
Access to all articles, new health classes, discounts in our store, and more!
Newer Data for Establishing a Basis for Judgment Regarding Focal Infection With Special Consideration for Child Welfare
Stenographic report of a lecture read before the Northern Ohio Dental Association, Cleveland, Ohio, June 1924.
* * *
I assure you I feel it a very great honor to be given an opportunity to follow up the splendid addresses that have been rendered the last few days, and I shall try briefly to put into practical form for you some of the splendid lessons given to us by the previous speakers, together with the researches that we have been carrying on in our work.
I want you first to keep in mind that it is impossible, in the short space of time we have this afternoon, to cover this field as it should be covered, and I shall ask also that you keep in mind that as I try to report to you some of the research work along with some more completely-controlled data, that you will please differentiate between the suggested new information, which is not yet in any form that we can call its data established facts, and use things that are sufficiently well-established for us to accept as being verified.
Many of the things I shall tell you I shall present simply as experimental data, and ask you to make your own deductions. You are the court, and I shall ask that you think of our present situation in the study of child welfare, for I am to address you on the subject of child welfare from the standpoint of the newer knowledge of the fundamentals for making a diagnosis.
The newer knowledge that has impressed me greatly has been that we have not appreciated the child as we have the adult. The child is helpless, largely; the adult is not. Many of the children that come under our observation are led in by somebody, a nurse or a parent, and they are led out, and they are entirely dependent in this matter of dental care.
You also will think with me of where our entire civilization stands at this time. Mankind has been moving forward during the centuries and eons of time through three great forward movements. The first was when he learned to compress the palm and the digits of the hand, and then that animal of the jungle, picking up a stick, could reach the other animals of the jungle before they could reach him or her, and immediately that animal became master of the surrounding environment to that extent; and that was a very important step. Another great step forward was when man, in the ice age, found himself being hedged in by the ice, and the difficulties of controlling the environment to keep him from perishing from the cold were so great that he learned to utilize the fire that he perhaps had seen kindled by the lightning or in some other way; and he warmed himself, and he built his shelters, and he tied a stone to his stick. Out of that age and out of man’s difficulties came his splendid march forward.
Then man found himself in control of the environment, because he could build fires and shelter, and could save the food which the other animals could not; but he found himself subject to a parasitic enemy growing within his body, and immediately that he recognized the presence of these parasites he started a new campaign, which was to rid himself of his parasitic enemies. During the last two hundred years that campaign has been going on unrelentingly against the parasites of the body, and today man has lengthened the average tenure of life from an average of twenty years, two hundred years ago, to an average now of 51.49, and fifty per cent of that advance has been made during the lifetime of men sitting within the hearing of my voice.
But we find ourselves in this situation: that this control of the parasitic enemies that has made this splendid advance possible, has been largely because man has controlled the epidemic infections, scarlet fever, diphtheria, yellow fever, and that host of great plagues that devastated the entire world. Today man has controlled largely the epidemic diseases. People do not die now of smallpox, but they do die of the degenerative diseases; and our study for this hour will be the relation of the dental profession to the degenerative diseases, with special reference to child life.
If you will think with me of these great efforts that are being made to control the degenerative diseases, you will think at once of our campaign against tuberculosis, which is wonderful, and by that campaign we have practically reduced tuberculosis fifty per cent, a splendid acquisition. At the same time that we have made this great advance against tuberculosis, we have made almost no defense against heart disease, and as we think of the degenerative diseases, you will think of heart arthritis, and those disturbances of the digestive tract and the nervous system, rheumatism, kidney lesions, etc.; and all of those degenerative processes seem to have baffled pretty largely our diagnosticians, so much so that at the meeting of the American Association for the Advancement of Science in Boston a year ago last December, at which there were 2500 delegates, Dr. Livingston Farrand, who was addressing the Association on “The Nation and Its Health” summed up the situation as quoted by Science:
“Dr. Farrand reviewed the progress of public health work in this country and pointed out that since 1870, the average length of life has been increased by 15 years; that marked reduction has occurred during this period in infant mortality and in mortality due to tuberculosis, typhoid, smallpox, and many other diseases. The efforts of health workers and organizations have, however, been unable thus far to prevent increases in certain unconquered diseases, such as cancer and diseases of the heart and kidneys. The most outstanding problem at present concerns the control of the degenerative diseases of later life, an increase in mortality from these being an inevitable consequence of improvements in the control of diseases of infancy and youth.”
You see we have not made progress very fast against these diseases that are taking people today. Of the people who are sitting within the hearing of my voice, the probabilities are that nine out of ten will die of degenerative diseases, some of kidney, some of heart, others from diseases of the digestive tract, others of the nervous system. We do not yet know those fundamental etiological factors entering into them.
Dr. Haley Fiske, the President of the Metropolitan Life Insurance Company, has compiled figures that show something like this: We have two million cases of heart disease alone in the United States, a wonderful army if we could utilize it, but very largely dependents. Of those two million people, 150,000 die every year, so we are recruiting 150,000, every year. Where do the 150,000 come from? Approximately one in fifty of all industrial workers has heart disease and they die on an average in six years. Have you realized that one in ten of all funerals is a case of death from heart disease? If we take the economic problem, we will see it amounts to something like $500,000,000 a year for lost time of workers, according to estimates for tuberculosis, and it is probably more per year for heart disease. If we could approach this thing from the standpoint of economics alone, we would make a campaign to try to save some money for our treasuries by saving lives. But we do not do that in this age. We save hogs and forests, but we do not make very much of an expenditure to save humans.
I want you to note this circumstance: In London they have made important studies regarding child life, and they find that a large number of the children that developed chorea, and this is true of every part of the country, later develop rheumatism and heart involvements. Of course that is common knowledge. They took a group of the children that had developed chorea, which so often precedes heart lesion, and moved them out from London to the seashore, and gave them a vacation out in the sunshine in the refreshing breezes from the ocean, and all of those children recovered from the chorea and none of them had heart disease. They took them back to their original environment in London, and in six months’ time re-examined them all, at which time sixty per cent had developed heart lesions.
I find myself recoiling at their taking those children back to that environment, and I do that because researches we are doing show so conclusively that those children were doomed at the time they were born. Their death certificates were made out practically all ready for signing. The difference was that since they looked like other children, and since that advance in civilization had yet not come so that it might be recognized, they were treated like other children, and were not given the advantages they should have had, because they were born with an inherited susceptibility for these streptococcal lesions.
I want you to note that when we would study the nature of heart disease to find out its principal etiological factor, we would naturally go to some of our great bacteriologists. We probably have none greater in the study of bacterial endocarditis than Libman, of New York City. He makes the statement that of the subacute cases, about ninety-five per cent are due to the streptococcus viridans; the remaining five per cent are caused by bacillus influenza.
The difference between acute and subacute is that if they die within six weeks, it is acute; if they live more than six weeks, it is subacute. The acute cases of bacterial endocarditis, that run their due course in less than six weeks are due chiefly to hemolytic streptococcus, but can be caused also by a great variety of other organisms. Please note that streptococcus viridans is simply a group name for those that grow green colonies on blood agar, and that is the organism which is found in over ninety-five per cent of infected teeth. It has low virulence and low attacking power. There is a poor reaction on the part of the host to fight it, and therefore it lives within the body almost without any warfare on the part of the body. It is exceedingly significant that this streptococcus viridans, which is found so continually that it is almost universal, as the chief infecting organism of pulpless teeth, is also the organism that is responsible for such a large proportion of the subacute heart cases.
Dr. Libman in summing up that splendid resume, which was in the form of a paper published in the Journal of the American Medical Association in March, 1923, makes the following important conclusion:
“It is evident that I have presented the subject of the characterization of the various forms of endocarditis in a very broad way only. It is realized that the various subjects that have been discussed must later be taken up in a more detailed fashion. One thing is clear: It is evident that the disease which was considered rare, subacute bacterial endocarditis, is now recognized as one of the common diseases. Of greatest interest is the change in our point of view. It was supposed to be a practically uniformly fatal disease. Now we are observing more and more partial or complete recoveries. We find that very mild cases exist and that there is a recurrent form of the disease. In other words, the interest is shifted toward the question of healing. It will be of the greatest value if an active campaign is undertaken for the purpose of preventing this as well as other forms of endocarditis.”
Had I time to go into the studies of Raven, of London, and of several others, we would find they are noting that they have more cases of carditis to care for in their clinics than they have of tuberculosis, and in some clinics more than all other diseases combined.
You see, then, we are dealing with a great problem. Have you realized that three times as many people die of heart disease and from other complications following the “flu” as the result of the “flu,” as die from the epidemic itself during the epidemic or immediately following it? It is during the one, two, or three years following “flu” that they die of these carried-over “flu” complications.
Going to arthritis, another of the degenerative diseases, Dr. Ely, working in the Leland Stanford Clinic, makes this statement, (and he is speaking only of the second great type of chronic arthritis, the proliferative type, with multiple arthritis, and that is only one of the two chief kinds of arthritis):
“In the orthopedic clinic at Stanford it is by far the most frequent disease with which we have to deal. Established always with the roentgen rays, its diagnosis comprises more than one-tenth of the diagnoses in our clinic. A very large proportion of the so-called sciaticas owe their origin to spinal arthritis.”
Sir William Willcox, one of the great surgeons of England, and Dr. Beddard, a great internist, are agreed in their deduction that ninety per cent of the cases of non-specific arthritis are due to infections arising from the teeth. Then take this next statement. This is by Boas in the Journal of the A. M. A. for May, 1924. He says regarding arthritis:
”About forty-five per cent. of all patients with chronic multiple arthritis present organic lesions of the heart. Valvular disease, the result of an endocarditis, was found in 17.5 per cent, and in 28 per cent of those who were under 40 at the onset of their arthritis; heart disease due to arteriosclerosis of the valves or to hypertension in twenty-six per cent, and in four per cent of those who were under 40 when the disease began. Of those over 40 at the commencement of their illness, none had endocarditic lesions, and sixty-three per cent. had arteriosclerotic heart disease. The age distribution of the heart lesions is probably explained by the greater susceptibility to infection of the heart valves in younger persons. These observations give added support to the theory that chronic multiple arthritis (arthritis deformans) is caused by an infectious agent.”
I am just giving you a general bird’s-eye view to show you how these lesions, the so-called degenerative diseases, may be related to a force we have not fully appreciated.
Going on now to one other thought, cancer, before I take up the slides: What is the cause of cancer? I do not know, and probably I will be misunderstood by some people here this afternoon. I am going to read now a statement, and note what this authority has to say. This is by Dr. William Crofton on January 4, 1924:
“It was suggested that the cancer cell was really of the nature of a phorozoon, the normal cell being degraded to this stage as the result of chronic submaximal stimuli and enabled to live owing to a change in the body fluids. Dr. Crofton suggested that in many cases, if not in all, the stimulus was caused by chronic infection with non-pathogenic bacteria, and that the change in environment which enabled this stimulus to become effective was the result of destruction of the cell islets of the pancreas by pathogenic germs. In explanation of this view Dr. Crofton cited Baird’s hypothesis of the alteration of generation, and gave an interesting account of the cell metabolism in the body.”
I am not saying that. This is the language of Dr. Crofton, and I want you to remember it as we go on and I show you some data that will relate our cancer cases to types of infection.
Owing to the necessity for very great brevity, we will now hurry on to the slides, and the first will show some phases of this which we must keep in mind when we undertake to make studies of dental pathology.
Figure 1 shows two teeth extracted from the same patient, and they are typical of a condition you may frequently find. Here we have the first permanent molar A, with an extensive zone of rarefaction, and the second, B with much less rarefaction, if any. Most people would read that second molar as X-ray negative. I am now discussing only that phase of diagnostic procedure which has to do with the Roentgen-ray. I do this to suggest to you that you cannot read them correctly, in the terms of our former standards. In A’ and B’ are seen the roots extracted, showing their granulomata attached, and you will note on the second molar they are as large as on the first molar, although it was not disclosed in the roentgenogram. Here the first permanent molar developed earlier, of course; caries developed in it during the teens. This man had splendid resisting power at that time, and during his period of good reaction he was able to tear down an extensive zone around the end of the tooth, for the purpose, among other things, of making room for a membrane there which becomes a quarantine station. His second permanent molar became infected during the thirties. He had less resistance at that time, and a different type of reaction, and he had as much condensing osteitis there as he had rarefying osteitis, so that the rarefaction is hidden by the condensation, and we do not see the cavities that contain these granulomata. The roentgenogram does not necessarily disclose things as they are. It is seldom true that the physical condition is as it appears in the roentgenogram.
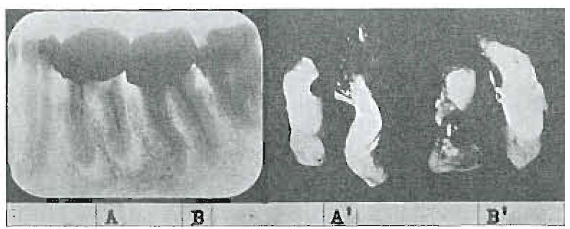
Fig 1. Comparison of apparent and real condition. A and B, roentgenographic appearance of second molars. A’ and B’, photographic appearance of roots and granulomata. Note: those on B are larger than on A.
Figure 2 shows the molar and bicuspid region of an adult, and you would not have anticipated that the buccal roots were entirely absorbed from this molar tooth. The incidence of the rays is in the direction of these buccal roots because of the low palate and the position of the film, and you do not get a true picture. You would not expect that this bicuspid root filling is penetrating the apex as it is here. Fig. 3 shows different views of that same tooth, and you can see different lengths of filling according to the angle. We must have a definite knowledge of the angle at which the ray was taken in order to make the proper interpretations.
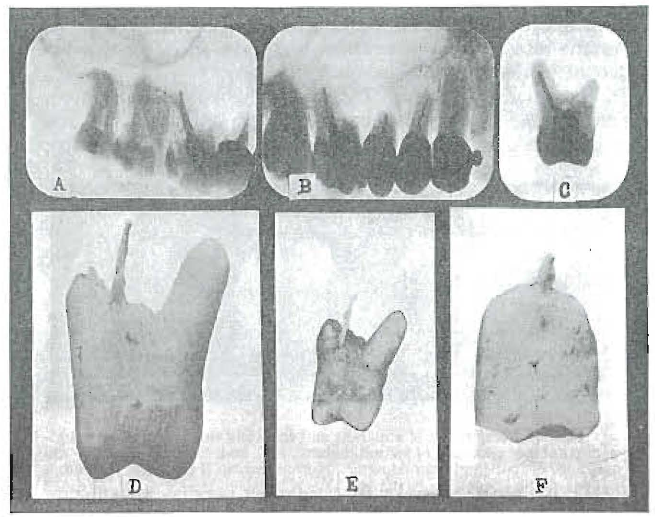
Fig. 2. Comparison of apparent and actual condition of molars and bicuspids.
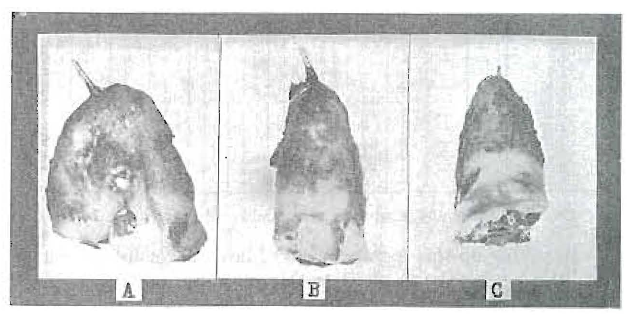
Fig. 3. Three views of the second bicuspid shown in Fig. 2.
When we pass to another phase of this question, namely, the type of organism that invades dental infections, I think we arrive at the point where we recognize that it does not matter much what the biological classification of the streptococcus is, for there are something like two hundred different strains of the streptococcus isolated, but it does matter a great deal about the environment, and whether or not the particular type of biological classification of streptococcus is injuring the patient.
When we make a study of this quality of the behavior of organisms, and how dependent they are upon their environment, I wish to call attention to the fact that the same organisms may grow in many different forms. (One was presented growing in twelve different forms morphologically; all of the changes were produced by simply changing the culture medium, indicating the adaptability of the organism and its morphological changes that take place due to the culture medium.)
Formalin
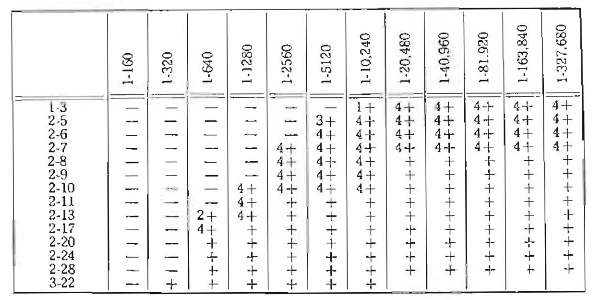
In taking up this next problem of how successful we may be if we undertake to sterilize the tooth, we have very important data. When we take the strains from teeth, which are chiefly streptococci, though we may have other organisms growing with them, and put them in any of the medicaments that we use in the teeth, we will find at first they will be killed by very great dilution. In Chart 1, using formalin, the first growth was at 1 to 10,240. In two weeks’ time, and by transferring, we were able to increase the concentration, until we were able to grow them in a concentration of 1 to 320 of formalin. That is very many times stronger than it was possible for the organisms to live in at first. What has happened? Something similar to that which has made possible all advancement in all biological forms on the face of the earth, viz., their capacity for adaptation; and by it organisms will come to grow in a tooth that you saturate with formalin solutions, or with iodin, or with some other compound, perhaps in a year, or in ten years, or perhaps in a month. But suppose there is no material that we can put in a tooth that will not finally dissipate considerably, and to which the organisms cannot adapt themselves in part, and they grow finally at the edge of our zone of sterilization, and finally into it. At this time we are carrying on studies of various trade preparations and we have an especially good nurse for the micro-organisms. Dr. Meisser has been able to grow many of them in greatly advanced concentrations. What does that mean? Do not think because you render teeth sterile, assuming you can do it, that those organisms will continue to consider that concentration as a barrier for them. We do not yet know all there is involved in this problem. I have never yet tested a tooth saturated with iodoform, even where we could get the odor so you could smell it all over the room, where they did not grow. We have, then, to readapt ourselves. We cannot sterilize teeth so easily as we thought. We cannot make them an uninhabitable place for that organism as easily as we thought we could.
Chart 1. Shows the progressive adaptability of streptococci to formalin.
If you have been reading about Teapot Dome, you probably noticed a picture in the Literary Digest. That article shows a little insect whose larvæ thrive in crude oil. When these little insects are taken out and put in a normal salt solution or water, it kills them. They are so used to this bad environment that they cannot stand to have it any better. It is simply the old law of adaptability. They don’t eat that oil; they live on the insects that drop into the oil and which are killed by the oil.
Now another phase of the question: We have thought of the danger as being proportional to the zone of rarefaction. Again I will be misquoted and misunderstood. I may be quoted as saying that the small tooth without rarefaction is worse than the one with large rarefaction. No; that is not so. But with a given dental infection, that patient who cannot make a large zone of rarefaction, but who makes a little one, is in more danger than the patient who makes the large zone with that given dental infection.
In Fig. 4A-1 we have a central, and there is a large zone of rarefaction about it; and in A-2 there is a lateral with a slight zone of rarefaction; and in A-3 there is a molar with a large zone, and in B-3 a molar with a slight zone of rarefaction and some condensation. This patient with the large zone of rarefaction is very much more safe with that tooth than the patient is who has the tooth in B-3. As a matter of fact, the first patient has no lesions at all, and A-2 is a bedridden arthritis case. And yet we have gone on the assumption that the danger was in proportion to the size of the zone. And how many times men will pick up a roentgenogram and will undertake to tell what should be done for the patient on the basis of how large that zone is. This tooth (A-2) they will say they can treat, but that one (A-1) they had better extract. Now as a matter of fact, that thing that is happening there is a measure of something provided by the host, and not a measure of the organism either in quantity or irritability.
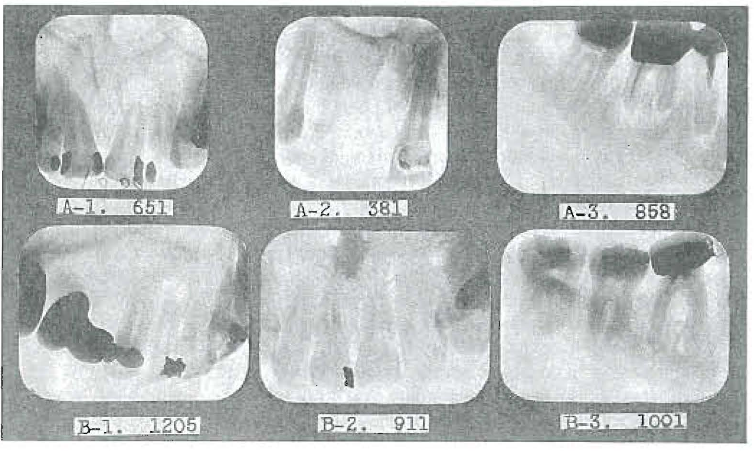
Fig. 4. Three typical types of dental pathology representing characteristics of three different groups of people.
We will find a marked condensing osteitis sometimes, and if we inject our organisms into animals, sometimes we will find, not a hole produced in the bone, but a condensation in the bone. Fig. 5 shows three views of a rabbit’s spine. The rabbit was inoculated intravenously with a dental culture of streptococci, and there has been produced a marked condensation of bone, not a rarefaction.
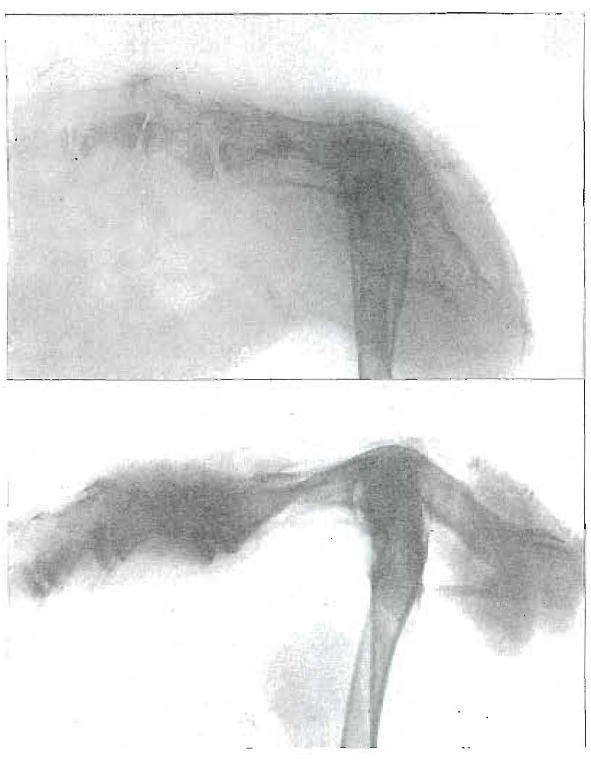
Fig. 5
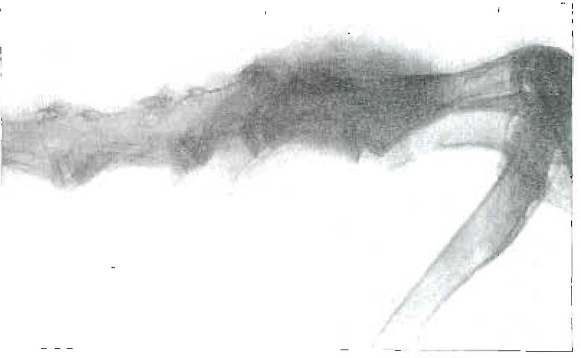
Fig. 5. Progressive development of a spinal disease resembling Pott’s from inoculation of a dental culture. “C” four months after “A.”
When we consider the different types of lesions, we find that some of the animals develop a building on of bone onto the joint, and others will have a tearing down of bone. One we speak of as the proliferative type of arthritis and the other the degenerative type of arthritis, and these two different types are related to two different types of systemic calcium.
Figure 6 shows how these different teeth may have different conditions about the roots. What do you see when you look at a tooth or at a patient? How many of us are simply looking at a hole in a tooth, and our horizon will be the cavity walls. Perhaps we are simply building or repairing grist mills.
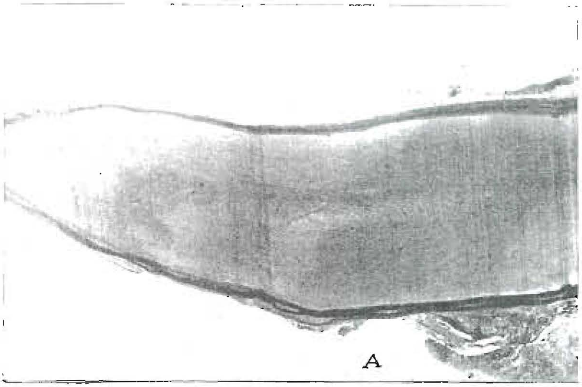
Fig. 6

Fig. 6. Two opposed types of reaction. A, with marked thinning of the cementum of the root; and B, with marked thickening as excementosis.
In A we have a tooth that has had its cementum almost entirely removed, and below it another tooth of the same type, but the cementum has been built on in successive layers until we have this tremendous excementosis. Those patients are as different as can be. This patient always tends to have pyorrhea; that patient never has pyorrhea around that condition at the time that is forming. These two processes go right back to systemic expressions, and this patient has something expressed in the bones of the body all through the body, and so does this one. Every bone in the body probably records this same thing that is recorded in the teeth. “A new truth is a new sense,” for with that new truth you can see things you never could see before. I want to give you some of these new truths, so that you can, when you diagnose a case, treat that case as an individual case, and when you see a condition like that in B, Fig. 6, do not think that you can treat that patient as you would a patient with the condition as shown in A. Their backgrounds are different, and there is here a key to an important underlying process.
Figure 7 is the case of a patient who presented in April 1923 with a putrescent pulp, and this tooth is tender, and there is a distinct zone of rarefaction. Had you or I treated that tooth, and the patient had come back a year later and we found that zone had decreased to this point, wouldn’t we have patted ourselves on the back and said our treatment was successful? As a matter of fact, that tooth was not treated at all. That patient got the “flu” and has been sick for a year, and while she has been getting worse and worse, this zone has been getting smaller and smaller, and condensing osteitis has been filling in that process that had not formed at the time of her high defense. Her calcium, which goes down at once, or goes into solution, is controlled by factors in the body, independent of whether or not the irritant has been changed. The tooth has remained infected, and here we have the apex showing the dead cementum area when the tooth was extracted. Had we filled this tooth we probably would have fooled ourselves. This type will fool many of us if we do not see that condensation may be an expression of infection, and not an expression of protection.
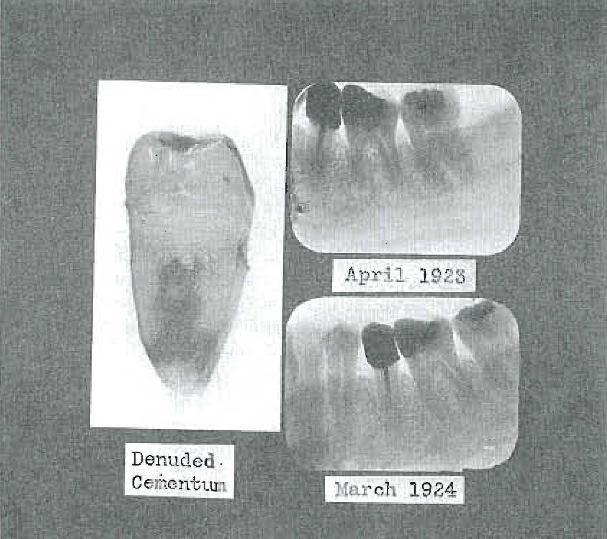
Fig. 7. Two roentgenographic views of same tooth, eleven months apart, showing reduction in size of periapical zone of radiolucency. Tooth not treated. Photograph of extracted tooth shows denuded cementum.
We have come to be able to classify all patients into three groups upon the basis of the kind of reaction about their teeth. I will relate that to the systemic in a moment. First, the group that will tear down the bone extensively and then absorb the root of the tooth. Then we have a group whose members have relatively large zones, and they build this zone of condensing osteitis around it. Then we have a group that will have, say, a putrescent lateral, by absorption. What is going on? Those patients in those three different groups are so typical of their kind that when they come to you, if you have learned this new key to dental interpretation, you will be able in part to tell the history of the patient from the roentgenogram. I do not advise that method of making diagnoses. Get your physical also, and read them together. You need the physical. But time after time I have made this test. I go to conventions, and have them prepare for me some sets of roentgenograms of teeth of patients. I will not see these patients until the slides are put on the screen, and then, with the patient before me, I undertake to tell that patient’s history, whether or not they have had heart disease or kidney trouble or rheumatism, and whether or not they have had recently a break, and then let them tell the audience whether or not I am right. And in doing that I am playing the game with marked cards, because people behave alike in the different groups.
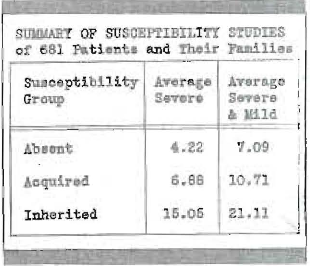
All people are not in the same danger. Some people can stand a lot of infection and not have rheumatism or heart or kidney trouble. Few things have been so hard for us to reconcile and for the medical men to reconcile in connection with dental infections as the fact that in the clinics where there are seen people suffering from, let us say, fractures of limbs or various things of that kind, that so generally those patients that have even a large number of suppurative pyorrhea pockets and evident abscessed roots have no rheumatism or kidney trouble; and isn’t it fair for these medical men to conclude that if these people with all these infections have no trouble, why should we expect it in somebody with much less? In this new light we see that this is just exactly what we should expect. When we study people on the basis of whether or not they do or do not tend to have heart or kidney trouble, etc., they divide into three groups, viz: those that never have rheumatism; those that never have had it during the great majority of their lifetime and then suddenly have developed it, and we find it related to an overload of some kind; and third, those that have always been troubled more or less. If we take those three groups, and study the other members of the family, the brothers and sisters, the father and mother, uncles and aunts, and the four grandparents, we will see that in this group of people we have the results shown in Chart 2.
Chart 2. Grouping of patients on the basis of their susceptibility to rheumatic group lesions.
In Chart 3 we have the various groups, and have taken fifteen families for each of these groups. You see we have from twenty to thirty times as much danger if the person belongs in the third group as the first. That is the tendency to the rheumatic group. Note this: If we take caries in these different groups, the individuals in the absent group show little, but you see that the caries increases in proportion to the susceptibility, or in the same order as susceptibility to rheumatic group diseases.
Chart 3. Relation of caries and periodontoclasia to presence or absence of susceptibility to rheumatic group lesions.
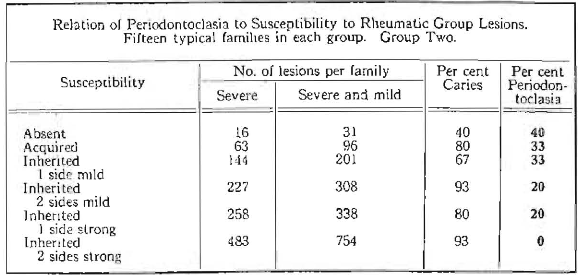
Note that as the caries increases, the pyorrhea decreases. For those who think pyorrhea is a local disease due to trauma, traumatic occlusion or local infection, how do they account for the fact that as pyorrhea decreases, caries increases, and that the pyorrhea decreases in the same proportion and same order as the increase in susceptibility? These people have just as irregular teeth, just as much traumatic occlusion as the others, and yet no pyorrhea. Every one here will see that in everyday practice. There isn’t a man or a woman here who hasn’t already observed that the patients with pyorrhea do not usually have caries, and vice versa, those mouths with very extensive caries, as a rule, are not the ones with pyorrhea. But here is a great law. We can divide these people into groups.
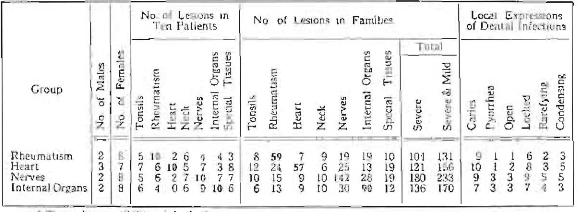
When we take these ten individuals for rheumatism, (Chart 4) and then study all the other members of the families, taking in this case ten families, out of all the members of the ten families, there were 59 cases of rheumatism, where the patient had rheumatism, whereas in the other three groups the numbers are 24, 15 and 13. Or, if you take heart disease, note that it is 57 in comparison with 7, 9, and 9. For nervous system, 142 compared with 19, 25, and 30 and for internal organs 90 compared with 19, 28, and 13. We might say that the ancestors, of course, might influence the children, but I am here taking the incidence in the child, and asking you to see all the members of the ancestry, and you have these figures. So we have evidence of an inheritance of this quality which makes people susceptible to the rheumatic group lesions.
Chart 4. Comparison of susceptibilities to rheumatic group lesions of other members of the families of involved individuals.
The balance of the lecture was largely slides presenting evidence of a definite relationship between the type of dental pathology and the presence or absence of systemic susceptibility, and the relation of both of these to the development of degenerative diseases, and also of evidence of relationships between other diseases, such as cancer, tuberculosis, and diabetes, to both of these factors, the lecture being largely a consolidation and extension of the recently published text by the author in two volumes entitled Dental Infections, Oral and Systemic and Dental Infections and the Degenerative Diseases. (Published by the Penton Publishing Co., Cleveland, Ohio.)