
Access to all articles, new health classes, discounts in our store, and more!
The Biology of the Endodontic Patient: III. Variability in Periapical Healing and Blood Glucose
Published in Journal of Oral Medicine, Vol. 23, No. 3, pp. 87-90, July 1968.
* * *
Introduction
An initial report1 summarized the two-hour postprandial blood glucose values in a group of 55 routine endodontic patients. Four points warrant special mention. First, the blood glucose values ranged from a low of 72 to a high of 120 mg. per cent. Second, according to traditional standards, no one of the group was regarded as classically diabetic. Third, utilizing physiologic standards of 60 to 100 mg. per cent, 14.5 per cent of the subjects showed marginal hyperglycemia. Finally, with more restricted limits of 70 to 90 mg. per cent, 47.2 per cent of the group was viewed as being suggestively hyperglycemic. A second published report2 was designed to study relationships between the clinical causes for periapical pathosis and the two-hour postprandial blood glucose in the same sample of endodontic patients. The group with no apparent cause for periapical pathosis showed a significantly higher mean blood glucose than the groups with periapical pathosis apparently due to carious exposure or accidental trauma.
It is well established clinically that the response of the periapical lesion to routine endodontic therapy is quite variable. Specifically, in one subject following root canal therapy, the periapical lesion may vanish completely in a short period of time. In other cases, the periapical pathosis may disappear more slowly. Finally, in some instances, there is no resolution. This report is designed to cast additional light upon factors which might help explain the variable response to orthodox root canal treatment. Specifically, an attempt will be made to answer two questions:
- What is the usual periapical sequence of events following routine endodontic therapy?
- Can one explain the variability in response to such treatment on the basis of carbohydrate metabolism?
Method of Investigation
The 25 subjects selected for this project were routine dental patients at the University of Alabama School of Dentistry, Birmingham, Alabama. The age distribution is summarized in Table 1.
Table 1–age distribution
|
age groups |
number of subjects | percentage of subjects |
| 10-19
20-29 30-39 60-69 70-79 total |
9
10 4 1 1 25 |
36.0 40.0 16.0 4.0 4.0 100.0 |
The selection of teeth for this study was based on these six criteria: (1) the tooth must be an incisor or cuspid, (2) it must have a fully formed root apex, (3) the pulp canal must not have a direct or indirect opening to the oral cavity, (4) the tooth must not require a cast core during the course of this study. (5), the tooth must be in functional occlusion, and (6) there is roentgenographic evidence of periapical pathosis. An initial roentgenogram was taken at the first visit. A second film was made at a subsequent examination two weeks later. At this visit endodontic therapy was initiated. The root canal treatment regimen has previously been described.3 A third roentgenogram was taken (7 to 14 days later) at the time the root canal was filled. For six weeks thereafter, films were taken at two week intervals. Following the tenth week, they were taken at monthly intervals. The roentgenographic technique for measuring the size of the periapical lesion has been previously reported.3 The initial visit findings are summarized in Table 2. For the total group, the mean and standard deviation was 31.1 ± 19.2 sq. mm. Thus, 68 per cent of the periapical lesions ranged from a low of 11.9 to a high of 40.3 sq. mm.
Table 2–frequency distribution of size of periapical lesion
|
periapical lesion size (sq. mm.) |
70-89 mg. per cent blood glucose | 90-110 mg. per cent blood glucose | total group |
| 0- 9
10-19 20-29 30-39 40-49 50-59 60-69 80-89 totals means standard deviation |
1
1 5 2 3 1 0 0 13 31.1 13.4 |
2
3 2 1 1 1 1 1 12 31.2 24.6 |
3 4 7 3 4 2 1 1 25 31.1 19.2 |
Results
Question One: To resolve the first question, the mean size for the periapical lesion was calculated for the 25 subjects at each visit. Figure 1 pictorially portrays the results. It is clear that, with time (shown on the abscissa), mean periapical size decreased. For the entire group, the lesion was approximately halved (56 per cent reduction) in thirty weeks. Thus, in answer to the first question and consistent with clinical experience, the periapical lesion slowly decreases following routine endodontic therapy.
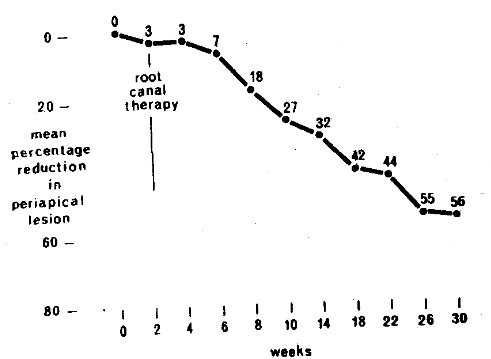
Fig. 1.
Question Two: In order to determine factors which may help explain the variability in response to root canal therapy, the 25 subjects were divided into two near-equal subgroups. The division was based upon two-hour postprandial blood glucose levels. Thus, there were 13 subjects with blood glucose in the 70-89 mg. per cent range and 12 with values of 90-110 mg. per cent. The mean periapical lesion size for the two groups (Table 2) was very similar at the initial examination (31.1 and 31.2 sq. mm.).
Figure 2 graphically depicts the results following endodontic therapy in the two glucose groupings. During the first ten weeks the periapical lesion decrement was very similar in both groups. After that point, however, the groups diverged. At 30 weeks, a 74 per cent reduction had occurred in the lower blood glucose group (70-89 mg. per cent). In contrast, the lesion decrement was only 48 per cent in those with the higher blood glucose (90-110 mg. per cent). Thus, in answer to the second question, carbohydrate metabolism (as measured by two-hour postprandial blood glucose) appears to be a predictor of the periapical course of events following routine endodontic therapy.
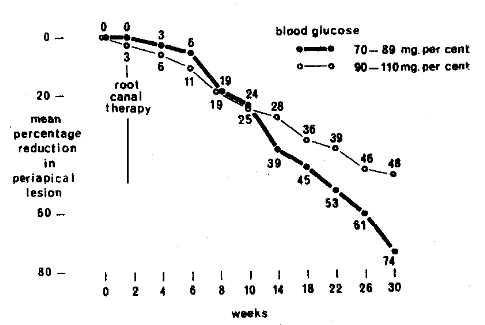
Fig. 2.
Discussion
It is a well known clinical fact that periapical pathosis usually disappears following root canal therapy. The evidence presented here (Figure 1) in 25 subjects supports the clinical experience. It is also clinically well established that considerable variability in periapical response occurs even in similar cases treated similarly by the same operator. Within the limits of this preliminary investigation, the resolution is, in part, predictive when viewed in terms of carbohydrate metabolism. This is not to imply that disturbances in carbohydrate metabolism are necessarily the cause of the variability. On the other hand, aberrations in carbohydrate metabolism cannot be excluded from the etiologic constellation since host resistance is obviously impaired in classically diabetic individuals. The detrimental effect of this metabolic flaw upon the periodontium has been repeatedly substantiated.4-9
Summary
- Twenty-five subjects participated in a study of periapical lesion resolution following routine root canal therapy.
- The evidence supports the time-tested conclusion that periapical lesion size diminishes following endodontic treatment.
- The variability in periapical resolution parallels the two-hour postprandial blood glucose. Specifically, the subjects (n = 13) with the lower blood glucose showed greater lesion reduction than those (n = 12) with the higher blood glucose values.
- The question logically arises as to whether blood glucose is a specific reflection of host resistance in the endodontic subject. In order to resolve this question, a report to follow will analyze the variability in periapical response following endodontic treatment in the light of another biochemical parameter.
The authors gratefully acknowledge the assistance of Dr. Thomas A. Masters, who performed the root canal therapy and measured the periapical lesions. Also, our gratitude to Dr. J. B. Freedland for his counsel and assistance in the preparation of this report.
References Cited:
- Cheraskin, E. and Ringsdorf, W. M., Jr. “The biology of the endodontic patient: I. Two-hour postprandial blood glucose frequency distribution.” (submitted for publication)
- Cheraskin, E. and Ringsdorf, W. M., Jr. “The biology of the endodontic patient: II. Causes of periapical pathosis and two-hour postprandial blood glucose.” (submitted for publication)
- Masters, T. A. “The effect of a preparation of multivitamins and trace minerals upon periapical healing; a thesis.” 1967. University, Alabama.
- Stahl, S. S., Witkin, G. J., and Scopp, I. W. “Degenerative vascular changes observed in selected gingival specimens.” Oral Surg., Oral Med., and Oral Path. 15: #12, 1495-1503, December 1972.
- Camerini-Davalos, R., Caulfield, J. B., Rees, S. B., Lonzano-Castaneda, O., Naldjian, S., and Marble, A. “Preliminary observations on subjects with prediabetes.” Diabetes 12: #6, 508-518, November-December 1963.
- Belting, C. M. Hiniker, J. J., and Dummett, C. O. “Influence of diabetes mellitus on the severity of periodontal disease.” Periodont. 35: #4, 476-480, November-December 1964.
- McMullen, J. A. Legg M., Gottsegen, R., and Camerini-Davalos, R. “Microangiopathy within the gingival tissues of diabetic subjects with special reference to the prediabetic state.” Periodontics 5: #2, 61-69, March-April 1967.
- Campbell, M. J. A. “Periodontal disease in the diabetic patient and its treatment.” Dent. J. 12: #2, 117-122, April 1967.
- Finestone, A. J. and Boorujy, S. R. “Diabetes mellitus and periodontal disease.” Diabetes 16:.#5, 336-340, May 1967.