
Access to all articles, new health classes, discounts in our store, and more!
Resolved: That a Clean Tooth Does not Decay and That Mouth Cleanliness Affords the Best Known Protection Against Dental Caries (Negative Doctor Weston A. Price)
Report of a debate held in the Grand Ballroom of the Pennsylvania Hotel, New York city, March 27, 1934. Published in Dental Cosmos, Vol. 76, August 1934.
* * *
AFFIRMATIVE
Thaddeus P. Hyatt, D.D.S., F.A.C.D., Assistant Medical Director, Metropolitan Life Insurance Co., New York, N. Y.
In our approach to an elucidation and a better understanding of the problem of dental caries and what are the best known measures for its prevention, certain facts are presented and, being axiomatic in principle, they cannot be excluded or ignored in any discussion or debate on the resolution presented this evening.
Dental caries is a chemico-vital process of destruction of the hard structures of the tooth carried on through the agency of acid-producing bacteria.1
The first fact which we shall present, and which you are requested to constantly keep in mind, is the fact that dental caries starts on the outside of the tooth, and not on the inside. In olden times the theory was that decay started on the inside of the tooth, but Dr. W. D. Miller pointed out “that teeth from which the pulps have been removed which are mounted on pivots or worn on plates are subject to decay the same as teeth with vital pulps, and when decayed, they show the same microscopic changes in the structure.”2
Dr. K. H. Thoma of the Dental School, Harvard University, after having conducted some research work on dental caries, writes as follows: “Histopathological study of dental caries in human teeth shows it is the first state of an infectious process starting at the exposed surface of the tooth.”3
After several years of research work on dental caries, carried on by Dr. H. E. Friesell, dean of the Dental College, University of Pittsburgh, and the Mellon Institute of the same university, Dr. Friesell makes the following statement: “When caries attacks a tooth, it does not affect the tooth uniformly all over its exposed surface.”4
Dr. G. V. Black and Dr. J. Leon Williams have shown by the most careful microscopic investigations that dental caries starts on the outside of the tooth.
The second fact which we wish to present tonight is one that is accepted by all investigators of dental caries, that bacteria are always present; in fact, if there are no bacteria we do not have decay. Tonight we are not concerned with what particular brand, stripe or style of bacteria they are. They may be the old-fashioned kind or the more modern varieties, such as the Bacillus acidophilus, and others. Just so long as they really are bacteria and they really can produce acids, and that they really can be trapped and, in fact, are trapped and held in close contact with the tooth, this is all that is needed to show why decay starts at that place.
When these traps or little garbage pails filled with bacteria and fermenting food debris are not present, we do not find dental caries.
To return to the research work of the Mellon Institute and the School of Dentistry of the University of Pittsburgh, Dr. Friesell states that decay “begins at points so definite on the various anatomical surfaces of the tooth that an experienced operator can readily predict where decay will begin on a given surface, and to what limits it will extend on that surface.” We would also add that any senior or junior student in any dental college can also point out on a given surface where decay will start.
Not only do we know where decay will start but we also know where decay does not start.
Dr. William Robertson, as far back as 1835, wrote that decay never occurs on clean surfaces. And seventy-four years later Dr. G. V. Black stated: “Caries never attacks the enamel in the open where the surface is freely cleaned.”5 Those parts of the tooth’s surfaces are easy to keep clean, and it being known that no decay ever starts in these places, is the reason why they are referred to as being immune. This fact is so generally accepted that when Dr. Black advocated “extension for prevention” every one saw the logic of it, and it is now taught in all colleges. In other words, when it becomes necessary to fill a tooth, we should extend the filling into these immune areas because, these places being clean, decay will not occur around the fillings.
The outstanding and distinguishing feature of these parts of the tooth where caries never starts is the interesting and very significant fact that they have no defects or tiny openings in the enamel impossible to keep clean.
Can the free acids of the mouth cause caries? In the words of Dr. Black: “It is well demonstrated that the whole saliva never becomes sufficiently acid to act on the teeth and that so long as microorganisms have no protection from the dissipation of the acids they form they cannot produce caries.”6 And this is what also happens with the free bacteria of the mouth; having no protection against the dilution of the acids they produce, their free presence in the mouth does not produce decay. Therefore the free acids and the free bacteria of the month do not start caries.
If the saliva could be sufficiently acid to act on the teeth, we should find a uniform breaking down of all surfaces of all the teeth. This we know does not take place. We have shown that there are well known parts of the teeth’s surfaces which, because they are kept clean, are free from decay.
As every medal has two sides, the obverse and the reverse, let us now present the facts which explain why some parts of the tooth are favorable for the starting of decay and what are the distinguishing and characteristic features of those parts which students of dental caries can so easily point out.
Dr. Robert Arthur writes: “Whatever may be the source of the agent causing decay, the disorder is always observed to commence at points which favor the lodgment and retention of particles of food. Wherever, therefore, a defect in the continuity of the enamel of a tooth exists, decay is sure to occur.”7
Dr. C. N. Johnson writes that enamel defects provide “A leak for the ingress of foreign matter.”8
Dr. McQuillen writes that defective formation of the tooth presents conditions favorable for the retention of fluids and semi solids which undergo decomposition.
Defects, or flaws in the formation of the tooth during the process of growth, are breaks or openings in the surface of the tooth. These flaws or openings do not occur very frequently in the lingual surfaces of the lower front teeth, facing the tongue. We examined over 198,000 lower front teeth before we found the first enamel defect, and in this small and uncleanable opening decay had started.
Drs. J. Leon Williams and G. V. Black have shown that the bacteria must be attached to the enamel in such a way as to prevent the acid produced by the bacteria being washed away or from being diluted by the fluids of the mouth.
If we study the shape and formation of the teeth, we find certain definite places so located that they are difficult to keep clean, while other places are so shaped that it is impossible by any kind of mouth toilet to keep them clean and free from food debris and bacteria. The difficult places to keep clean are the proximal surfaces, and the places impossible for the owner to keep clean are these small openings or defects. These small openings called pits and fissures are the traps in which are caught those essential factors without which dental caries will not start. Dr. A. E. Webster of Toronto, Ontario, Canada, writes: “If it were not for pits and fissures, caries would rarely occur.”
These defects are insurmountable hindrances to the patient in keeping his teeth clean. Drs. Phillip Jay and Ralph Voorhees of the Department of Research, University of Rochester, New York, write: “The old slogan that a clean tooth never decays has been universally challenged as false. We doubt very much that an acidophilus-free tooth will decay.”9
Dr. S. F. Gottlich of Amsterdam, Holland, writes: “From whatever point of view, however, we may consider the problem of dental caries, still the direct causative agent remains fermentation of carbohydrates, originating from food debris lodging around the teeth”; accordingly the proverb, also gradually becoming in vogue in Europe, in this conception finds its support that “A clean tooth does not decay.”10
In conclusion, we claim that there are certain factors that are essential and necessary for the starting of dental caries, and they are (1) acid-producing bacteria; (2) conditions which make possible the undisturbable retention of these bacteria and food debris next to the tooth for a definite time; (3) the acid produced by these bacteria to be protected, so that the acid concentration or strength cannot be diluted by the fluids of the mouth.
And we also claim that any tooth that provides all these conditions is not and cannot be a clean tooth; furthermore, any tooth that does not provide these conditions is a clean tooth and does not decay.
References Cited:
- Anthony’s Dental Dictionary.
- McKay, F. S.: Journ. A. D. A., 21:420, March 1934.
- Journ. of Dental Research, 13:251, June 1933.
- “Studies of the Cause and Nature of Dental Caries.” Journ. Dental Research, 12: 759, October 1932.
- Dental Cosmos, 51:1390, December 1909.
- Idem: 41:828, September 1899.
- Arthur, Robert: Prevention of Decay of the Teeth.
- Dental Cosmos, 41:7, January 1899.
- Text-Book of Operative Dentistry.
- Tijdschrift voor Tandheelkunde, p. 683, July 1929.
AFFIRMATIVE
Alfred Walker, D.D.S., F.A.C.D., New York, N.Y.
In presenting my argument for the affirmative of this question, I shall not enter into any hair-splitting or equivocation. The title is clear-cut and concise. It is not our intention, nor do we expect to solve the problem of the cause and prevention of tooth decay tonight, but we do hope to relieve, in a measure at least, a confused public mind as to what may be the best means for protecting the teeth against caries.
It is agreed from the outset that all of those participating in this debate are sincerely desirous of promoting methods or procedures that will best accomplish the prevention of this, the most prevalent of all human diseases.
Frankly, I know of no means for absolutely preventing dental decay, but I propose to show that a clean tooth does not decay, and that the maintenance of tooth cleanliness provides the best known protection.
By a clean tooth, I do not mean a surgically clean tooth, but one having on all its surfaces that degree of cleanliness which with no extreme effort we are able to maintain on the surfaces that are easily accessible to the cleaning processes. By best known protection against dental caries we mean a method of protection available, applicable and acceptable to the masses of the civilized people.
The arguments which I shall present are based upon the results of many years of observation and study among people of all the social levels, at all ages and of many different nationalities. They include those seen in private practice, in institutions and in clinics, the healthy as well as the sickly. I shall present facts only, and since there is to be no formal decision, the audience will have to draw its own conclusions and make its own decision.
It is well known to every dentist that decay of the teeth always begins in certain places and under certain conditions. Dr. Hyatt, who preceded me, has given you some historical data and has presented irrefutable evidence of the prevalence of decay on the occlusal or grinding surfaces of the molars and bicuspids. He has shown you that, due to their form, certain places on these surfaces are not easily kept clean; that it is in these places that decay occurs and that it never occurs on those areas which are accessible to cleansing influences which the mastication of food or other mechanical methods provide. As further support for the affirmative I shall present some facts concerning other surfaces of the teeth.
Grossly, every tooth has five surfaces. Dr. Hyatt has discussed the occlusal or grinding surfaces. The remaining four are, one, the surface toward the tongue; two, the surface toward the lips or cheek, and the two surfaces which face the adjoining teeth on each side.
It is a well-known fact that in the absence of some fault, the surface of the tooth which faces the tongue and the surface which faces the cheek or lips do not decay. To be sure, there are exceptions to this rule, but they are comparatively rare. If you will observe your own teeth you will quickly verify this statement.
The reason for the immunity of these surfaces is very plain. They are normally continuously smooth and are easily accessible to the natural and artificial cleansing processes. Not so, however, with those two surfaces which face the adjoining teeth on each side, for here we find that dental decay is rampant. The reason for this is just as easily explained.
Normally, these surfaces are in contact with each other and, in consequence, the areas near where the teeth touch provide a trap for food which resists cleansing processes. By cleansing processes we do not refer to toothbrushing alone, but also to what Enright and Friesell have referred to as the scouring action which the chewing of food provides.
It is true that these in-between surfaces differ somewhat in shape from the other surfaces, but this fact does not account for their susceptibility to decay. This is proved by the following rather frequently observed condition. As you know, teeth do not always come through the gum in regular and normal alignment. Instead of arranging themselves in even and regular relationships, they will be more or less out of line, thus sending a crooked or irregular appearance. Quite frequently they will be turned around or rotated. For example, the side of the tooth that should be facing the adjoining tooth will face the cheek or tongue, depending upon the direction in which it is rotated. When this happens we find that the side of the tooth which should face the tongue and the side which should face the lips or cheek–which if they were in those respective positions would not decay, because they could be kept clean–are now facing the adjoining teeth and are therefore difficult or almost impossible to keep clean, and, if not already involved, will sooner or later succumb to the ravages of caries.
These facts prove quite definitely that even if the tooth surfaces are continuously smooth they offer no protection against decay if their positions and relationships to the other teeth interfere with cleansing processes.
These observations are quite in keeping with what has been said of the irregular or grinding surfaces.
As further evidence of the value and importance of maintaining tooth cleanliness, we note the fact that tooth decay does not start on the inside of the tooth but that it does start on the outside. If this were not true, the filling of teeth would prove of no avail, because if decay started from the inside, the process of decay would go right on under the filling. Every dentist knows that a well-executed filling operation definitely safeguards the filled area of the tooth. We know also that in the days before porcelain artificial teeth were made, natural extracted teeth were used on plates as substitutes for lost teeth. These natural teeth, which were completely detached from any circulatory influence from within, decayed just as did the individual’s own teeth.
One of the arguments most frequently used as controverting the statement that a clean tooth does not decay is that caries-free teeth are seen in the most filthy mouths. This argument is not only fundamentally weak and illogical, but it is analogous to the deceptive belief that the unclean often escape contracting filth disease, consequently body hygiene is ineffective and therefore unnecessary.
If it be true that a clean tooth does not decay, and if it be true that tooth decay begins on the exposed surfaces of the teeth–more specifically those surfaces not accessible to the cleansing processes–it logically follows that mouth cleanliness affords the best protection.
It is not my contention that teeth can be kept clean only by the toothbrush and the dentifrice. I stated before that the chewing of food had a scouring effect upon certain surfaces of the teeth, but that others, such as the in-between surfaces, were not exposed to these scouring influences. It is not at all impossible that the immunity to decay of the six lower front teeth may offer a clue as to how these in-between surfaces may be protected.
It is a matter of everyday observation that an individual may have almost every other tooth involved in decay and show a complete absence of any such involvement in his six lower front teeth. This immunity is so common that I dare say few in this audience have any cavities in these teeth. When these teeth do become decayed it is a certain index of an extensive, and frequently a hopeless, involvement of all of the other teeth. What is it that provides this immunity? If it is a nutritional factor conveyed through the internal circulation of the tooth, why does not the same influence affect the other teeth?
Reasoning from every angle, we cannot escape the conviction that the influence is environmental rather than a resisting factor within the tooth. These teeth are of the same substance as are the other teeth; they are surrounded by the same structure; their form is essentially the same; somewhat different, to be sure, but not sufficient to justify the deduction that the tooth form provides the immunity.
When these teeth do decay, it is always on the in-between surfaces and not on the easily cleaned areas.
I do not question the importance of nutrition as a preventive or arresting agent in dental decay, but I am convinced that its influence must be exerted first during the period of tooth development, and that any subsequent immunizing factor will be concerned with environmental conditions.
That dental decay may persist in spite of our best efforts toward oral hygiene does not disprove our claim, but it is an admission that we have thus far been unable to attain the degree of cleanliness necessary to tooth protection.
When we review the history of the search for the cause of dental decay, we cannot escape the thought that, in some respects at least, it is similar to the search for the cause of cancer–both admittedly complex problems. You will recall that at various times diet has been brought forth as a causative factor in cancer, and who knows but that it may yet be shown to bear an important relationship?
In this connection and as a conclusion to my part in the debate, I quote from the New York Times of February 20, 1934. In an editorial on that date, commenting on the work at the Memorial Hospital in this city, which, as you know, is one of the leading cancer research institutions in the world, the Times says:
“Dr. James Ewing, the president of the medical board of the hospital, sums up his general preventive advice in two very simple, easily adopted recommendations:
First, habits of moderation in eating, drinking and smoking; and
Second, the liberal use of soap and water on the skin and in all accessible cavities of the body.”
This sound advice of Dr. Ewing applies equally well to the problem of the prevention of dental decay.
In summarizing this necessarily brief presentation, I desire to impress upon you that:
- Immunity to dental caries in civilized peoples is rare indeed.
- That individuals who habitually disregard prescribed diets are frequently caries-free to a high degree.
- That, on the other hand, individuals who faithfully follow prescribed diets frequently show a high degree of susceptibility.
- That members of the same household on identical diets will show wide variation to susceptibility and immunity.
- That the belief that isolated groups owe their immunity to dental caries to diet alone is an opinion not supported by proof. There are other factors that must be taken into account.
- That such authorities in the nutritional field as Hess, Bunting, Eddy and others have recently admitted that the problem was still unsolved.
- That clinical observers support this view and that until a proved dietary formula is available, the best protection against dental caries is mouth cleanliness.
AFFIRMATIVE
Maurice William, D.D.S., F.A.C.D., New York, N.Y.
As the last speaker for the affirmative, my task has been greatly simplified by my colleagues who preceded me. I am convinced that this intelligent audience has been convinced that “a clean tooth does not decay.” More than that; I am convinced that the distinguished gentlemen who undertook to defend the negative are now convinced that “a clean tooth does not decay.” And what may seem still more surprising, I am convinced and my colleagues are convinced that a “clean tooth does not decay.” I submit that, when the affirmative on question can convince itself that its position is sound, no further proof is needed to completely establish its case.
Since both the affirmative and the negative are at last convinced that “a clean tooth does not decay,” there is little further to be said, and the debate is won and closed. I am reminded, however, that I have been allowed fifteen minutes which should be put to profitable use, and to what better purpose could I apply the time still available to me than to submit a few suggestions which the gentlemen for the negative may find useful in future debates on this question, in which I am quite sure they will be defending the affirmative.
I would therefore suggest, first of all, that the full implications of the subject should be pointed out and clearly stated, so that an audience may obtain an intelligent understanding of the degree to which the public welfare is involved in the question under discussion. For example, we are discussing clean teeth and dental caries. Is this, then, the full significance of the subject and is it entirely devoid of a bearing upon the broader fields of general health and systemic disease? Such a narrow view would betray woful ignorance of the findings of advanced medical science. Scientific research has traced many serious systemic diseases to infections originating in the mouth and teeth. Dental caries is a disease of the teeth, and diseased teeth have often induced disease in vital organs of the body, undermined health and vitality, and sent to premature graves many fine men and women who were cut off at a period of greatest usefulness to their own families and to society. Such are the tragic discoveries of modern medical research, and these discoveries teach the inescapable lesson that we can no longer regard dental caries merely as a disease of the teeth; we must recognize it as a disease which may prove a menace to life.
It is appalling to contemplate that, of all the diseases that afflict mankind, dental caries is the most prevalent. More than 90 per cent of our children are afflicted with it. Dental caries is subtle, insidious, relentless; it attacks the child and undermines the man.
Must mankind continue to fall victim to this deadly enemy or is there ground for hope that we may yet conquer this menace as man has conquered countless others in his age-long struggle with his environment? The answer rests with science. Emancipation from dental caries is possible only if we discover its secret. As the first and fundamental step in a successful campaign against this scourge, science must set itself the task of determining its cause.
What is the cause of dental caries? What relation does the slogan, “A clean tooth does not decay” bear toward the possible cause of dental caries? Was this slogan conceived merely as a bright idea and did it “just grow,” like Topsy? Was this slogan broadcast to the public before or after scientific research into the cause of dental caries? Be it ever remembered that many years of scientific research devoted to an investigation of the cause of dental caries constitute the foundation and justification for the slogan “A clean tooth does not decay.” Moreover, this conclusion does not rest upon the findings of one man. Miller, Black, Williams–each an outstanding scientific investigator–have independently arrived at the same general conclusion.
Does clinical experience and scientific investigation carried forward since their day support or refute the findings of those students? All recent observers have corroborated the findings of Miller, Black and Williams; findings which indicate that dental caries seems to possess a peculiar affinity for certain surfaces of a tooth and is quite indifferent to the other surfaces of the same tooth. This discovery marked an epoch in the progress of dental science. It paved the way for further discoveries. There remained one great question for dental science to answer. That question was, Why this selective affinity? Why does dental caries attack only certain surfaces of a tooth? What conditions are present on or about the surfaces so attacked? What conditions are present on or about the surfaces dental caries fails to attack? If we can discover the answer to these fundamental questions, we have discovered the secret of dental caries.
The quest for an answer revealed that dental caries possesses an affinity only for those surfaces which present two specific conditions. Those two conditions are (1) structural and (2) proximal. The structural surfaces are invariably rough and depressed, and because they are rough and depressed serve as a trap for food debris. The biting surfaces of posterior teeth are of this type. The proximal surfaces are neither rough nor depressed and in consequence cannot of themselves serve as a trap for food débris, but their anatomical relation to their immediate neighbors serves to create mechanical traps for food.
Since dental caries possesses an affinity only for rough, depressed and proximal surfaces which trap food, what can be the relation between this trapped food and dental caries? It has been established that acid-producing bacteria and trapped particles of food must always be present before dental caries can attack any surface of any tooth. Now, any surface of any tooth which traps food is not clean and if dental caries attacks that tooth, it will be this unclean surface which will be attacked and which will decay. Conversely, any surface of any tooth which does not trap food is clean, and dental caries cannot attack any clean surface of any tooth; these clean surfaces therefore do not decay. If all the clean surfaces of all the teeth do not decay, are we not forced to the inevitable conclusion that “a clean tooth does not decay”?
Millions of teeth have been saved; the health of thousands of men, women and children has been served through this beneficent slogan. Could any one conceive of a more fitting memorial to the great men whose painstaking scientific investigations inspired the slogan, “A clean tooth does not decay.”
NEGATIVE
E. V. McCollum, M.D., Ph.D., Sc.D., Baltimore, Md.
It is the purpose of this debate to set forth the present state of our knowledge concerning the subject, “Resolved: That a clean tooth does not decay, and that mouth cleanliness affords the best known protection against dental caries.” There are several aspects of this question on which we possess very definitely established facts, which I shall consider as concisely as possible.
Diet and Tooth Structure
There is, I believe, no difference of opinion among investigators on the relation of the state of nutrition during tooth development to the structure of the tooth. Diets of a character unfavorable to calcification of the osseous system tend to cause the formation of hypoplastic teeth, characterized by deficiency in hardness, pits and fissures and other physical qualities which would be expected to render them more susceptible to the establishment of the carious process than would be teeth of perfect structure. M. Mellanby, in a long study worthy of high praise, appears to have established that there is generally a relation between tooth structure and susceptibility to dental caries. Her hypothesis is that primary structure and incidence of caries are directly associated. Since this is true in most cases, but not in all, she formulates a second hypothesis, which is, that there may be a change in resistance after a tooth is erupted, which is indicated by the character of the secondary dentin. Only about 2 per cent of 1500 human teeth examined were gross exceptions to these two hypotheses.
Since there is a direct relationship between body chemistry and tooth structure, if there is provided by Nature any protective mechanism, whether from within, through the nourishment of the tooth as reflected in the character of the dentin, or from without, as reflected in the environment through conditions in the mouth, we should expect that such protective mechanism would function most effectively when the body chemistry is such as, during the developmental period, would cause the formation of teeth of perfect structure. Since body chemistry is known to be profoundly influenced by the character of the diet, validity of the hypotheses of Mellanby can hardly be denied either on the basis of logic or experiment. Regardless of the ultimate explanation which may be accepted by investigators concerning the chemical nature of the protective mechanism which, under favorable conditions of diet, tends to protect the teeth from decay, the evidence that there is such a mechanism appears to be fully established.
Hypoplastic Teeth Do Not Necessarily Decay
That hypoplastic teeth do not necessarily decay cannot be denied. This fact is one of the strongest supports for the view that there is some protective mechanism which protects teeth from decay. The most obvious possibilities as to why such teeth may escape decay are (1) absence of aciduric microorganisms; (2) absence of fermentable residues in contact with the teeth; (3) good response of dentin to irritation.
One could quote workers of distinction in support or in refutation of any statement concerning these three factors in relation to tooth decay, and since Dr. Merritt will consider mouth cleanliness, I shall call your attention to the studies of Boyd and Drain and their co-workers, to offset the expressed views of Bunting, and emphasize only the work of Mellanby, Price and others which have a bearing on possibilities 1 and 3.
Boyd and Drain conclude: (a) B. acidophilus and other organisms of equivalently high acid-producing power may exist in large numbers in mouths persistently free from active caries. (b) Children receiving diets of a nature such that caries becomes inactivated and remains so, show no characteristic change in the morphological nature of the oral flora or in the acid-producing capacity of the organisms. (c) The incidence of B. acidophilus and all other organisms having similar acid-producing ability appears to be as great in frequency and numbers in the mouths of children receiving continuously such protective diets as in the mouths of those whose diet is not supervised. (d) No available facts demonstrate that bacteria can of themselves induce caries in the teeth of individuals whose diet is adequate.
Concerning the changes in the character of secondary dentin, there should be no difference of opinion. The illustrations given by Mellanby and by Price show that very dense dentin may be formed as a response of the tooth to irritation, and so tend to wall off the progress of caries. Such deposition of secondary dentin is the usual thing in lower animals, whose teeth are worn away by attrition. The fact is fully demonstrated that qualitatively the same principle holds in man. The fact that this resource fails in the majority of human mouths in regions where tooth decay is rife and that the diets of people highly susceptible to decay of the teeth are almost universally of the type which Mellanby calls “non-calcifying” lends strong support to the view that failure of the protective function of dentin is an expression of deviation from the normal of the body chemistry. Mellanby’s illustrations showing differences of structure of extracted human teeth as influenced by diet seem to establish the existence of a protective mechanism from within the tooth.
Other Points on Which There is A Conflict of Views
There is conflict of opinion on the following points: (1) the protective function of the saliva; (2) the protective function of mucin against caries; (3) the relation of vitamin C to susceptibility to dental caries; (4) the significance of an optimal intake of calcium, phosphorus and vitamin D in promoting caries immunity.
Saliva is a secretion of great variability of composition. Although there are recorded analyses which show on the average a significantly higher calcium and phosphate content of saliva in caries-immune as compared with caries-susceptible persons, no convincing arguments can be based on these studies at present because of the availability of many conflicting data.
It appears to me that the data respecting the possible role of vitamin C in determining susceptibility to dental caries are not sufficiently convincing to warrant basing any arguments on either side of this debate on this factor. The recorded experiments describing the favorable effects of giving large doses of orange juice have the defect that other sources of vitamin C have not yet been tried, and orange juice so treated as to destroy its ascorbic acid content, leaving the results to turn upon the inorganic moiety, including the alkalizing value, has not been tested. Furthermore, the fact that primitive Eskimos, whose immunity to caries is high, subsist upon a low vitamin C diet, points strongly to the existence of other dietary factors of greater importance. This statement is made with a full appreciation of the fact that in man ascorbic acid is of the greatest importance for maintaining the health of the pulp structures, especially the capillaries and odontoblasts, and there can be little doubt that deficiency of ascorbic acid will impair the function of the dentin-forming cells.
Calcium, Phosphorus and Vitamin D
Relative to the importance of the intake of calcium, phosphorus and vitamin D in increasing resistance, I can speak from experience covering many years. My own experience is limited to studies on the rat, but they confirm in every respect the human studies made by others. This experience is in harmony in every respect with the far more extensive studies of Mellanby, whose hypotheses have been set forth above. Both human and rat studies seem to establish that a diet of the calcifying type not only tends to insure the formation of teeth having perfection of structure, but likewise promotes the maintenance of those phases of body chemistry which afford the greatest protection to the teeth against caries throughout life.
It is well known that in the absence of sufficient vitamin D, calcium absorption is impaired, and that the phosphate-ion concentration of the blood tends to fall below the optimum. The principle is well established that the composition of the secretions of the glands is changed to a fairly marked degree reflecting the changes in the composition of the blood. No one has succeeded in securing twenty-four-hour samples of saliva nor of saliva during sleep. No adequate studies are available of the extent of variation of composition of mucin, which, because of the position of the mucinous glands, would appear to be provided especially as a protective coating for the teeth.
Any one familiar with modern physical chemistry can scarcely believe that the constant presence of calcium and phosphate ions in saliva is without significance. Any relatively insoluble mineral is protected against surface dissolution when in contact with a solution containing a favorable concentration of the ions which it is capable of giving off to that solution. The substance of enamel is capable of dissociation into these ions, hence a protective function of calcium and phosphate ions appears to be significant for protecting the integrity of the enamel.
Similarly, the high buffer value of saliva would appear to be important, not only for the purpose of maintaining a proper medium for amylolytic action of saliva, but for the neutralization of acids originating from fermentation of food, especially for protecting the teeth against decalcification. If such were not the case, why should the saliva of cattle and other ruminants, whose saliva contains no starch-digesting ferment, have a high buffer or acid-neutralizing value?
The function of vitamin D in regulating the process of calcification through its control of calcium absorption and of the phosphate content of the blood is so well established that it needs no discussion here. The simple theory here presented fits well with the observed fact that dental caries can be controlled through diet, and appears to satisfactorily explain all experience of investigators in this field.
All the cavities of the body are protected by the secretions which bathe them. The ear is covered with wax; the tears protect the eyes; the stomach mucosa is covered with mucus which underlies the acid-pepsin system which digests food. The presence of a neutralizing power and a high content of calcium and phosphate ions reflects against the view that saliva has no protective power on the teeth.
The Experience of Primitive People
Dr. Price will present his own studies on several primitive peoples, which show clearly that it is a general rule that such people have a low incidence of dental caries while subsisting on their native diets, which vary widely in nature in different geographical environments, but become susceptible to caries when they come into contact with a trading-post and secure a food supply similar to that eaten by man in highly organized society where tooth decay is rampant. The diet inimical to the health of the teeth contains an excess of refined cereal foods, sugar, etc., and too little of what I have called the “protective foods,” viz., milk, eggs, meats and the leafy type of vegetables. I shall call your attention to a few older observations which illustrate this fact.
The primitive Eskimos have been so frequently discussed that I shall not dwell upon their experience further than to say that when they had changed their diet in the manner just described, in Alaska and Labrador, they became highly susceptible to dental caries. The people of Iceland had a low incidence of tooth decay until the island was opened to world trade and the European and American type of diet came into general use. This event was followed by a marked rise in incidence of dental caries.
In Kenya, Zanzibar, Southern Rhodesia and Johannesburg, Orr and Gilks, Mellanby and others have observed native tribes living under primitive conditions and others in contact with civilization, and without exception have found the latter to have a markedly higher incidence of tooth decay than the former. Mellanby gives a good account of these studies.
The Island of Tristan da Cuhna is of special interest. There, isolated in the South Atlantic ocean, the 163 natives subsist upon fish, potatoes, eggs and milk, which are all abundant, and green vegetables during the summer. We should expect this diet, rich in mineral elements and the fat-soluble vitamins, to protect the teeth against decay. These people were inspected in 1926 by Marshall and Sampson, and in 1932 by Marshall and Moore. Although they do not clean their teeth, 128 out of 154 mouths were perfect. Only one decayed deciduous tooth was seen in sixty-two children. Only five decayed permanent teeth were found in people under thirty-three years of age, while above that age twenty-one out of forty-four people had perfect mouths. Tartar was found on the teeth in sixty-seven mouths.
The Maori show in the skulls of former generations under 1 per cent of carious teeth, but suffered equally with Europeans when their diet became similar.
Boyd and Drain and their co-workers reported a prolonged study of forty-five children. Thirty-four of these were on a weighed diet prescribed for the purpose of preventing dental caries. Thirty-two of the children showed no evidence of active caries; six had no cavities; the remainder had arrested caries. Repeated dental examinations over months and years established the constancy of their dental status.
Mellanby, in her institutional studies in Birmingham, by the administration of cod-liver oil reduced the initiation of caries from 3.976 to 1.825, the spread of old caries from 0.529 to 0.186, the spread of caries from 4.5 to 2.0, the increase in “degree” of caries from 1.564 to 0.302. She increased the relative “hardening” or arrest of caries from 0.058 to 0.407. The results of Boyd and Drain are of the same order.
At the University of Toronto, Drs. Tisdall, Anderson and Agnew and others have recently reported an extremely important investigation which again emphasizes the soundness of the views of Mellanby. They conclude that the administration of vitamin D in the form of irradiated ergosterol to children living under good hygienic and dietetic conditions markedly decreases dental caries. Their results are summarized as follows:
(1) The number of cavities originally present is not an index of susceptibility to new cavity formation,
(2) The effect of vitamin D in reducing the number of new cavities per child and in reducing the number of children who develop new cavities has been shown to be striking in the children of from three to ten years of age.
(3) Vitamin D is equally effective in reducing new cavity formation in both deciduous and permanent teeth.
(4) The favorable effects of vitamin D were as apparent within the family group as in the children not within the family groups.
I approve of mouth hygiene on general principles for the same reason that I approve of body cleanliness. I agree with Dr. Hyatt that pits and fissures predispose to caries, but I wish to state emphatically that pits and fissures are caused by faulty diet during the developmental period. I believe that any effective program of preventive dentistry must be based upon a dietary reformation by the nation which will insure (1) perfection of tooth structure; (2) continued health of the pulp structure through abundance of ascorbic acid; (3) blood chemistry, which will be reflected in a salivary chemistry optimal for protecting the tooth surface. This can only be accomplished through an abundance of calcium, phosphorus and vitamins D and A.
NEGATIVE
Weston A. Price, D.D.S., M.S., F.A.C.D., Cleveland, Ohio
Oral cleanliness is not the best known means for the control of dental caries because:
(I) It is not Nature’s method.
(II) Immunity and susceptibility can be clinically altered at will by modifying the nutrition.
(III) The controlling factors for immunity can be shown to be in the saliva and can be traced from plants to animal tissues and sera.
(IV) Tooth decay is not a disease, but a symptom, like many other degenerative processes.
(I) IT IS NOT NATURE’S METHOD
Since primitive man has had high immunity to dental caries he becomes our control in the great experiment of civilization. It is essential, therefore, that we study the controlling factors in his environment, of which he is the product, and use these as our yardstick for studying modern civilization. For this I have studied remnants of several primitive racial stocks where their physical isolation had sheltered them from the influences of our modern civilization, and by studying them and their foods and their methods of living, certain underlying factors are found to be common to all these primitive groups, even though they were living in different countries and on very different foods. This permits us to critically analyze modern civilizations at their points of contact with the primitives and, by studying them and their problems with the standards of the immune primitives, note the factors which are contributing to dental caries.
By studying the children in four isolated valleys in Switzerland–Loetschental, Visperterminen, Grachen and Ayer in the Swiss Alps–I found the incidence of dental caries to be only 4.6 per cent of the teeth studied. Here oral prophylaxis and modern equipment for practising it were largely unknown. At St. Moritz, however, at approximately the same altitude, which is a highly modernized community with excellent training in oral prophylaxis, the incidence of caries was 29.8 per cent of teeth studied. At Vissoie and Zinal, which were partially modernized, 22 per cent of the teeth examined had been attacked by dental caries. At Herisau, in the plains country of Switzerland, also a highly modernized community with splendid instruction and equipment for mouth cleanliness, the incidence of caries was 24.7 per cent of the teeth examined.
Similar studies were made in the Outer Hebrides off the west coast of Scotland and revealed that in the isolated districts of the Isles of Lewis and Harris only 1.2 per cent of the teeth examined had been attacked by dental caries. Oral prophylaxis was almost unknown. In the ports and modernized sections the incidence of dental caries was found to be 30 per cent of the teeth examined.
The natural foods available for these two primitive groups were very different in origin but similar in chemical content, as will presently be shown.
Similarly, studies were made of remnants of the primitive Eskimos and Indians of Alaska and northern Canada and of those individuals of these groups who are at the point of contact with modern civilization. The Eskimos of western and northern Alaska were reached by airplane and for several groups who had been but little influenced by modern civilization, hence living entirely on native foods, the per cent of teeth found to have been attacked by dental caries was 0.09, that is, only two teeth out of 2138 in seventy-two individuals. No effort apparently had ever been made at oral prophylaxis in these groups.
At the point of contact with modern civilization, where a government supply boat comes once a year to provision a government station, the incidence of caries among the local Eskimos increased to 13 per cent of the teeth, or 394 teeth out of 2254 in eighty-one individuals. At this point oral prophylaxis was being taught and practised and, in spite of it, the increase in dental caries was 144-fold. The controlling factors in producing these changes will presently be shown to be nutritional.
The natural food of the primitive Eskimos was almost entirely the animal life of the sea.
Similarly, quite primitive Indians were sought for and found in northern Canada who were living practically entirely on wild animals. Their physical isolation from the influence of modern civilization was very complete.
Three groups were found, consisting of seventy-six individuals with 2144 teeth and without a single tooth having been attacked by dental caries. In a total of 2464 teeth examined for eighty-seven individuals in four groups, only four teeth had ever been attacked by dental caries, or 0.16 per cent. These people knew nothing of oral prophylaxis as understood by modern civilizations.
For the groups of these Indians at the point of contact with modern civilization, 21.5 per cent of 1878 teeth in seventy individuals, or a total of 405 teeth, had been attacked by dental caries. This is an increase of 134-fold. These individuals had been taught oral prophylaxis.
When we arrange the incidence of dental caries according to the degree of contact with modern civilization and its foods, beginning with the coast towns and settlements of the Pacific coast of Canada and Alaska, including Wrangell at the mouth of the Stikine River, from which connection is made with Telegraph Creek up the Stikine River by boat in the summer and then by trail over the Rocky Mountain Divide into the Interior, we find that the percentage of teeth involved for seven coast settlements for all individuals for all groups studied is 40.8; Telegraph Creek, 14.9; Dease Lake, just over the divide, the first inside Hudson Bay Post, 9.6 per cent; and McDames and Liard, the two Hudson Bay Posts farthest in the interior, 3.1. For the most isolated and primitive of these last two groups a 0 per cent of teeth had dental caries. This is shown graphically in Fig. 1 for twenty-four places which reveal the relation of caries to nutrition.
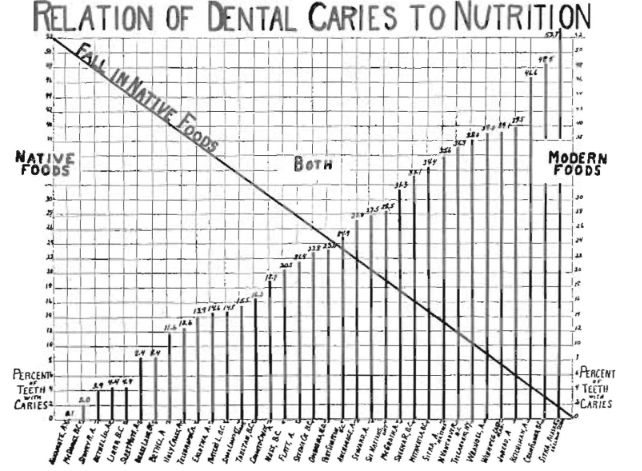
Fig. 1–This is an arrangement of groups of Eskimos and Indians in various stages of modernization in the order of incidence of dental caries. Note its reverse relationship to the decrease in the use of native foods.
Knowledge of and equipment for oral prophylaxis are in direct proportion in these groups with the incidence of dental caries, and dental caries is in direct proportion to the displacement of native foods with modern foods.
Accordingly, since the incidence of dental caries is shown to be in direct proportion to the utilization of modern foods to displace the native foods, we are concerned to know the chemical or physical qualities of the foods which constitute the controlling factors. Large numbers of samples of foods are collected for chemical analysis to provide this information.
The requirements of the normal human for two of the several requisite minerals, namely, calcium and phosphorus, have been shown by Sherman1 to be approximately two grams of each in suitable chemical form in the daily diet in order that the body may obtain at least one gram of each per day, which can only be accomplished when there is present an adequate quantity of the various vitamins, particularly the fat-soluble vitamins.
The quantity of these two minerals found from a study of the diets of both the immunes and susceptibles in Switzerland shows a marked reduction in several minerals as provided in the normal daily diet, consisting chiefly of entire rye and dairy products in comparison with the displacing diets obtained from modern civilization. This decrease was from 1.6 to 0.4 grams for calcium, from 1.8 to 0.8 for phosphorus and from +++ for fat-soluble activators to + on a basis of 2000 calories. This amounts to a reduction of 73.4 per cent for calcium, 55.1 per cent for phosphorus and 67 per cent reduction for the fat-soluble activators. This change is illustrated in Fig. 2.
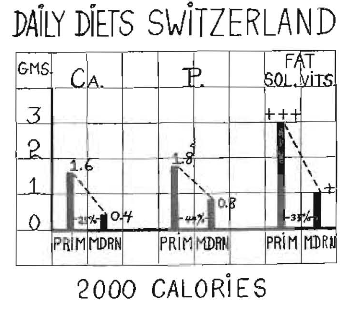
Fig. 2–Two minerals and the fat-soluble activators only are shown for the diets in Switzerland for comparison of the more primitive with the modernized groups. These were mostly children seven to sixteen years of age.
For the Outer Hebrides when their native foods, which consisted chiefly of oats and sea foods, are displaced with the diet used by modern civilization, there is a reduction from 1.7 to 0.8 grams for calcium, from 3.04 to 1.3 grams for phosphorus and from +++ to + for fat-soluble activators, a reduction of 52.3 per cent for calcium, 57.2 per cent for phosphorus and 67 per cent for fat-soluble activators on a basis of 2000 calories daily. This change is illustrated in Fig. 3.
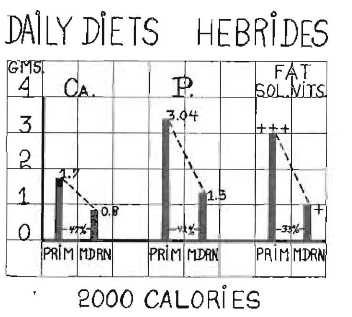
Fig. 3–Two minerals and the fat-soluble activators only are shown for the diets in the Outer Hebrides for comparison of the more primitive with the modernized groups. These were mostly children seven to sixteen years of age.
When the native diets of the Eskimos are changed from the animal life of the sea to those used by modern civilization, there is a reduction from 2.1 to 0.3 grams for calcium, from 5.7 to 1.1 grams for phosphorus, from +++ to + for fat-soluble vitamins or a reduction of 86 per cent of calcium, 80 per cent for phosphorus and 67 per cent for fat-soluble activators on the basis of 3000 calories for their severe climate. This is illustrated in Fig. 4.
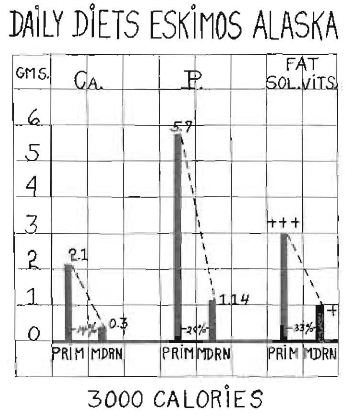
Fig. 4–Two minerals and the fat-soluble activators only shown for the diets of the Eskimos for comparison of the more primitive with the modernized groups. Both children and adults are represented.
For the Indians of northern Canada the loss of immunity when their normal diet, consisting chiefly of wild animal life of the land, was displaced with diets as used by modern civilization, the reduction was from 2.3 to 0.39 for calcium, from 6.6 to 1.14 for phosphorus and from +++ to + for fat-soluble activators on a basis of 3000 calories. This is a reduction of 84 per cent for calcium, 83 per cent for phosphorus and 67 per cent for fat-soluble activators. This is illustrated in Fig. 5.
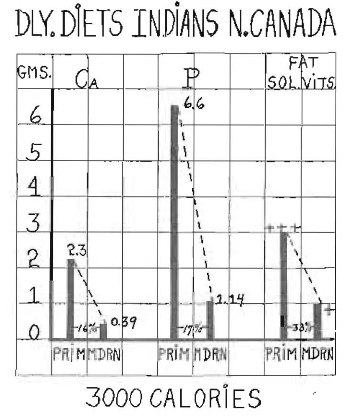
Fig. 5–Two minerals and the fat-soluble activators only are shown for the diets of the Indians for comparison of the more primitive with the modernized groups. Both children and adults are represented.
Determinations were made of several other minerals, which for brevity are not shown in Figs. 2 to 5. These have included in the analysis of the foods of the Eskimos and Indians the determination of magnesium, iron, copper and iodine. The per cent reduction for all of these for the two groups, the Eskimos and Indians, when changing from high immunity to high susceptibility to dental caries, is shown in Fig. 6, in which it will be seen that the reduction in each, magnesium, iron, copper and iodine is very great, which is doubtless quite as important as in calcium and phosphorus.
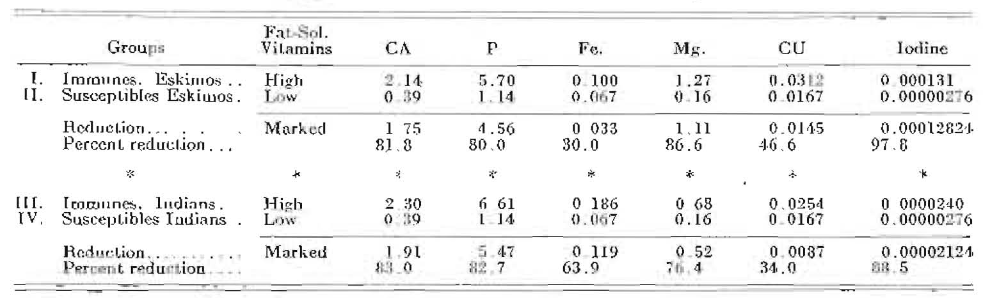
Fig. 6–Comparison of Diets of Caries Immunes and Susceptibles. The totals of six elements in the various foods used for an average day among each the immune and susceptible Eskimo and Indian groups are shown, also the total reduction and percentage reduction.
The minerals I have shown to be supplied in greatly reduced amount in the displacing foods as obtained from modern civilizations are building blocks out of which animal life has been constructed. The natural foods of the various primitive groups contained them in high proportion to the calories, or energy-producing factors. Ordinarily, hunger applies primarily to energy-producing foods. The primitives, accordingly, like the individuals of modern civilizations, choose the high-calory foods both because they easily satisfy hunger and provide energy and heat.
Since the maintenance of life is dependent upon at least a minimum of minerals and other chemicals of which blood and other body fluids are made, these must be borrowed in proportion as the daily intake fails to supply them. This produces nutritional stress which affects the blood and saliva. Dental caries is one of the direct expressions or effects of this nutritional stress. Nature, as we shall see, provides immunity to dental caries by maintaining these minerals and activators in normal balance.
(II) IMMUNITY AND SUSCEPTIBILITY CAN BE CLINICALLY ALTERED AT WILL BY MODIFYING THE NUTRITION.
If, as seems indicated in the data just submitted, the loss of immunity to dental caries is caused by an inadequate quantity of minerals and activators as provided in the daily diet, it should be possible by nutritional reinforcement to change individuals from a state of high susceptibility or loss of immunity to a state in which caries ceases to be active. I have previously reported several groups who have been so treated and in which dental caries had been reduced more than 90 per cent. I have been accomplishing this for ten years in individuals in clinical practice.
In addition to individuals in clinical practice, I have selected groups of children in districts where the industrial depression has most seriously curtailed income, and consequently has reduced nutrition. Severe cases of dental caries have been given a reinforcement of the nutrition in order to determine the effect of that procedure upon the progress of the dental caries. This has been based upon a reinforcement of the mineral and activator content of the nutrition.
In three mission clinic groups of children selected because of their high susceptibility to dental caries, who had their nutrition reinforced by the addition of fat-soluble activators obtained from high vitamin butter and high vitamin sea foods, particularly liver oils, together with foods that are rich in the needed minerals in proportion to the calories, the active caries has been practically completely controlled. This was provided in one meal a day. This complete control of dental caries was accomplished without making any change in the oral prophylaxis program. Associated with this reinforcement of the nutrition the decalcified dentin of open cavities was remineralized and in pulps that were nearly exposed by the decalcification process, zones of normal dentin were built in, walling off the approaching caries. This remineralization of the dentin is illustrated by the increase in density, as indicated by the inability of silver nitrate to penetrate the previously decalcified dentin, as shown in Fig. 7. The dentin in many cases became so dense that when scratched with a steel instrument it produced a metallic tone. An illustration of the building in of a protective wall of dentin is shown in Fig. 8.
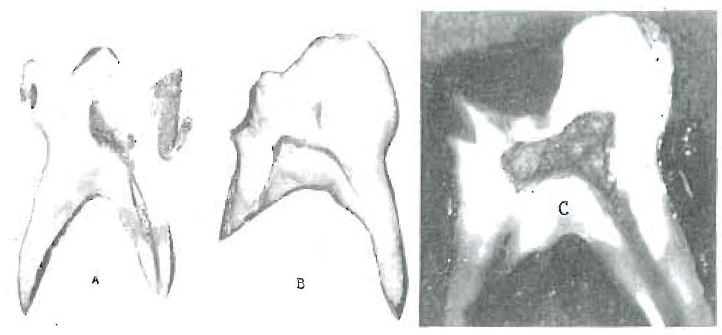
Fig. 7–The decalcified dentin of typical caries in B and C has been remineralized by changing the saliva through reinforcing the nutrition. The caries was not removed. A was extracted before treatment and shows the silver nitrate has penetrated the decalcified dentin.
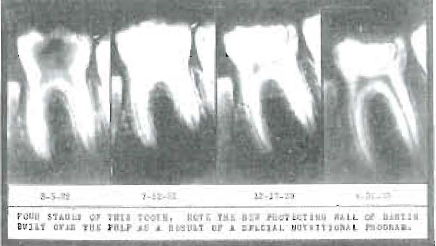
Fig. 8–Under suitable nutritional reinforcement not only is decalcified dentin remineralized but pulps are induced to build a new protecting wall of normal dentin, as shown in this case. A temporary filling was placed to protect the pulp from pressure.
(III) THE CONTROLLING FACTORS FOR IMMUNITY CAN BE SHOWN TO BE IN THE SALIVA AND CAN BE TRACED FROM PLANTS TO ANIMAL TISSUES AND SERA.
Typical dental caries has never been produced without the presence of saliva and even crowns of teeth attached to artificial dentures may be attacked by typical tooth decay in susceptible mouths. No teeth have been made dirty enough to induce typical tooth decay inside the mouth. Active caries promptly ceases with death. While the aciduric bacteria play a role, their action is rigidly controlled by the saliva, which provides the environment for the teeth. This control has been shown by me to be associated with the behavior of the inorganic phosphorus in its relation to adsorbents such as the structures of the tooth.
One phase of this is disclosed by shaking finely powdered dry bone in a sample of the saliva and noting its effect on the inorganic phosphorus level as compared with the untreated sample. In cases of high immunity the effect of the powdered bone is to markedly lower the reading of inorganic phosphorus. In cases of lost immunity or active dental caries, this reduction of inorganic phosphorus is greatly lessened or in very severe cases is increased and will follow the changes in immunity or susceptibility and vice versa as produced clinically. This is typically illustrated in a mission experimental group, as shown in Fig. 9. This shows the progressive effect produced by providing one meal a day in which mineral-carrying foods and fat-soluble activators were reinforced. It will be seen that an average change in the level of the inorganic phosphors of the saliva progressed from a plus 2.48 to a minus 11.7.
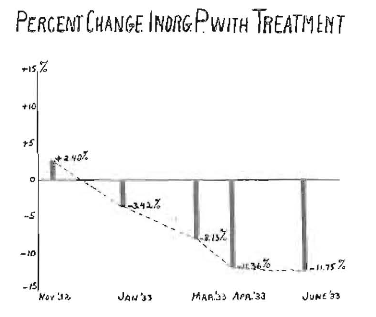
Fig. 9–In cases of active dental caries, the inorganic phosphorous of the saliva behaves abnormally in the presence of finely powdered bone and moves progressively toward normal under treatment by reinforcement of the diet, and occurs simultaneously with the cessation of active caries.
In a group of eighty-two individuals suffering from active dental caries who received reinforcement of the mineral and activator-providing foods, in all of whom there was complete control of the dental caries, there was a shift in the per cent of the inorganic phosphorus of the saliva when shaken with powdered bone, from an average of plus 8.4 to minus 11.2. This is shown in Fig. 10. In a group of 119 individuals, including both severe and mild cases of active caries, the per cent change was from an average of plus 5 to a minus 12 as the result of reinforcing the nutrition. Further evidence that this effect is due to the activating substances added to the nutrition is indicated by the changing of this chemical characteristic of the saliva of individuals suffering from rampant tooth decay and showing a plus reading by shaking the saliva for a few minutes with an activating substance, such as a high-vitamin butter or a high vitamin animal fat, then separating them and noting the effect of this procedure on the inorganic phosphorus when the saliva is shaken with finely powdered bone. Twenty-seven salivas with a plus reading changed when treated from an average plus of 9.7 to a minus 6.1. Much additional data are available which space does not permit including.
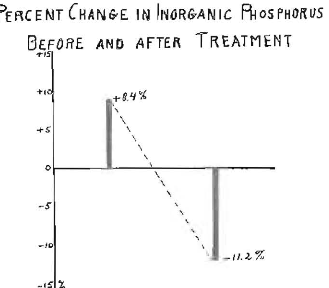
Fig. 10–In a group of eighty-two individuals receiving a reinforcement of the nutrition, the inorganic phosphorus of the saliva changed from the characteristic of active caries to the characteristic of immunity, as shown.
The route of the activating substances can now be traced from their original formation in the tissues of plants through the plant and animal foods to the blood and saliva and various tissues and fluids of the body. In the light of newer knowledge, some enzymes which are organic catalysts are directly formed from some of the vitamins. The vitamins in this very direct way influence and control function. These plant pigments that act as precursors of the vitamins include, according to Willstatter,5 Kulin6 and Gyorgy,7 the carotenes, lycopenes and flavines, of which several have been isolated. The carotenes have been termed fat-soluble, or lipochromes, and the flavines, water-soluble or lyochromes. These pigments are very widely distributed in plant and animal tissues and give evidence of being directly related to radiation. When crystallized, the flavines concentrated from milk have proved to be the most active growth-promoting substances as yet obtained. Evidence has been developed relating the vitamins directly to the organic catalysts or enzymes by several workers, including Kuhn and associates6 and Purr.8
(IV) TOOTH DECAY IS NOT A DISEASE, BUT A SYMPTOM LIKE MANY OTHER DEGENERATIVE PROCESSES.
While dental caries is recognized as the most universal affliction which accompanies civilization and is, as we have shown, a direct expression and effect of nutritional stress, it can now be shown to constitute or represent only one of many injurious effects or expressions of faulty nutrition. Rickets of childhood has been recognized as one of these. Several affections or so-called diseases of modern civilization are progressively on the increase. Others are particularly destructive for certain groups. Others chiefly maim and produce deformities in various parts of the body, such as the face and dental arches.
Facial and dental irregularities have been chiefly ascribed to mixed racial physical characteristics. In my investigations of primitive racial stocks and of the effects produced by their displacing of part of their natural food with foods of modern civilization, it has been disclosed that the rigid conformity to physical type characteristics of these races has been lost in a single generation as an effect of nutrition on the developmental processes during prenatal and postnatal life.
For the face this may express itself as retarded growth of either the middle third or lower third or both. This directly affects the arrangement of the teeth in the dental arches as well as the interrelation of the dental arches. It occurred in as high a percentage of full bloods in the first generation after adopting the nutrition of modern civilization as in the mixed bloods. This deficiency was also found to have an expression in many other structures of the body.
One of the most serious defects results in abnormal pelvic development and consequent increase in difficulties involved in child-birth, jeopardizing either or both mother and child. This greatly increases mortality for both.
These injuries were not limited in their expression to abnormal or disturbed physical development, but were found to be associated with a marked loss in ability to combat infections, both acute and chronic. Focal infections more readily metastasized, involving other organs and tissues of the body. For example, in twenty homes at the point of contact with modern civilization, ten bedridden cripples were found, chiefly involved with arthritis. Not one was found among the most primitive group.
It is common knowledge that primitive races are destroyed rapidly by tuberculosis when they make contact with modern civilization. This has been chiefly ascribed to an absence of an inherited defense. My studies of the primitives at the point of contact with modern civilizations have revealed that the individuals chiefly affected are those who show distinct evidence of nutritional disturbance in infancy and childhood, as indicated by a disturbed development of the facial structures.
Every one of twenty Eskimo and Indian boys and girls in the Government Hospital at Juneau, Alaska, showed marked irregularities of the teeth and dental arches. The same nutritional injury that had made normal physical development impossible had prevented the development of a normal chemical laboratory for producing the immunity maintaining factors. Most of these individuals suffered also from active dental caries. (Fig. 11.)
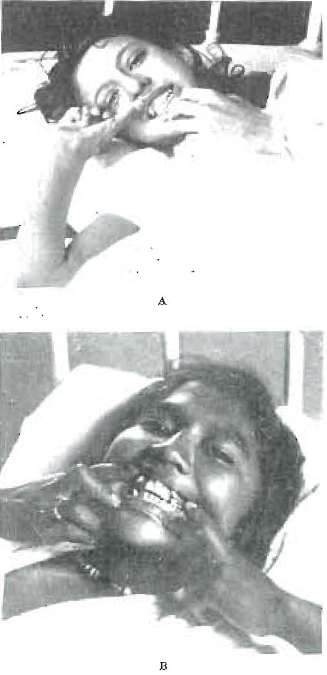
Fig. 11–These two girls are typical cases of pulmonary tuberculosis associated with deformity of dental arches and evidence of early nutritional deficiency which has also injured the chemical laboratory of the body, reducing the immunity-maintaining factors.
In my investigations now in progress I am finding this association to obtain in modernized communities. I am also finding that a very large percentage of the individuals referred for the study of a possible relationship between dental focal infections and chronic or acute systemic involvements in a very large percentage of individuals have evidence of physical injury which has resulted from a nutritional deficiency in childhood. This throws important new light on the clinical findings previously reported9,10 that over 95 per cent of the cases of heart involvement beginning before ten years of age (which includes over 70 per cent) suffered from rampant dental caries. Neither is necessarily the cause of the other; both are symptoms of a common nutritional cause, and neither is related to the presence or absence of oral cleanliness. (Fig. 12.)
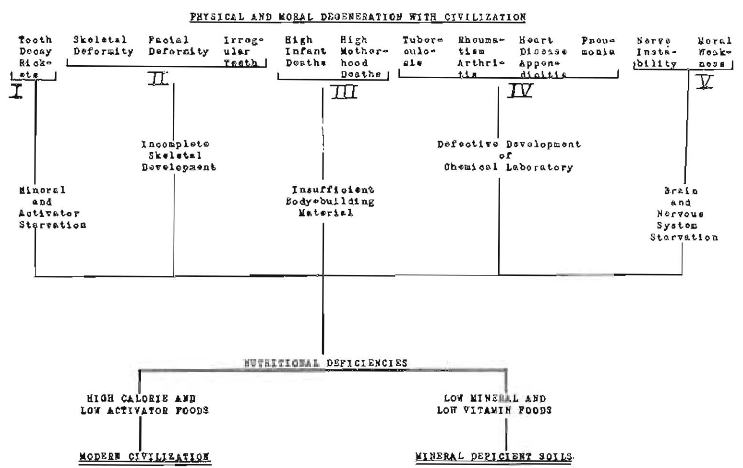
Fig. 12–The relation of some nutritional deficiencies to modern degenerations. In reading this tree from below upward, we trace the controlling factors for nutritional deficiencies to many of their expressions as modern degenerations or diseases of civilization.
A new truth is a new sense, but new truths come only to prepared minds. We must think of life in terms of its building blocks, and these are partly static and partly dynamic. Physical decadence, including dental caries, is in large part the absence of these dynamic vital forces. They have largely been overlooked because of the difficulties in their visualization and identification.
The arguments of the affirmative are typically those of this mechanistic or machine age.
References Cited:
- Sherman, H. C.: Chemistry of Food and Nutrition.
- Price, Weston A.: “New Light on Some Relationships Between Soil Mineral Deficiencies, Low Vitamin Foods and Some Degenerative Diseases. including Dental Caries. with Practical Progress in Their Control.” Indiana State Dental Association Bulletin, September 1932.
- Idem: “The Experimental Basis for a New Theory of Dental Caries, with Chemical Procedures for Determining Immunity and Susceptibility.” Dental Cosmos, 72:1139, December 1932.
- Idem: “Additional Light on the Etiology and Nutritional Control of Dental Caries with Its Application to Each District Showing Immunity and Susceptibility.” A. D. A. Journal, 20:1648, September 1933.
- Willstätter, R., and Mieg, W.: Annalen, 1907. 355, 1.
- Kuhn, R.: “On Natural Colouring Matters Related to Vitamins, Carotenes and Flavines.” Chemistry and Industry, December 8, 1933, p. 981.
- Kuhn, R., Gyorgy, P., and Wagner, TH. Jauregg, Berlin, 1933, G6, 317.
- Purr, A.: “The Influence of Vitamin C on Intracellular Enzyme Action.” Biochemical Journ., 27: No. 5, 1933. “
- Price, Weston A.: Dental Infections, Oral and Systemic. Vol. I, 1923. Penton Publishing Co., Cleveland.
- Idem: Dental Infections and the Degenerative Diseases. Vol. I, 1923, Penton Publishing Co., Cleveland.
NEGATIVE
Arthur H. Merritt, D.D.S., New York, N. Y.
No one engaged in the practice of dentistry can have failed to note the strange contradiction between theory and practice regarding the prevention of tooth decay.
Notwithstanding the fact that the dentist has been told repeatedly that clean teeth do not decay, that mouth cleanliness affords the best known protection against dental caries, he finds himself face to face in daily practice with another fact, namely, that teeth do decay under certain conditions in spite of the most painstaking efforts of himself and his patients. Although he exhausts every resource of mouth hygiene and arranges to see his patients at frequent intervals for prophylactic treatment, he finds that, notwithstanding the most conscientious efforts of his patients in daily care, all his efforts at prevention, with few exceptions, are more or less of a failure. By these measures he may succeed in reducing somewhat the incidence of tooth decay and may reap some of the rewards of early treatment, but the goal toward which all his efforts are directed is never reached; teeth continue to decay despite the united efforts of himself and his patients.
On the other hand, he sees cases in which no attention whatever is paid to oral hygiene, where the mouth and teeth are never clean, and yet the teeth remain throughout life free from caries.
Moreover, as he studies the records of his patients, he finds there are those among them who continue for years without the decay of a single tooth, and then, without any change in the cleanliness of the mouth, caries develops in teeth that have never before been affected.
Again, as he studies this strange contradiction, he finds that the human race was at one time in its history more or less immune to tooth decay; that to a limited extent this is true of certain races at present, and that this is true, in spite of a complete disregard of every principle of mouth hygiene.
He observes, furthermore, that notwithstanding all that has been said and done about mouth hygiene in the past twenty-five years, in spite of its application to daily practice by many dentists in every part of the world, in spite of prophylactic odontotomy, little real progress has been made in the actual prevention of tooth decay; it still remains the most nearly universal affliction of civilization.
If, then, this be the experience of the dentist actively engaged in practice, who exercises every resource of mouth hygiene, what is the explanation of this tantalizing contradiction?
One is, that no matter what is done, teeth cannot be kept so clean that, under certain conditions, they will not decay. A surgically clean tooth is an impossibility. And since bacteria are the local exciting cause of tooth decay, there can be no assurance on the theory of mouth cleanliness that teeth will not decay as long as there are bacteria in the mouth. Bunting says: “Cleanliness is only relative, absolute and permanent cleanliness not being attainable.” This is confirmed by Fones, who says: “It is impossible to sterilize the human mouth,” a statement which no one will deny. If it be said that sterilization is not necessary, that one has only to remove bacterial plaques from the teeth as they occur in order to prevent decay, Bunting’s reply is: “We have seen with what rapidity mucus and bacterial plaques form on the smoothest surfaces, even under the most careful and rigorous prophylactic measures.”
When it is remembered that in a full complement of teeth there are 160 surfaces; that many of these are difficult of access; that each surface must be kept clean if by this means tooth decay is to be prevented, one must be an incurable optimist who believes that by measures so unreliable tooth decay can be prevented.
Another explanation is that tooth decay is not simply a matter of mouth hygiene, but one that is subject to the law governing all infections, namely, the measure of resistance which the host offers to the infecting organisms. When this resistance is normal, teeth will not decay, no matter how unclean the mouth may be. Even pits and fissures are immune, as shown by Bödecker in his studies of the Pueblo Indians. When it is subnormal, as is usually the case under conditions of modern life, susceptibility to decay may reach a point where the most intelligent efforts at mouth hygiene will avail but little. Bödecker says: “There is a class of patients whose resistance to caries is so low that no amount of oral prophylaxis will prevent the destruction of their teeth. All dentists and many patients know that our best available methods for keeping the teeth clean will not prevent decay.” And when it is further understood that there are varying degrees of susceptibility; that these are subject to frequent changes and are wholly independent of local conditions, is it reasonable to suppose that tooth decay can be prevented by the application of measures that are purely local?
If, following one’s efforts at mouth cleanliness, there is a decrease in the incidence of tooth decay, how is one to know that this has been brought about by the establishment of mouth hygiene? May it not, with equal logic, be ascribed to a coincident decrease in susceptibility? To put it in another way, how is one to know in a given case whether the decrease in tooth decay has been brought about by mouth cleanliness or by a coincident increase in immunity? Is it not probable that, in our ignorance of the laws governing immunity and susceptibility to tooth decay, we have in many instances given credit to mouth hygiene that should in reality have been given to immunity?
When resistance is high, our prophylactic measures appear to be eminently successful. We take to ourselves great credit, and immediately jump to the conclusion that a clean tooth does not decay. When it is low, we fail in our local efforts at prevention, not because they are less efficient in themselves, but because, under conditions of lowered resistance, they are ineffective.
That there are forces governing immunity and susceptibility to tooth decay that are wholly independent of local conditions, there cannot be the slightest doubt. They are the dominant factors, the control of which is absolutely necessary if tooth decay in the aggregate is ever to be prevented. What these factors are and how they operate to influence favorably or favorably the problem of dental caries are matters which have been explained by Drs. McCollum aud Price. They have given years to their study and have shown in many ways that it is not through the uncertain operations of mouth cleanliness that the key to prevention is to be found, but in a wider knowledge of the constitutional mechanism which controls immunity and susceptibility.
How true this is has been shown by the work that was done and is being done in Honolulu by a group of investigators dealing with preschool children. So rampant was tooth decay among these children that in many instances the deciduous teeth were destroyed within a few months after corruption, a condition which was wide-spread among them. As a result of their researches they found that, by controlling the diet, they were able not only to reduce the incidence of tooth decay almost to the vanishing point, but at the same time to curtail the mortality rate to a marked degree. And this was done without any attention whatever being given to mouth cleanliness.
Based on their experience, extending over a period of years, it is their belief that “dental decay is primarily a systemic disorder, an imbalance perhaps in the tissue fluids and oral secretions in the direction of a decrease of basic ions, either relative or absolute, resulting from varying intensities of those factors which regulate metabolism. It is believed that any type of diet, any factor or combination of factors which tend to decrease the relative or absolute amount of base in the tissue fluids, will proportionally increase the liability of the teeth to decay.” As a further example of the constitutional origin of dental caries, McBeath has shown that resistance to tooth decay can be greatly increased by the use of ultraviolet light. In two groups of children, living under identical conditions in an orphanage, it was found that the experimental group exposed to ultraviolet irradiation had eight times less tooth decay than the control group.” It must be apparent, therefore, that tooth decay is not simply a local phenomenon, but one controlled by the laws of immunity and susceptibility.
At the same time it should be said that, other things being equal, the cleaner the teeth the less liable are they to decay. This is seen when one compares the relative freedom from caries of one group of teeth with another group in the same mouth, as, for example, lower incisors with third molars. This is further emphasized when one considers the relative immunity of the different surfaces of the same tooth.
For these and other reasons we should continue in our efforts at mouth cleanliness, for cleanliness is an important factor in the health of the mouth and teeth. The fallacy consists in believing that teeth can be kept clean and that mouth cleanliness affords the best known protection against dental caries. Can it be that Bödecker is right in saying: “Most people cling to old ideas and thus an accepted theory is maintained long after its period of usefulness is over.”
The real question, therefore, is not whether hypothetically clean teeth do or do not decay, but whether, under the conditions of modern life, by which their susceptibility to caries has been enormously increased, they can be kept so clean that they will not decay.
The answer may well be left to any one who has tried it.
References Cited:
- Bunting, R. W.: Oral Pathology, p. 213. Philadelphia: Lea & Febiger, 1929.
- Fones, A. C.: Mouth Hygiene, p. 252. Philadelphia: Lea & Febiger, 1934.
- Bödecker, C. F.: “Concerning Defects in the Enamel of Teeth of Ancient American Indians.” Journ. Dent. Research, 10:313, June 1930.
- Idem: Letter to the author.
- Jones, Larsen and Pritchard: “Dental Disease in Hawaii.” Dental Cosmos, 72: 698-797. July and August 1930.
- McBeath, New York State Journ. of Medicine, September 15, 1933.
REBUTTAL–NEGATIVE
Dr. McCollum. I shall take about five or six minutes, and leave the rest to Dr. Price. The affirmative has failed to give a satisfactory explanation for a certain type of observation which has been in literature now for from a year to ten years, and it is illustrated by the following type of study.
The Toronto group of pediatricians and dentists, Dr. Tisdall and Dr. Agnew in particular, have reported a study in which they have compared the incidence of dental caries in children living at home, where there is no special care given to the selection of the food, that is, no special knowledge applied. They find in that group an average of three new cavities per child per year. In a group of children of the same racial stock in Toronto, children who have grown up in an orphanage under the supervision of persons of intelligence and education, where the diet according to all present standards is of excellent quality, but undoubtedly still falls short of the optimum, they find one-half as many, or one and one-half new cavities per child per year. In this same orphanage and with this diet of high class, the addition of vitamin D to the diets of these children shows a further reduction of caries.
The affirmative also avoids the discussion of a problem which is illustrated by the Island of Tristan da Cunha, which is about 1500 miles west of the Cape of Good Hope in the South Atlantic, a place where there is relatively little sunshine, and which has had a human population for about 125 years. In 1932 there were 163 persons on the island. They are of mixed English, Dutch, American and South African Negro stock, and this island, formerly visited by whaling vessels, has not frequently been visited since the introduction of the steam trawler thirty years ago. So they are living under very primitive conditions as respects food. This island was visited in 1932 by Dr. Becbe on a British ship, and he examined the teeth of 163 people on the Island. The incidence of caries in the entire population is extremely low; there was one man of seventy-eight years of age with no evidence of dental caries. These people subsist largely upon fish and milk, and have a large supply of eggs, both hen’s and penguin’s. They eat potatoes freely throughout the year, and cabbage and turnips during the part of the year when they can keep them. They have no cereal. I mention this especially because the presence of a fairly high starch content of the diet in the form of the potato has not increased appreciably their susceptibility to caries.
So that after considering all the knowledge which is available to me, I would suggest a modification of the slogan which has so long been repeated, to read–a clean tooth with perfection of structure, well exercised and well nourished will not decay. And in so far as we work toward the objective of getting the public to change its dietary habits to an extent which will result in the development of teeth without physical imperfections, and then help them to adhere to such a diet throughout life, shall we be relieved, as a nation and as individuals, of a health hazard which is among the two or three greatest health hazards we know.
Dr. Price. I know of no more universal fallacy than the conception that the reason why extension for prevention has helped to save teeth is because the food keeps the surface of the inlay or filling clean, because if that were the reason, why build close contacts so the food cannot crowd across the margin of the filling that is under the gingival border to keep it clean. I can tell who are dentists by the response. Do you see what I am saying? That the reason we found, or thought we found, that extension for prevention saved the teeth by keeping them clean, was a misconception, for what we really did was to make every surface of that tooth either a foreign substance or a surface that could be bathed with normal protective saliva. ln every argument that has been made this evening, if those men will just substitute the smooth surface that does not retain food for one that will let normal protective saliva reach that surface, they will have accomplished all that they think they are doing with their present method.
What I am saying is, this whole problem of the control of dental caries has been based upon two or three major misconceptions. One of them was the tremendous fallacy that, by having our teeth cleaned, we were going to prevent dental caries. The thing that has really happened through all the ages, with man and the animals, is that they are not making the proper kind of saliva when they do not have suitable food to make the proper kind of blood and saliva. For we get the same chemical changes in the saliva of the animals that we get in the human. It would be fortunate, if time permitted, if I could go into more detail. There are preventive means in the saliva, as in tears, that control bacterial growth, and those in saliva are related to the condition of the inorganic phosphorus, and the inorganic phosphorus apparently has its action in part by controlling the capacity of the ferments of the bacteria in breaking down the sugars. But something else has happened. When an individual tooth is in the proper kind of saliva, there is a migration at all times of ions of phosphorus and calcium toward that tooth, from the saliva on the outside and from the blood on the inside. And that same reaction will produce the laying down of the layer of protective dentin in the pulp chamber, and will make a deposition of minerals from the saliva into the tooth surface by a process of adsorption. There is a mechanism there that makes a deposition of minerals into decalcified dentin.
When I studied the people who are breaking in the hospitals with tuberculosis, and it is tremendously interesting and so far as I know the first time it has been reported, it was chiefly those people who had evidence of an injury in childhood as expressed in irregularity of the teeth that were breaking. In twenty boys and girls in the Juneau Hospital, dying with tuberculosis of the lungs, every one of them had irregular arches. Dental irregularities affected large numbers of them, and irregular teeth were not found, except one or two that were pushed out of place by supernumeraries. That problem has its corollary in this other important thing; viz., that when we take these boys and girls who are in the hospitals and are breaking with heart and inflammatory rheumatism and put them on a properly reenforced diet, we are making them so much more capable of fighting their infection that many of them are getting back on their feet again.
Back of all of this is an injury to the chemical laboratory of the body, due to the imperfect nutrition which makes us susceptible to degenerative diseases.
The reason we have failed is because we have read into life and nutrition and dental science and medical practice too much of the role of mechanical problems. We must learn to think in a new dimension, and that new dimension is dynamic; it is not static. It is energy that was in the sun last year or last month or last week and strikes the plants, and the pigments formed go into the structure of plant life and become the food of the animal life. The animal stores it in every organ, particularly the liver, heart and kidneys, and the animal that eats that animal will be saved, provided he eats those organs in which the pigments are stored. These things are transmitted from the plant to the animal and from one animal to another, and if we will do like the Eskimo, not eat just the muscle meat only but some of every organ, we will eat the pigments that come forward to us. And when they come into our body (and this should be particularly interesting for my dear friend, Dr. Hyatt), when these pigments are built into our tissues as vitamins, these vitamins can be made over into what we call enzymes or organic capsules, which are the substances that control metabolism in the cells of all the body, including the salivary glands, and thus make it possible for the individual to make the proper kind of saliva that will maintain immunity to dental caries.
REBUTTAL–AFFIRMATIVE
Dr. Hyatt. I believe every one present has enjoyed this evening. I hope you all remember my first sentence: “It is in high challenges that high truths have the right of appearing,” and I think we are all agreed that our dietitian friends have said all that is possible for diet.
While I am a firm believer in a well balanced diet, I feel there is yet much to be learned as to what are the correct foods for us who are living in New York. Take the people living in India near the Himalaya Mountains who have not eaten meat for thousands of years; bring them to New York and put them on the Eskimo’s diet and what will happen? Take the Eskimos and bring them to New York and place them on a vegetarian diet and what will happen? If you want to go to Labrador and be an Eskimo, all right; but who wants to be an Eskimo?
May it not be that our bodies have to become acclimated to new foods? In other words, our system or method of metabolism is upset by drastic changes in food habits.
Dr. Walter, of the Division of Medicine of the Mayo Clinic, has just published a report showing the effects of ordinary articles of diet on 100 patients.
Many of these foods caused acute indigestion, while others caused severe poisoning. Permit me to read to you the list of foods presented in this report: Cabbage, apples, tomatoes, milk, chocolate, onions, lettuce, coffee, strawberries, eggs, meat, cucumbers, fats, sweets, radishes, cheese, cauliflower, spices, peanuts, corn, cantaloupe, peppers, prunes, oranges, sweet potatoes, sour food, peas, pickles. Now I ask you what is a fellow to eat?
It so happens that I am very fond of those little raw onions called scallions. I ate a lot for lunch one day and after lunch I went to the Children’s Preventive Clinic of the New York University Dental College. My friend, Dr. Waite Cotton, was there, and we had to go over some problems together. Dr. Cotton has made a study of diet for over thirty years, and has advised me regarding different foods. After our conference Dr. Cotton very kindly laid his hand on my shoulder and advised me not to eat onions. I had not told him I had eaten any onions. Now why did he tell me that?
This whole problem is not a one-sided question. Permit me to call your attention to the fact that none of our learned friends on the negative side took exception to my so-called axiomatic statements. Not one denied that decay starts on the outside of the tooth; that it is the acid produced by the bacteria that breaks down the lime salts; that bacteria and food debris have to be retained undisturbed for a definite time at one place to start decay: that when these factors are not present you do not have decay. Not one of our opponents denied these facts.
Our Children’s Preventive Clinic has only been in existence about four years. There are over 275 children of all walks of life, and their ages run from six months to five years when first admitted. Up to the present time, by operative preventive measures and mouth cleanliness alone, we have not lost one baby tooth or one first permanent molar through or by decay. This, too, with no change in diet.
Therefore I still stand by Dr. J. Leon Williams’ slogan “A clean tooth does not decay,” knowing, as I do, the good this slogan has done for the people of our country.
Dr. Walker. May I remark at this time that the subject for debate is “A clean tooth will not decay.”
We are not unmindful of the fact that unclean teeth may not decay. Why? We do not know. Perhaps the answer to this will prove the solution of the problem, but the simple fact remains that a clean tooth will not decay.
Dr. Merritt tells us that our very best efforts toward mouth cleanliness have not succeeded, which is but another way of saying that we have not yet learned how to attain the same degree of cleanliness ou the irregular and in-between surfaces as on those accessible (to cleansing) surfaces which resist decay.
Dr. McCollum referred to hypoplastic teeth. Obviously, only teeth with normal enamel protection are under discussion.
Dr. Price’s belief that the saliva is the protecting agent supports the theory of external as against the internal influence, and brings us to a consideration of environment and the possible cleansing influence of mouth secretions.
Dr. William. The affirmative underlook to defend the proposition that a clean tooth does not decay. They defended it here in the Pennsylvania Hotel, New York City. The negative attempted to refute our contention and where did they go? They went thousands of miles away from the United States of America in an effort to show that the affirmative did not prove its case.
There are 125,000,000 people in the United States, every one of whom is interested in the subject of this debate.
Dr. Price made the statement that immunity and susceptibility can be controlled at will. Is that quoting you correctly, Dr. Price? Now, that is optimism of the highest order, and I am very happy to note this optimism. I want to remind Dr. Price, however, that such optimism carries with it grave responsibility. We are all agreed on one thing; that is, that the most prevalent disease of man is dental caries. When a member of our profession undertakes to make the sweeping statement that immunity and susceptibility can be controlled at will, he has something to answer for, he and his profession have something to answer for to the American people, 90 per cent of whom are afflicted with this disease. Why have not the dietitians in all these years discharged their obligation to the American people through their specific method of creating immunity? Why have they left it to us to deal with the problem which diet might have prevented?
The dietitians have created a condition with which we must deal, and we have attempted to discharge the obligation which thus fell to us. We have done this for many years, and we have shown results. Wherever a program of mouth hygiene has been systematically instituted, a decrease in the incidence of den; tal caries has been achieved. What does this prove? It proves that proper cleansing of tooth surfaces prevents the decay of those tooth surfaces. Which, in turn, proves what? It proves once again that a clean tooth does not decay.
Editor’s note: Since the era in which this article was written, society’s understanding of respectful terminology when referring to ethnic and cultural groups has evolved, and some readers may be offended by references to “primitive” people and other out-of-date terminology. However, this article has been archived as a historical document, and so we have chosen to use the authors’ exact words in the interest of authenticity. No disrespect to any cultural or ethnic group is intended.