
Access to all articles, new health classes, discounts in our store, and more!
Protein Consumption and Cardiovascular Complaints
Published in The British Journal of Clinical Practice, Vol. 22, No. 5, May 1968.
* * *
Introduction
The increasing efforts to identify dietary factors in the genesis of heart disease have been largely directed to the fats (saturated versus unsaturated) and, more recently, to the carbohydrates (complex versus simple). In a review of the literature only one reference (Pilgeram et al. 1964) to a possible correlation of protein consumption and heart disease was noted. Specifically, in a group of men with proven myocardial infarction, plasma albumin (an essential receptor of free fatty acid produced by the lipoprotein lipase clearing system) was shown to be significantly deficient. This co-factor defect of the fat clearing mechanisms was shown to be corrected, in vitro, by the addition of electrophoretically pure human albumin. These data may prove quite significant when considered in the light of relationship between dietary and serum proteins. The following report is intended to relate dietary protein intake with early characteristic, if not pathognomonic, findings suggestive of cardiovascular pathosis in relatively healthy individuals.
Method of Investigation
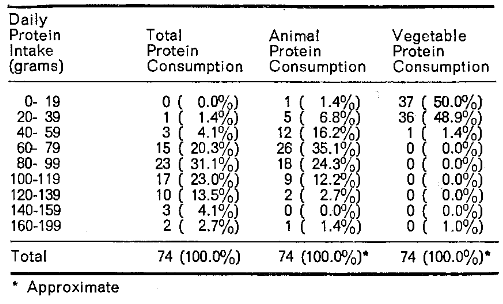
Seventy-four dental practitioners and their wives (members of the Southern Academy of Clinical Nutrition) shared in this experience. The relevant raw data are included (Table I). It will be noted that the majority of the subjects were in the fourth decade (Table II). Each of the participants completed the Cornell Medical Index Health Questionnaire (Brodman et al. 1949). Thirteen of the questions (Table III) concern cardiovascular symptoms and signs. Table IV shows the frequency distribution of affirmative responses. It is clear that the majority (41 of the 74 persons) reported no positive answers. However, affirmative answers ranged to a height of seven in one person. Each subject also submitted a seven-day dietary record and protein consumption was calculated (U.S. Agriculture Handbook No.8,1963). Summarized is the daily total protein intake expressed in grams per day (Table V). On the basis of recognized protein requirements (Pub. 1146. Nat. Acad. Sci. 1964), there is no gross protein deficiency. Since the difference in nutritive value of animal versus vegetable protein is frequently emphasized, outlined also (Table V) is the daily animal and vegetable protein consumption. On the basis of the available evidence, animal protein consumption is much greater than the consumption of vegetable protein foodstuffs.
Table I–Relationship of Cardiovascular Complaints and Daily Protein Consumption
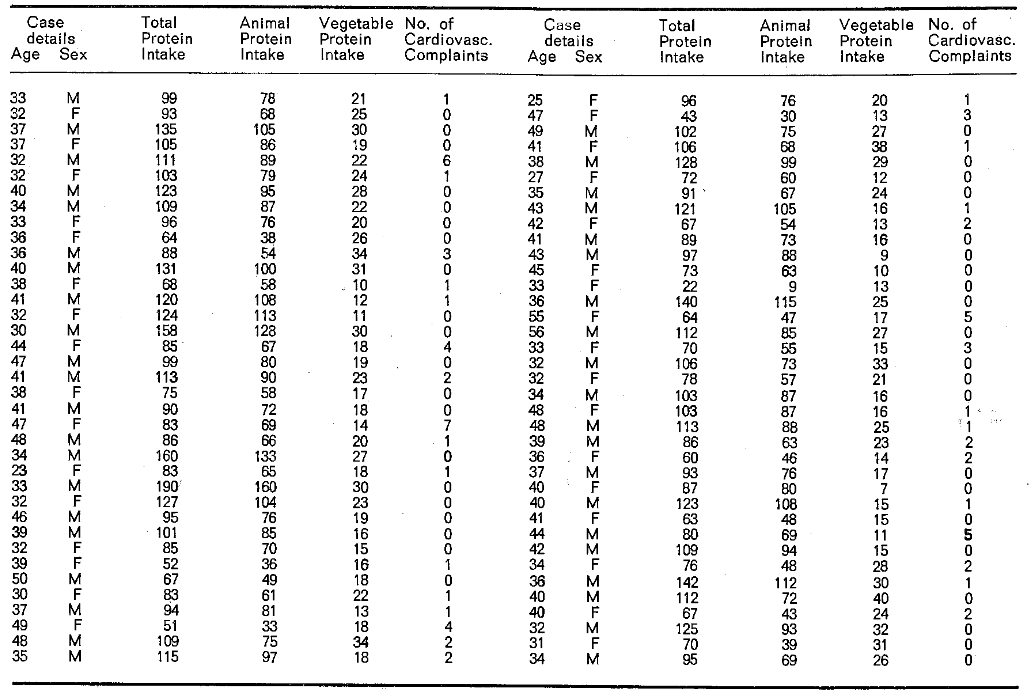
Table II–Age and Sex Distribution
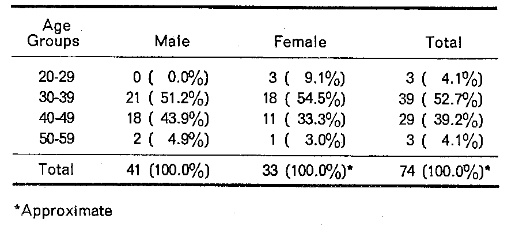
Table III–Cardiovascular Questions in the Cornell Medical Index Health Questionnaire
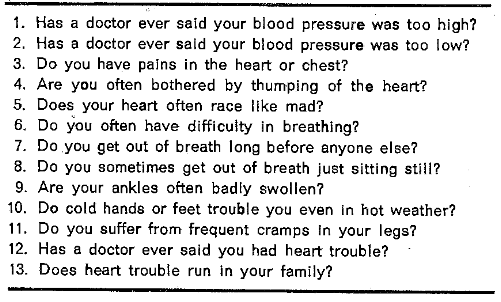
Table IV–Distribution of Cardiovascular Complaints
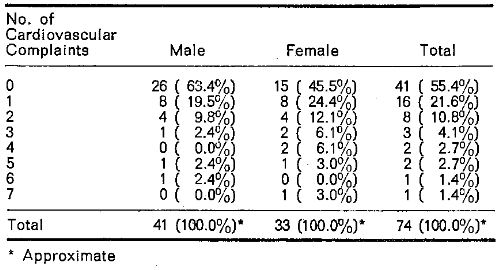
Table V–distribution of Daily Protein Consumption
Results
The 74 individuals were divided as nearly equal as possible into two categories in terms of animal protein consumption (Table VI). By this technique, 38 subjects consumed the lesser (9-75g.) and 36 the greater (76-160g.) intake. Likewise, the 74 subjects were divided on the basis of vegetable protein intake with 37 consuming the lesser (7-19g.) and 37 ingesting the greater (20-40) amount.
Table VI–Relationship of Cardiovascular Complaints and Daily Animal and Vegetable Protein Consumption
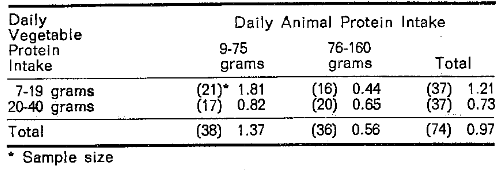
Table VI summarizes the mean cardiovascular scores in terms of animal and vegetable protein singly and in combination. First, the mean score for the entire group (n=74) is 0.97. The average score for the group consuming the greater amount of animal protein (76-160g.) versus lesser consumption (9-75g.) irrespective of vegetable protein is 0.56 versus 1.37 respectively. Table VI also shows that the greater the vegetable protein intake (irrespective of animal protein), the lower the mean score (0.73 versus 1.21). Finally, Table VI demonstrates that the highest mean score (1.81 positive responses per person) occurs in the group with the smaller vegetable and animal protein intake.
There is general agreement that one of the important ingredients in chronic disease is time (duration). In other words, not only must there be a problem, but it must be extended in time in order to produce visible evidence of illness. Accordingly, the sample has been further subdivided by age into two near-equal subgroups.
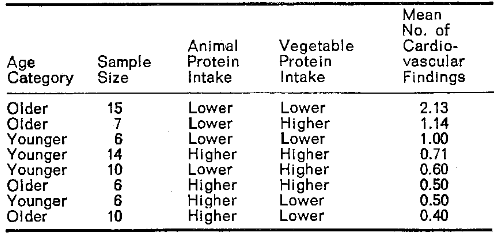
Table VII summarizes the mean number of cardiovascular complaints in terms of age and the quality and quantity of ingested protein. It is noteworthy that the mean number of cardiovascular findings is greatest (2.13 per subject) in the older individuals (n=15) with both relatively low intake of animal and vegetable protein. In fact, the three subgroups characterized by the lower animal protein show the greatest number of cardiovascular symptoms and signs (2.13, 1.14, and 1.00). In contrast, the three groups characterized by the relatively high animal protein consumption display the least number of cardiovascular findings (0.40, 0.50, and 0.50).
Table VII–Summary of Mean Number of Cardiovascular Complaints
Discussion
A comparison of these findings with those previously reported in connection with carbohydrate consumption and cardiovascular findings discloses two important differences. First, carbohydrate intake and cardiovascular symptoms and signs related positively. In other words, the greater the carbohydrate consumption, the more the complaints. In contrast, the relationship of protein intake and cardiovascular score in this paper is negative. Second, a comparison of the carbohydrate and protein studies discloses that the latter relationship is more sharply defined. (Cheraskin et al. in press).
It is recognized that dietary analysis, at best, is crude. It is also noted that the cardiovascular history derived from the Cornell Medical Index Health Questionnaire is gross. Finally, it is well to emphasize that the conclusions, in the form of relationships, do not prove cause-and-effect. Notwithstanding, the correlations (the first such recorded) could be tested by noting cardiovascular state following the addition and elimination of protein.
Individuals who consume large amounts of carbohydrate very frequently eat less protein. Hence, one wonders whether the findings in this report and those in the earlier one may not be related purely on this reciprocal basis. For this reason, a report to follow will consider the frequency of cardiovascular complaints in four dietary groups: (1) high protein and high carbohydrate, (2) high protein and low carbohydrate, (3) low protein and high carbohydrate, and (4) low protein and low carbohydrate.
Summary
- This is a study of the correlation of cardiovascular complaints (elicited from the Cornell Medical Index Health Questionnaire) and daily animal and vegetable protein consumption in 74 dental practitioners and their wives.
- The results suggest a greater frequency of positive cardiovascular responses in the relatively older persons who consumed lesser quantities of protein, particularly of the animal variety.
- The findings reported here with protein are reciprocally related to those previously described with carbohydrate consumption (Cheraskin et al. (A)). For this reason together with the observation that persons who eat large amounts of carbohydrate frequently do not consume much protein, a report will follow (Cheraskin et al. (B)) which analyzes cardiovascular complaints in the light of both carbohydrate and protein consumption.
References Cited:
- Brodman, K., Erdmann, A. J. Jr. & Wolff, H. G. (1949) Cornell Medical Index Health Questionnaire: Manual. Cornell University Medical College, New York.
- Cheraskin, E., Ringsdorf, W. M. Jr., Setyaadmadja, A. T. S. H. & Barrett, R. A. (A) “Carbohydrate consumption and cardiovascular complaints.” Angiology. (In press); (B) “Carbohydrate-protein consumption and cardiovascular complaints.” (In preparation).
- Food and Nutrition Board (1964) Recommended dietary allowances. 6th rev. Edn. Pubn. 1146. National Academy of Sciences, Washington.
- Pilgeram, L. D., Bandi, Z. & Thelander, P. F. (1946) “Albumin correction of the clearing factor defect in ageing, arteriosclerotic subjects.” Atheroscl. Res., 4, 244-253.
- United States Department of Agriculture (1963) Composition of foods, raw, processed, prepared. Agriculture Handbook No. 8 US Government Printing Office, Washington.