
Access to all articles, new health classes, discounts in our store, and more!
Healing of Tuberculosis
Read before the Fourteenth Annual Clinical Session of the American College of Physicians, Minneapolis, February 10-14, 1930. Published in Annals of Internal Medicine, Vol. 4, No. 3, September 1930, pp. 281-323.
* * *
We are able to estimate the value of therapeutic measures as applied to any disease in proportion to our understanding of the manner in which the body naturally combats such disease.
Infectious diseases, as they affect different people, produce a varying picture. While the same disease is always produced by the same microorganism, yet identical conditions whether in pathology, symptomology or in ultimate results will never be found.
Grant that all human beings would react toward a given microorganism in the same general manner, variations in the disease picture would still occur because of the differences in virulence and differences in numbers in the causative microorganisms; on the other hand, grant that dosage and virulence in infectious microorganisms were always the same, they would meet varying conditions of tissue response in different individuals and in the same individual at different times, which would likewise produce disease pictures of great variation.
Applying the above principles to tuberculosis we shall see that the tubercle bacillus acting upon different individuals produces disease pictures of great variety, which are combatted with different degrees of effectiveness.
Principles Underlying Healing of Tuberculosis
Regardless of variations in the disease and differences in the outcome of tuberculous infections, the body carries out its program of protection along certain definite lines, the nature of which we may inquire into with profit. The defense in tuberculosis seems to be largely cellular, yet we can not deny that a certain amount of humoral defense is likewise brought to bear against the invaders (McCutcheon, Strumia, Mudd and others,1 and Opie2).
The program of defense differs according to whether it is a first or a succeeding infection. The former is opposed at first by only the natural defense of the host, and later by a developing specific defense; the latter by both natural and specific defense from the start.
Inasmuch as the host shows evidence of immunity in from five or six days to two or three weeks after infection has taken place, and since no symptoms appear until the immunity mechanism has been called into action, in our study of clinical tuberculosis we are always dealing with infection in the immune; so the specific factors in defense are always present and upon the degree of their competence depends largely the nature, the course, and the outcome of the disease.
Healing in tuberculosis in the immune or adult type, as we speak of it, is accomplished through several different processes, among which are: (1) destruction of bacilli; (2) retardation of the passage of bacilli through the tissues; (3) elimination of bacilli through natural channels by caseation and cavity formation; (4) development of a state of desensitization to bacillary and other toxins; (5) encapsulation or rendering inactive, viable bacilli which remain in the tissues; (6) ridding the body of the inflammatory products which accompany the infection; and, (7) repair of the injury inflicted upon the body by the disease.
In studying tuberculosis as we meet it day by day in the clinic, we get the impression that healing depends upon the controlling of the size and the effects of the reinoculations and keeping them within the range of the individual’s powers to cope with them. To this end the acquired bactericidal action of immune tissues, the retarding influence of the allergic inflammation upon the passage of bacilli through the tissues, and the desensitization of the host of toxic substances, are probably the major contributing factors. Many otherwise large and dangerous reinoculations are thus rendered ineffective and eventually overcome.
Destruction of Bacilli. To what extent destruction of bacilli takes place in the course of healing of a tuberculous process, and how important this factor is in cure has never been satisfactorily established by experiment. Kraus and Hofer3 reported that they observed destructive effects upon bacilli within an hour after they had been introduced into the peritoneal cavity. Wolff-Eisner4 speaks of a lytic action upon the bacillus which takes place within the body. Certain humoral effects have been shown by the presence of antibodies in the blood by numerous observers, but most observers have considered them as being of secondary importance, when compared with the cellular response of the host. The action of phagocytes was established by Metschnikoff,5 and Wright6 showed the effects of opsonins in preparing the bacilli for phagocytosis.
Recently new data bearing upon the subject has been brought forth. Rich7 believes, although he offers no direct proof, that destruction of bacilli is a very important mechanism granted to the body by a previous infection. Lurie8 reports experiments in which, by using one type of bacillus for primary inoculation and another type for reinoculation, he has been able to show that the resulting pathogenesis was due to activity on the part of the bacilli remaining in the tissues from the first infection, and that the bacilli of reinoculation were practically all destroyed, without preliminary multiplication.
I have long assumed that an enormous destruction of bacilli must take place in the bodies of patients suffering from clinical tuberculosis. It has seemed to me to be the only way that we can understand the healing of an extensive lesion. Such visible infections as those in the eye, testicle and larynx are of comparatively frequent occurrence in the course of chronic pulmonary tuberculosis, and very often prove to be abortive showing that the bacilli have been destroyed. Other infections which take place from one part of a lung to another, and prove to be only temporary affairs, are frequently noted when patients with advancing lesions are closely watched and frequently examined, and particularly when frequent x-ray plates are taken for comparison. Often such serial x-ray plates show a new focus to appear in a certain part of the lung field, only to clear away after being present for a brief time, say a month or two. The very fact that bacillemia, which is so often present, fails to cause uncontrollable extensions regularly is further proof of the body’s destructive action on bacilli.
Retardation of Passage of Bacilli Through the Tissues. The allergic inflammatory reaction performs what is usually recognized as a special protective service in inhibiting the free passage of bacilli through the tissues. Were it not for this service nothing but a quick and efficient bactericidal action on the part of the body tissues could save any one suffering from advancing tuberculosis from destruction, yet the recovery of such patients is a common observation in clinical practice. Koch9 first observed the restraining influence of allergy and Krause and Willis10,11 showed the extent of the retardation experimentally. They showed that bacilli are carried from the site of inoculation to the adjacent lymph glands in nonimmune pigs in an hour; but require two weeks in the immune. They make the circuit of the entire body and are found in the organs generally in three or four days in the nonimmune, but require three or four weeks in the immune. Inasmuch as preventing the disease from spreading is a condition necessary to healing it readily can be seen how important and how necessary this property of allergy becomes to the tuberculous host.12,13
In normal hosts, bacilli lying in the air passages are quickly picked up by phagocytes and carried through the alveolar and bronchial walls, as has been shown in experimental animals. In advanced tuberculosis, where not a few bacilli at infrequent intervals, but millions of bacilli daily, are found in the air passages under conditions in which phagocytosis is increased, in order to account for the failure of infection to take place we must assume either that the bactericidal power which exists on the part of the immune tissues of the host have attained almost an unbelievable degree of competency, or that the tissues themselves resist the entrance and transport of the bacilli. Rich7 does not believe that the evidence for the restraint of bacilli from entering and passing through the tissues is sufficient, but believes the real defense, which has been so generally observed from the early experiments of Koch9 to the present time is due to the destruction of bacilli and not to the retardation of their migration in the tissues
Opie,14,2 on the other hand, has recently reaffirmed his view formerly expressed,15 to the effect that immune tissues fix foreign protein at the site of injection from which it may be recovered for a period of time, and states that anaphylactic shock is prevented by this local fixation process. While this may not prove that the same thing is true of bacteria, he calls attention to the similarity of behavior of the immune tissues to tuberculin, abortin and other similar bacterial products, and also cites, apparently with approval, the experiments of Cecil and Blake16 who found that the blood stream of monkeys vaccinated against pneumococci by intratracheal inoculation shows less invasion than the unvaccinated.
The Elimination of Bacilli from the Body by Necrosis and Cavity Formation. The elimination of bacilli through the natural channels of the body, such as the bronchi, bowel, and urinary tract becomes an important phase of defense in extensive lesions.
In advanced destructive lesions large numbers of bacilli are gotten rid of daily by being ejected from the body through the bronchi, and countless others through the gastrointestinal canal. During the time that these bacilli are within the natural channels of the body, if the patient were not protected by some specific barrier of defense, he would be in danger of their penetrating into the tissues and forming new foci of disease.
The destruction of tissue as it occurs in pulmonary tuberculosis through the breaking down of conglomerate tubercle and cavity formation with the discharge of the focal contents into the bronchi to be carried outside of the body must be looked upon as having paradoxical interpretation. The destruction is due to the relatively large numbers of bacilli engaged in the reinoculation at a time when the tissues are markedly sensitive to tuberculoprotein. It would not take place if the infection were produced by a few bacilli only, even if sensitization were marked; but it results because of massive dosage when sensitiveness is marked. It is doubtful whether any host could withstand the disease which would be caused by such quantities of bacilli should they scatter into the tissues, if we may judge by the consequences of ruptured bronchial glands and the resulting caseopneumonic lesions which follow, or of miliary infection following severe bacillemia. So from this standpoint the destructive process is without doubt conservative. Nor could the tissues heal with such masses of bacilli within them. Therefore, unless the host is able to destroy the large numbers of bacilli contained in the caseous masses, the only opportunity for healing must come through their expulsion, even though damage be done to the host by the loss of tissue.17
Desensitization of the Patient to Toxins. While we have no method of measuring the toxins which a patient withstands during the course of pulmonary tuberculosis, it seems reasonable to assume that his capacity to withstand must increase many fold as the disease progresses; for a small limited lesion at the beginning of infection will cause a syndrome of severe toxemia with equal or more prostration than will be caused later when the infection has extended and multiplied many fold and increased the amount of toxins enormously.
It is undoubtedly one of the results of the action of the patient’s own tuberculoprotein that it desensitizes him and prepares him to withstand larger and larger doses of bacillary protein without serious harm. This seems to be a necessary part of the immunity mechanism without which patients with advanced tuberculosis would not be able to endure their disease, let alone having an opportunity of overcoming it (Pottenger18). It is also probable that the patient is desensitized to the toxins produced by his own tissues. This is illustrated by the following case:
No. 9564. Mrs. E. W. Aged 35 years. Entered sanatorium May 5, 1929. Important previous history: measles at 32–quite severe; appendectomy at 27; operation for acute ileus at 30; influenza at 35; pneumonia at 31, followed by pleurisy for three weeks. Excellent health except dry hacking cough up until October 1928, when she developed severe cold followed by persistent cough and expectoration. Treated for bronchitis. Another severe cold December 1928. Temperature not taken. Tuberculosis not suspected. During April 1929 patient complained of severe exhaustion; loss of appetite, poor digestion, nausea, eructation of gas, profuse sweats, right sided pleurisy, a loss of fifteen pounds in weight, and severe cough with considerable sputum.
The temperature and pulse curves for a period of eight months, and X-ray films taken at intervals during the eight months, are shown in Fig. 1 and Fig. 2 A, B, C, and D. On entering the sanatorium patient was too weak to sit up for examination. Showed extensive bilateral tuberculosis; caseopneumonic in type, throughout upper half of the left lung, with cavitation, and a lesser in filtration in the upper third of the right lung, as shown in Fig. 2 A. Temperature 103-104°; pulse 90-108, as seen in chart, Fig. 1. The disease continued to extend and showed increased areas of softening, as indicated in the film Fig. 2 B, taken August 30, 1929, which shows entire left lung involved. Temperature, however, had become lower, as will be noted in the chart. Appetite improved; digestive disturbances lessened; and sweats disappeared. Patient felt much better. This improvement in symptoms continued through November, although temperature remained high, and as will be seen in the film Fig. 2 C, taken October 15, 1929, softening continued to take place throughout the lower portion of the left lung, where several cavities seem to be in process of forming. In December patient began to have chills and increased symptoms of prostration: drenching sweats; appetite and digestion poor; increase in temperature, and the cavities in the lung were more definite, as shown in film Fig. 2 D, taken December 2, 1929. Whether this will continue and cause the death of the patient, or whether after excavating the lower lobe she will improve, remains to be determined.* (*Patient has continued to run the same temperature of 100-101° and maintains same general condition. Aug. 10, 1930.)
I should like to call attention to the disparity between pulse and temperature throughout the course of the disease. A relative bradycardia is present, indicating a preponderant action of the vagus in spite of the severe stimulation of the sympathetics caused by the toxemia.
In comparing the temperature curve, the symptoms as here recited, and the extent and severity of the lesion, as indicated by the plates, it will be seen that the patient had fewer symptoms, and lower temperature, with a severe and more widespread lesion than she had originally, with a more limited lesion. In explanation of this, we must assume that it was due to the establishment of a strong immunity to both tuberculoprotein and to whatever protein was derived from the destroyed lung tissue; otherwise, there is no explanation of her ability to improve her general physiologic activity while the disease was spreading and showing increased activity pathologically. Desensitization to the patient’s own tuberculoprotein, and to whatever other protein was thrown into the system from the broken down lung tissue, is a condition necessary to the understanding of the apparently paradoxical relation between the advancing disease and the lessening of symptoms. Another very interesting thing which suggests the existence of a high degree of specific protection (immunity) is the failure of the disease in the right lung to extend, and a failure of the large quantities of tuberculoprotein which must have been thrown into the blood stream during this time, to cause sufficient reaction to produce marked exudation and caseation in the upper right lung.
Temperature Chart
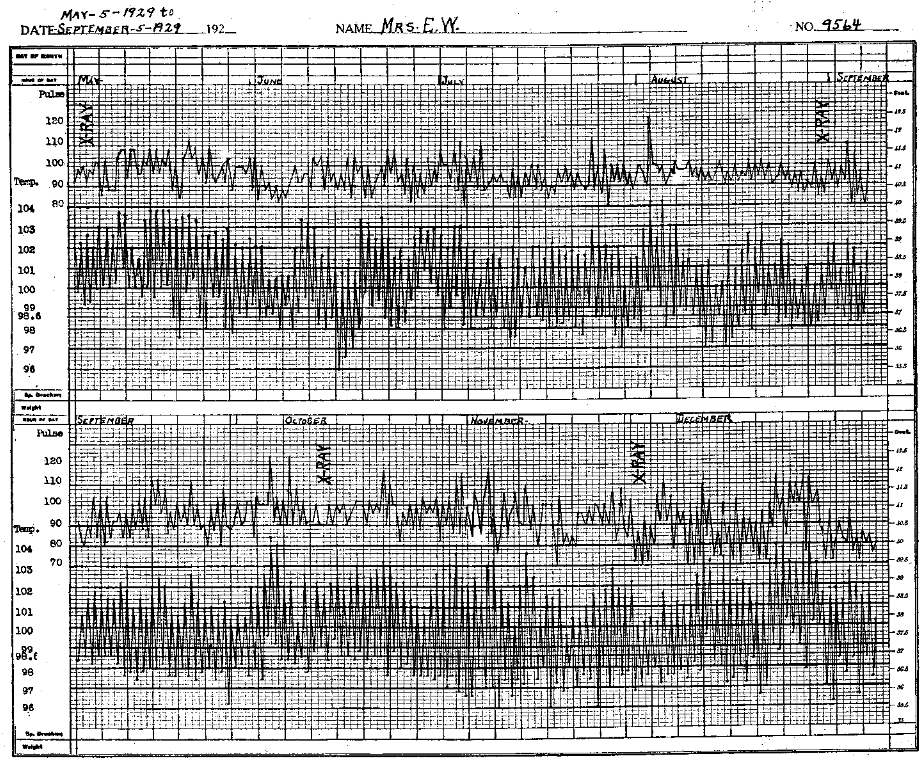
Fig. 1. Temperature and pulse curve of patient suffering from chronic exudative tuberculosis, involving at first the upper two-thirds of left lung, most extensive above the third rib, with cavity in first interspace. Slight involvement in right lung. Patient profoundly toxic. Disease extended and cavitation increased, as will be seen in Fig. 2 A, B, C, and D. The temperature, however, lowered somewhat (fig. 1) as did all symptoms of toxemia; appetite improved, patient was less nervous and sweats disappeared. This condition continued until December 1929, in spite of the extensive disease, as shown in Fig. 2 B, C, and D. Then resistance began to lower, the disease spread, and symptoms of toxemia again increased. The lessening of symptoms, regardless of an extending and destructive process, as indicated by Figs. 1 and 2, suggest that desensitization to both tuberculatoxins and the toxins from the patient’s own broken-down tissue must take place.
Note the vagus effect on the pulse. The pulse is relatively slow for the amount of toxemia present.
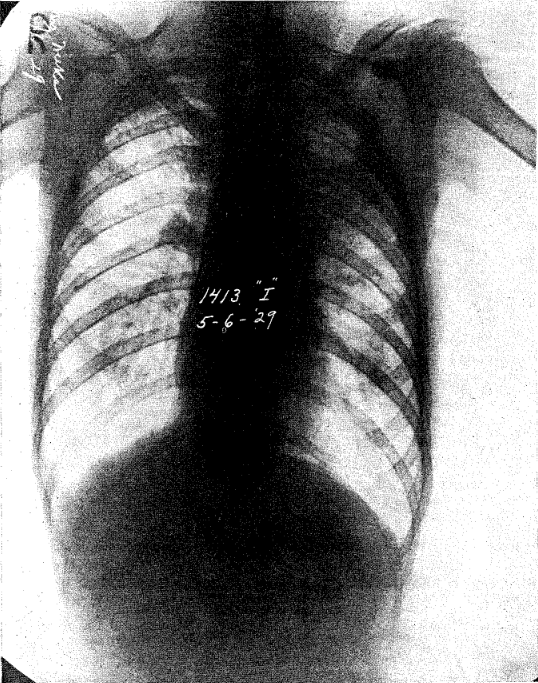
Figs. 2 A, B. C. and D illustrate an extensive exudative lesion with cavity, followed by extension and increased cavitation. The toxic symptoms, however, were much greater at first, with the limited amount of disease shown in Fig. 2 A, than they were later, as shown in Fig. 2 A, B, C, and D, although the disease has extended and cavitation has decreased. The temperature curve is shown by chart, Fig. 1.
Fig. 2 A, May 6, 1929, shows a moderate infiltration in the upper half of left lung, with cavity near apex; slight lesion in upper right.
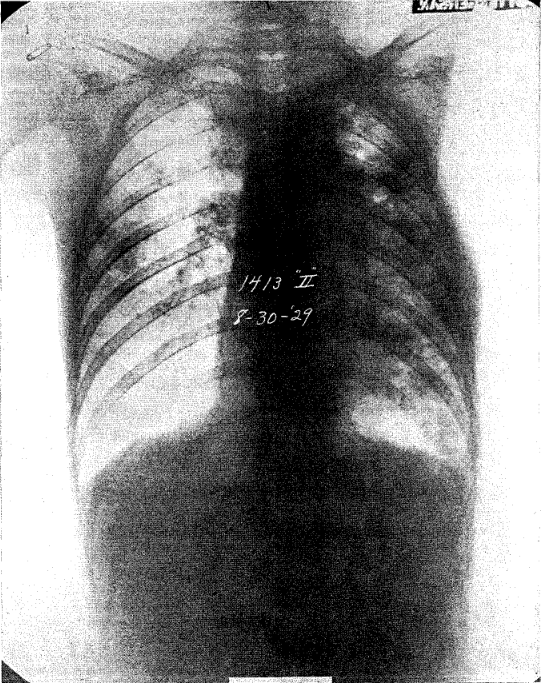
Fig. 2 B, August 30, 1929, shows entire left lung involved with increased softening.
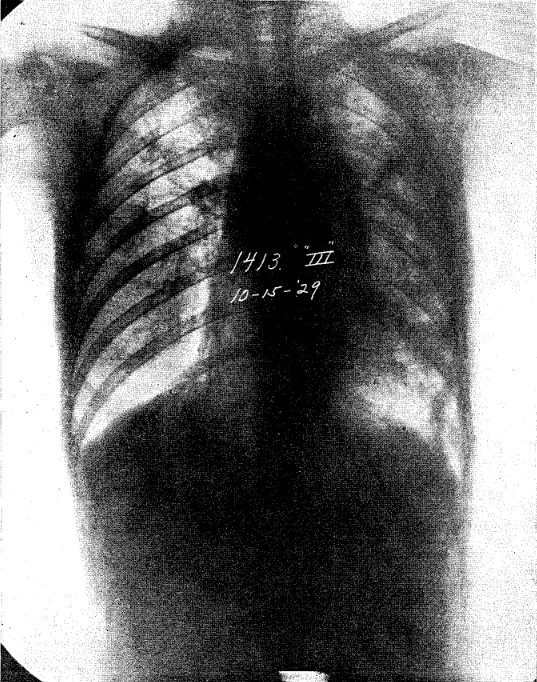
Fig. 2 C, October 15, 1929, shows softening continued to take place throughout the left lung, where several cavities are in the process of forming.
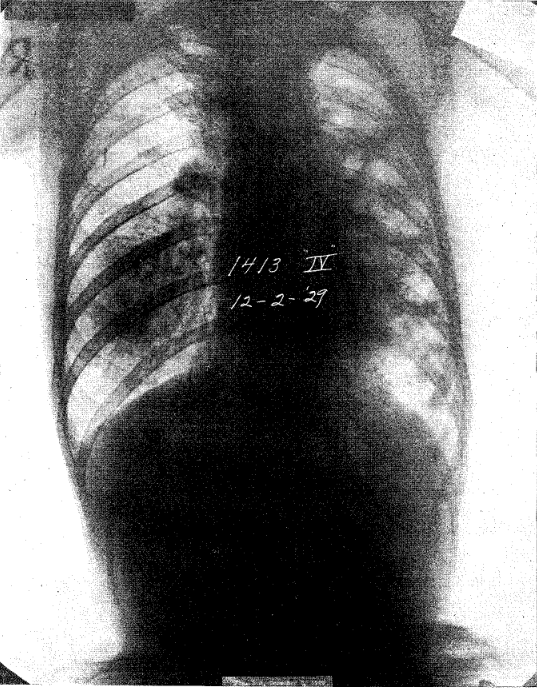
Fig. 2 D, December 2, 1929, shows extensive cavitation throughout left lung.
Encapsulation and Rendering Inactive Viable Bacilli. Encapsulation is one method by which the host renders bacilli harmless though remaining within the body. The condition precedent to such a favorable procedure is that the numbers of bacilli be few; so few that they fail to produce sufficient reaction to cause more than a temporary exudation or more than a very slight necrosis. When extensive necrosis, with loss of much tissue, has once taken place then a replacement must be brought about, and this must be preceded by the elimination of most of the bacilli from the caseous focus and the regeneration of the destroyed tissues. So healing under these circumstances is more complicated.
Attention must also be called to the fact which has been pointed out by Bartel,19 Opie,20 and others, that bacilli may remain in the tissues, maintained in a viable though inactive state, for long periods of time. This must be due to another phase of specific defense though as yet there seems no adequate explanation for it.
The Elimination of Products of Inflammation. Exudation of some degree is the part of every active tuberculous process. Healing can not be said to have taken place until all exudative phenomena have disappeared. According to the severity of the lesion, exudation may mean only a slight hyperemia, or it may mean the pouring out of serum, cells and fibrin in the tissue. In clearing the field for healing it is necessary to have all such products rendered absorbable or in a condition to be. dealt with by the phagocytes. Purely exudative phenomena accompanying tuberculosis clear away by resolution, the same as occurs in acute pneumonia, except a much longer time is required. Should irritation reach a certain degree, however, when resolution has been completed, changes of a proliferative type will be necessary to complete the healing process.
The Repair of Injury Done. If the lesion is caused by only a few bacilli, the destruction of tissue is negligible and healing is a comparatively simple process. If the lesion is a slowly advancing one, and caused by the repetition of many small inoculations, the necessary amount of injury may be brought about to disturb the patient’s physiologic activity before sufficient specific resistance has been engendered to overcome the infection, and still there be a minimum of tissue loss.
Lesions produced by many bacilli, or bacilli of high virulence, in patients with highly sensitized cells, on the other hand, create conditions which are markedly inflammatory and often destructive in character from the very beginning; and require a complicated program of resolution and tissue regeneration to repair the damage which has been done. Bacilli and the various inflammatory elements are subjected to enzyme action, and phagocytosis until the field is relieved of all abnormal debris; and then if destruction has taken place, repair follows the usual pathological course of regeneration, being modified of course by the fact that healing must often be accomplished while viable bacilli remain embedded in the tissues. Even cavities of considerable size may be healed at times with a regeneration of tissue.
How Therapeutic Measures Aid the Process of Healing
Healing depends on the power of the patient to meet successfully the various requirements of his own particular infection, no matter what they may be. Therefore, measures of therapy have been devised which have for their purpose the creating of the best possible physiologic balance on the part of each individual patient, and the keeping of his infection quantitatively and qualitatively as mild as possible.
The hygienic life which is pursued by the tuberculous patient has for its purpose the making of the physical and psychical machines to function as perfectly as possible. The most perfect metabolism consistent with the disease is thus brought about and, if maintained for a long period of time, guarantees the maximum protective response on the part of the patient.
Rest is not the ideal status of any individual for a prolonged period of time, but in tuberculosis it is a matter of necessity.21 The eight or nine hours of daily rest which is capable of maintaining the physiologic balance of the body cells in states of health is wholly inadequate in tuberculosis. In the treatment of tuberculosis we often find it necessary to maintain rest for the entire twenty-four hours for long periods of time–sometimes for many months–because we have a departure from the normal status of such a nature that exercise during the stage of active disease favors extension of infection, increase of toxemia, and lowers resistance, causing the patient’s body functions to be carried on at a low standard of efficiency. These factors interfere with healing.
This is where rest to the lung, such as comes from body rest, and such local measures as compression by weights such as shot bags, strapping, operations on the phrenic nerve, pulmonary compression, whether by pneumothorax, or thoracoplasty, are of value. They all serve the purpose of giving the lung more rest, of causing less blood to pass through the diseased areas, and of limiting the motion of the lung to the lowest body demands. The simpler of these measures prove to be satisfactory in a very large percentage of limited lesions and the more elaborate ones are successful in many of the serious ones.
While we are not able to say that scientific knowledge has advanced to the place where we can claim the attainment of a specific diet, we have learned that a well balanced diet containing not only adequate calories but also vitamins and salts in ample amounts is necessary to the best progress against tuberculosis. The Sauerbruch22,23,24 diet has seemed to be of decided advantage in tuberculosis of the skin; but, so far, not much has been claimed for it in diseases of the pulmonary form. But it has long been recognized that the patient who is a poor eater and unable to take a well balanced diet rarely makes a satisfactory progress in the healing of tuberculosis.
From the discussion above it is clear that it is the mild infections which disturb the patient least and are easiest to overcome, and that it is the severe ones which are dangerous. Larger infections are more dangerous to the patient because they cause more acute inflammatory and destructive reactions, multiply the foci from which extensions may take place, and increase the toxemia which the patient is obliged to combat.
Anything that will increase the likelihood of the disease extending or of carrying the tissue reaction beyond the limits of safety are prejudicial to recovery. On the other hand, anything that will decrease the number of extensions, tend to hold their severity to a low limit, and make the patient more tolerant of toxins and stimulate perifocal fibrosis, will aid recovery.
In the final analysis the patient, if healed at all, is healed by his immunity mechanism. The effect of the patient’s own reinoculations of bacilli or bacillary protein are helpful in promoting healing unless they are too severe; but if very severe, they may be harmful; but that he could not attain the necessary immunity to heal without them must be evident to all careful students of the immunological reactions in tuberculosis. It is his reinoculations that, acting on his sensitized cells, cause the allergic inflammatory reactions which result in restraining, the passage of bacilli through his tissues, in stimulating the bactericidal properties of the tissues, in desensitizing the patient to the poisonous proteins, and in stimulating the perifocal cells to the formation of fibrous tissue. Whether the patient wills it or not, he is treated and aided in cure by his own tuberculin, as has been stated by Long,25 and retarded in healing only if the dosage be exceeding large. Therefore, the necessity of tuberculoprotein reinoculations is obvious, but the necessity of keeping them within bounds is equally obvious.
The following cases, whose clinical progress may be judged from the plates and the appended charts, illustrate the principles discussed in the preceding pages.
The plates shown in Figs. 3 and 4 both represent limited apical lesions, one of which healed promptly under the usual sanatorium regime, the other only after compression therapy had been employed. The difference in time of healing in these two patients was probably due to differences in their respective resistance, which probably means differences in the physiochemical reaction of their body cells. There is no evidence of virulent infection in either case; neither is there evidence of spread, aside from that noted in Fig. 2 C; but there is a great difference in the time of healing; the case represented by Fig. 3 requiring a year, and that represented by Fig, 4 requiring three and one-half years to complete the healing.
Figs. 3 A and B illustrate healing of early infiltration with almost complete resolution.
Fig. 3 A, June 26, 1928; shows moderate infiltration of the upper half of left lung and apex of right lung.
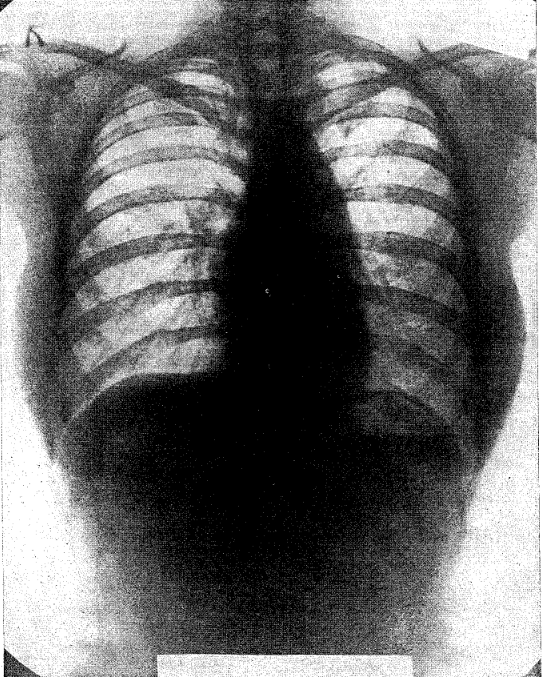
Fig. 3 B, January 10, 1930, eighteen months later, shows almost complete disappearance of lesion.
Case No. 9026. Miss A. C. Fig. 3 A and B, are films of a patient with an early tuberculosis involvement of both apices. She came under my care June 26, 1928. Film A shows the involvement at the beginning of treatment. Film B, taken January 10, 1930, shows how completely the lung had cleared. This patient was under treatment from June 26, 1928 until August 23, 1929. She had been away from the sanatorium four and one-half months, when film B was taken.
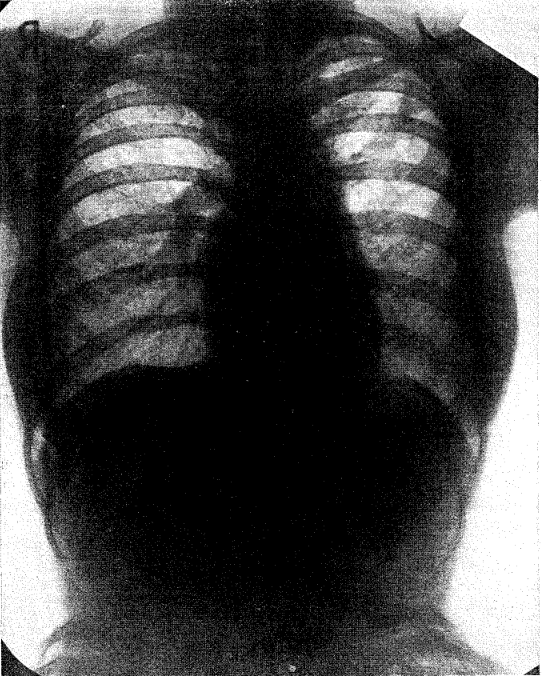
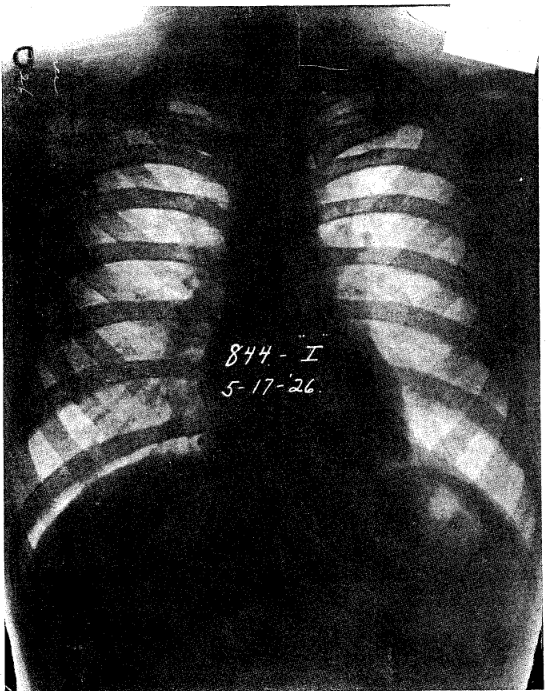
Case No. 9481. Mr. E. P. Fig. 4 A, B, C, and D, are films of a patient with slight involvement of the left apex, who came under my observation May 17, 1926. Film A shows involvement at beginning of treatment. He had not been able to clear the lung in fourteen months time, as will be shown in film B, taken July 13, 1927. Two months later, as will be seen in film C, the disease had extended very markedly. An exudative lesion is seen through the upper half of the left lung. On account of the apparent lack of resistance on the part of the patient, we considered it necessary to institute artificial pneumothorax, which resulted in a healing, as shown in film D, taken November 12, 1929.
Figs. 4 A, B, C, and D show an early apical lesion which failed to heal under ordinary hygienic regimen, but, on the contrary, the disease extended and was healed only after pneumothorax was instituted.
Fig. 4 A, taken May 17, 1926, shows limited lesion of both apices, more marked on the left.
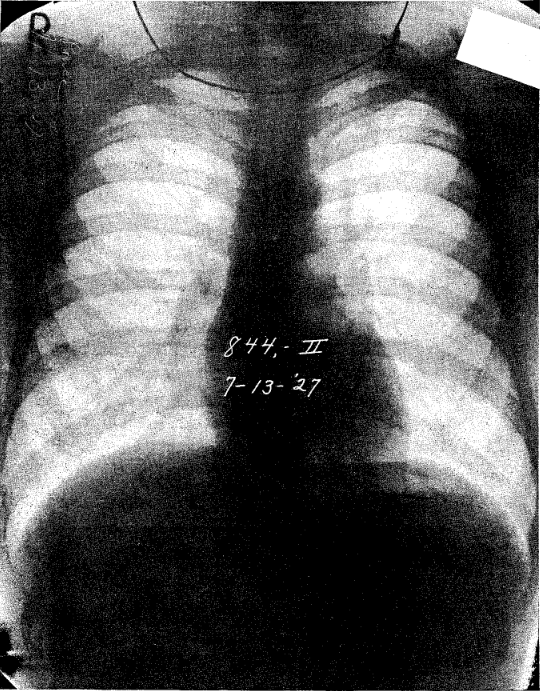
Fig. 4 B, July 13, 1927, twelve months later, shows left apex improved but still unhealed.
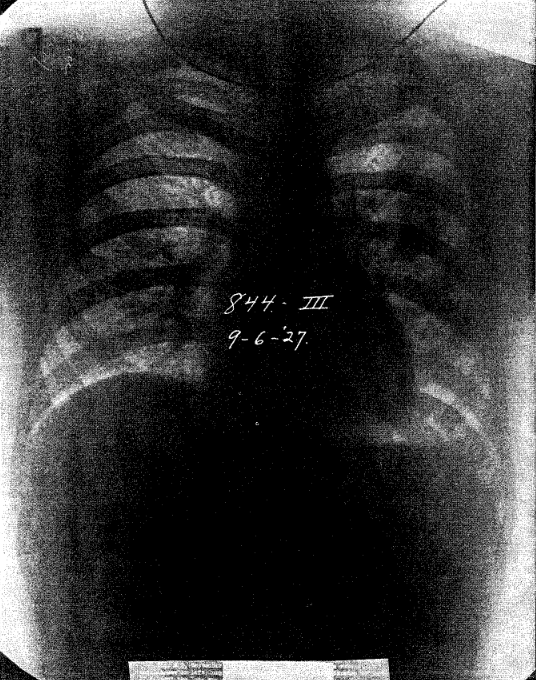
Fig. 4 C, September 6, 1927, two months later, shows extension of the disease in left lung. Owing to apparent lack of resistance on part of patient the lung was collapsed.
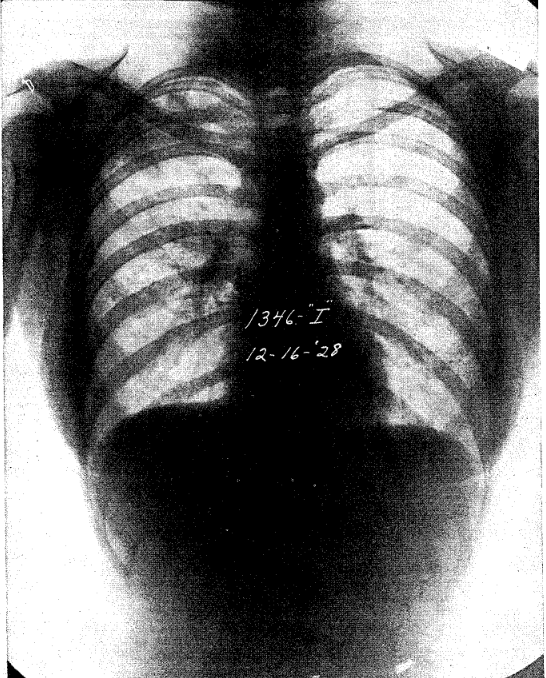
Fig. 4 D, November 12, 1929, shows apex fairly clear, but lung still unexpanded. Patient symptom free.
Figs 5 and 6 represent tuberculosis with acute onset in which cavity was formed very shortly after the first symptoms appeared. Cases such as these have been recently described by Redeker. He recommends that they be treated by the immediate institution of pneumothorax, because he believes that otherwise they will usually fail to heal. We have found, on the contrary, that these lesions usually heal satisfactorily by rest and the regular sanatorium regime, provided treatment is started at once. The healing is by resolution and a mild degree of fibrosis, except in case of the cavity which requires the formation of considerable fibrous tissue. The cavity that heals best is the fresh cavity without too much fibrous tissue about it. Immediate treatment is essential to the successful handling of these cases.
Case No. 9388. Miss R. M. Fig. 5 A, B, and C, are films of a patient with acute onset in which the process was preponderantly exudative in type, with cavity formation within three weeks after the onset of clinical symptoms. The patient was apparently in perfect health when she was taken ill with influenza on Thanksgiving day, 1928. She was examined by me in less than three weeks following the onset of influenza, and gave the picture as shown in Fig. 3 A, taken December 18, 1928. This process, under rest and other sanatorium measures went on to a satisfactory healing, the progress of which is shown in film B, taken August 8, 1929, and film C, taken January 1930.

Figs. 5 A, B and C represent an early exudative lesion with rapid cavity formation, which healed under regular sanatorium regime, without mechanical interference. Three weeks before onset of symptoms patient was attending High School. An attack of influenza was accountable for the acute onset of tuberculosis. Sputum became negative.
Fig. 5 A, December 16, 1928, shows acute exudative infiltration in the upper third of right lung, with cavity formation.
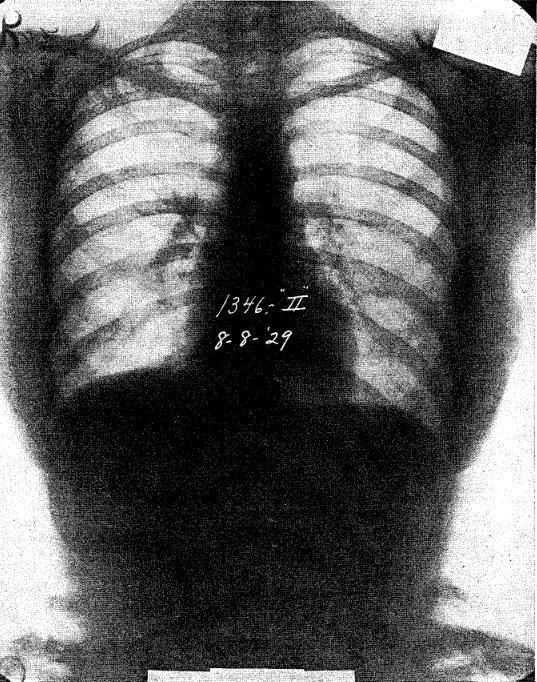
Fig. 5 B, August 8, 1929, shows cavity healing.
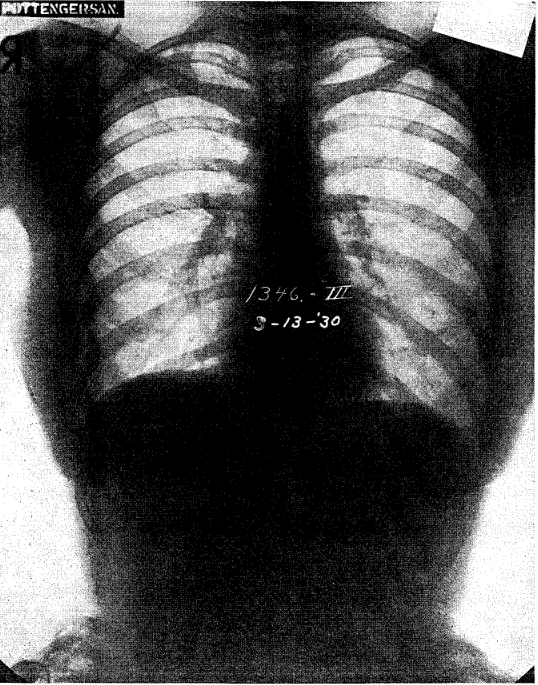
Fig. 5 C, March 13, 1939, shows cavity healed.
Case No. 9679. Miss G. M. Fig. 6 A and B, represents a similar acute process. Patient gives history of dieting for overweight until August 7, 1929, when she had two teeth removed and failed to regain her usual health thereafter. In September she noticed a cough with expectoration, and a temperature of 101°, and severe pain over the right lung. On October 13, the film shown in Fig. 4 A was taken, in which there is an extensive right-sided involvement, with definite cavity formation.
Patient was put on rest and given the usual sanatorium treatment. She had a temperature of 101° for about a month, when it subsided, and with its subsidence the cough and sputum disappeared. Film B, taken on January 13, 1930, shows that the cavity has disappeared. This patient is not yet well, but is rapidly recovering.* (*August 10, 1930–cavity healed.)
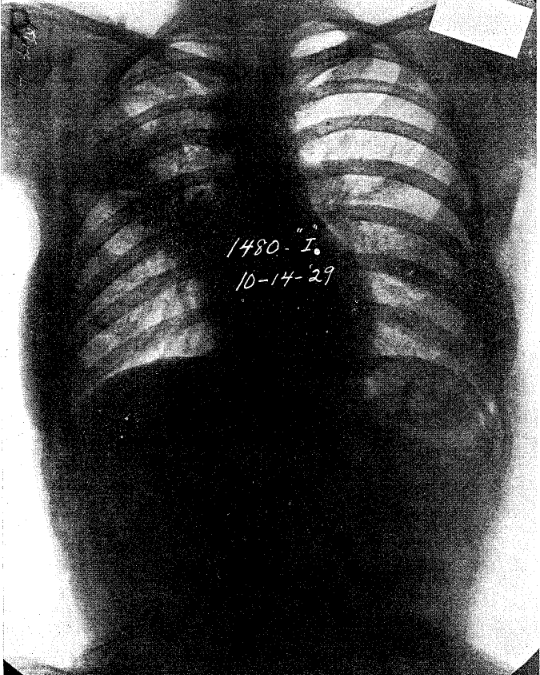
Fig. 6 illustrates the healing of acute exudative tuberculosis with subclavicular cavity, under regular sanatorium regimen, without mechanical interference of any kind. Sputum became negative.
Fig. 6 A, October 14, 1929, shows very extensive infiltration of the upper half of right lung. with cavity.
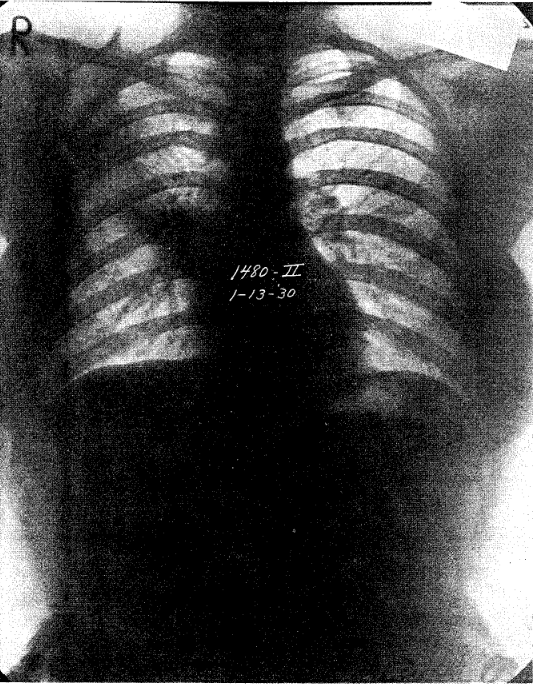
Fig. 6 B, January 13, 1930, shows cavity disappearing and healing progressing satisfactorily.
We also see the tendency to heal in many cases which are of longer standing, even though temperature has persisted for a considerable time. The determining factor seems to be the way the patient’s physiologic balance is restored, together with the degree of specific defense that he is able to establish.
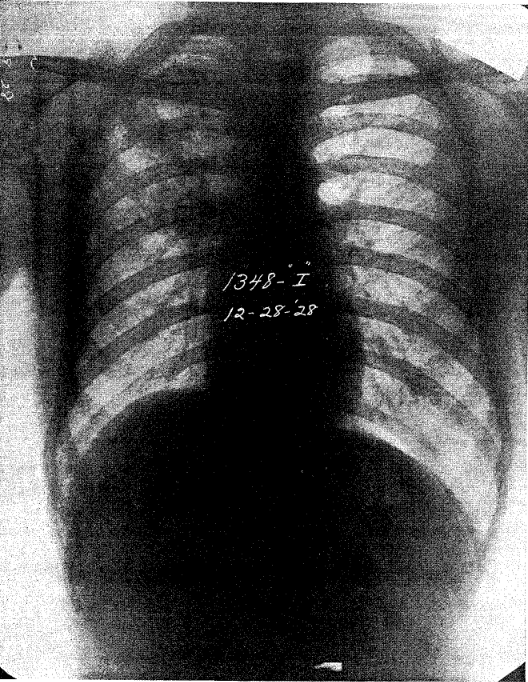
Case No. 9395. Mr. S. H. Fig. 7 A, B, C, and D, illustrates an advanced combined proliferative and exudative lesion with excavation. The patient entered the sanatorium on December 28, 1928. He had been treated by me for an early tuberculosis occupying the upper portion of the right lung, some six years before, and had made a recovery. In July 1928 he had an acute respiratory infection, accompanied by high temperature, which was diagnosed as influenza. Recovery was slow. After recovery from the influenza he again had a rise of temperature accompanied by a persistent cough and expectoration. Failing to make satisfactory improvement, he was sent to the sanatorium, with the condition as shown in film A. There are several areas of loss of tissue in the upper half of the right lung. In his temperature chart, shown in Fig. 8, it will be noticed that during the first six months he had considerable elevation of temperature. Film B, taken February 8, 1929, shows a slight increase in the exudative character of the lesion, but no increase in destruction of tissue. Film C, taken May 10, 1919, shows a very marked increase in the exudative type of the lesion, but a general improvement in the areas of involvement in the second and third interspaces. These changes had taken place during a course of continuous temperature, which we assume accompanied repeated reinoculations of bacilli and bacillary protein, as will be seen in Fig. 8. Shortly after this all appreciable reinoculations ceased; the temperature came to normal; the tuberculous inflammation proceeded to heal by resolution and fibrosis. Film D, taken January 22, 1930, shows the extent to which the right lung has cleared to date.
The clinical improvement in this case was exceptionally gratifying. Upon entering the sanatorium his sputum was 160 cc in 24 hours, with 250 tubercle bacilli per microscopic field. At the time film B was taken, it was 160 cc in 24 hours, with 100 tubercle bacilli per microscopic field. When film C was taken it had dropped to 65 cc in 24 hours, with 6 tubercle bacilli per microscopic field. When film D was taken it was 2 cc in 24 hours, with 30 tubercle bacilli per microscopic field. While the lesion is not quite healed, yet it is rapidly approaching that state. This shows that a far advanced destructive lesion can be turned to a favorable ending, provided cooperation can be had for a sufficient length of time.* (August 10, 1930. Now healed and bacillus free.)
Figs. 7 A, B, C, and D illustrate healing of extensive combined proliferative and exudative tuberculosis, with cavity formation, under regular sanatorium regimen, without mechanical interference. The temperature, pulse and weight of this patient are shown in Fig. 8.
Fig. 7 A, December 28, 1 928, shows marked involvement of upper two-thirds of right lung; slight involvement in left; multiple cavitation in right.
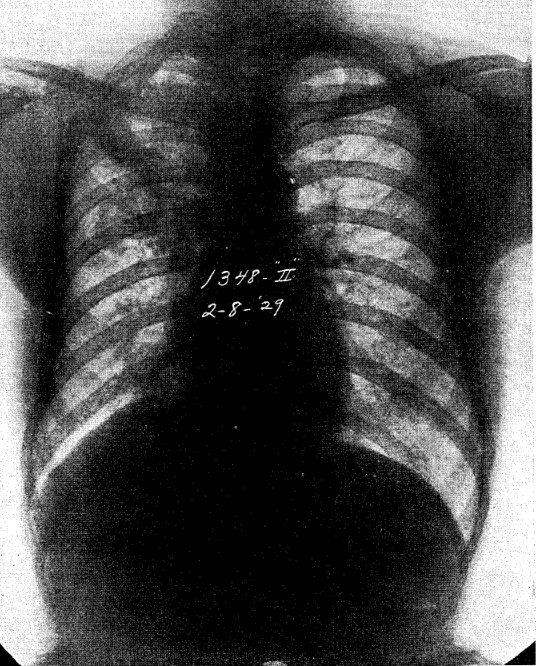
Fig. 7 B, February 8, 1929, shows extension of the disease in lower right lung and also in central portion of left lung. At this time an unsuccessful attempt was made to collapse lung.
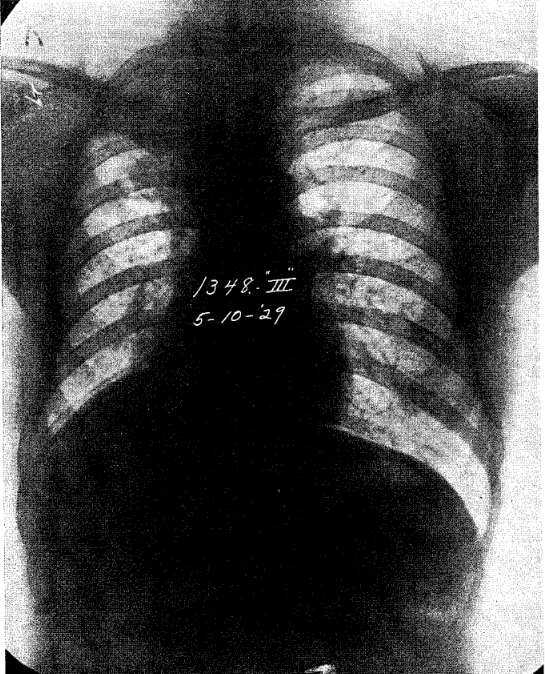
Fig. 7 C, May 10, 1929, shows the beginning of resolution in the middle portion of right lung; pleurisy over the apex.
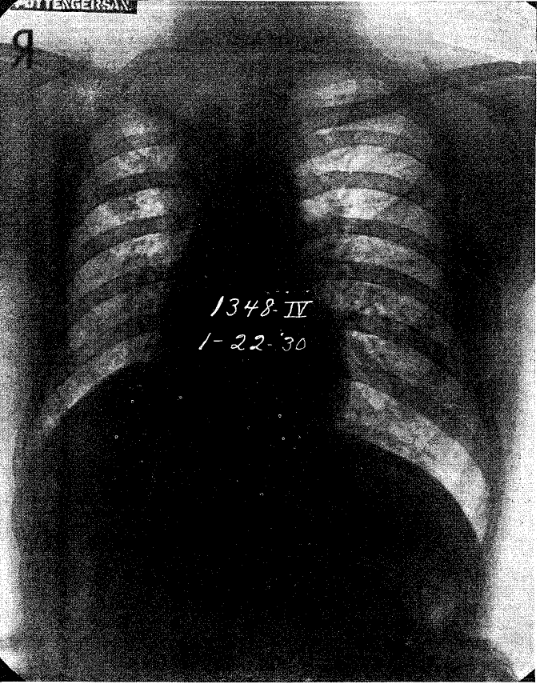
Fic. 7 D, January 22, 1930, shows almost complete absorption of exudate through right lung.
Patients who show a preponderantly exudative reaction are usually considered as belonging to a more serious group, but they too will often heal even though the disease is widespread.
Case 7670. Mrs. W. J. Fig. 9 A and B, illustrates an extensive fibrocaseous tuberculosis, with marked allergic reaction causing a severe exudative process. The patient had been ill for more than a year; had lost weight to eighty-five pounds, and had had fever for several months. On entering the sanitorium (Fig. 9, film A) she had a temperature of 101°. The sputum shows 30 cc in 24 hours, with 100 tubercle bacilli per microscopic field.
The patient was under the usual sanatorium treatment. On May 9, 1927, eighteen months later, the lung fields had practically cleared, as shown in film B. At that time she was free from cough, expectoration and tubercle bacilli, and weighed 105 pounds. The case illustrates the natural healing of an extensive lesion largely by resolution.
Temperature Chart
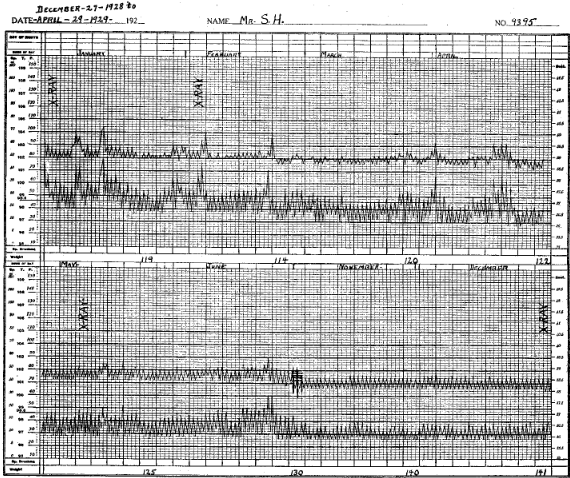
Fig. 8 illustrates the temperature and pulse of the patient whose films are shown in Fig. 7 A, B, C and D. Patient had constant temperature during first two months, followed by remission during the third month;and again followed by two periods of prolonged temperature in the latter half of the third and fourth months.
Temperature then dropped, remaining below normal for the most of the time except during early May and the latter part of June. Temperature again dropped to below normal, where it remained, as is shown in the latter portion of the chart.
Patient’s weight decreased from 119 to 114 during the first two months. After that patient made steady gain in weight until 141 lbs. was reached, January 1920.
Sputum, December 1928, 160 cc in 24 hours, with 250 tubercle bacilli per microscopic field; December 1929, 2 cc in 24 hours, with 30 tubercle bacilli per microscopic field.
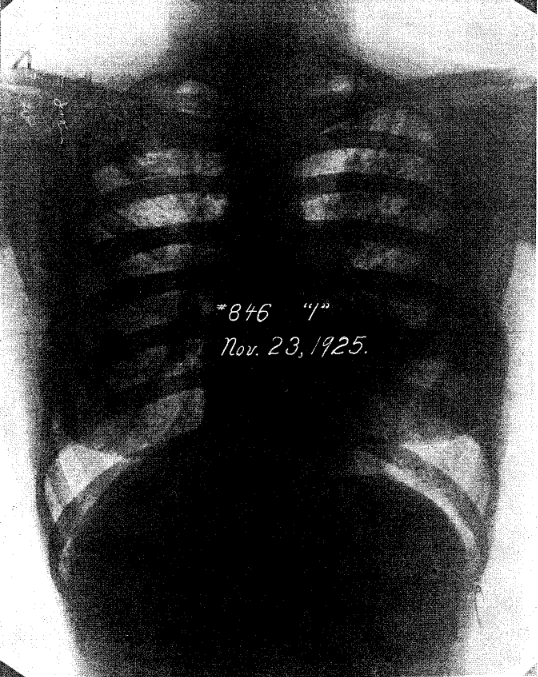
Figs. 9 A and B illustrate an extensive fibrocaseous tuberculosis with marked allergic exudative inflammation, which healed under regular sanatorium regimen, without mechanical interference. Sputum became negative.
Fig. 9 A, November 23, 1925, shows extensive exudative process in both lungs.
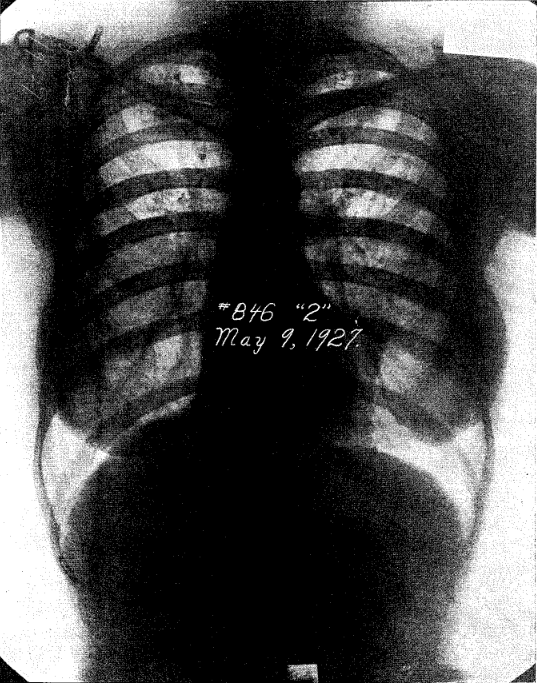
Fig. 9 B, May 9, 1927, shows a very marked clearing, although marked shadow due to proliferative process and also deposits of calcium, remain in the upper portion of both lungs. Marked pleuro-pericardial adhesions on left side will also be noted.
In cases where a satisfactory physiologic balance can not be restored and immunity can not be built up, the disease will spread in spite of all that can be done. Such patients suffer severe reinoculations accompanied by marked allergic response. Toxicity is marked, and even with moderately low temperature, they continue to show toxic symptoms. Healing under these circumstances usually fails. We must either assume that the lesion is caused by bacilli of unusual virulence, or that the numbers of bacilli in the reinoculations are extremely large, or that the resistance on the part of the individual is very low; or it may be that all of these conditions are present. The case which follows illustrates this type.
Case No. 9443. Miss M. W. Fig. 10, A, B, C, and D, illustrates an acute onset with an exudative lesion in the upper portion of the right lung, which went on to cavitation and death of the patient in spite of treatment. This patient had been working up until two weeks before she entered the sanatorium. Film A was taken February 17, 1929, when patient was having considerable temperature. This went on to cavity formation, regardless of treatment, as shown in film B, taken May 20, 1929. Film C, taken August 27, 1929, shows an increase in the exudative reaction in the upper portion of the right lung, and film D, taken October 7, 1929, shows a very extensive excavation of the right apex. It will be noted, however, that in spite of the severity of the disease there was very little extension of infection in the left lung. Not until film D was taken was any particular extension shown, and this was taken only about three weeks before death, following a general breaking down of the patient’s resistance.
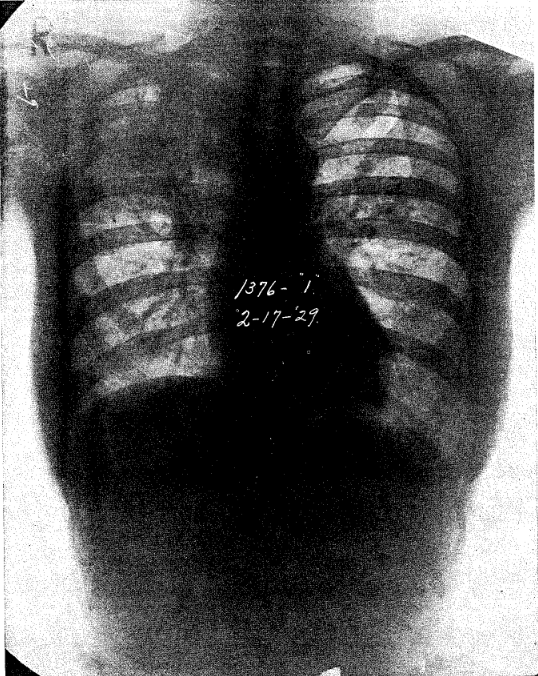
Figs. 10 A, B, C, and D show an acute exudative lesion involving upper half of right lung and middle portion of left lung, which extended regardless of treatment. Patient died from extension of disease, with meningeal involvement. Patient was not able to muster sufficient resistance to bring the disease to a standstill.
Fig. 10 A, February 17, 1929, shows acute exudative lesion in the upper half of right lung, with cavity formation near apex; a moderate lesion in the middle of left lung. Patient was severely toxic.
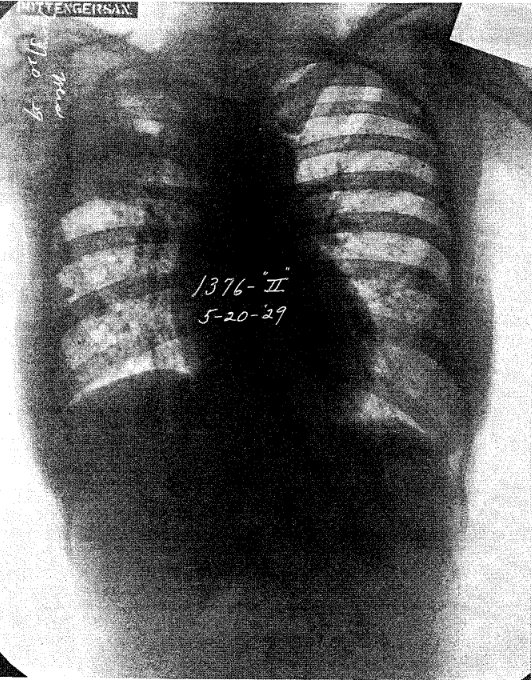
Fig. 10 B, May 20, 1929, shows increase in exduation and cavity more definitely formed; lesion in right lung much the same as in Fig. 10 A.
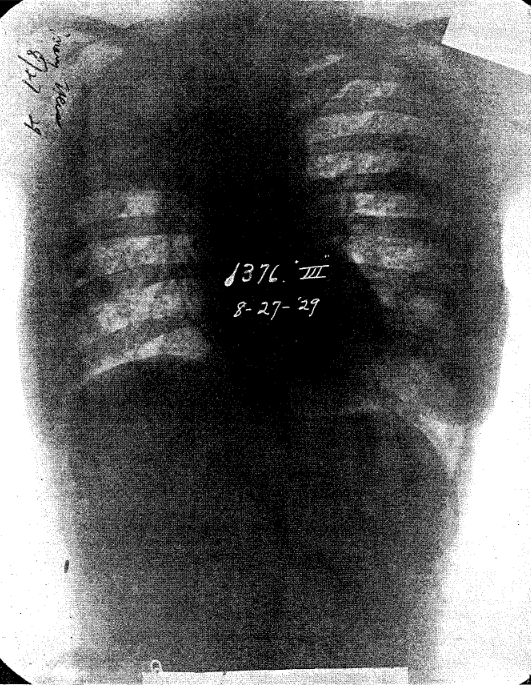
Fig. 10 C, August 27, 1929, shows the lesion still markedly exudative; extension of infiltration in left lung.
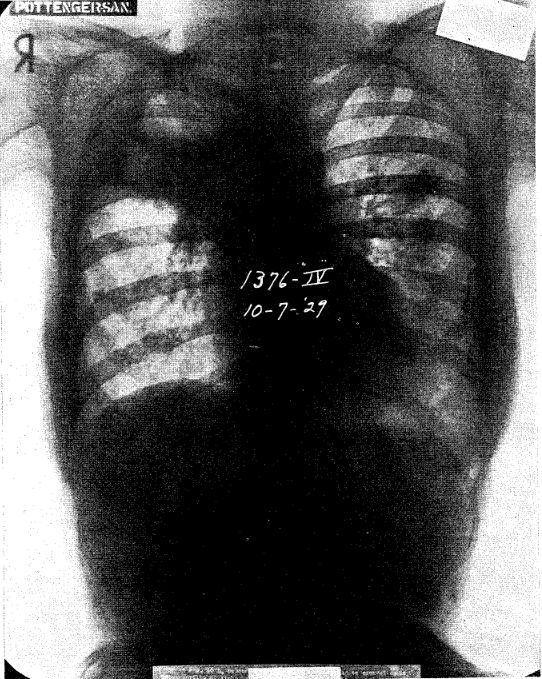
Fig. 10 D, October 7, 1929, shows a more definite excavation in upper portion of right lung; some disappearance of the pleural haze; very marked extension in left lung.
Preponderantly fibroid lesions are usually spoken of as being the most favorable type. This is probably due to the fact that they exist for a long period of time and are of a milder degree. The difficulty with a preponderantly fibroid type, however, is that the patient is apt to delay treatment until he is seriously handicapped by extensive fibrosis, general emphysema, pleural adhesions, and until the disease is beginning to take upon itself more active and destructive aspects, all of which produce permanent and serious effects. The patient can live comfortably with this form of the disease for a long time, but from the standpoint of healing, it has been my experience that it is not so favorable, or at least not more favorable than the more acute types, because the latter will heal and leave a much freer lung field than the preponderantly fibroid type.
Case No. 9438. Mr. A. R. Fig. 11 A, B, and C, represents an extensive lesion preponderantly proliferative in character. This patient had been working continuously, free from symptoms of any character, until a hoarseness was noted, which interfered with his work as a salesman. On consulting a throat specialist, an ulceration was found in the larynx, which involved the cords and arytenoids, and on examination of the chest revealed an extensive lung involvement. The extent of this is shown in Fig. 11, film A, taken February 12, 1929. It will be noticed that there is an exudation of mild degree in numerous areas on this plate, in both lungs, although the process as a whole is preponderantly proliferative. This patient improved satisfactorily under sanitorium regime, as may be inferred from film B, taken August 7, 1929, and film C, taken January 22, 1930.
This case illustrates how the lung fails to clear in a preponderantly proliferative lesion; even though healing has been attained. New tissue has been formed, which replaces the elastic tissue of the normal lung. Although healing is nearly accomplished, as shown in film C, many shadows continue to show. Contrasting this with the preponderantly exudative types Figs. 3, 4 and 9, it will be seen that in the latter the lung field clears, leaving very few shadows on the plate.
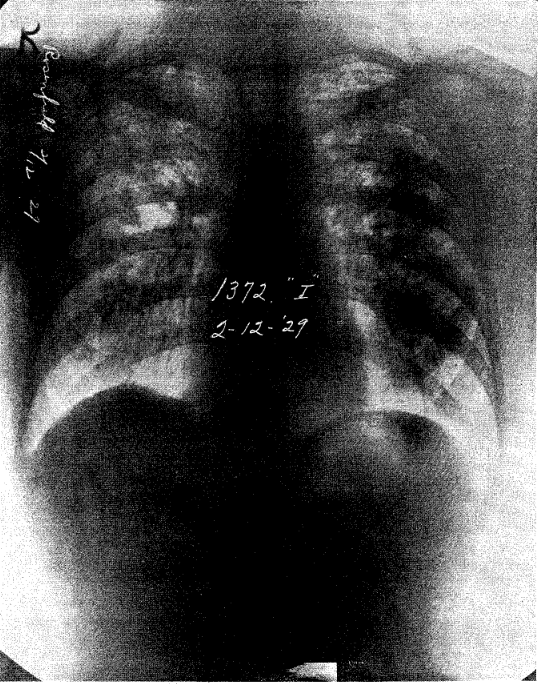
Figs. 11 A, B, and C represent preponderantly proliferative lesion. Regardless of the extent of the lesion, as shown in Fig. 11 A, February 12, 1929, patient did not know he was ill until hoarseness from laryngeal ulceration developed one week previously. Extensive proliferation is shown through the major portion of both lungs, with areas of increased exudation scattered through.
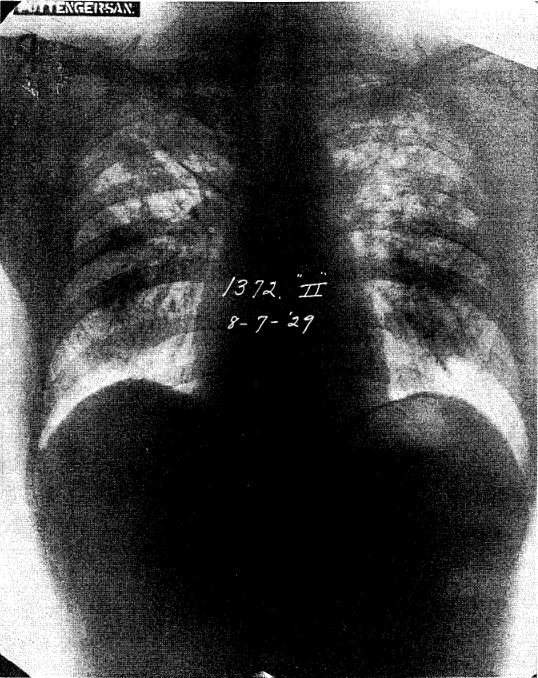
Fig. 11 B, August 7, 1929, shows resolution of a considerable portion of the exudation.
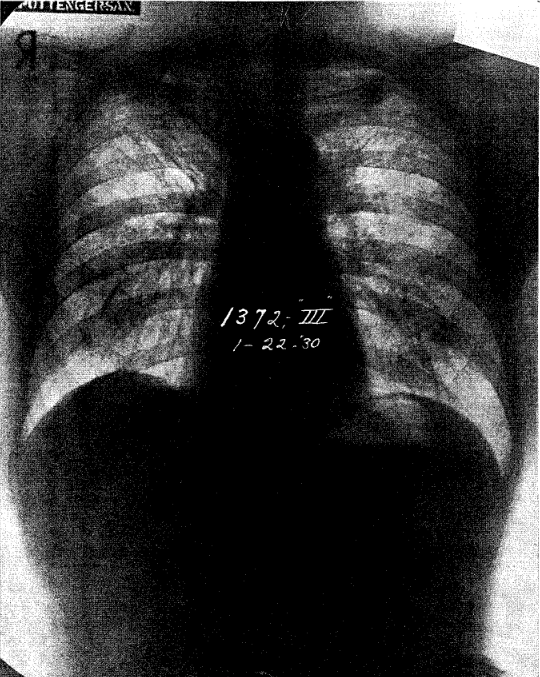
Fig. 11 C, taken January 22, 1930, shows a continued resolution, but the lung fields still show extensive shadows due to the chronic proliferative process. Such lesions leave far more evidence of infection in the lung than do the preponderantly exudative type, which clear largely by resolution.
We are probably justified in assuming that the difference between a preponderantly exudative and a preponderantly proliferative lesion is a difference in the specific defense. In the preponderantly exudative type we have a higher sensitization of cells and a more active allergic reaction. In the preponderantly proliferative type sensitization is much less in evidence and the allergic reaction only takes place to a minimal degree. The difference in the lesions might be due to a difference in the virulence of bacilli, a difference in reaction on the part of the patient, or to the establishment of a more complete immunity, in which sensitization and the allergic inflammatory process take a lesser part. In the preponderantly proliferative group, the toxic symptoms are usually mild, in fact, they are often absent until the disease becomes very extensive; while in the exudative group, the toxic symptoms are marked and come on early.
From these illustrative cases it may readily be seen how tuberculosis tends to heal under favorable conditions; how the patient may become desensitized to his own and to bacillary protein, which enables him to withstand severe disease for long periods of time; and too, how, now and then the disease will spread and cause a severe and fatal illness without calling out an effective specific resistance.
Summary
- Tuberculosis heals as a result of the patient’s immunity reaction.
- The efficiency of the immunity reaction is increased by repeated reinoculations.
- The effects of immunity are shown in the following services rendered to the host:
- Destruction of bacilli.
- Retardation of the passage of bacilli through the tissues
- Elimination of bacilli through. natural channels by caseation and cavity formation.
- Development of a state of desensitization to bacillary and non-bacillary toxins.
- Encapsulation or rendering inactive viable bacilli which remain in the tissues.
- Ridding the body of the inflammatory products which accompany the infection.
- Repair of the injury inflicted upon the body by the disease.
- Treatment is efficacious to the extent that it is able to limit reinoculations of bacilli and bacillary protein to a minimum and create within the patient a resistance capable of coping with them as they occur.
References Cited:
- McCutcheon, Morton; Strumia, Max; Mudd, Stuart; Mudd, Emily B. H. and Lucke, Baldwin: “On the Mechanism of Opsonin and Bacteriotropin Action. III. The Development and Effect of the Antibodies found in Experimental Tuberculosis of Rabbits.” Jour. Exp. Med., 1929, Vol. 49, p. 815.
- Opie, Eugene I.: “The Pathogenesis and Transmission of Tuberculosis.” Am. Jour. Med. Sci., Jan. 1930, Vol. CLXXIX, No. I, pp. 104-118.
- Krause and Hofer: “Bakteriolyse.” Deutsch. med. Wochenschr., 1912, No. 26.
- Wolff-Eisner, A.: “Die neue Erklärung der Tuberkulinwirkung.” München. med. Wochenschr., 1908, No. 35.
- Metschnikoff, Elie: Immunity in Infective Diseases. Cambridge Press, 1905.
- Wright, Sir A.: Studies on Immunization. London: Archibald Constable Co. Ltd., 1909.
- Rich, Arnold, Rice and McCormick, Howard A.: “An Enquiry Concerning the Role of Allergy, Immunity and Other Factors of Importance in the Pathogenesis of Human Tuberculosis.” Bulletin of the Johns Hopkins Hospital, 1929, Vol. XLIV, pp. 273-425.
- Lurie, Max Von B.: “The Fate of Tubercle Bacilli in the Organs of Reinfected Rabbits.” Jour. Exp. Med., 1929, Vol. L, p. 747.
- Koch, Robert: “Fortsetzung der Mitteilungen über ein Heilmittel gegen Tuberculose.” Deutsche med. Wochenschr., 1891, Nr. 3.
- Krause, Allen K., and Willis, H. S.: “Studies on Immunity to Tuberculosis. The Results of Virulent Reinfection into Tuberculin-reacting Areas (Skin) of Tuberculous Guinea-pigs.” Amer. Rev. Tuberc, 1920, No. 8, 563.
- Krause, Allen K., and Willis, H. S.: “The Dissemination of Virulent Tubercle Bacilli after Infection and Reinfection.” Transactions National Tuberculosis Assn., 1924.
- Pottenger, F. M.: “Exudative and Proliferative Processes not a Basis for Classifying Tuberculosis into Types But Represent Different Phases of Allergic Reaction.” Am. Rev. Tuberc., Nov. 1928, Vol. XVIII, No. 5.
- Pottenger, F. M.: “Allergy in Clinical Tuberculosis.” Tubercle, London, John Bale, Sons & Danielsson, Ltd., June 1929, Vol. X, No. 9, p. 409.
- Opie, Eugene L.: “Inflammation and Immunity.” Jour. of Immunology, 1929, Vol. XVIl, p. 329.
- Opie, Eugene L.: “The Fate of Antigen (Protein) in an Animal Immunized against It.” Jour. Exp. Med., 1924, Vol. XXXIX, p. 659.
- Cecil, R. L., and Blake, F. G.: “Studies on Experimental Pneumonia. IV. Results of Prophylactic Vaccination Against Pneumococcus Pneumonia in Monkeys.” Jour. Exp. Med., 1920, Vol XXXI, p. 519.
- Pottenger, F. M.: “Factors Fundamental to Healing in Tuberculosis.” Proceedings of the Inter-State Post Graduate Medical Assembly of North America, 1927. Am. Rev. Tuberc., 1928, Vol. XVII, No. 5, p. 459.
- Pottenger, F. M.: “Similarities and Differences in Bacterial and Nonbacterial Allergy.” The Jour. of Allergy, 1930. Vol. 1, No. 3, p. 235.
- Bartel, J.: “Das Stadium lymphoider Latenz im Infectionsgӓnge der Tuberkulose.” Wien. klin. Wochenschr., 1913, No. 13, p. 485.
- Opie, Eugene L.: “Pathology of the Tuberculosis of Childhood and Its Bearing on Clinical Work.” Brit. Med. Jour. 1927, pp. 1130-1135.
- Pottenger, F. M.: “The Physiologic Basis of Rest as a Therapeutic Measure in Pulmonary Tuberculosis.” Annals of Clin. Med., Sept. 1924, Vol. III, No. 3.
- Sauerbruch, F., Herrmannsdorfer, A., and Gerson, M.: “Attempts to Influence Grave Forms of Tuberculosis by Diet.” München. med. Wchenschr., 1926, Vol. 73, pp. 47-51, Jan. 8.
- Sauerbruch, F., Herrmannsdorfer, A.: “Ergebnisse und Wert einer diätetischen Behandlung der Tuberkulose.” München. med. Wchenschr., 1928, Vol. 75, pp. 35-38, Jan. 6.
- Mayer, Edgar and Kugelmass, I. Newton: “Basic (Vitamin) Feeding in Tuberculosis.” J.A.M.A., 1929, Vol. 93, No. 24 (Dec. 14).
- Long, Esmond R.: “Tuberculin and Tuberculin Reaction.” Reprint from The Newer Knowledge of Bacteriology and Immunology. Ed. by E. O. Jordan and I. S. Falk, University of Chicago Press.