
Access to all articles, new health classes, discounts in our store, and more!
Pain and Muscle Tension Caused by Inflammation of the Diaphragmatic Costal and Lower Parietal Pleura Simulating That From Abdominal Viscera
Read before the Seventieth Semi-Annual meeting of the Southern California Medical Association, Santa Barbara, California, April 4-5, 1924. Published in Surgery, Gynecology and Obstetrics, January 1925, pp. 62-70.
* * *
Innervation of Diaphragm and Certain Abdominal Viscera
Just as anatomy and histology are fundamental to gross and microscopic pathology, so is a knowledge of normal physiology the basis of abnormal or pathological physiology. A knowledge of vegetative neurology and the laws governing reflexes is fundamental to the interpretation of pain, increased muscle tension, and degenerative processes which result from visceral inflammation.
In this paper it is my purpose to discuss the innervation and reflex relationships of the diaphragmatic and lower parietal segments of the pleura and compare them with those of certain important abdominal viscera so as to make clear the manner in which symptoms on the part of the one may simulate those of the other and cause errors of diagnosis to be made.
The diaphragm is an organ made up of two parts: the crura and central tendon innervated almost wholly by the phrenics, and the costal portion innervated almost wholly by the intercostals. Above it is covered by pleura and below by peritoneum which share the same innervation. The lower segments of the pleura which consist of the costal portion of the diaphragmatic pleura, and the lower parietal pleura, receive innervation not only from the lower six intercostal nerves but also from sympathetic nerves, the connector fibers of which arise from the six lower thoracic segments of the cord. These same segments also send sympathetic fibers to all of the important abdominal viscera, and, together with the upper two or three lumbar segments supply sympathetic fibers to all abdominal and pelvic organs as shown in Figure 1. These same segments supply the peritoneum.
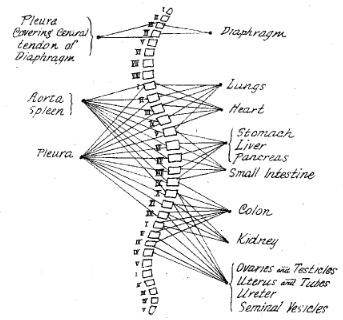
Fig. 1. The connector neurons for the important thoracic, abdominal, and pelvic viscera. In the figure the connecting neurons are those which belong to the thoracicolumbar outflow; except those going to the diaphragm, which are spinal nerves (phrenics). The motor cells for the viscera are found in the various collateral ganglia.
The figure shows that the innervation of the various viscera may be divided into groups. The heart and lungs are innervated from practically the same segments, the upper first to sixth thoracic; the stomach, liver, and pancreas from the same segments, fifth to ninth thoracic; the colon, kidney, and pelvic viscera from practically the same segments, ninth and twelfth thoracic to third and fourth lumbar.
In spite of this grouping in innervation, each organ is brought in reflex connection with efferent neurons, both sensory and motor, which are more or less definite, in such a way that the motor and sensory reflexes do not overlap as much as might be indicated.
The stomach, liver, gall bladder, pancreas, small intestine, upper colon and kidney are almost wholly innervated by sympathetic nerves, the connector fibers for which arise in the lower six thoracic segments. The aorta and spleen receive innervation from the upper six thoracic segments as well. The lower colon and pelvic viscera receive part of their innervation from the lower thoracic quadrants but part also from the upper lumbar.6
It is thus evident that there is an intimate association in the lower six thoracic segments of the cord between neurons coming from the lower segments of the diaphragm and those from all abdominal and pelvic organs and the peritoneum which affords an opportunity, according to Sherrington’s law which will be stated later, of mediating reflexes with the motor and sensory spinal nerves arising from these same lower six thoracic spinal segments. Were it not for the fact that each organ has areas of election, as we might loosely term them, for its reflexes there would be no end of confusion. In spite of the fact that the nerve impulses return from many viscera to the same segments of the cord, the impulses from each organ are most easily transmitted to motor nerves which produce muscle tension in certain definite muscles or certain parts of muscles and to sensory nerves which affect skin areas which are more or less limited and definite, and when other areas are involved the spread follows laws which are well established although not generally known.
In order to understand the role played by the nerves which arise from the lower six thoracic segments of the cord in the production of reflex symptoms when the organs which they supply are the seat of inflammatory disease, it is necessary to understand something of the developmental relationships of the various organs and to know the laws which govern the mediation of visceral afferent impulses and their expression in action in skeletal structures.
Innervation of the body follows an orderly arrangement, the exactness of which is quite remarkable. This can best be understood by considering the body as a segmental organism. This segmental nature of the human body is evident from a comparison of the primitive vertebrate–Amphioxus–and the human embryo in the early weeks of development as shown in Figures 2 and 3. In the primitive vertebrate here represented each segment is more or less independent of other segments. In man the segmental arrangement has also been preserved but individual segments are not so independent as they are in the more primitive state. Different parts are linked together more intimately as the body becomes more complicated and the nervous system becomes more complex. In the simple segmentally arranged organisms the skeletal and visceral structures belonging to each segment are innervated by that portion of the cord lying within the segment. It will be seen that the heart (Fig. 2) is located in the second, third and fourth segments; and so, it is innervated by those same segments of the cord. We know from clinical experience that when diseased the human heart expresses reflexes through somatic motor and sensory nerves arising in these segments, and that there are definite segmental arrangements between the skeletal structures and each organ. When reflexes are expressed in segments other than those usually involved even the variations follow certain physiological laws. These will be given later in this discussion. The early relationships of an organ in its developmental stages determines its innervation and, regardless of where the organ is finally situated in the body, determines the parts of the skeletal structure in which reflex symptoms (muscle tension, pain and degenerative processes) will be expressed when it is inflamed.
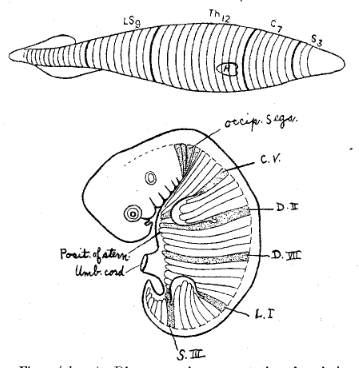
Fig. 2 (above). Diagrammatic representation of a primitive vertebrate animal–the Amphioxus–divided for convenience into three segments for the head, seven for the neck, twelve for the thorax, nine for the lumbosacral region, and an indefinite number for the coccygeal region. For clearness of comparison the heart, H, is represented as occupying the same position as in man, so that an adequate stimulus from the heart would cause pain in the distribution of the four upper thoracic nerves covering and protecting the heart. (After Ross7 and Mackenzie.4)
Fig. 3. Diagram of a human embryo, fifth week, showing the arrangement and extension of the mesoblastic segments. The first and last of each segment entering into the formation of the limbs is stippled (C. V and D. II and L. I and S. III). The position is indicated in which the sternum is formed. (A. M. Patterson.)
Laws Governing Reflexes
Reflexes follow certain physiological principles which, on account of the regularity of their operation are spoken of as the “laws of the reflexes.” An understanding of these is necessary to the interpretation of many symptoms met in clinical practice. The following are some of the more common laws.
- Afferent nerves from the viscera carry normal stimuli centralward during health which result in physiological action; and abnormal stimuli when the organs are diseased which result in symptoms. There is an inhibition exerted normally by higher centers which prevents impulses returning from the viscera from producing undue reflex action, and keeps reaction within physiological limits. When the impulse is stronger, however, and adequate to break down whatever resistance is offered, then such abnormal or exaggerated reaction occurs as is recognized as symptoms of disease. So that what is known as an adequate stimulus6 is essential to the production of a reflex symptom.
- Sherrington8 suggested it as a law of reflexes that each afferent nerve finds in the same segment of the cord which it enters an efferent nerve which mediates with it as readily or more readily than nerves arising in any other segment. This holds for all of the important viscera except the lung. The fact that the lung differs calls for a modification of the law. So I have suggested that the law be modified to meet the conditions of all viscera, as follows: Every afferent nerve finds in the segment of the cord with which the viscus which it supplies is connected developmentally an efferent neuron which mediates with it as readily or more readily than efferent neurons in other segments. This means the connection is in the same segment as suggested by Sherrington for all important viscera except the lung. The exception on the part of the lung is based on the embryological fact that it develops as the most anterior of all important viscera and arises in the pharynx from a diverticulum given off from the anterior portion of the oesophagus.
- When a nerve fibril is stimulated to action no amount of increased stimulus can cause it to produce greater action (Lucas,3 Ver Worn9). Increase in the stimulus, however, is manifested by a spread of the impulse to neighboring neurons and results in a wider spread of the action. This fact must be taken into consideration in estimating the origin of visceromotor and viscerosensory reflexes. An overlapping of reflexes is often met in clinical practice which would be inexplicable if it were not for an understanding of this law.
- While referred sensory disturbance is not a true reflex in the physiological sense of the term, clinically it may be so treated. Consequently, it is necessary to note that pain arising in viscera is not expressed in the organs themselves, but in the more highly sensitive somatic neurons which supply the superficial structures, skin, subcutaneous tissue, and muscles. The nerves which transmit pain to the surface of the body in diseased states are those whose cell bodies lie adjacent in the cord to the cell bodies of the neurons which bring the impulse from the viscus affected. This law has been expressed by Head1 as follows: “When a painful stimulus is applied to a part of low sensibility in close central connection with a part of much greater sensibility, the pain produced is felt in the part of higher sensibility rather than in the part of lower sensibility to which the stimulus was actually applied.”
Discussion of Laws of Reflexes
If one will understand the reflex motor, sensory and trophic symptoms of disease, he must be familiar with these four laws. The adequate stimulus must be understood. Afferent impulses are constantly being carried centralward from the viscera, in conditions of health which result in normal reflex action, but which in conditions of disease result in pathological reflex action. Before such pathological action can be brought about, however, it is necessary for the resistance between the afferent and the efferent nerve components to be broken down. This resistance differs in different individuals; consequently, the strength of the impulse necessary to disturb nerve balance and bring about reflex action differs in different individuals. One patient will show a reflex symptom when another under apparently the same circumstance will not.
The second law, the law of Sherrington as modified by myself, explains the location of the reflex but must be considered in connection with the third law in order to explain fully what tissues may be involved in reflex action. For example, angina pectoris as a rule is expressed in the first, second, and third thoracic segments on the left side; but with intense stimuli such as occurs when the attack is unusually severe, it may be transferred to neurons across the cord and be expressed on the right side of the body, or it may be transmitted upward in the cord to the cervical segments and be expressed in those tissues supplied by the cervical nerves; or, less commonly downward into tissues supplied by neurons arising lower in the cord. The same is true with disease of the stomach, liver and gall bladder, appendix, kidney, and every other organ. While there is a definite narrow path through which the reflex is usually expressed, with increased stimulation it may spread upward or downward in the cord and produce reflexes in what would be considered unusual areas if this law were not understood.
The character of the pain expressed when viscera are inflamed has given rise to considerable discussion. The best opinion, however, is that of Ross,7 Mackenzie,4 Head,1 and Lennander2 and is to the effect that the pain is not expressed in the viscus itself, but in the superficial structures of the body supplied by sensory neurons whose cell bodies in the cord lie adjacent to those of the neurons which are stimulated by the disease in the organ, according to the fourth law above. It is a physiological law that tissues form a defensive mechanism which protects them against all harmful impulses with which they naturally come in contact. But internal viscera, being protected by the superficial structures have been shielded from most ordinary injurious influences, so they are insensitive to many stimuli which cause reaction in the superficial tissues. Viscera, however, are provided with a mechanism by which they express pain and other altered sensation in the superficial structures of the body, the location of which is determined by the segmental nature of the body and the close proximity existing intrasegmentally between the neurons which supply the viscera and those which supply the surface of the body.
Motor, Sensory, and Trophic Reflexes from the Diaphragmatic and Lower Costal Pleura
I shall now attempt to clearly set forth the reflex symptoms which result from inflammation of the diaphragmatic and lower costal segments of the pleura and to show the tissues in which they are usually expressed. At the same time I shall also show how these symptoms, under extraordinary conditions, following the laws of reflexes, sometimes extend to tissues in other areas, particularly over the abdomen and under such circumstance simulate symptoms of disease of the abdominal viscera.
As previously mentioned the diaphragm is a dual organ, being composed of: (1) the crura and central tendon innervated almost wholly by the phrenic nerves which arise from the third and fourth, or fourth and fifth cervical segments of the.cord and which produce reflex symptoms, particularly pain, in the neck and shoulders, in those tissues supplied by somatic sensory nerves which arise in the third, fourth, and fifth cervical segments of the cord; and (2) a costal portion innervated almost wholly by the lower six intercostal nerves, which express reflex symptoms in tissues supplied by these same nerves.
The pleura overlying the diaphragm has not only the same innervation of the diaphragm itself, but also is further supplied with sympathetic nerves from the lower six thoracic segments. The lower parietal pleura has the same innervation and the same location of reflexes as the diaphragmatic pleura.
When the lower parietal pleura and the costal portion of the diaphragmatic pleura are acutely inflamed, they produce tension of the intercostal muscles and pain in the tissues which as a rule immediately overlie the seat of inflammation. Under exceptional circumstances both the muscle tension and pain may extend below the costal margin and spread out over the abdomen. If the inflammation passes over into a chronic state and results in adhesions, then atrophy results in those tissues which show muscle tension and pain during the acute stage of the disease. Areas of atrophy of the skin and subcutaneous tissues are commonly found on inspection and palpation overlying pleural segments which have been the seat of chronic inflammation, particularly those which have resulted in adhesions. When one has learned to appreciate the importance of this trophic reflex, he will not be surprised at the recurrent pain of which these patients complain in the area affected, for the sensory neurons affected become hyperirritable and respond to stimuli of less than normal strength.
Figure 4 (A and B) shows the usual as well as unusual areas involved in reflexes when these portions of the pleura are inflamed. The phrenic nerves supply the crura and central tendon of the diaphragm and possibly send filaments to the overlying diaphragmatic pleura and diaphragmatic peritoneum. It also sends filaments to the capsule of the liver. This must be kept in mind in differentiating inflammation of viscera in this region, as will appear more fully as our discussion proceeds.
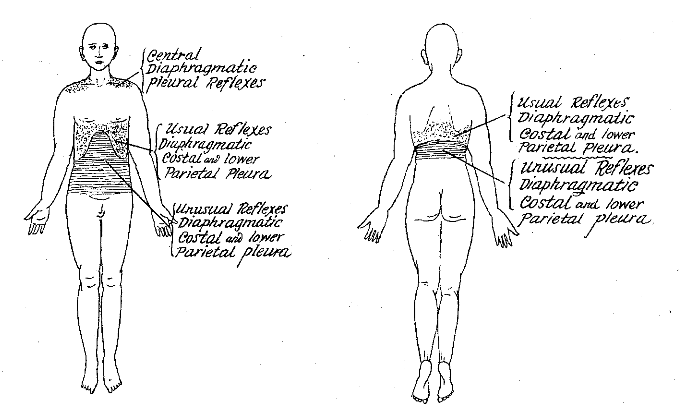
Fig. 4 (A and B). Dotted area above lower costal margin, usual area of reflexes from diaphragmatic costal and lower parietal pleura. Horizontal lines below costal margin, areas to which reflexes from diaphragmatic costal and lower parietal pleura may extend. Dotted area in cervical region, area of reflexes from the central portion of diaphragmatic pleura.
It is the reflex symptoms arising from the costal portion of the diaphragmatic pleura and the lower parietal pleura, however, that I wish to discuss more fully in this paper. While each viscus, according to Sherrington’s law, has certain tissues in which it expresses its reflexes most readily, yet not uncommonly under great stimulation the area of reflex action is widened so that we often find, in studying inflammation involving the pleura at the base, that the reflexes extend down over the abdominal wall in the areas where abdominal organs regularly express their reflexes.
Usual Location of Reflexes from Abdominal Organs
Referring to Figure 1, it will be seen that the stomach, liver, pancreas and small intestine are supplied by sympathetic fibers from that portion of the cord between the fifth and the ninth thoracic segments inclusive. On the surface of the body reflexes from these organs are expressed regularly through motor and sensory nerves arising from the fifth to the ninth thoracic segments of the cord inclusive. The preponderant path of the reflexes, as shown in Figure 2, however, is in neurons arising in the sixth and seventh segments, the liver and gall bladder expressing their symptoms on the right side of the body, and the stomach and pancreas on the left. Figure 5 (A and B) shows the usual as well as the unusual location of reflexes for the principal abdominal viscera.
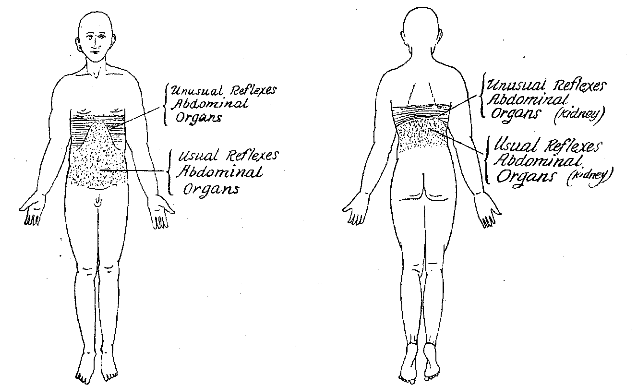
Fig. 5 (A and B). Dotted area below lower costal margin, usual areas of reflexes from abdominal viscera. Horizontal lines above lower costal margin, areas to which reflexes from abdominal viscera may extend.
It readily can be seen how a pleurisy arising in the costal portion of the diaphragmatic pleura or the lower parietal pleura might extend down over the abdomen and, expressing increased muscle tension and pain immediately below the costal margin, be mistaken for inflammation in some abdominal organ. This is all the more apparent from the fact that when the liver is involved as when the central tendon of the diaphragm is involved, the pain may extend through the phrenics and be expressed in the neck and shoulder on the right side. Under these circumstances there would be reflex symptoms, probably muscle tension and pain below the right costal border and pain in the shoulder, all of which could be produced either by inflammation of the pleura or inflammation of the abdominal organ. Likewise, on the left side, ulceration of the stomach, particularly if it results in adhesions to the diaphragm, causes not only increased muscle tension and pain in the area immediately below the costal border, but quite often pain in the neck and shoulder on the left side. Acute pancreatitis is accompanied by such intense stimuli that it usually causes a wide-spread area of reflexes extending throughout a great portion of both thoracic and cervical segments. Reflexes arising in these organs are expressed in the same areas as those from the adjoining pleura and at times require careful consideration for their differentiation.
The small intestine reflects most readily in the eighth, ninth, and tenth segments, and the pain is usually expressed around and above the navel. Sometimes inflammation of the lower segments of the pleura will give pain extending into this area.
The appendix and the ascending colon usually show tension of the muscles and pain in the right lower quadrant of the abdomen. Pleurisy on the right side involving the costal portion of the diaphragmatic pleura and the lower parietal pleura not infrequently expresses itself in pain in this same region.
The colon is supplied by sympathetic nerves which arise in that portion of the cord represented by the segments from the ninth thoracic to the third or fourth lumbar inclusive. Pain expressed by the colon varies in its location. It may be on the right side of the body in the upper or lower quadrant; it may be on the left side–either in the upper or lower quadrant; or, it may be below the umbilicus extending across the abdomen.
Not infrequently do we see inflammation of the lower segments of the pleura giving pain over these same areas. I have frequently seen pain of pleural origin extend down over the abdomen. While I have often seen muscle tension in the upper part of the abdomen below the costal arch resulting from pleurisy, I have never recognized definite muscle tension in the lower abdominal segments.
The kidney receives innervation from that portion of the cord embraced between the tenth thoracic and the third or fourth lumbar segments. The muscle reflex from the kidney as described by me5,6 is expressed posteriorly in the lumbar muscles. Pain may be expressed in the lumbar region posteriorly, or in the front of the abdomen below the umbilicus and running down over the upper areas of the thighs. Not infrequently does pain arising in the posterior segments of the diaphragmatic and lower parietal pleura extend down over the same areas in the back as are involved in pain from the kidney.
One must not forget that even the pelvic organs receive part of their innervation from the lower thoracic segments–the tenth, eleventh, and twelfth–as well as from the upper lumbar, and that pain from the pleura may occur in the lower abdominal areas in which the pelvic organs express pain.
Subacute and Chronic Pain Caused by Inflammation of the Pleura and Abdominal Viscera
In clinical practice the diagnostician often meets patients who are complaining of recurrent pain.. It is not necessarily sharp; in fact, most of the time it is dull. The examiner failing to find an acute condition at the time is too apt to consider the subject as a malingerer. In order to understand this type of pain it is but necessary to appreciate the fact that long continued irritation may so injure neurons that they pass into a state of hyperirritability and react (showing pain in the instances under discussion) to a stimulus of much lesser magnitude than that normally withstood. This condition of the neurons may exist for a long period of time, often years, after the acute inflammation has subsided. I see a great many patients who show pain of this type. Unless the condition is properly explained to them they are apt to go from one physician to another, or have one operation after another–all without avail because the underlying facts have not been recognized. Such pain recurs under many different circumstances. In order to grasp what occurs in the production of discomfort in these patients one must realize that the organism is required to adapt itself to every unusual stimulation to which it is subjected. Thus a continuous adaptation takes place during life to such conditions as changes in weather, such as heat, cold, dampness, dryness, wind, calm, light, darkness, fog, and barometric changes; psychical stimuli such as fear, anger, worry, unhappiness and joy, fatigue, overwork, toxins, other effects of disease, the menstrual cycle, and myriads of other conditions that require marked adjustment. Patients who have hyperirritable neurons either generally or in special areas as a result of some previous organic disease adjust but poorly and consequently suffer unduly from discomfort and pain when required to make adjustment. The location of the pain differs with different organs, and in many instances is widespread. The repeated recurrence of the pain is one of the most disappointing and discouraging factors connected with it.
Discussion
I am calling attention to the reflexes which arise when the lower segments of the pleura are inflamed, and showing how they may overlap the areas involved when the abdominal viscera are inflamed, because in studying diseases of the chest I frequently see pleural reflexes which are mistaken for acute abdominal conditions. Every year numbers of patients come under my observation who have been operated on for supposed inflammation of abdominal viscera when the symptoms were due to pleural inflammation. Likewise I see others who, suffering from diseases of the upper abdominal viscera, believe their lungs to be involved because of the pain which they feel over the lower costal areas.
From our discussion it is evident that there are certain muscles or certain parts of muscles and certain skin and subcutaneous tissue segments which are more intimately connected reflexly with each internal viscus than others; and further, that it is in these particular tissues that each viscus shows the preponderance of its reflexes. It is further evident from the discussion and can be seen in the illustrations that the areas subject to reflexes for each organ are much more extensive than those which usually show the reflexes. If the reflexes arising in each organ were confined to the tissues which are most prone to show reflexes from that organ, there would be little difficulty in recognizing the origin of the stimulation; but unfortunately for diagnosis there is such an intimate correlation and integration of action through the nervous system that reflexes have a tendency to spread to many neurons instead of being confined to those which are most intimately connected with each organ.
If muscle tension and pain were always located above the diaphragm for pleural involvement, and below the diaphragm for inflammation of abdominal viscera, there would be less difficulty of diagnosis; but with the same intercostal nerves supplying the tissues both above and below the costal border the conditions are present for considerable confusion.
Until one has given considerable study to the innervation of these various tissues and familiarized himself with their developmental relationships, it is difficult for him to conceive of how one organ can reflect in a certain muscle or portion of a muscle and not involve other muscles or other portions of the same muscle when the filaments which innervate the entire mass are contained in the same nerve trunk. This is clarified, however, by an understanding of developmental and embryological facts.
I have emphasized above that inflammation of the costal portion of the diaphragmatic pleura and the lower parietal pleura may show reflex symptoms over the abdomen, simulating inflammation of abdominal viscera. It is just as necessary to know that inflammation of abdominal viscera may show reflexes in tissues above the lower costal margin. This is particularly true of the pain reflex (referred pain). Not uncommonly do we find pain over the lower portion of the left side of the chest in patients who are suffering from distention of the stomach with gas, and over the lower portion of the right side of the chest when the patient is suffering from a diseased condition in the liver. The kidney produces pain which is felt over the lower costal areas; so does the descending colon. It is necessary for the diagnostician to understand thoroughly this intimate relationship if he wishes to accurately determine the origin of these reflex symptoms.
There are several acute conditions in which we find the reflex symptoms from the pleura extending over the abdomen which should be especially emphasized, because the symptoms are so apt to lead to operative measures for some supposedly acute abdominal condition at a time when the patient is already seriously ill and unable to withstand the tax of an operation. An instance is the pain which sometimes appears in patients with severe pulmonary hemorrhage, in which the blood trickles down into the finer bronchi at the base of the lung and settles over the pleura, causing an inflammatory reaction. This condition is often accompanied by acute pain which not infrequently extends downward and is felt over the upper abdomen. If the inflammation is severe, quite frequently tension of the upper abdominal muscles is also present. The same thing occurs occasionally now and then in pneumothorax–either spontaneous or induced–probably as a result of stretching or tearing of adhesions in the lower pleural segments. It is also met now and then in cases of acute pleurisy accompanying pneumonia and in pericarditis.
In calling attention to the confusion which occurs in differentiating supradiaphragmatic and infradiaphragmatic reflexes, and by showing the innervation of the viscera responsible for them and the nerve paths through which they are expressed, and further, by discussing the laws which govern reflex action, it is hoped that differential diagnoses in this important area may be aided.
References Cited:
- Head, Henry: Studies in Neurology. London: Oxford University Press, 1920.
- Lennander, K. G.: “Beobachtungen ueber die Sensibilitaet in der Bauchhoele.” Mitt. a. d. Grenzgeb. d. Med. u. Chir., x, Nos. 1 and 2.
- Lucas, Keith: The Conduction of the Nervous Impulse. New York: Longmans, Green & Co., 1917.
- Mackenzie, Sir James: Symptoms and Their Interpretation. London: Shaw & Son, 1909.
- Pottenger, F. M.: “Spasm of lumbar muscles; a diagnostic sign.” J. Am. M. Ass., 1913, lx, 980.
- Idem: Symptoms of Visceral Disease. St. Louis, Missouri: C. V. Mosby Company, 1922.
- Ross, J.: “On the segmental distribution of sensory disorders.” Brain, 1888, x, 333-344.
- Sherrington, C. S.: The Integrative Action of the Nervous System. New York: Charles Scribner & Sons, 1906.
- Ver Worn, Max: Irritability. New Haven: Yale University Press, 1913.