
Access to all articles, new health classes, discounts in our store, and more!
Certain Factors Militating Against Accurate Correlation of Physical and Roentgen Ray Examinations of the Chest
Abstract of Discussion before Los Angeles Clinical and Pathologic Society, September 22, 1927. Published in the American Journal of the Medical Sciences, May 1928, Vol. CLXXV, No. 5, p. 676.
* * *
In the practice of clinical medicine today, when laboratory and mechanical methods are employed so generally in the investigation of the sick, it is necessary to evaluate and determine the limitations of each established method of examination if we would approach anything like accuracy. In this paper, I shall discuss some of the sources of discrepancy between physical and Roentgen ray examination of the chest in an effort to show why the results of these two methods are not always comparable.
The most accurate diagnosis and prognosis in a given case of illness can be made only by studying the manner in which the patient is able to carry on his body functions in spite of the disease; or, in other words, by carefully studying the symptoms present and combining this study with a competent physical examination of the patient himself. The results of laboratory and mechanical investigation are rarely to be interpreted as making the diagnosis but rather as strengthening or weakening the opinion gained by the careful examination of the patient.
I realize that this statement may be opposed by many who have learned to accept data obtained by the test tube and by mechanical devices as being more accurate than those obtained by clinical examination; nevertheless, it will appeal to that group of clinical observers who, while utilizing all methods, have especially trained the eye to see, the ear to hear, the fingers to reveal what they touch, and above all the mind to analyze and evaluate what is seen, heard and felt.
For years, physicians who have been devoting their attention to the study of the clinical phases of tuberculosis have noted that in many instances the results of Roentgen ray examination of the same chest fail to reveal the same extent or the same intensity of the disease process. Sometimes the physical examination seems to reveal lesions that the Roentgen ray does not and often the Roentgen ray reveals something missed on physical examination. The tendency has been for the clinician to accept the Roentgen ray plate as being a true picture faithfully representing the lesions within the lung, and because of these differences to lose confidence in his ability to detect the amount of pathologic change in the lung by physical examination. This opinion of the relative value of the Roentgen ray and physical examinations of the chest has been so definitely established in the minds of a large group of clinicians that they send their patients to the Roentgen ray room before they make a physical examination; and endeavor to make their physical findings conform to shadows found on the plate. Not only is such a method to be greatly deplored because of its influence in underrating the value of physical examination, but even more so because it sets up in many instances an erroneous standard with which to compare physical examinations.
We have made it a fixed rule never to look at a plate until we have completed our physical examination, and in most instances until we have stated our opinion. In comparing the data from the two methods of examination, the evidence of the presence or absence of a probable tuberculosis will coincide in the great majority of instances, but the extent of signs on physical examination and the extent of shadows on the plate will quite often be at variance, and occasionally pathology will be suspected by one method, which is not revealed by the other.
In seeking an explanation for this variance, we were confronted by: (1) Certain well recognized sources of error in physical examination, and, (2) by certain errors inherent in the Roentgen ray. The results of physical examination, as well as the results of Roentgen ray examination, will differ according to the ability and experience of the examiner and operator. On physical examination, there are no signs or sounds that can be interpreted as always indicating a definite pathologic lesion, so the interpretation will depend on the examiner. The condition of the chest, aside from the pathologic changes due to the tuberculosis, must be taken into consideration. Especially must the remains of previous diseases, the compensatory changes that have taken place, and the condition of the pleura be considered. In this connection, the differentiation of pulmonary and extrapulmonary râles is attended with particular difficulty. Likewise, the character of the plate, the judgment used in proper penetration, the placing of the patient, the time of exposure and the experience in reading shadows are all generally recognized as influencing the plate reading.
But aside from this there are two very definite sources of error, which are not so well known, that I wish to discuss in this paper. One is due to the fact that, while different tissues intercept rays differently, yet pathologic tissue does not always intercept the rays more or to a sufficiently great degree to make pathologic processes stand out in shadow when compared with nonpathologic tissue. This was shown by Assmann1 who made a careful comparative study of Roentgen ray and postmortem findings. He took plates before and after death and then sectioned the lung carefully, investigating every portion of the pulmonary tissue and comparing it with the plates. As the result of this critical study, he says: “At times the Roentgen ray shows details of unexpected minuteness; for example, nodules scarcely as large as pin heads are at times shown, exact in position, size and relationship. Again, nodules as large as walnuts fail to appear on the plate and areas of thickened tissue even larger than this, cast no shadows or shadows which are scarcely recognizable. Aside from the thickness and specific chemical composition of the focus, the detail of the shadow which it produces depends upon its depth in the tissues.”
In the examination of tuberculous patients, we have long been convinced that it is impossible to correlate physical and Roentgen ray findings too closely. When we were using exclusively in our Roentgen ray examinations stereoscopic plates taken dorsoventrally with a distance of 40 inches between the tube and the screen, we particularly noticed that the greatest discrepancy was found in comparing physical findings over the posterior wall of the chest with the plates. We then began taking plates ventrodorsally as well as dorsoventrally and found that the shadows on the plates of chests showing more disease posteriorly on physical examination also showed a greater density or more widely spread density when taken ventrodorsally than plates taken dorsoventrally and vice versa.
We should have suspected this from the fact that the scapulae are well visualized in plates taken ventrodorsally, while they cast little or no shadow in plates taken dorsoventrally. This is of particular import because the scapula is made up of calcium, which intercepts the rays to a much greater extent than the softer tissues which make up the pathology of tuberculosis.
We then began to study our cases roentgenologically with plates taken both ways and found that when the greatest amount of disease was on the side of the lung nearest the plate it showed best; and that oftentimes when on the side away from the plate, the extent of the lesion was greatly minimized and at times even failed to be recorded. In comparing plates taken dorsoventrally with those taken ventrodorsally on the same day, with the same distance from tube, there was some difference in nearly all; in many, not sufficient to make any great difference in our opinion of the disease. In quite a few, however, there was a marked difference, and in some it was so great that when the two plates were placed side by side they would not be recognized as being those of the same chest. While stereoscopic plates, as compared with single plates, will eliminate some of this error they cannot eliminate it all, as will appear from our discussion of the factor in technique which is responsible for it. Our plates are all taken with the distance of 40 inches between the patient and the tube, the patient leaning firmly against the screen. We use the same distance and same method whether taken ventrodorsally or dorsoventrally.
I find that the basis for the above observation was established experimentally by Ziegler and Krause,2 in 1910. They studied the effect on plates made by placing strips of lung containing tuberculosis lesions on the chest wall before Roentgen raying the chest. They found that when the strips were lying on the chest wall nearest the plate, they caused sufficient absorption of the rays to cast a shadow, but when on the side nearest the tube they influenced the plate little or not at all. As a result of these experiments they suggested that both dorsoventral and ventrodorsal plates should be taken in all cases where small lesions were suspected. Gräff and Küpferle have also discussed this phase of the subject in two valuable communications.3,4
Probably the best suggestion that has been made for overcoming this difficulty is that of Groedel,5 who considers that the chief difficulty in securing proper definition of lesions situated in that portion of the lung nearest the tube is due to the secondary rays which come from these lesions, the effect of which can be overcome by taking films with the tube two meters from the patients, and instead of the patient standing directly against the screen, by placing the screen at a distance of 20 cm. from the surface of the body.
Since so much dependence is being placed on the Roentgen ray in diagnosis, and since errors in diagnosis of early tuberculosis may prove to be so costly to the patient, it is necessary that the nature and cause of inaccuracies be understood so that methods for overcoming them may be devised; and, if this proves to be impracticable, so that the fact of the existence of error at least be generally known.
Roentgen Ray Shadows Depend on the Chemical Composition of Tissues
In order to determine the true place of the Roentgen ray in the examination for chest diseases, it is necessary to understand what the Roentgen ray plate is and what it is capable of showing. A Roentgen ray plate of the chest is a composite picture in which many different structures take part. The variations in the plate are due to the way in which different structures interfere with the passage of the Roentgen rays and the manner in which the shadows from such structures are superimposed upon each other. The obstruction of the rays follows definite laws, the understanding of which is necessary to the appreciation and the interpretation of the plate. The rays are obstructed to a different degree by different tissues and different pathologic processes, because different elements enter into the composition of the various tissues and pathologic processes.
The power of the physical elements to obstruct rays varies approximately with the fourth power of their atomic number.6 The elements which make up the structure visualized by the chest plate are those found in the normal and pathologic intrathoracic tissues, the air in the lungs, and the bones and soft structures composing the thoracic cage. The soft structures are made up largely of the elements, carbon, oxygen, hydrogen and nitrogen; the bones of calcium; while sodium, potassium, magnesium, phosphorus and iron are present in the cells and fluids in small quantities. Each one of these elements has its own particular power of intercepting the rays as they pass through, and the degree to which tissues will be visualized will depend on the relative quantities of elements of higher and lower atomic numbers which compose them.
The thicker any structure which absorbs rays the denser is its shadow. The shadow of edematous tissue should be more pronounced when many cells take part in the infiltration, and these cells, on the other hand, affect the shadows on the plate much less than fibrous tissue and calcareous deposits. But no matter what the shadow-casting power of a given tissue, the intensity of the shadow on the plate will vary with the thickness of the tissues responsible for it. The relative capacity of the common elements found in the tissues of the chest for intercepting rays, according to the rule given above, taking hydrogen as 1, is as follows:
Relative Capacity of Different Elements for Intercepting Roentgen Rays
| Element | H | C | N | O | Na | Mg | P | K | Ca | Fe |
| Atomic No | 1 | 6 | 7 | 8 | 11 | 12 | 15 | 19 | 20 | 26 |
| Capacity to intercept rays | 1 | 1296 | 2401 | 4096 | 14641 | 20736 | 50625 | 130321 | 160000 | 445976 |
From this table, it can be seen that the tissues which make up the soft structures offer comparatively little hindrance to the passage of the rays, while the alkalies and alkali earths, phosphorus and iron offer relatively greater obstruction. Ca, which is found in large quantities in bones and calcified nodes, casts very dense shadows.
The shadows on a plate will depend upon the aggregate of intercepted rays caused by the particular tissues superimposed on each other. To the extent that the relative quantity of the different elements in the tissues which intercept rays differ under conditions of health and disease, so the plate of the normal and pathologic lung will differ.
It is often taken for granted that pathologic structures are revealed in all instances, but nothing could be farther from the truth. Some are shown; others are not.
Assuming that the Roentgen rays are passing through the chest in such a manner that they will be intercepted in accordance with the fourth power of the atomic number of the elements entering into their composition, we can see that tissues containing large quantities of Ca, Fe, P and alkali earths would cast comparatively heavy shadows, while others made up of C, H, N and O, such as the ordinary protein material of the tissues would interfere but slightly and might hardly make an impression on the plate. This occurs in practice as has been pointed out by different observers. This inability of certain pathologic tissues to intercept rays because the elements which enter into their composition are of low atomic number, we accept as a limitation of the use of chest plates which cannot be overcome.
Error Due to Vertical Plane in which Chest Pathology is Found
Another serious source of error in chest plates arises from the depth of the chest through which the rays must pass and the fact that the pathologic foci lie in different vertical planes. The tube gives off both soft and hard rays at the same time and in order to make a plate that is sufficiently clear for interpretation the operator must give careful heed to the penetration of the rays. In order to visualize structures near the screen it is necessary to use rays which overpenetrate the tissues nearest the tube and vice versa.
In order to secure a true picture in which all parts of the lung would be equally represented, every vertical plane of the chest through which the rays pass would have to be exposed to rays of the same degree of hardness or softness. These conditions cannot be met in the application of Roentgen rays to the examination of the chest and therein lies certain very definite sources of error.
This source of error, however, can be overcome to a certain extent by taking plates both dorsoventrally and ventrodorsally. A plate taken dorsoventrally will show the structures in the anterior portion of the chest at the expense of those in the posterior. When the two are considered together the combined plates will come more nearly representing the actual lesions within the chest than that shown by plates taken in one direction alone; but even then, there must of necessity be certain areas which will not be properly visualized.
It is impossible to secure sufficient definition and detail in a cut to illustrate the small but very important differences which appear in some of the plates when taken both dorsoventrally and ventrodorsally. Particularly is this true in instances where the amount of infiltration is very limited. Therefore, I deem it much better to illustrate the point by plates taken of patients suffering from advanced tuberculosis, leaving it to each clinician to satisfy himself in his own practice in case of less extensive lesions.
The following cases with plates taken in both directions will bear out the assertions which are herein discussed.
Case 7277–(Fig. 1 and 2). The patient entered the sanatorium in March, 1926, at which time she had two small cavities in the left apex, an extensive active disease through the upper lobe and a slight involvement in the upper right. The disease become temporarily quiescent after a time, but nine months after beginning treatment, an extension of the disease took place in the neighborhood of the cavities, the tissue between them sloughed out, and the tissues below the cavity became the seat of an exudative process. Physical examination revealed more active disease posteriorly than anteriorly and more than was indicated by the plate taken dorsoventrally. A. ventrodorsal plate was then taken which gives us a truer picture of the condition, one which corresponds more nearly to the findings on physical examination. On comparing these two plates, Figs. 1 and 2, one would not recognize them as being of the same chest. The difference in both pulmonary and pleural shadows is very marked.
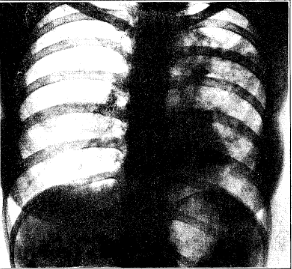
Fig. 1. Dorsoventral plate. A large irregular cavity is seen near the left apex, with moderate exudative inflammation immediately below, and widespread scar and a lesser activity toward the base. Apparently little evidence of pleural involvement. Right lung emphysematous but practically free from disease.
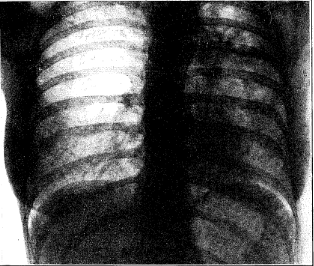
Fig. 2. Ventrodorsal plate. Cavity same as in Fig. 1. Much more extensive exudative infiltration below the cavity than shown in dorsoventral plate. Marked pleural haze over left hemithorax.
Case 7877–(Figs. 3 and 4.) The patient entered the sanatorium in July, 1922, at which time she had a double lesion with cavity in both apices. The cavity in the right side finally shrank and almost disappeared. That in the left enlarged greatly, extending from the apex to the second interspace, and the disease process in both upper lobes and a portion of the lower became very active. The patient showed poor resistance and at no time was she entirely free from symptoms for more than a few weeks at a time. In December, 1926 the disease began to show increased activity. The temperature became more elevated, toxic symptoms appeared, and cough and expectoration increased. Repeated examinations showed extensive activity in both lungs. The Roentgen ray plates taken dorsoventrally showed a gradual lessening in the lung shadows, but the patient continued to show toxic symptoms and loss of strength. Signs on auscultation at the base of the cavity anteriorly showed lessened activity but those posteriorly and in the upper half of the right lung were those of a very active process. The ventrodorsal plate revealed a much more extensive disease than was shown by the dorsoventral plate, both in the lung and in the pleura.
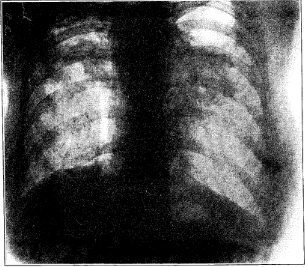
Fig. 3. Dorsoventral plate. Large cavity in upper portion of left lung. Extensive fibrocaseous infiltration below to fourth rib. Right lung shows some tissue loss at apex. Fibrocaseous lesion in upper half. Slight pleural haze over left hemithorax.
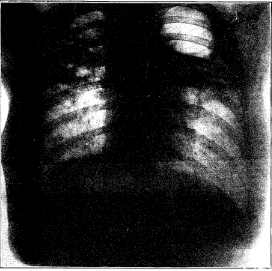
Fig. 4. Ventrodorsal plate. Large cavity occupying apex of left lung. Considerable fibrocaseous infiltration immediately below, more extensive and more active than shown in Fig. 3. Right lung also shows large fibrocaseous infiltration in the upper half of the lung, more extensive and more active than that shown in Fig. 3. Pleural haze over left hemithorax more marked than in Fig. 3.
Summary
- The findings on physical and Roentgen ray examination of the lungs show some variation in nearly all instances, and in a small percentage the differences are very marked.
- The ability of the disease process in the lung to produce shadows depends upon the power of the various elements making up the structures to intercept the rays, and this varies approximately according to the fourth power of the atomic number of their composing elements. Therefore, on the plate, small lesions may show perfectly if composed of elements whose atomic number is high, and large ones may not show at all if the atomic number of the chief component elements is low.
- Lesions nearest the plate (taken at a distance of 40 inches) show best, because the tissues nearest the tube are overpenetrated and consequently fail to intercept the rays and produce shadow. Therefore, there is considerable variation in plates taken anteroposteriorly compared with those taken posteroanteriorly. If a spinal lesion lies near the surface of the chest wall nearest the tube, it may not be detected at all by the Roentgen ray. This error is lessened, but not eliminated, if the tube is some distance from the patient.
- When small lesions are suspected on physical examination, the patient should be placed dorsoventrally if the lesion is suspected anteriorly, and ventrodorsally when suspected posteriorly, or, what is better, plates should be taken in both directions.
References Cited:
- Assmann, H.: “Erfahrungen über die Röntgenuntersuchungen der Lungen,” Arb. a. d. med. Klinik zu Leipzig, Jena, G. Fisher, 1914.
- Ziegler, O., and Krause, P.: “Roentgen-Atlas der Lungentuberkulosis II,” Supplement-band zur Beiträge zur Klinik der Tuberkulose, 1910, Wurzburg, Curt Kabitzsch.
- Gräff, S., and Küpferle, L.: “Die Bedeutung des Röntgenverfahrens für die Diagnostic der Lungenphthise auf Grund vergleichender röntgenologisch-anatomischer Untersuchungsergebnisse,” Beitr. z. klin. d. Tuberkul., 1920, vol. 44, Wurzburg, Curt Kabitzsch.
- Gräff, S., and Küpferle, L.: Die Lungenphthise Ergebnisse vergleichender röntgenologisch-anatomischer Untersuchungen, Berlin, Julius Springer, 1923.
- Groedel, F. M.: Personal communication.
- Russell, B.: A, B, C of Atoms, New York, E. P. Dutton & Co., 1923.