
Access to all articles, new health classes, discounts in our store, and more!
Oral Manifestations of Systemic Diseases
Read at the 46th Annual Meeting of the John A. Andrew Clinical Society, Tuskegee Institute, Alabama, April 13-16, 1958. Published in Journal of the National Medical Association, Vol. 50, No. 4, pp. 241-247, July 1958.
* * *
The fact is well established, if one surveys the standard texts,1-11 that there are approximately 200 systemic disorders which are accompanied by oral symptoms and/or signs. In a sizable number of instances, the oral clues are the first and sometimes even the only evidence of a disturbed state. Among the classic examples are the much described Koplik’s spots in the buccal mucosa which precede, by about 24 or so hours, the cutaneous eruption of measles.12 It follows that the recognition of this highly pathognomic lesion is helpful in the early detection of what might otherwise, at that early stage, be a rather nonspecific prodromal picture of a host of disorders. In other cases, the oral symptoms and/or signs may parallel, not precede, the complaints and clues elsewhere in the body. Thus, the simultaneous development of an erosive lesion on the buccal mucosa near the angle of the lip along with a butterfly dermatosis on the face is certainly presumptive proof for lupus erythematosus.13 Lastly, in still other situations, the oral reflections follow, rather than precede or parallel, evidence in other parts of the body. For example, in pemphigus,14 bullae may erupt on the skin days, weeks, or months before oral ulcers can be demonstrated.
From what has just been said, it is clear that the examination of the oral cavity can indeed contribute to the detection of systemic disease. The use of the mouth as a diagnostic zone is heightened by the fact that there are few other regions of the body which can be examined more easily and with fewer tools and less training. It is an easily demonstrable fact that the oral cavity can be surveyed in a matter of seconds under bright illumination with just the aid of a tongue blade.
Diagnostic Importance of the Oral Cavity
The question frequently posed as precisely why the oral cavity is so important a diagnostic area. This is so because: 1) the oral cavity contains derivatives of all of the primary germinal layers, and 2) the mouth includes tissues not demonstrable anywhere else in man.
Similarities Between the Mouth and Other Organs
It is well established that diseases which affect other regions can also involve the oral tissues. This is so because the oral, vaginal, and rectal mucosae and the skin are developmentally related. Thus, it is a fact that generalized cutaneous and mucosal disturbances may show oral reflections. Next, there are cartilage, bone, fat, and the other connective tissue cousins well represented in the mouth. It is, therefore, not at all surprising that disorders of lipid metabolism, the reticuloendothelial diseases, collagen pathoses, and osteodystrophic problems have their representation in the tissues of the mouth.
The important point to be underscored is that the oral cavity is made up of the same cell types and cellular aggregates found throughout the body. It follows that the afflictions will be much the same.
Differences Between the Mouth and Other Organs
On the one hand, there are special cells and tissues in the oral cavity. The mouth is different both structurally and functionally.
Structural Differences: The anatomy which makes the mouth so unique includes: 1) the temporomandibular joint, and 2) the presence of teeth and their associated periodontal tissues.
The Temporomandibular Joint: As an articulation, the temporomandibular area is subject to all of the problems encountered in other joints. This is amply shown by the fact that rheumatoid arthritis, osteoarthritis, and the infectious arthritides involve the temporomandibular joint just as they afflict the interphalangeal spaces, the elbow, or the back. At the same time, the temporomandibular joint is a special articulation because: 1) it is, in effect, two joints, 2) it is the only articulation where the right joint must always know what the left is doing, and 3) it is the only joint in the body which is at the mercy of the teeth.15
The Odontogenic Apparatus: The most obvious special feature of the oral cavity is the presence of the teeth and associated periodontal structures. Actually, though it is not well popularized, this mechanism is one of the most sensitive in the human body. For instance, the thickness of sheets of paper, differing from each other by a few thousandths of an inch, can be recognized by biting down upon them.16 This is so because of a very delicate proprioceptive system housed within the periodontal membrane which surrounds the teeth and a similar apparatus built into the muscles of mastication.
Functional Differences: The oral tissues are unique in that they are asked to cope with trauma which one would ordinarily not expect of most tissues. For example, in one breath the oral mucosa is subjected to boiling coffee and freezing ice cream. Surprisingly enough, the oral tissues survive–but only when the substrate is in good health. Thus it is that the slightest systemic imbalance will lead to changes in the mouth before lesions will be demonstrable elsewhere. The reasons for this sequence of events are now clear.
The evidence is now abundant that disease, in general, is a function of the product of an appropriate systemic substrate and local irritating factors.17,18,19 For example, pellagra may first become clinically evident as a dermatitis after exposure to the sun. Surely, the patient was just as pellagrous before actinic exposure.
For the reasons just cited, the mouth may be regarded as an excellent barometer of systemic disease. It is, therefore, quite understandable why approximately 200 systemic diseases may show oral manifestations.
It is impossible to list, let alone discuss, all of these systemic disorders with oral manifestations. Rather, an attempt will be made to underscore, by example, the role of the oral cavity in the detection of systemic disease.
Case Reports
Representative illustrations will be discussed to bring into focus the oral reflections of infectious disease, chemical intoxication, hormonal imbalance, and the nutritional deficiency state.
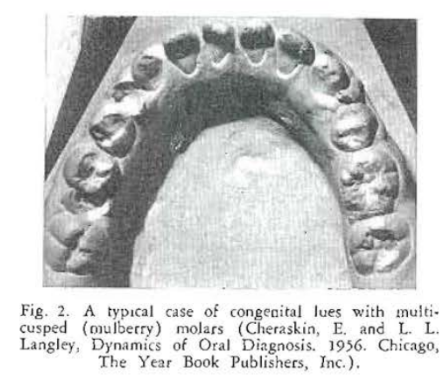
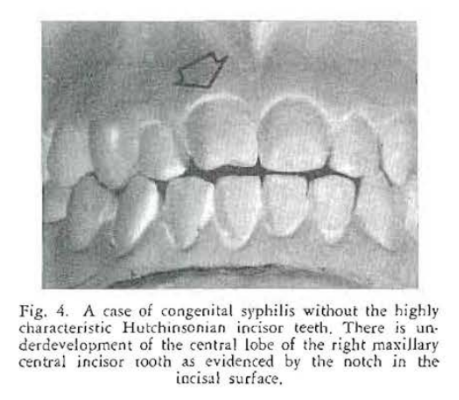
Case Report No. 1: Mention is made in almost every standard textbook20,21 of the classical signs of congenital syphilis. Thus, there is frequent reference to the typical screwdriver-shaped anterior teeth (Hutchinsonian incisors), cuspuled posterior teeth (mulberry molars), and the disturbance in occlusion of the anterior teeth (medial openbite). Figures 1-3 show such a case. It is true that these are the classical oral findings in congenital lues. One gains the impression that they are, therefore, common observations. The fact of the matter is that Hutchinsonian incisor teeth and mulberry molars are noted in about two-thirds of all cases of congenital lues. Medial openbite is encountered in about one out of every three cases. Interestingly enough, a shortened first molar is present in over 90 percent of such patients22 (Figs. 4 and 5).
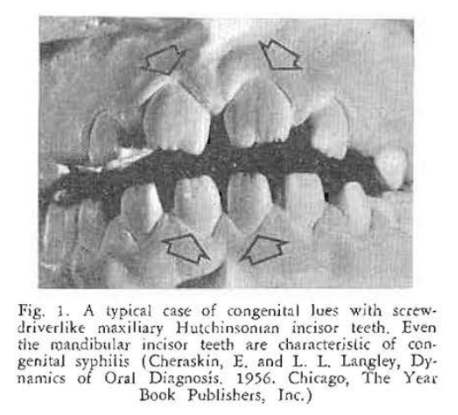
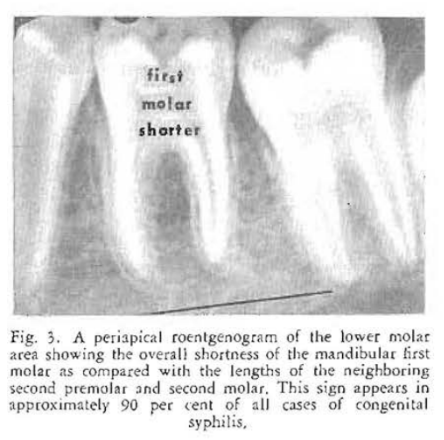
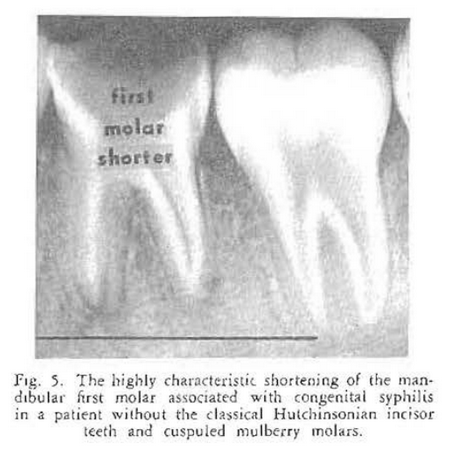
Congenital syphilis provides an excellent opportunity to show that infectious diseases do have oral counterparts. More important, it demonstrates that oral signs, easily detected, may occur in an overwhelming percentage of the cases. In this particular instance, there is no other known sign which occurs with the regularity that one encounters shortened first molar teeth.
Case Report No. 2: This case to be reported now differs from the preceding one in several respects: 1) congenital syphilis is not a common disease compared to tapeworm infestations, and 2) less information is available about the oral manifestations of cysticercosis.1
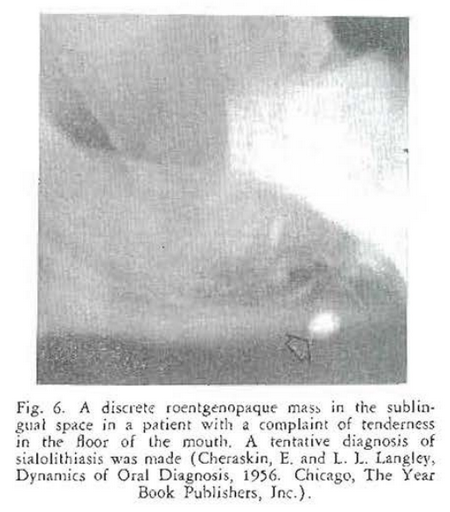
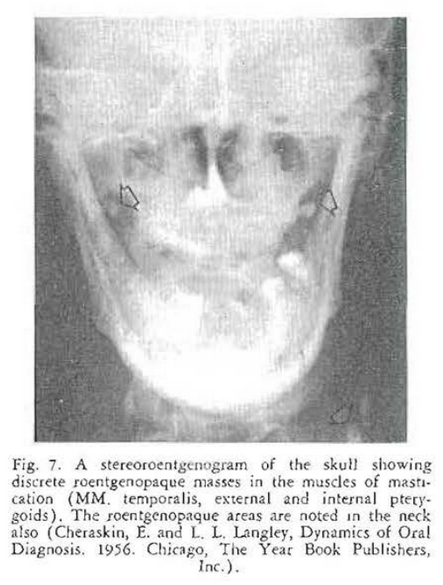
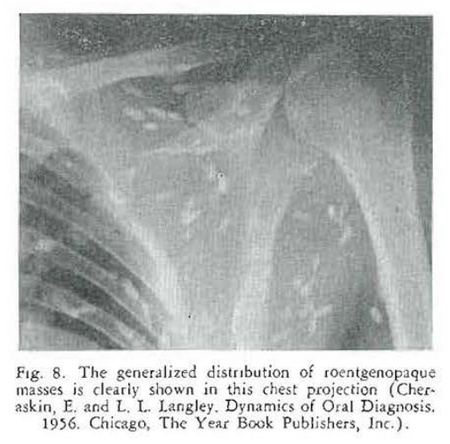
This is the story of an elderly gentleman who presents himself in the clinic with a chief complaint of soreness and tenderness in the floor of the mouth. Oral as well as physical examination is essentially negative except for tenderness in the sublingual space–in the general area of the distribution of Wharton’s duct. A lateral jaw roentgenogram (Fig. 6) confirmed the original tentative diagnosis of sialolithiasis–a salivary stone in Wharton’s duct as shown by the discrete, roentgenolucent shadow. However, additional skull (Fig. 7) and other roentgenograms (Figs. 8 and 9) indicated that this patient was probably suffering with something much different from sialolithiasis. Biopsy confirmed the suspicion of cysticercosis.

Case Report No. 3: Chemical intoxication, and particularly lead poisoning,23,24 is a common occurrence. Sometimes the chemical agent is acquired occupationally. Occasionally, an agent is taken for suicidal purposes. Quite often, the problem is iatrogenic in that the patient is given the agent for medicinal purposes. Finally, the problem may be a social one as it was in the case to be reported.
This is the story of a young man who reported to the clinic because of abdominal pain. The symptoms and signs were unequivocally those of a peptic ulcer. However, before a gastrointestinal series was performed and as part of his initial examination, the oral cavity was inspected. A blue-black, thin, pigmented line was observed in the free marginal gingiva in the neighborhood of a lower molar tooth (Fig. 10). This led the examiner to take a more detailed history. It was then learned that the patient had been making spirits in an old radiator. Examination of the blood confirmed the suspicion of plumbism.
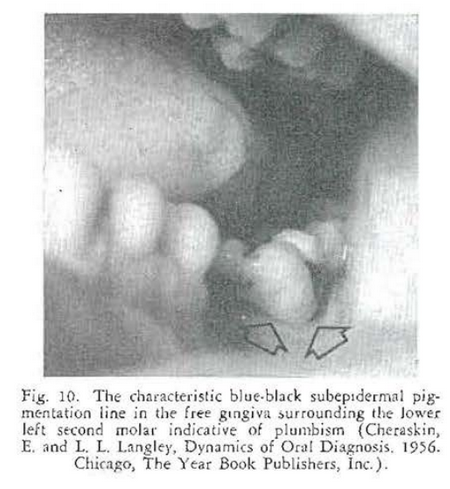
It is clear that, in diseased tissue, hydrogen sulphide is produced. In the presence of a circulating heavy metal in the bloodstream, the metaI unites with the hydrogen sulphide. In this particular case, the molar (Fig. 10) stood alone. This meant that it was under excessive trauma since it was being expected to carry the occlusal load ordinarily shared by other teeth not present in the arch in this patient. Thus, hydrogen sulphide was being produced in the tissues which united with the circulating lead. This is the explanation for the blue-black deposition of lead sulphide in the marginal gingiva.
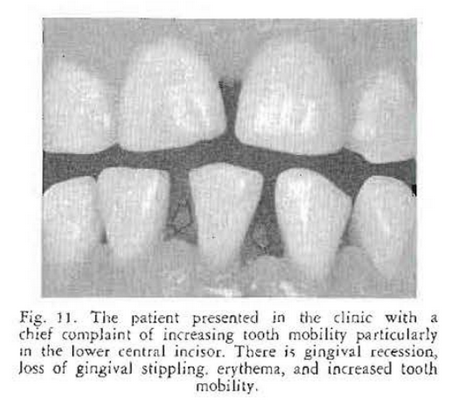
Case Report No. 4: This is the story of a young lady who presents in the clinic with a chief complaint of increasing tooth mobility. She had visited several physicians and dentists who had all agreed that the patient was suffering with so-called “idiopathic pyorrhea”. The joint recommendation was made that she have full mouth extraction of her teeth and full denture prostheses.
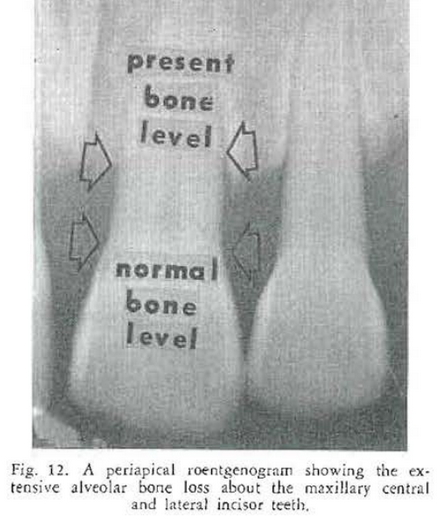
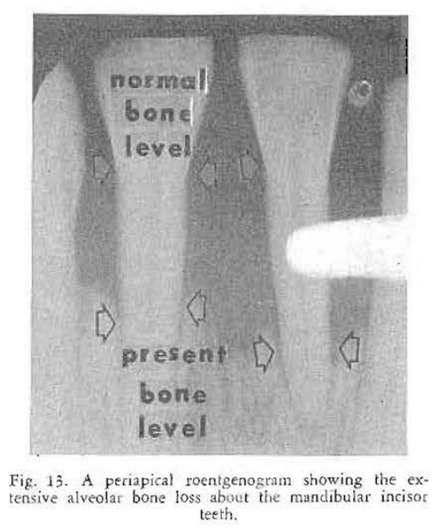
Examination at the clinic revealed evidence of a disturbance in the periodontal tissues. There were gingival recession, loss of gingival stippling, erythema, and tooth mobility especially in the lower central incisor (Fig. 11). Examination of the roentgenograms of the upper (Fig. 12) and lower (Fig. 13) teeth showed moderate alveolar bone loss. The personal past and family history were negative.
As part of a research project on the relationship of alveolar bone loss and diabetes mellitus, a glucose tolerance test was performed. It can be seen (Fig. 14} that the fasting blood sugar and urinalysis were within normal limits. However, the general pattern of the curve was suggestive of diabetes mellitus. She was referred to the Diabetic Clinic where a special diabetic diet was recommended, One month later she returned to the dental clinic reporting great improvement at the symptom level. She had noted that she “felt much better” and that tooth mobility had disappeared.
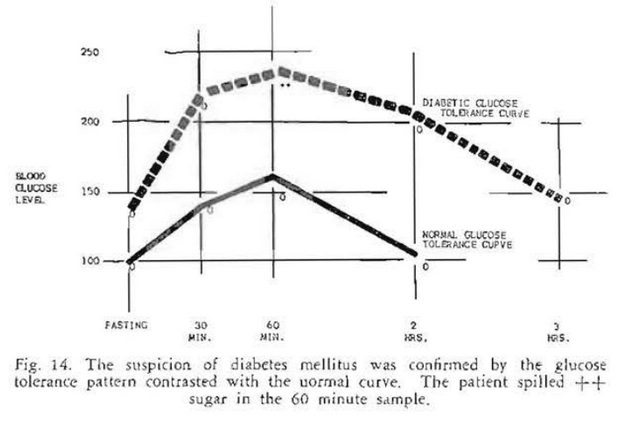
Parenthetic mention should be made that the first clinical evidence of diabetes mellitus may be by way of oral symptoms and signs.25,26
Case Report No. 5: Nutritional problems often make their clinical debut by way of oral symptoms and signs.27-30 This case report emphasizes that relationship.
A young lady reported to the clinic with a story of a strange tongue pattern of about nine years’ duration. She had consulted a number of doctors who had all agreed that the lingual picture was that of geographic tongue (Fig. 15). The personal past history was negative.
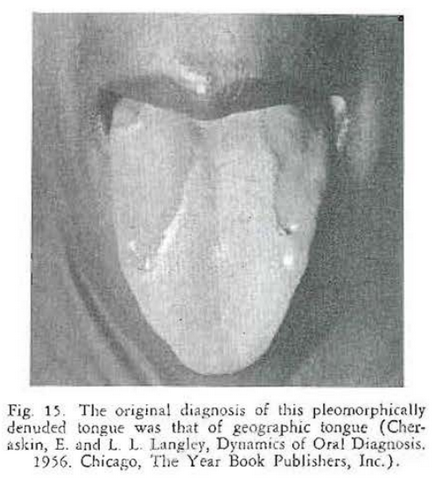
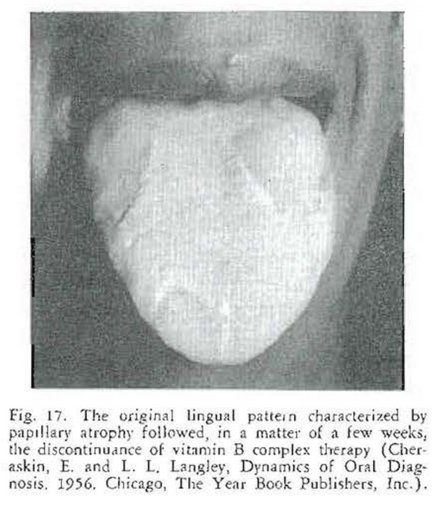
Examination of the oral cavity was essentially negative. Areas of the tongue were found to show atrophy of the papillae. She was given a trial dose with vitamin B complex. In one week, papillae were evenly distributed on the dorsum of the tongue (Fig. 16). The medication was withdrawn. A short time later the tongue lesions had appeared (Fig. 17).
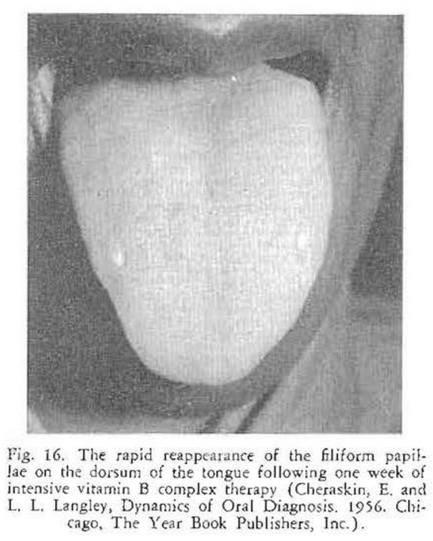
This case is of particular interest because it shows how rapidly changes can occur in the oral tissues. It should be recalled that, in a matter of days, the filiform papillae developed.
Summary
- There are approximately 200 systemic diseases which are accompanied by oral symptoms and/or signs. The oral reflections may precede, parallel, or follow symptoms and signs elsewhere.
- Disease is a product of a suitable systemic substrate and an appropriate local factor. Since trauma is ordinarily high in the mouth, it follows that oral symptoms and./or signs may be the first evidence of a systemic disturbance.
- Five case reports are included to emphasize the role of the oral cavity in the detection of systemic disease.
References Cited:
- Cheraskin, E. and L. L. Langley. Dynamics of Oral Diagnosis. The Year Book Publishers, Inc., Chicago, 1956.
- Miller, S. C. Oral Diagnosis and Treatment. Blakiston Co., N. Y., 2nd Ed., 1950.
- Thoma, K. H. and H. B. G. Robinson. Oral and Dental Diagnosis. W. B. Saunders Co., Phila., 4th Ed., 1955.
- Burket, L. W. Oral Medicine. J. B. Lippincott Co., Phila., 2nd Ed., 1952.
- Bernier, J. L. The Management of Oral Disease, C. V. Mosby Co., St. Louis, 1955.
- Thoma, K. H. Oral Pathology. C. V. Mosby Co., St. Louis, 4th Ed., 1954.
- Stones, H. H. Oral and Dental Diseases. E. and S. Livingstone Ltd., Edinburgh, 3rd Ed., 1954.
- Comroe, B. I. and L. H. Collins and M. P. Crane. Internal Medicine in Dental Practice. Lea and Febiger, Phila., 4th Ed., 1954.
- Orban, B. J. and F. M. Wentz. Atlas of Clinical Pathology of the Oral Mucous Membrane. C. V. Mosby Co., St. Louis, 1955.
- United States Naval Dental School. Color Atlas of Oral Pathology, J. B. Lippincott Co., Phila., 1956.
- Glickman, I. Clinical Periodontology. W. B. Saunders Co., Phila., 1953.
- Koplik, H. “Diagnosis of the Invasion of Measles, from a Study of the Exanthema as it appears on the Buccal Mucous Membrane.” Arch. Pediat. 13: 918-922, 1896.
- Tumulty, P. A. “The Clinical Course of Lupus Erythematosus.” J.A.M.A., 156:947-953, 1954.
- Dean, R. D. and M. T. Dean. “Gingival Symptom Complexes.” Am. J. Orthodont. and Oral Surg. (Oral Surg. Sect.) 31:473-486, 1945.
- Sicher, H. Oral Anatomy. C. V. Mosby Co., St. Louis, 2nd Ed., pp. 157-177, 1952.
- Langley, L. L. and E. Cheraskin. The Physiological Foundation of Dental Practice. C. V. Mosby Co., St. Louis, 2nd Ed., 1956.
- Johnson, R. E. and R. C. Darling, W. H. Forbes, L. Brouha, E. Egana and A. Graybiel. “The Effects of a Diet Deficient in Part of the Vitamin B Complex upon Men Doing Manual Labor.” J. Nutrition, 24: 585-596, 1942.
- Follis, R. H., Jr. “Effect of Mechanical Force on the Skeletal Lesions in Acute Scurvy in Guinea Pigs.” Arch. Path., 35: 579-582, 1943.
- Cheraskin, E. “Preventive Medical Case-finding Opportunities and Responsibilities of the Dentist.” Dent. Clin. North America (in press).
- Harrison, T. R. Principles of Internal Medicine. Blakiston Co., New York, 2nd Ed., pp. 1015-1016, 1954.
- Cecil, H. L. and R. F. Loeb. A Textbook of Medicine. W. B. Saunders Co., Phila., 9th Ed., pp, 351-352, 1955.
- McCormick, J. “Congenital Syphilis.” Ala. Dent. Rev., 3: no. 1, 16-23, 1954; 3: no. 2, 3-9, 1955; 3: no. 3, 3-7, 1955.
- Aston, E. R. “Dental Study of Employees of Five Lead Plants.” Indust. Med. and Surg., 21: 17-20, 1952.
- Levy, A. T. “Plumbism: Report of a Case.” J.A.D.A., 30:863-864, 1943.
- Knishkowsky, E. and P. Person and H. Pollock. “The Mouth in Diabetes Mellitus.” J. Mt. Sinai Hosp., N. Y., 17: 192-202, 1950.
- Rudy, A. and M. M. Cohen. “The Oral Aspects of Diabetes Mellitus.” New Eng. J Med., 219:503- 505, 1938.
- Mann, A. W. and T. D. Spies and M. Springer. “Oral Manifestations of Vitamin B Complex Deficiencies.” J. Dent. Res., 29: 269-270, 1941.
- Bakwin, H. and H. W. Reardon, J. S. Winn, M. S. Tenbrink, M. L. Stern and M. G. Engel. “Relation of Lesions of the Tongue in Children to Niacin Deficiency.” Am. J. Dis. Child., 74:657-668, 1947.
- Kruse, H. D. “The Lingual Manifestations of Aniacinosis, with Special Consideration of the Detection of Early Changes by Biomicroscopy.” Milbank Mem. Fund Quarterly, 20:262-286. 1942.
- Mueller, J. F. and R. W. Vilter. “Pyridoxine Deficiency in Human Beings Induced with Deoxypyridoxine.” J. Clin. Invest. 29: 193-201, 1950.