
Access to all articles, new health classes, discounts in our store, and more!
Effects of a Raw Food Diet on Hypertension and Obesity
Published in Southern Medical Journal, Vol. 78, No. 7, July 1985.
* * *
ABSTRACT: We examined responses to cooked and uncooked food in 32 outpatients with essential hypertension; 28 were also overweight. By varying cooked and uncooked food percentages and salt intake, patients acted as their own control subjects in this unblinded study. After a mean duration of 6.7 months, average intake of uncooked food comprised 62% of calories ingested. Mean weight loss was 3.8 kg and mean diastolic pressure reduction 17.8 mm Hg, both statistically significant (P <.00001). Eighty percent of those who smoked or drank alcohol abstained spontaneously.
Since 1970 we have studied responses of patients with two important health problems, obesity and hypertension, to uncooked diets. We interviewed nonpatients living on raw food and found them lean and normotensive. We thus postulated salutary properties for uncooked foods. For ten years we explored this possibility by placing patients (and ourselves) on diets with a high percentage of uncooked food.
Cooked food is commonly considered healthful; however, before the use of fire, man and his evolutionary ancestors ate only uncooked food. When viewed in the perspective of primate life on earth, eating cooked food is a relatively new innovation that might be introducing stressors or removing protective mechanisms. Indeed, there have been reports that cooked diets may not be optimal.1-4 Davies et al1 noted, “There is evidence that heating of a protein modifies its antigenicity. Processed foods could, therefore, constitute an almost unlimited source of possible antigens.”
Methods
Our study included 32 patients (21 men, 11 women) with essential hypertension; 28 also had mild (5% to 15% overweight) to moderate (15% to 40% overweight) obesity. All voluntarily consented to participate in the program. Sixteen were white, 11 black, four Hispanic, and one Oriental. These patients had minimal or no target organ damage, normal vanillylmandelic acid (VMA), sodium, and potassium levels, and little or no serum urea nitrogen elevation. We used an arbitrary classification to group patients based on diastolic blood pressure (DBP): five had pressure of 119 or higher, ten between 105 and 119, and 17 between 90 and 105.
We advised patients to include at least 40% uncooked foods (vegetables, seeds, nuts, berries, melons, fruits, seed oil, and raw certified milk) in their diets, an increase of 35% over the amount they were eating. Because of a lesser risk of tuberculosis and brucellosis, we preferred raw goat milk to raw cow milk. We recommended reasonable portions, but put no limits on numbers of meals, food quantity, or calorie consumption. Although reports state that patients have eaten uncooked eggs, fish, and animals,4 we proscribed this because of possible infection and parasitic infestation.
Initial physical and laboratory examinations were followed by office visits on a four- to six-week schedule (usual for hypertensives). Patients taking medication continued it unless response to the diet was sufficient to allow drug discontinuation. Medications were added to the regimen only when blood pressure response was inadequate, or when ingestion of raw food fell to levels below 15%. One physician treated all patients. At each visit, weight, blood pressure (average of two recumbent readings after a five minute rest), medications, symptom changes, and current dietary percentages of uncooked food were recorded. Since efficacy of a diet depends partly on patient compliance, we judged this by their food diaries and their answers to questions about availability and prices of uncooked food (presumably, only patients following the test diet would be likely to answer correctly). Although an outpatient milieu has the disadvantage of uncertain compliance, we believe it provides more clinically relevant information than a metabolic ward whereby patients are removed from the stress of daily living. A double-blind study was impossible, but by varying consumption of uncooked food and salt, each patient presumably acted as his own control. Close clinical observation of responses and side effects during this study would, we thought, provide evidence for or against efficacy of the test diet.
Data generated were statistically evaluated using the t-test for paired observation. Average percentage of uncooked food was calculated for each patient and for all patients collectively. Changes in body weight and diastolic blood pressures were calculated from differences between pretreatment and posttreatment values. Pretreatment values were obtained when the diet was 5% uncooked and, in some instances, when the patients had discontinued medication. Posttreatment values were those of the most recent drug free month (where possible) during which the test diet had been continuously 30% or more raw. We also attempted to correlate weight loss and DBP decrease with “raw-food months.” We defined raw-food months as the equivalent number of months each patient was ingesting a totally raw diet (eg, one raw-food month equaled a 50% uncooked diet for two months or a 20% uncooked diet for five months).
Results
Mean weight loss was 3.8 kg with a standard error of 0.73 kg, which is highly statistically significant (P <.00001, t = 5.21 on 31 degrees of freedom). The 95% confidence interval for the mean weight loss is from 2.3 kg to 5.3 kg, which does not include zero kg. The 28 patients who were overweight at the start of the study lost an average of 4.4 kg. Twenty-four of the 32 patients lost weight, with 21 losing 2.2 kg or more. These 21 tended to ingest the highest percentages of uncooked food for the longest time. Figure 1 displays the relationship between mean weight loss and raw-food months for all patients.
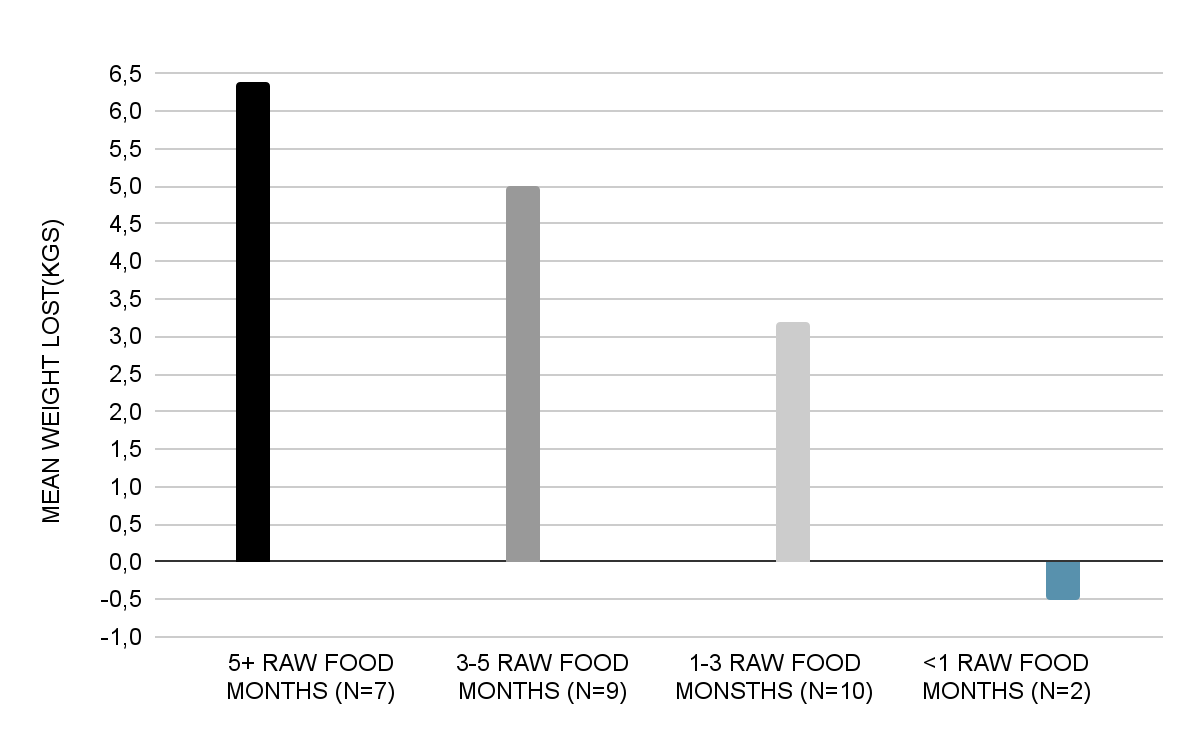
Figure 1. Mean weight loss in overweight patients by raw-food months (N = 28).
The mean reduction in diastolic blood pressure was 17.8 mm Hg for 32 patients with a standard error of 1.7 mm Hg. This yields a highly statistically significant t value of 10.1 on 31 degrees of freedom (P <.000001). Five patients receiving concomitant drug therapy were able to discontinue their medication. Fourteen patients who would have received anti-hypertension drug therapy were managed by diet alone; an additional four patients had poor diastolic blood pressure response to the test diet and required medication. When responders decreased their percentage intake of uncooked foods, their diastolic blood pressure rapidly returned to pretest values. The lack of relationship between mean diastolic blood pressure decrease and raw-food months is shown in Figure 2.
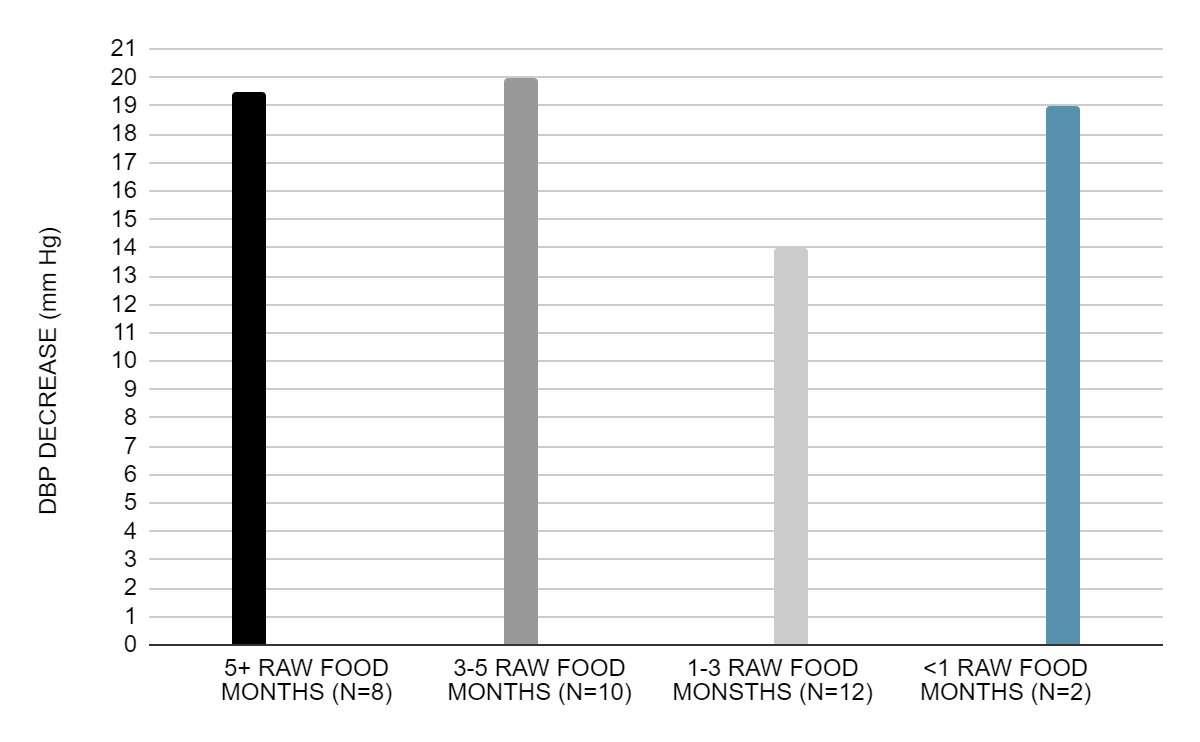
Figure 2. Mean decrease in diastolic blood pressure by raw-food months (N = 32).
The decrease in diastolic blood pressure was highest in the five patients with initial DBP greater than 119 mm Hg. Their DBP decreased 24.8 mm Hg (standard error of 3.9 mm Hg, t = 5.36 on 4 df, P = .002). The second group of ten patients had initial DBPs ranging from 106 to 119 mm Hg. They dropped an average of 21.0 mm Hg (SE of 2.9 mm Hg, t = 7.24 on 9 df, P <.00001). In the 17 patients with initial DBPs of 90 to 105 mm Hg, the mean decrease was 13.9 mm Hg (SE of 2.0 mm Hg, t = 6.95 on 16 df, P <.00001).
Although both weight and blood pressure decreased in the 32 patients, the correlation of 0.07 between the decrease in weight and decrease in diastolic blood pressure did not approach statistical significance. Figure 3 shows that of the five patients with the greatest decrease in weight, two had a small decrease in diastolic blood pressure, two had a large decrease, and one had an average decrease.
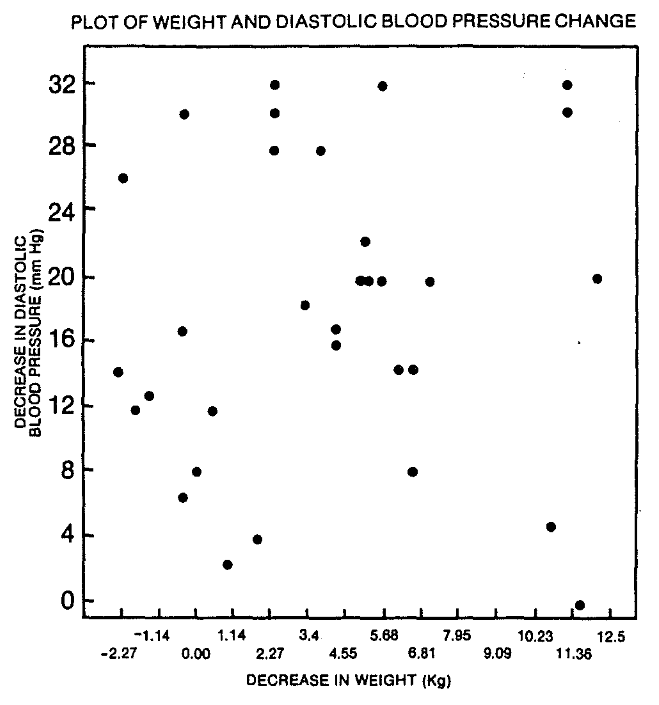
Figure 3. Decrease in diastolic blood pressure (DBP) versus decrease in weight (N = 32, r = .074).
To determine whether weight and blood pressure changes were due only to sodium reduction, we had eight posttest patients use salt ad lib (salt shaker allowed) after they had achieved clinically acceptable weight and blood pressure. Weight did not change appreciably; although a blood pressure rise of 4 to 6 mm Hg occurred, all readings were below pretest values.
Patient acceptance of uncooked diets appeared good: all reported using 40% or more uncooked foods. Although 60% to 70% levels were generally associated with good responses, some patients at first experienced mild weakness and more frequent stools (reduced gastrointestinal transit time). Constipation and indigestion were less problematic, and the feeling of having overeaten was rarely noted, even after a large meal.
Several social factors were reported. Dining out was more difficult, and more frequent shopping was required. Limited food choices sometimes) engendered feelings of “being left out” during celebrations with friends and families where only ordinary foods and beverages were served. Despite these constraints, most patients reported that they continued to eat high percentages of uncooked foods even after the study was over.
Side effects reported included increased sensitivity to alcohol, cigarette smoke, chemical odors, and medication. Approximately 80% of the patients who smoked or drank reported that they abandoned these habits. Several also had nausea, vomiting, and malaise after typical restaurant or banquet dinners. Certain foods (citrus fruits, nuts, tomatoes), too, gave rise to gastrointestinal, cutaneous, musculoskeletal, and central nervous system symptoms, though these were mild.
Discussion
Diets containing a high percentage of uncooked foods are significantly associated with weight loss and decrease in diastolic blood pressure in these patients. Still, there are important questions as to why this diet works, since the mechanisms of action remain hypothetical.
In obesity, possibly the reason is that the raw diet is more satiating. Cooking can cause loss of up to 97% of the water-soluble vitamins (B and C) and up to 40% of the lipid-soluble vitamins (A, D, E, and K)5 without decreasing calories. Uncooked food thus may contain more vitamins and, thereby being more satiating, may reduce caloric intake and lower weight.3 Supporting this finding, two other patients who were massively obese claimed high percentage raw diets gave them long-term appetite control not obtained with cooked foods.
Hypotensive effects of a raw diet may occur for somewhat different reasons. Patients switching from the test diet to a cooked diet (without altering caloric or sodium intake) showed rapid increase of blood pressure to pretest values, possibly a function of increased stressors in cooked food. Benefits of raw foods might be ascribed to their low calorie and high fiber content,6 though weight loss had no correlation with blood pressure decrease. Increased fiber content, causing faster intestinal transit, is probably only part of the answer, as some raw diets with little fiber content had similar effects.
Irrespective of food rawness, salt may adversely influence blood pressure.7-8 Nevertheless, eight test patients used salt in quantity and failed to raise DBP to pretest values. (Test patients were told to use salt and the salt shaker sparingly, not to stop using it.) When cooked diets were eaten, however, ad lib salt use raised DBP to baseline levels. Additionally, we attempted to evaluate a potassium effect (because of its putative role as a protectant) by a retrospective analysis of five hypertensive patients. These individuals had taken 2 to 4 tablespoonsful of KC1 daily for more than two months without notable effects on DBP. We also considered a placebo response but doubted this, as the magnitude of mean DBP decrease seemed too large.9
“Milder stressors” in uncooked foods may play a valuable role in health improvement. When cooked, the test diet did not produce the same results; thus, the antigens, excretions of gut flora, and heat labile enzymes associated with raw diets may be more healthful.
For the reasons mentioned, certain people have adopted raw food diets. Obviously, successful raw dieting, usually without professional guidance, should not blind one to the hazards. Inadequate or non biocompatible raw diets can be devastating. Although our test patients did well, persons on long-term, self-choice raw-food diets, especially fruitarian, have died of myocarditis, inanition, and anasarca. Others have lost teeth or developed staphylococcal infections from drinking fruit juice or eating large quantities of fruit, and the mental dysfunctions observed with fasting and certain of these diets range from compromise of judgment and memory to fully developed psychoses.10 We do not recommend exclusively raw-food diets for extended periods without a vitamin B12 source included. Patients should be reminded to be especially careful in washing their raw foods.
To conclude, patients with increased diastolic blood pressure and obesity have shown salutary response to an uncooked diet. We urge critical study to further delineate our hypothesis and those of the researchers who have preceded us, and to determine the scope of clinical utility of the results.
Acknowledgments: We thank Roslyn Alfin-Slater, PhD, Ulnar Register, PhD, H. R. Saraydarian, MS, and John Yudkin, MD, PhD, MRCP, whose advice aided in this project. We also thank Irving Ackerman, MD, Robert Foor, MD, Mr. Ronald Landry, Charles Naness, MD, Irving Page, MD, Bernard Pogorel, MD, Jerrold Rotwein, MD, Leonard Sadoff, MD, Samuel Sapin, MD, and Sheldon Wolf, MD, for helpful comments in preparation of the manuscript.
References Cited:
- Davies DF, Johnson AP, Rees BWG, et al: “Food antibodies and myocardial infarction.” Lancet 1:1012-1014, 1974.
- Douglass JM: “Raw diet and insulin requirement.” Ann Intern Med 82:61-62, 1975.
- Douglass JM, Rasgon I: “Diet and diabetes.” Lancet 2:1306, 1976.
- Walters JD: “Proper nutrition and its relation to hormone therapy.” J Appl Nutr 10:466-470, 1957.
- Priestly RJ (ed): Effects of Healing on Food Stuffs. London, Applied Science Publishers Ltd, 1979, pp 121-156.
- Burkitt DP, Walker ARP, Painter NS: “Diet, fiber and disease.” JAMA 299:1068-1074, 1974.
- “Hypertension–salt poisoning?” (Editorial). Lancet 1:1136, 1978.
- Trowell HC: “Hypertension and salt.” Lancet 2:204, 1978.
- Shapiro AP, Swartz GE, Ferguson DCE, et al: “Behavioral methods in the treatment of hypertension.” Ann Intern Med 85:626-636, 1977.
- Douglass JM, Douglass SN, Schmidt RD, et al: “Nutrition, non-thermally prepared food and nature’s message to man: a method of predicting nutrient compatibility?” J Int Acad Prev Med 7:53-59, 1982.