
Access to all articles, new health classes, discounts in our store, and more!
Dental Infections, Their Dangers and Prevention
Read before the Twelfth Annual Meeting of the Radiological Society of North America, Milwaukee, December 3, 1926. Published in Radiology, May 1928.
* * *
Few, if any, of the general health problems entail more difficulties in diagnosis than do dental infections in relation to systemic disease. The question may also readily be asked whether any causative or contributing factor to the degenerative diseases is more important than focal infections. The problem concerns the radiologists probably quite as much, if not more, than the members of other specialties. Since the interpretation of physical records almost of necessity is related to quantitative expressions, we would expect that, by comparison, quantitative infections will be found disclosed roentgenographically. Large areas of involvement have naturally been taken to signify relatively large quantities of infection. Probably no more serious misapprehension has obtained with regard to dental focal infections than that large zones of radiolucency are indicative of large quantities of infection and small zones indicative of slight infection. This has been based on the premise that the organisms made the chamber of rarefaction. We now know this to be an error. The defensive mechanism of the host makes the zones of rarefaction, and the extent of these zones is in largest part an expression of the individual’s reaction to the irritant.
In order to orient ourselves, let us review the present situation. The current belief and basis of practice is, in my judgment, about as follows: That the roentgen ray will reveal the presence or absence of dental infection, because dental infections produce changes in the supporting structures about an infected tooth in the form of a zone or chamber about the apex of the tooth. This absorption is, in volume, in direct proportion to the amount of infection present, and therefore the danger to the individual is expressed quantitatively by the extent of the zone of rarefaction. The precise measure of this extent is believed to be revealed by roentgenograms. I shall present further evidence, which I find myself unable to interpret in any other way than as contradicting the validity of much of the foregoing premise and as indicating an entirely new basis for judgment.
In my recently published text1 I furnished a quantity of evidence which I shall assume that readers are, in general, familiar with. I have shown, for example, that the presence of an extended zone of pus in the joints and muscles of the limbs of a rabbit is not revealed by the roentgenogram, and have presented other data to demonstrate that dental infections may be present without being revealed.
In Figure 1 there will be seen the two central incisors of each of four individuals.
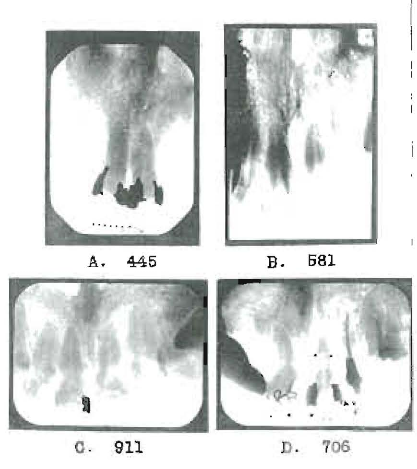
Fig. 1. Four pairs of incisors. One of each pair is putrescent. Three of the patients were seriously ill. The true condition is not revealed.
One central incisor in each case is putrescent, with little or no indication roentgenographically of either the identity of the tooth or the extent of the infection. Three of these individuals are seriously ill and one gravely so, with heart involvement. This raises the question at once: Are we correct in the premise as previously stated; and, if not, why not?
As a further introduction to the consideration of this problem, in Figure 2 we have a comparison of the apparent and actual appearance of a practical case in which, in A and B, above, will be seen the roentgenographic appearance of the first and second 4 molars. In A there is distinct roentgenographic evidence of periapical radiolucence, which is but slightly, if at all, evident about the roots of B, the second molar; and, in A and B, below, we see that the granulomas on these roots are larger on B than A. Why has not the roentgenogram told us the whole truth? (There is no question but that it tells the truth.) Is it not because we do not understand its message?
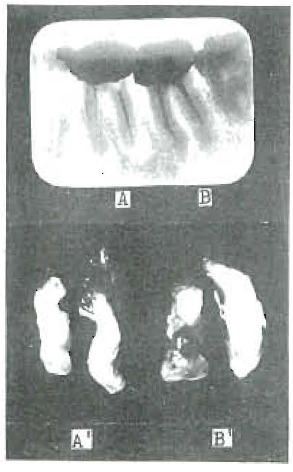
Fig. 2. First and second lower molars (shown in A and B, above), and their roots, with granulomas, after extraction (shown in A and B, below). The granulomas are larger on the second molar than on the first molar, though their presence is not revealed roentgenographically.
In order to determine the explanation for this phenomenon, I have made a series of determinations, some of which are as follows: By taking a piece of beef bone, and for this the sternum (the butchers refer to it as the “brisket bone”) is particularly well suited because it has a considerable portion of spongy bone in proportion to dense, and by cutting it in half and then placing a metal bar, approximately one-fourth inch square but with teeth on one side, between the two pieces, and placing these pieces in a vise and forcing the metal into the spongy bone, an indentation is made the size of the metal bar. This metal bar is shown roentgenographically in position in Figure 3-A. In Figure 3-B we see the photographic appearance of these two indentations, and it will readily be observed that the teeth have registered their imprints in detail in the half in which they were embedded, while the opposite surface is relatively smooth. In 3-C we have the roentgenographic appearance of these two pieces put in juxtaposition, and several important things are at once discernible. The bone looks entirely different on the side to the left where the metal bar had teeth, but since the tooth prints are in alignment, there is a shading of the density, which, if we did not know what had caused it, would not be suggestive. On the other, or right-hand side, where the metal bar was smooth and flat, the hole has a clear-cut limited margin but the bone below it or beside it is more dense than the surrounding bone, because of its condensation. In 3-D we have rotated the two pieces approximately 10 degrees, and the line that separated the two pieces in the middle of the chamber now appears to be to one side of the chamber, and the chamber instead of appearing to be square with a diffused margin at one side where the teeth made their impressions is now oblong and would give one the impression of being only a fraction of the size that it appears in 3-C, while it is actually the same. In 3-E we have the roentgenographic appearance at 20 degrees from 3-C and the margins are lost and the chamber is indistinct. In 3-F we have a view at 30 degrees, and the chamber is nearly lost, as also at 60 degrees in 3-G. In 3-H we see it at 90 degrees, and the chamber does not show, although there is a faint suggestion of the tooth prints. In 3-I we have the roentgenographic appearance of the two halves laid side by side, corresponding with 3-B in position. It will be noted that while the bone was compressed in each half about the same amount, the final distribution of material, due to displacement, is a little different on account of the tapering shape of the teeth; and the half of the bone which received the plain surface of metal shows practically no impression or record of the chamber, shown photographically in the lower part of 3-B.
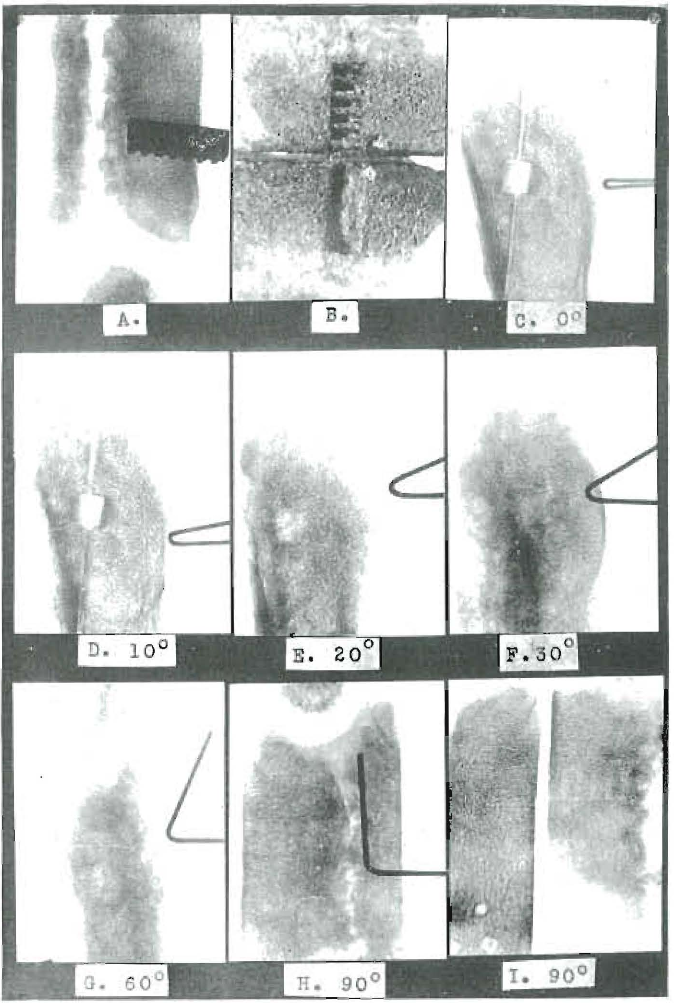
Fig. 3. Chamber in bone at different angles: A, as made by a metal bar, producing a chamber ¼ x ¼ x ½ inch; B, appearance of chambers in separated bones; C, appearance with rays in line with the long axis of the chamber; D (10 degrees); E (20 degrees); F (30 degrees); G (60 degrees), and H (90 degrees) at different angles; (90 degrees), the two pieces separated and roentgenographed at right angles to the long axis of the chamber. The bent wires indicate the angles. There is practically complete disappearance of this large chamber.
What I am desiring to demonstrate here is the effect of a zone of condensation when it occurs in the same path as an area of rarefaction. This is quite clearly demonstrated in Figure 4. In this case, a square-ended punch was driven into the bone, as shown in 4-A, and the bone was then roentgenographed without the tool in position (in 4-B) in the same direction in which the presence of the chamber is but slightly recorded, and in 4-C, at right angles to the chamber which not only shows the chamber distinctly but the condensed bone, which was nearly equivalent in total absorptive quality to the same bone before the tool was driven.
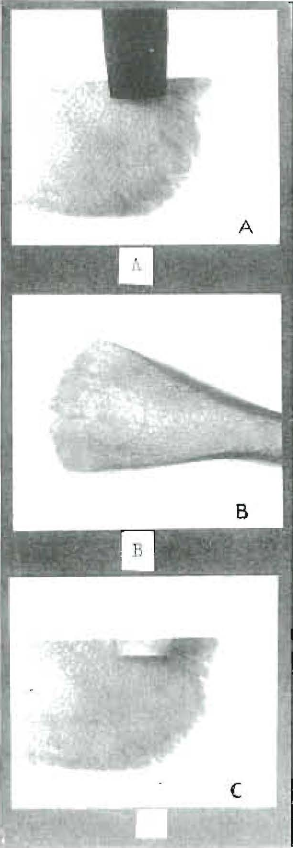
Fig. 4. Limitations of roentgen ray to disclose chamber in bone: 4, square-end punch in position; B, perpendicular roentgenographic appearance of chamber; C, right angle appearance of chamber. A zone of condensed bone obstructs the view in B.
We have here a duplicate of the physical condition that is found in dental practice, though it is produced by a different process. In Nature, the zone of condensation around the chamber of rarefaction is produced as part of the reaction process, and when superimposed above the zone of rarefaction, more or less completely disguises or obliterates its presence. We shall discuss later when and why Nature builds this type of bone.
That this is just what is happening when teeth are roentgenographed for evidence of infection is abundantly demonstrated by the clinical findings. In Figure 5 will be seen the photographic appearance alongside the roentgenographic appearance of a number of extracted teeth in cases in which the granuloma remained attached to the root and by its presence could demonstrate the size and shape of the chamber from which it had been removed. The men who have been doing surgical work in these conditions are all familiar with the frequency with which they find the physical condition very different from that suggested by the roentgenogram. Since we are studying here only the question of the limitations of the roentgen ray, I am not justified, because of the large number of problems we wish to cover in taking more time for this particular phase.
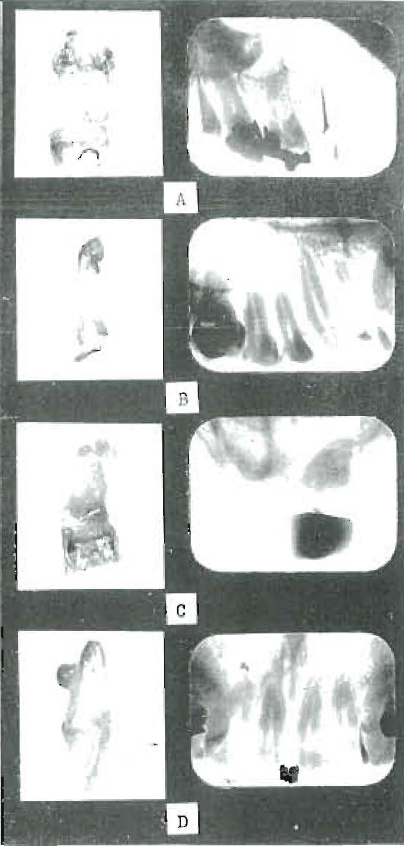
Fig. 5. Comparison of roentgenographic appearances with the actual as revealed by photographs of extracted teeth with granulomas. The absence of roentgenographic evidence of periapical involvement may be noted.
Differences in Type of Local Reaction as a Basis for Classification of Individuals
Another of our accepted fundamentals presupposes that an infection, if present in a tooth, will produce a destruction of bone about its root apex, which of necessity must appear as a zone of radiolucence. This assumes that individuals will behave similarly in the presence of an infection or rather as a result of the presence of an infected tooth structure within their tissues. I previously have presented extended detailed evidence indicating that individuals do not react similarly, as regards the supporting structures, to a given dental infection. Our further detailed studies add much evidence that, in general, individuals do not present similar reactions, but that they can be divided into three main groups on the basis of the type of reaction or tissue change produced in the supporting structures by a given dental infection. I probably should repeat frequently the words “given dental infection,” for I am continually misunderstood because people apparently do not understand what I mean by a given dental infection. If a single-rooted tooth has a putrescent pulp, it presumably has more infection with both the capacity of the pulp chamber and dentin available than it would with the dentinal tubuli alone. Similarly, a molar has more capacity for holding infection than a lateral, assuming each to have a putrescent pulp. In the presence of a given dental infection, some individuals will produce a very large zone, some a large zone of radiolucence surrounded by a zone of radiopacity, and others very slight evidence of rarefaction at the apex, with or without considerable evidence of increased density; and a given dental infection may produce changes within this wide range in different individuals.
In Figure 6, we have six teeth, two of which represent one of three types. In 6-A we have a central incisor with an extensive zone of absorption of the alveolar bone about it. There is all the infection of a putrescent pulp. You will note particularly the absence of a zone of condensation about this zone of rarefaction. You will also note that there is distinct evidence of absorption of the root substance itself. In 6-B we have a similar condition about the molar. In this type, on surgically opening the bone tissue, it is found that there is a marked tendency for the organized tissue that occupies this space to be in direct contact with the medulla of the bone. The trabeculæ tend to be relatively small and the intratrabecular spaces relatively large. Figures 6-A and 6-B are typical of Group I. In 6-C we have a molar that shows a marked zone of radiopacity about a large zone of radiolucence. The zone of dense bone tends to shut off quite completely the direct communication between the organized granulomatous tissue and the medulla. In 6-D we see a similar condition, though more marked. Figures 6-C and 6-D are typical of Group II.
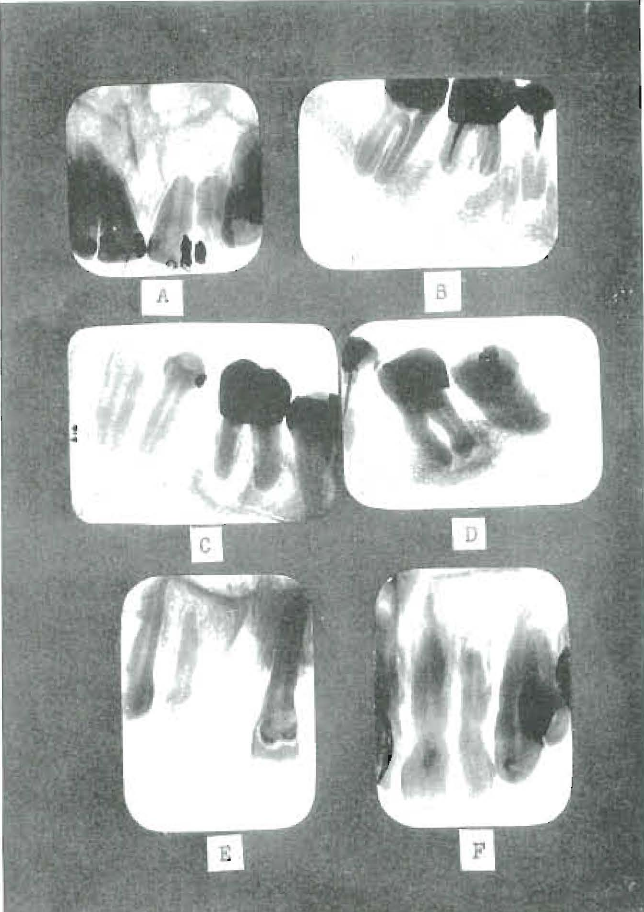
Fig. 6. Six cases representing three distinct types: A and B, extensive apical decalcifications with root end absorptions, in individuals with a high defense and susceptibility group absent; C and D, individuals with condensations surrounding zones of rarefaction, acquired susceptibility group; E and F, teeth with slight apical absorption with tendency to condensation, in sick patients, inherited susceptibility group.
In 6-E and 6-F we have the quantity of infection of putrescent pulps and laterals, and in each case relatively a much smaller zone of radiolucence; particularly in 6-E, it will be noticed that the intratrabecular spaces are smaller than in 6-A. Figures 6-E and 6-F are typical of the third group so far as they show the small zones, though in many cases we find more condensation than is shown here. These are both in young persons, however. It is strange that phenomena that are so far-reaching in importance have received so little attention when such a vast throng has been in close contact with this problem. This is probably largely due to the fact that we do not see the bone tissue free from its included organized or disorganized softer structures.
Degree of Susceptibility to Rheumatic Group Diseases as a Basis for Grouping Individuals
The diagnosis, prognosis, and treatment of dental infections, as almost universally conceived and practised, have, as the fundamental tenet, that various individuals are comparable to one another because they will, in the presence of similar infections, react with uniformity and similarity. Internists and surgeons have long observed that many individuals are found who, notwithstanding extensive dental infections, are in excellent health and give a history of always having been so. Several years ago, I began recording evidences of a familial aspect both for the type of systemic involvements that tended to develop and for the type of dental pathologic process that tended to exist in such individuals, classifying in detail the family characteristics in cases in which individuals suffered from acute and chronic infections associated with dental lesions. These data are now very extensive, including a study of more than 1,500 families. The individual in question, his or her brothers and sisters, the father and mother, the brothers and sisters of each, and the four grandparents have all been considered. These studies have shown, as I have reported in detail, that individuals may be divided into three main groups on the basis of the presence or absence of a susceptibility to the rheumatic group diseases. These groups are, first, those with an absence of susceptibility, which has characterized the past and present of the individual and in general the members of the family; second, those with an acquired susceptibility (these, in the main, having been free from rheumatic group disturbances but having recently developed them under physical overload), and, third, those who have frequently been affected, as have the members of their families. This is readily demonstrated by such analysis of the extensive data as the following:
Ten individuals were selected (and on the foregoing basis there is an average of approximately sixteen members for each of their families) having each of the following affections: rheumatism or arthritis, heart involvement, break in the nervous system, lesions of internal organs. This study is made to compare the number of lesions in the various members of these families with those of the members of each of the other groups. This study shows that in the group of ten families, or approximately one hundred sixty individuals, when the patient’s chief lesion was rheumatism or arthritis, there were fifty-nine suffering from this affection; whereas, in the other three groups, the number affected with this type of lesion was twenty-four, fifteen, and thirteen, respectively. In the group with heart involvement, the figures are fifty-seven as compared with seven, nine, and nine; in the nervous affections, one hundred forty-two as compared with nineteen, twenty-five, and thirty, and in lesions of an internal organ, ninety as compared with nineteen, thirteen, and twenty-eight. As important as this observation is, it has a vastly enlarged interest and use in the light of the next important discovery, namely, that individuals, when grouped on the basis of the type of dental pathologic condition, and the presence or absence of susceptibility, tend to have the same unit groups, for it proves to be the case that those individuals who have the large zones of rarefaction, as illustrated in Figures 6-A and 6-B, are the individuals in the group with the absence of rheumatic group susceptibility. By rheumatic group, we mean lesions of joints, muscles, hearts, kidneys, nervous system, etc., which tend largely to develop in susceptible tissues or to be aggravated by streptococcal focal infections. The accumulating data make the mass of evidence so overwhelming that there seems no other possible way to account for the close association between the type of dental pathologic condition and the type of systemic reaction.
Relation of Periodontoclasia to Systemic Disturbance
When we take fifteen families as being typical of each of these different groups, and then divide the last group (namely, those with an inherited susceptibility) into four groupings (one side mild, two sides mild, one side strong, two sides strong) and use fifteen families for each, we are able to make important observations which suggest elements that are involved factors, if not the fundamental causes, of some of these phenomena. This is illustrated in Table I, in which the column headed “Susceptibility” shows the different classifications as suggested, and the section headed “Number of Lesions per Group” shows the incidence of the rheumatic group disturbances. It will be noted that the total number of severe rheumatic group lesions (by severe, I mean those that have either incapacitated or caused death) is progressively greater as the inheritance of the susceptibility increases in intensity. There is not opportunity in this text to review in detail those data which have previously been reported.
Table I. Relation of periodontoclasia to susceptibility to rheumatic group lesions (fifteen typical families in each group).
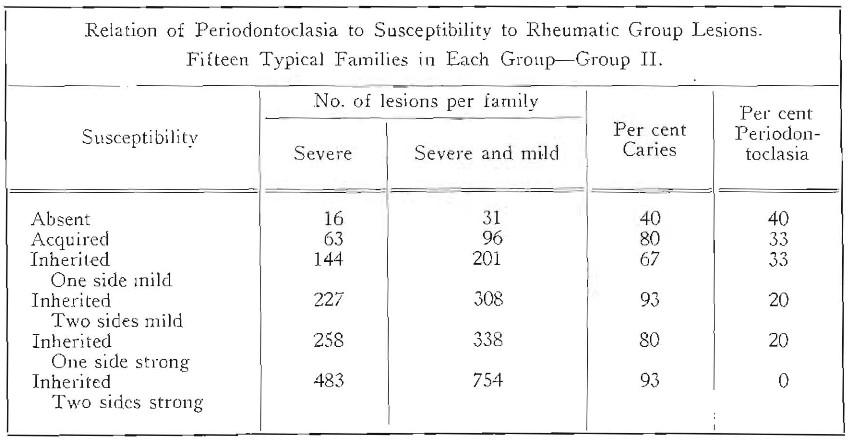
In the column headed “Severe and Mild” we have included the mild lesions with those that are severe (by mild, I mean those that have produced severe inconvenience and discomfort, but not caused incapacity or death), and here again it will be noted that there is presented the number of these lesions in the different families. These data suggest that the members of the families in the last group (namely, those with two sides strong) are subject to a probability for the development of these lesions from twenty to thirty times as great as those in the families of the groups classed as absent susceptibility. This furnishes a very important factor in each diagnosis, prognosis, and treatment, for the factor of safety of the last of these groups is very much less than that of the preceding groups.
These data immediately suggest the answer to the paradox that has produced probably more of the differences of opinion than any, if not all, other factors combined; namely, why it is, in our general clinics, that those patients who apparently have the most dental infection in their mouths, as judged by flowing pus from fistulas and number of broken-down and abscessing roots or suppurating pyorrhea pockets, generally present themselves without a history of the rheumatic group disturbances. as they appear in general or accident clinics? Conversely, why it is that the patients who do show severe or frequent breaks with the rheumatic group disturbances are so often those who have very little evidence of oral suppurative, infective processes? Whereas, in the former group there is a history of recurring tenderness of the teeth to make certain that the teeth are infected, in the latter group there is usually little or no history of such inflammatory reactions or painful disturbances.
If time permitted, we would desire to present many striking illustrations of elective localization. Typical of such would be shown in Figure 7, in which will be seen the rotation of the rabbit’s head from the culture taken from the tooth of a patient suffering from torticollis, and which was entirely relieved in the patient by the removal of the dental infection. When this animal was placed under an anesthetic, its head took a natural position only to return again when the animal came from the anesthetic. Another and perhaps more striking illustration is that of a patient suffering from acute torticollis which for a week had prevented her from lying down. It had been slowly developing with increasing severity during a period of two years, following the placing of a questionable type of dental restoration. (The denture was allowed to cover embedded roots.) The roots were removed, upon which followed, within twenty-four hours, a very marked improvement in the neck involvement. At that time a piece of the muscle of the neck was removed, under aseptic conditions, a part of it being cultured and another part sectioned. Figure 8 shows the streptococci within the sheath of a muscle fiber. Cultures were grown from the extracted roots and from the excised muscle tissue. Each culture was inoculated into a group of rabbits. Figure 9 shows several of these rabbits. One group was inoculated with the culture from the tooth, and another group was inoculated with the culture from the muscle. Both groups of rabbits had marked choreic movements, and displacement of the head as shown in the photographs. I have motion pictures of these two groups of rabbits, showing very similar nervous and muscular system disturbances. In over two thousand rabbits which I have used in making these studies, similar lesions have not developed, except with a few cultures, and when they have developed they have been characteristic of a large percentage of the group inoculated. This patient had no return of her torticollis for two years, when it developed suddenly on the opposite side of her neck with the rotation of her head in the opposite direction. A tooth was found with an exposed pulp beneath a bridge. Within five hours after the removal of the tooth the neck symptoms had practically disappeared and did not recur.
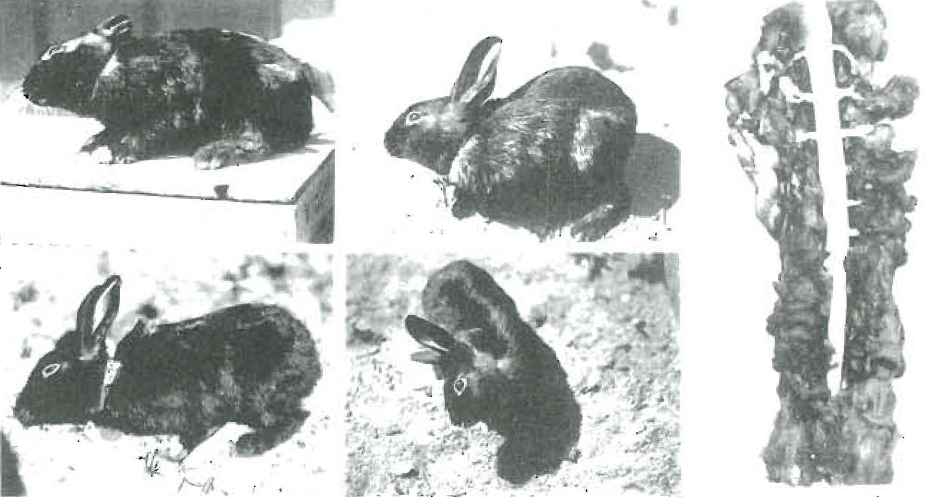
Fig. 7. This torticollis was produced with the culture from the tooth of a patient who had suffered severely for two years with recurring attacks of torticollis, which attacks did not recur after the removal of the infected tooth.
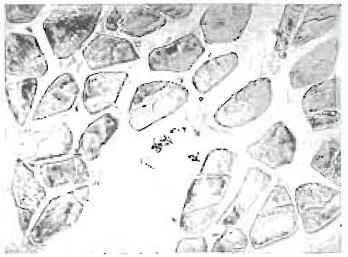
Fig. 8. Streptococci within the sheath of a muscle fiber. The tissue was removed from the neck of a patient suffering from torticollis which completely disappeared after the removal of dental infections. Part of the tissue was also cultured. (See Fig. 9.)
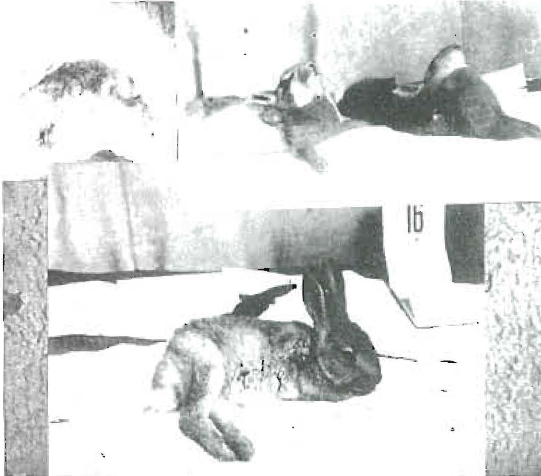
Fig. 9. These rabbits were inoculated with cultures from patients with torticollis, one of the two at the upper right with the culture from the extracted roots and the other with the culture from the neck muscle. Several rabbits from each group had involvement and choreic movement. The lower animal is paralyzed in his hinder extremities from the culture from the roots.
Another and very frequently seen illustration of localization is to be found in eye involvements. Figure 10 shows the eyes of rabbits, with the upper one normal, while the seven lower ones show various stages of corneal ulcer terminating in complete blindness. Cultures were taken from teeth of the patient suffering from acute retinitis with approximately 1/5 vision as reported by the oculist who sent him. Five rabbits were inoculated with this culture, and four developed lesions in one or both eyes.
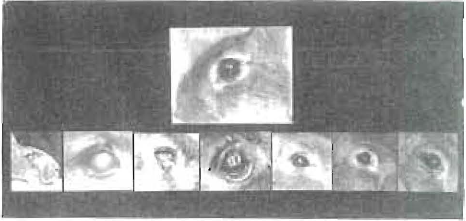
Fig. 10. Eye involvements in rabbit inoculated with culture from tooth of patient with acute retinitis. The upper eye is normal. Of five rabbits inoculated with this strain, four had acute eye involvement.
A striking illustration of involvement of the nervous system will be seen in Figure 11, the roentgenogram of the teeth of a patient, a young woman, who is suffering from recurring attacks of an obscure nervous type. Four rabbits were inoculated with the culture from these teeth. Three of the four were paralyzed from the center of their spines backward.
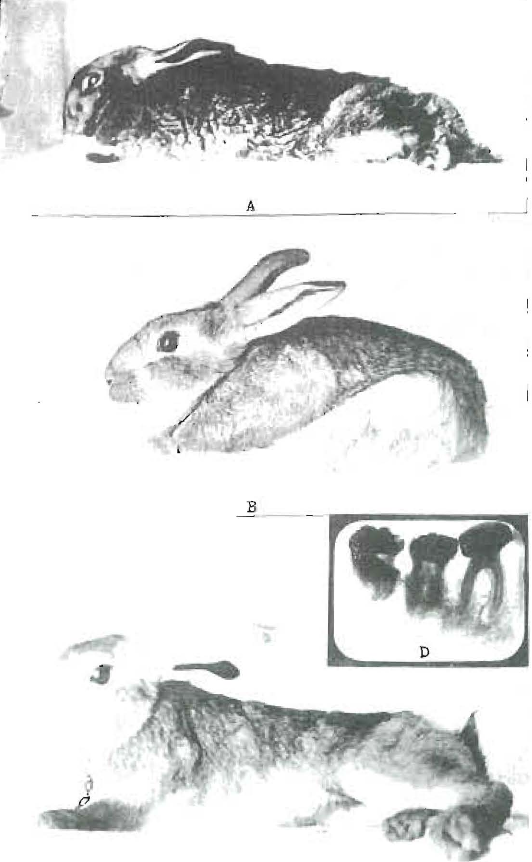
Fig. 11. These three rabbits are paralyzed from the center of their spines backward. Four were inoculated with the culture from the roots of the tooth shown, taken from a patient with severe but obscure nervous disturbance.
Another important localization expression that has developed in our work has not, so far as I know, been reported by others, namely, the very marked tendency of certain strains taken from infected teeth to select ovaries and tubes. In Figure 12, for example, will be seen an ovarian cyst as large as a hen’s small egg, which took about three months to develop. Six small ovarian cysts have developed in a single rabbit after inoculation with the culture from the tooth of a woman who had been operated on six weeks previously for removal of an ovarian cyst the size of a large goose-egg. These are also shown in Figure 12. In two thousand rabbits, divided approximately equally as to sex, such lesions have not developed in 2 per cent of female rabbits. In several cases, where the patient from whose teeth the culture was taken was suffering from ovarian involvement, a number of female rabbits have developed lesions. Direct smears and cultures made from the cyst shown in Figure 12 showed Gram-positive diplococci which corresponded morphologically with those inoculated into the animal from the dental infection. I have previously reported a number of such cases.

Fig. 12. Ovarian cysts produced by dental cultures. The one to the right was as large as a small hen’s egg. The rabbit at the left had six ovarian cysts. It had been inoculated with the culture from the tooth of a woman from whom had been removed six weeks previously an ovarian cyst as large as a goose egg.
Our usual method of inoculation has been to use about 1 c.c. of an eighteen to twenty four-hour culture of a strain grown in deep ascites tubes containing dextrose brain broth, usually with vaseline covering same. We have found that the elective localization qualities were very rapidly lost, particularly under aërobic conditions, and that it is more important to have a young culture of organisms, even though scant in growth, than to have an older culture even though the latter is rich in growth. We have, for example, been able to produce acute endocarditis, which caused the death of the rabbit in two weeks, with the organisms washed from two infected teeth of a young man suffering from acute endocarditis. The calculated weight of the organisms injected as determined by a count for establishing the concentration was in the neighborhood of one millionth part of a gram.
I have done much work by placing infected teeth beneath the skin of animals through the smallest button-hole incision that would permit of their entrance, care being taken not to contaminate the wound, which was carefully closed with sutures and sealed. Approximately 75 per cent of such teeth caused the death of the animal in a few days or weeks and about 25 per cent became encapsulated, in which cases the rabbits lived for months and frequently developed nephritis and streptococcal pneumonia, sometimes after a year. One tooth was transferred from rabbit to rabbit to see if the virulence of the organism could be broken by this procedure. Thirty rabbits were killed in succession, all but one in six days or less. This tooth had been removed from the mouth of a patient suffering from encephalitis. The chief symptom was recurring spasms of the muscles of mastication, chest, and arms. These repeated about every fifteen minutes and lasted for about five minutes. In the spasms, she would gnash her teeth so that it would be heard in the surrounding rooms. A culture was made from the above tooth, and inoculated subdurally into a rabbit. At the same time a culture from a tooth of a patient not suffering from encephalitis was inoculated in a similar manner into another rabbit. In a few hours’ time, the rabbit inoculated from the patient with encephalitis was having recurring spasms, with gnashing of its teeth and spasms of the muscles of the forelegs and the muscles of mastication very similar to the expression in the patient. These two rabbits are shown, one in spasm, in Figure 13.

Fig. 13. Intradural injection of culture from tooth of a patient with encephalitis. The rabbit to the right has spasms of the muscles of mastication and the forelegs, very similar to those suffered by the patient. The rabbit to the left was similarly injected with culture from tooth of a patient not suffering from encephalitis. It did not develop similar symptoms.
In the light of the later work of Dr. Rosenow relating strains of diplococci to affections simulating encephalitis, and in view of the results of our other inoculations with strains from patients not suffering from encephalitis, we feel impelled to give consideration to the association of these symptoms as produced in the rabbit with the infection from which the patient was suffering, quite regardless of whether the organism involved is a filter-passer or one of the streptococcus group.
For those who are interested in this phase of the problem I would refer to my recent review,1 which is made up almost completely of successive series of cases in which lesions were developed in animals corresponding to lesions from which the patients were suffering, and with a history of marked improvement in a large number of the patients upon removal of dental infections.
Spirochetal Infection of the Lungs
Several writers have recently stressed the importance of spirochetal infections from the mouth as primary or secondary invaders in lung lesions. Kline and Berger2 have reported sixteen cases that have come to autopsy in which the spirochetes were found in profuse numbers in the lung lesions. I have reported a case with the following history: A man about thirty-three years of age had a lung lesion which had been diagnosed as tuberculous. He was running a daily temperature, raising a very foul sputum, also had lassitude and was working only part time as a street car conductor. About his teeth were great quantities of spirochetal infection, due to an organism which is characteristic of periodontoclasial lesions. With the reduction of the gingival infection, partly by extraction and partly by treatment, the patient gained several pounds in a few weeks’ time, the afternoon temperature entirely disappeared, and for a year and nine months he has had no return of his tuberculous symptoms. Figure 14 shows the lung pictures before and six months after the removal of his dental infections. The diagnosis made by the lung specialist was, for the first study, “probable tuberculosis,” and at the time of the second, “no evidence of tuberculosis.” He now expresses doubt whether there ever had been a tuberculous infection. Since the patient who makes the poor fight against tuberculosis is of the decalcifying type, and since the decalcifying type of patient has a marked tendency to periodontoclasia, or pyorrhea alveolaris, and since pyorrheal infections are practically always spirochetal, there is always a marked danger of spirochetal involvement from pyorrhea pockets as a complication with tuberculous infection. The spirochete would usually be difficult to recognize except as the result of special search.
Fig. 14. Improvement in lung condition by removal of severe pyorrhetic teeth from a patient with tuberculous symptoms but without tubercle bacilli in the sputum.
Hemophilia
Another very important complication of gingival infection which should be emphasized will be found in those types of organisms which produce primary and secondary anemia. Some strains of streptococci show marked tendency to hemolyze red blood cells. We see these cases frequently presenting with disturbances of clotting, and death is not infrequent from slow spontaneous hemorrhage from the gums. Such a severe case is the following: A young man, about thirty years of age, suffered from hemorrhage from his gums for a period of three months, practically continuously night and day. On two occasions, he became unconscious from loss of blood and was given transfusions. A hemorrhage into the internal ear had produced complete deafness in that ear. His clotting time was about ten minutes. Close examinations showed that the hemorrhage was greatest about his pulpless teeth. Cultures from one of these teeth inoculated into rabbits produced multiple spontaneous hemorrhage throughout the body. Figure 15 shows the hemorrhages in the thigh and kidney of a rabbit which died in twenty hours after inoculation with this strain. The rabbit practically bled to death from hemorrhage into its tissues. With the removal of this patient’s infections, and the use of a vaccine made from these strains, his clotting time was rapidly reduced to three minutes and in five weeks’ time he was back on the road as a commercial traveller. I have reported similar strains that have killed animals in eight hours by multiple spontaneous hemorrhages.

Fig. 15. Multiple spontaneous hemorrhages in rabbit causing death in twenty hours, from culture from tooth of patient prostrated from spontaneous hemorrhage from the gums.
Since dental infections are so important a factor in health, and even in extent of life for so many individuals, we are immediately concerned with the responsibility of their prevention. This is a problem which primarily concerns humanity in general, and in the healing professions concerns the dentist in particular. Dental abscesses are the result chiefly of dental caries. Teeth with normal vital pulps give very little trouble or concern. When abnormal, however, even though vital, they may be an important source of infection invading the body. If a bone of the body is poorly organized during its formation, its high vascularity makes reconstruction not only possible but usually effective. This condition does not, however, obtain with regard to the teeth. Poorly organized or deformed tooth structure remains deformed during the period of its existence.
It is estimated that 90 per cent of adult individuals have dental infection, and of this number the majority have infected pulpless teeth. Since overloads, which are so important as contributing factors, cannot be entirely controlled, and since 25 per cent of all deaths are estimated to be due to degenerative diseases (over 10 per cent from the heart alone), a great responsibility falls on each individual to have focal infections removed before sufficient overload, whether of age or otherwise, lowers the defense sufficiently so that the organisms in the focal infection may bring about a serious break.
A surgeon has reported to me that he has within a period of two or three months removed seven eyes because of dental infection. In consideration of this, how important to those individuals it would have been if the dental infections had been found and removed before the involvement had occurred. Periodic examinations are extremely important for the safety of each individual. A boat may sail the seas with defective planking so long as the weather is calm, but the buffet of the storm breaks the weakened boards. It is not possible then for the boat to be taken into dry dock for the repairs which, if placed in time, would have prevented the tragedy. Individuals must act before, and not during, the storm, with regard to dental infections.
Programs for the prevention of dental caries are now capable of preserving in their normal state the majority of the teeth that formerly have decayed during childhood, periods of illness, pregnancy, etc. A detailed statement of these preventive measures involves calcium metabolism, a discussion of which would involve as much space as is available for this paper-already overlong. I have considered the question of prevention at length in other papers.3,4,5
Our entire viewpoint regarding dental infections has changed. Whereas formerly we looked upon dental caries and gingival infections as invasions by specific organisms, we now consider them to be expressions of the characteristics of the soil. We are now primarily concerned with the specificity of the host, rather than with the specificity of the organism.
References Cited:
- Price, W. A.: I. Dental Infections, Oral and Systemic; II. Dental Infections and the Degenerative Diseases. Cleveland, Penton Publishing Company, 1924.
- Kline, B. S., and Berger, S. S.: Jour. Am. Med. Assn., Nov. 7, 1925, LXXXV, 1452.
- Price, Weston A.: Industrial and Engineering Chemistry, July, 1926.
- Price, Weston A.: Jour. Am. Dent. Assn., December, 1926.
- Price, Weston A.: Am. Jour. Dis. Child. January, 1927.