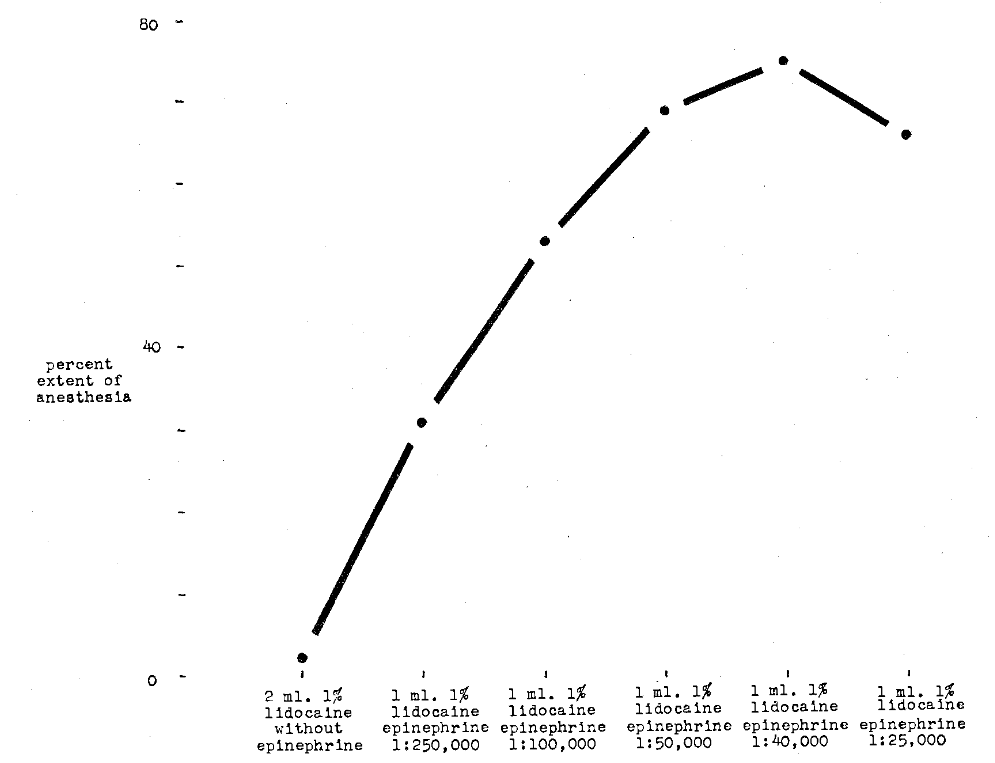
Fig. 12–Comparison of per cent extent of anesthesia versus concentration of epinephrine in a 1 per cent solution of lidocaine hydrochloride
Duration of Anesthesia–Huldt3 investigated length of anesthetic effect by maintaining a constant amount of lidocaine and varying the epinephrine concentration. Figure 13 emphasizes the point that duration increases with increase in epinephrine concentration.
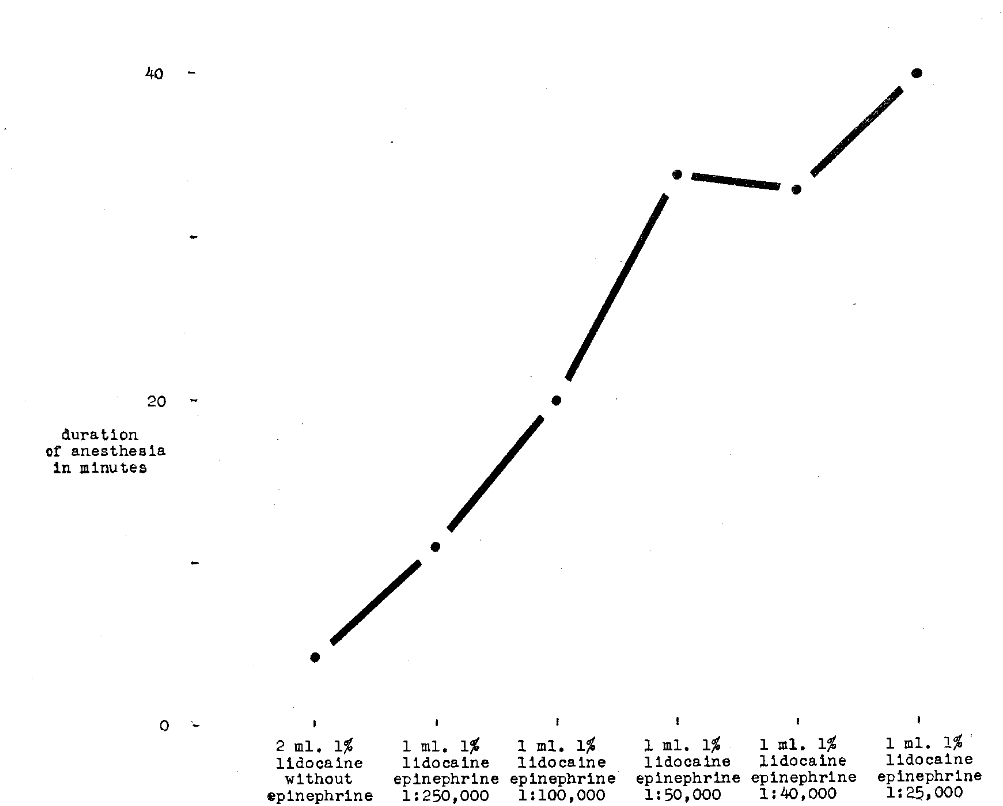
Fig. 13–Comparison of duration of anesthesia versus concentration of epinephrine in a 1 per cent solution of lidocaine hydrochloride
Huldt,3 using 1 ml. 2 per cent procaine without epinephrine in supraperiosteal injections over maxillary lateral incisors, failed to achieve anesthesia in any of ten test subjects. The addition of epinephrine 1:40,000 to the 2 per cent procaine solution resulted in an anesthesia duration averaging 25 minutes. Put more simply, this experiment suggests that adding a vasoconstrictor substance to a local anesthetic solution produces duration of anesthesia.
Costich7 studied duration of anesthesia in patients injected with 2 per cent procaine and 2 per cent procaine with 1: 50,000 epinephrine. He observed greater duration in the patients who received epinephrine.
Kramer6 investigated the duration of anesthesia after maxillary and mandibular injections with 1.5 per cent metabutoxycaine and 1:60,000 epinephrine and 1:125,000 epinephrine. He also studied the relative effect of 1:50,000 and 1:100,000 epinephrine with 2 per cent lidocaine. The evidence suggests little, if any, difference due to the additional epinephrine.
Harris and Worley8 (Fig. 10, 11) show only slight increase in duration with 1:50,000 epinephrine plus lidocaine over 1:100,000 epinephrine and lidocaine. No apparent difference can be observed in the metabutoxycaine series.
Side Effects–Costich7 analyzed the side effects encountered after the injection of 2 per cent procaine as against 2 per cent procaine with 1:50,000 epinephrine. He observed systemic reactions in 2.1 per cent of patients after epinephrine-free injections and side reactions in 15.3 per cent after the injection of procaine with epinephrine. Tremors were observed to be the most common side reaction.
Kramer,6 in comparing the incidence of untoward reactions (fainting, tremor, postoperative edema, nervousness, pain on injection, and headache) during clinical use of lidocaine 2 per cent with epinephrine 1:50,000 and with 1:100,000 and metabutoxycaine 1.5 per cent with epinephrine 1:60,000 and with 1:125,000 found that the solutions containing the more dilute concentrations of epinephrine produced no untoward reactions when used in maxillary injections. There was only a small percentage of side reactions when the more concentrated solutions of vasoconstrictors were employed in maxillary infiltrations. In the case of lidocaine used in mandibular blocks, there were fewer untoward symptoms with the use of epinephrine 1:50,000 than there were with the 1:100,000 solution. The converse was true of metabutoxycaine used in mandibular blocks; the more concentrated epinephrine solution produced a greater percentage of reactions than did the less concentrated solution.
Analysis of Combinations of Anesthetics and Vasoconstrictors
Thus far, consideration has been given to either the local anesthetic solution (with the vasoconstrictor substance constant) or the vasoconstrictor agent (with the local anesthetic substance constant). The evidence shows that each of these two ingredients plays a role in the onset, depth, spread, and duration of anesthesia. However, there is evidence to indicate that addition, antagonism, or synergism may also play a role. Accordingly, consideration will now be given to the studies which deal with combinations of local anesthetic and vasoconstrictor agents and their effect on:(1) depth, (2) extent, and (3) duration of anesthesia.
Depth of Anesthesia–Huldt3 investigated 37 subjects, each injected with 10 mg. lidocaine plus 20 micrograms epinephrine. The variable which was being studied was the total volume of the solution. Figure 14 shows that, as the volume of the solution decreases, the anesthetic depth increases.
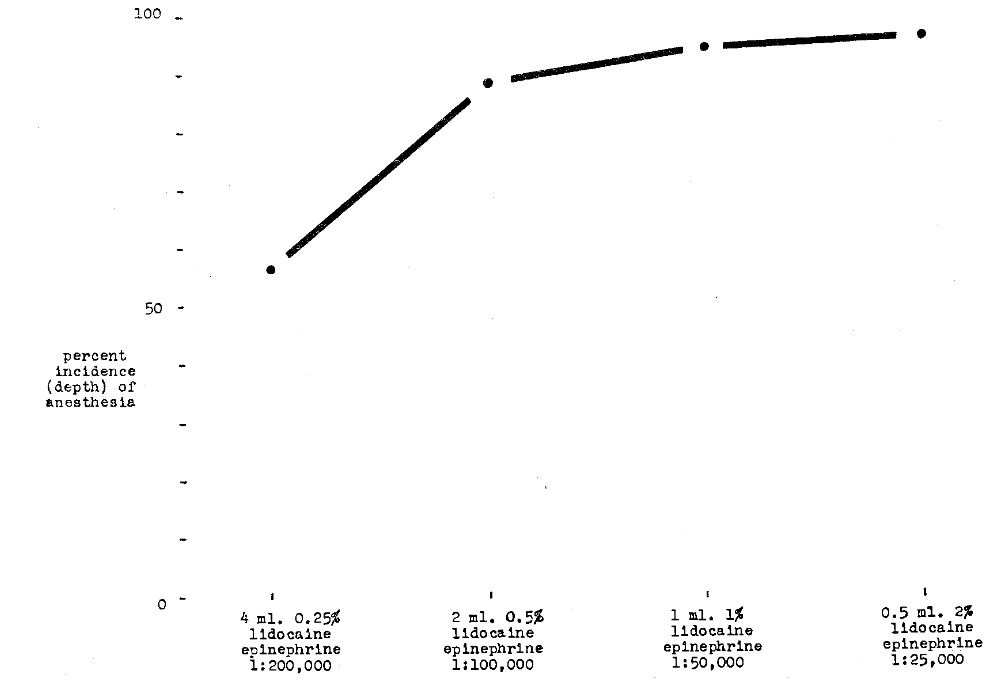
Fig. 14–Comparison of incidence (depth) of anesthesia with concentration of a total drug dose of 10 mg. of lidocaine hydrochloride and with 20 micrograms of epinephrine
Extent of Anesthesia–Huldt3 also analyzed the spread of anesthesia under the conditions just outlined. He observed that, with decrease in volume, there was increase in spread of anesthetic effect.
Duration of Anesthesia–Huldt3 also investigated duration of anesthesia. It can be seen (Fig. 15) that, as the total volume of injected solution decreases, the duration increases.
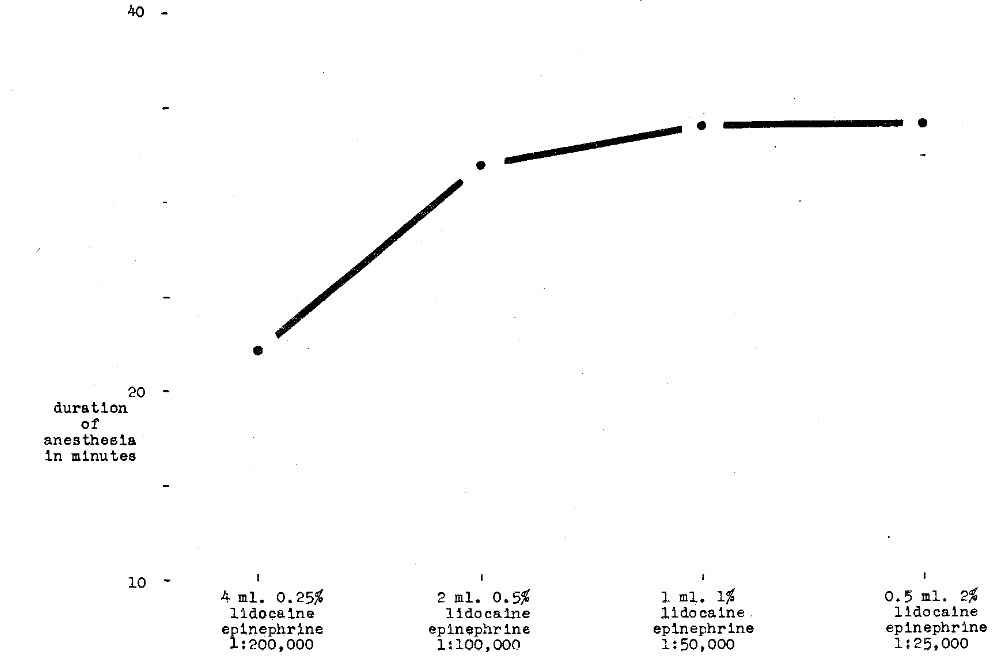
Fig. 15–Comparison of duration of anesthesia with concentration of total drug dose of 10 mg. of lidocaine hydrochloride and with 20 micrograms of epinephrine
Summary and Conclusions
An attempt has been made in this report to review the problems of concentrations of local anesthetic solutions and vasoconstrictor substances. Only studies dealing with human beings and those with quantitatable data have been included. The following conclusions are in order:
- The greater the concentration of local anesthetic solution, the more rapid the rate of the induction, the greater the depth of anesthesia, the more extensive the anesthetic spread, and the longer the anesthesia lasts.
- Induction time, depth, extent, and duration of anesthesia are enhanced the smaller the total volume of injected solution for a given drug dose.
- The greater the concentration of vasoconstrictor agent, the more rapid the rate of induction, the greater depth, spread, and duration of anesthetic effect.
- The evidence, though meager, suggests more side effects when epinephrine is added to a local anesthetic solution.
References Cited:
- Sherman, Harold; Fiasconara, J. E., and Grundfest, H. “Clinical efficiency of recent local anesthetics.” New York State D. J. 23:403 Nov. 1957.
- Rakower, W. “Value of having a vasoconstrictor in local anesthetic solutions.” D. Soc. Anesthes. Newsmonthly 4:15 Nov. 1957.
- Huldt, S. “Factors influencing efficiency of dental local anesthetics in man.” Acta Odont. Scandinavica 11: Suppl. 13, 1, 1953.
- Bjorn, H. “Electrical excitation of teeth and its application to dentistry.” Svensk Tandl. Tskr. 39: Suppl., 1946.
- Dobbs, E. C.; DeVier, C. W., Jr., and Rapoport, L. “A new local anesthetic agent.” A.D.A. 48:409 April 1954.
- Kramer, W. S. “Comparative clinical evaluation of some commonly used local anesthetic compounds.” A.D.A. 56:820 June 1958.
- Costich, E. R. “Study of inferior alveolar nerve block anesthesia in humans comparing 2.0 per cent procaine with 2.0 per cent procaine plus 1:50,000 epinephrine.” D. Res. 35:696 Oct. 1956.
- Harris, S. C., and Worley, R. C. “Comparative local anesthetic potencies of lidocaine and metabutoxycaine.” A.D.A. 57:66 July 1958.