
Access to all articles, new health classes, discounts in our store, and more!
Cataphoretic Time and Velocity of Streptococci and Pneumococci: Studies on Organisms Isolated in Cases of the Common Cold, Influenza, Bronchopneumonia and Lobar Pneumonia
Read before the American Association of Pathologists and Bacteriologists, Washington, D. C., May 10, 1933. Published in the Journal of Infectious Diseases, Vol. 54, January 1, 1934, pp. 91–122.
* * *
After it was found that the streptococci obtained in studies of arthritis, myositis, encephalitis1 and other diseases2 showed characteristic cataphoretic time and velocity as isolated in dextrose-brain broth, it was thought that a similar study of organisms isolated from the nasopharynx or sputum of persons having different diseases primarily of the respiratory tract might also reveal streptococci or pneumococci having distinctive cataphoretic velocity. In this paper I shall report the results obtained in a study of the cataphoretic time and velocity of streptococci and pneumococci isolated in different types of acute infections of the respiratory tract, chiefly in Rochester, Minn., during three consecutive years, from March, 1930, to March, 1933.
The study includes a series of cases of the common cold associated with varying degrees of rhinitis, pharyngitis, laryngitis, trachitis or bronchitis, two institutional and three community outbreaks of influenza, a series of cases of postinfluenzal exhaustion and cases of influenzal bronchopneumonia and of lobar pneumonia. A large number of control observations on well persons and persons with chronic diseases during and soon following epidemics of influenza and on persons who were remote from epidemics are also recorded.
Methods
The material derived from human beings for culture, animal inoculation and other studies was obtained as a routine by swabbing the nasopharynx with a sterile, cotton-wrapped, wire swab bent to a suitable angle, care being taken not to touch the tongue. The swab thus obtained was placed in a test tube containing 2 cc. of a mixture of gelatin (0.2 per cent) and Locke’s solution, and the material on the swab was thoroughly washed off by striking the lower end of the tube with the fingers of the right hand while the upper end of the tube was held loosely in the left hand. In cases in which sputum was obtainable, cultural and other studies were also made on this material after it had been washed in sterile solution of sodium chloride. Cultures were made as a routine on the surface of blood-agar plates and in tall tubes of dextrose-brain broth. The swab saturated with the gelatin-Locke’s solution was used for this purpose. A considerable amount (from 1 to 2 minims) of washed sputum was used for inoculation in like manner. Similar cultural and other studies were made at the same time on the milk supply and on Streptococcus lacticus “starters,” especially in connection with institutional outbreaks of colds and influenza, in order to see if the streptococcic flora of the milk might not be similar to that of the throats of persons suffering from respiratory infections. Accordingly, cultures were made of bulk milk and whenever possible of milk obtained in a sterile manner directly from the cows. Approximately 2 cc. of the milk was placed, chiefly in the bottom layer, in tall tubes of dextrose-brain broth, and 3 drops from a capillary pipet was spread over the surface of half of a blood-agar plate.
Cultures were made of the apical ends of pulpless teeth, under sterile precautions, immediately after extraction, and of material from adherent or curetted granulomas. The apexes were placed in 2 cc. of gelatin-Locke’s solution containing quartz sand and shaken vigorously for some time, and the apex and washings were used for inoculation of dextrose-brain broth, dextrose brain-agar and blood-agar plates. The absence of growth in dextrose-brain broth, in which was placed the control swab made from the margin of the gum after sterilization with tincture of iodine and alcohol just before extraction, and the absence of growth on the blood-agar plate also was considered as proof that heavy growth in the dextrose-brain agar shake culture and in dextrose-brain broth was not due to contamination but represented multiplication of living organisms at or in the apex of the tooth.
Cultures from the throat, from sputum, from milk and from teeth were incubated at from 33 to 35 °C. for from eighteen to twenty-four hours, after which time films and blood-agar platings were made of the growth in dextrose-brain broth and the type of growth on blood-agar plates was recorded. In this as in other papers dealing with streptococci, all diplococci and all organisms in chains of varying length having the usual form and size of streptococci when grown in liquid mediums, especially dextrose-brain broth, are considered as streptococci, irrespective of whether they are soluble in bile, ferment inulin or produce green, indifferent or hemolytic colonies on blood-ager plates. From 2 to 3 cc. of the primary growth in dextrose-brain broth of organisms derived from the nasopharynx, teeth and sputum, containing a pure or nearly pure culture of streptococci, was poured into scrupulously clean test tubes. A like amount of growth was transferred from the upper layers of those tubes containing the growth from milk, stained films of which revealed only, or a great preponderance of, streptococci. During the short period of incubation the dextrose-brain broth proved an almost differential medium for streptococci. Pure, or nearly pure, cultures were almost constantly obtained in tubes inoculated with material from the nasopharynx and teeth, with sputum and with milk obtained in a sterile manner from individual cows. This was true also in the majority of cultures of bulk raw milk. The tubes containing from 2 to 3 cc. of the growth were then centrifugated at 1,400 revolutions per minute for ten minutes; the supernatant broth was thoroughly drained off, and the sediment was suspended in approximately 17 cc. of distilled water. This was poured into the Northrop-Kunitz-Mudd cataphoresis apparatus. The determinations of velocity were made at approximately 120 volts to the zinc electrodes, and at a temperature of from 22 to 24 °C. The time required for each of from ten to twenty organisms, depending on the evenness of their rate of migration, to traverse the unit distance of 50 microns was determined with a stop-watch. The rate of migration in both directions was frequently checked, and readings were made immediately, or more often within one hour after the suspension in distilled water was made, and occasionally after the preparation was kept in the refrigerator over night. The time required in seconds and quarter seconds for each organism to traverse this unit distance was recorded, and from this the cataphoretic velocity was determined in terms of microns per second, volt per centimeter, according to the formula:
For example, neurotropic streptococci travel the distance of 50 microns in 4 seconds, with the effective voltage between electrodes 3.45 cm. apart 25.8 volts. Hence, microns per second, volt per centimeter =
or 1.67. The maximal error from variations in voltage, as determined by actual readings of the effective voltage in a large number of determinations, was ± 4 per cent, and in the great majority of instances the error was negligible, or less than ± 1 per cent.
The person determining the velocity in most instances was unaware of the diagnosis in the cases from which the culture or cultures were obtained. Cultures of material from atria of infection of patients having different diseases, old cultures and standard suspensions were often included on the same day throughout the study, and more recently the effective voltage between the platinum electrodes 3.45 cm. apart was determined just before and usually immediately after the timing of the streptococci, in order to be certain that the results were reliable. The effective voltage was nearly always about 25 volts, with an occasional variation of ± 0.5 volt in the large numbers of suspensions in which the streptococci from the different diseases were timed.
Cultures containing a moderate preponderance of streptococci having cataphoretic time and velocity of about 3 seconds and 2.22 microns per second, volt per centimeter, are designated as normal because this velocity chiefly obtains in cultures from the throats of normal persons in nonepidemic times; those with time and velocity of about 2.5 seconds and 2.66 microns per second, volt per centimeter, are distinguished as rhinotropic because this is the predominating velocity of streptococci isolated from the nasopharynx in cases of acute autumnal rhinitis; those with time and velocity of about 3.5 seconds and 1.90 microns per second, volt per centimeter, are designated as pharyngotropic because this is the predominating velocity of streptococci isolated from the nasopharynx in cases of simple pharyngitis or sore throat, associated often with rhinitis, laryngitis, trachitis or bronchitis and, in certain parts of epidemics, with much cough but relatively little constitutional reaction; those with time and velocity chiefly of 4, 4.5 and 5 seconds and 1.67, 1.48 and 1.33 microns per second, volt per centimeter, are designated as bronchotropic or influenzal because these are the velocities common in streptococci isolated from cases of influenza in which the throat and bronchi are chiefly affected and in which there is a relatively marked constitutional reaction as well as other symptoms and signs characteristic of influenza; those with time and velocity of about 3 seconds and 2.22 microns per second, volt per centimeter, are designated as arthrotropic because streptococci of these velocities occur in great preponderance in cases of arthritis and the organisms manifest marked affinity for joints when injected intravenously into suitable animals; those with time and velocity of about 2 and 4 seconds and 3.33 and 1.67 microns per second, volt per centimeter, are designated as neurotropic because these velocities predominate in poliomyelitis, encephalitis and other diseases of the nervous system. The time and velocity of 2 seconds and 3.33 microns per second, volt per centimeter, were especially predominant in the early stages of acute attacks; the time and velocity of 4 seconds and 1.67 microns per second, volt per centimeter. predominated later in acute attacks, in mild cases, in chronic cases and in early subcultures.
The number of streptococci the velocity of which was determined in individual strains and cultures (usually twenty) was approximately the same in each of the different strains tested in the different groups. The percentage incidence of the different units of time and velocity, as shown in charts 1 to 14, was determined by dividing the number of streptococci that had these different velocities by the total number of streptococci timed in each group. Corrections for the variations in voltage were not made because they were too slight to change the graphs appreciably.
Shibley3 and others showed that the agglutination of pneumococci and the cataphoretic velocity-slowing action of antipneumococcus serum on these organisms were fairly parallel. In the course of previous studies, specific agglutination was sometimes obtained with the serum of patients and the respective streptococci which had produced in animals diseases similar to those of the patients from which the streptococci were obtained. The streptococci were agglutinated in high dilution in the corresponding hyperimmune horse serums, but the agglutination in serum from patients was not constant enough to be of unmistakable diagnostic value. It occurred to me that possibly the serum of the patient might lower specifically the cataphoretic velocity of the streptococcus in question in sufficiently high dilution to be of unquestioned value. Accordingly, a series of experiments was undertaken to determine the most reliable method, by varying the density of the suspensions, the electrolyte content, the duration and degree of heating the suspensions and the method of holding the characteristic velocity of stock suspensions of the different strains of streptococci. The following technic was adopted as most reliable.
Dilutions of serum were made as a routine, in series, in suspensions of the bacteria as follows: 1 to 20, 1 to 40, 1 to 80, 1 to 160, 1 to 320, 1 to 640, 1 to 1,280, 1 to 2,560, and sometimes also 1 to 5,120 and 1 to 10,240, each tube containing 1.5 cc. The diluted suspensions of the respective streptococci were made from dense stock suspensions in glycerin (2 parts) and 25 per cent sodium chloride solution (1 part), which had been kept in the refrigerator. The dense suspensions were diluted with distilled water to about a fourth the density of a dextrose-brain broth culture, or about 500,000,000 streptococci in each cubic centimeter. After the suspensions and serum were thoroughly mixed the set-up was placed in the incubator for an hour and a half, in the oven at 52 °C. for two hours and then in the refrigerator over night. The following morning the tubes were inspected for evidence of microscopic agglutination; the controls, consisting of suspensions only, and each mixture containing various amounts of serum in turn were diluted with 14 cc. of distilled water poured into the cataphoretic cell, and the rate of migration was determined in the usual manner. The upper limit of dilution of the serum that had a slowing effect on the suspension in question was used as the measure of its antibody content. Owing to the large amount of time required to determine the end-point of action of the serum, I searched for a simpler method and found that a 1 to 200 dilution of normal serum had little or no slowing action on the different strains of streptococci in suspension in sodium chloride solution after two hours’ incubation and that the serum from persons presumably suffering from infection by streptococci having peculiar velocity had a decided, although a variable, slowing effect on the respective streptococci. Instead of the end-point, the amount of slowing of the streptococci over that of the control suspensions containing like amounts of normal serum, or serum from patients with other diseases, and sodium chloride solution only was used as the measure of antibody content.
The primary culture in dextrose-brain broth (which contained a pure or nearly pure culture of streptococci as isolated from throats, milk and material from injected animals), if free from gas, and single colony cultures in this medium were used for injection into animals to determine virulence. White mice were as a routine given 1.5 cc. intraperitoneally; white rats, 5 cc. intraperitoneally; guineapigs, 0.5 cc. for each 100 Gm. of body weight, intratracheally, and rabbits, 0.1 or 0.2 cc. intracerebrally and, as in studies of elective localization, about 0.5 cc. for each 100 Gm. of body weight intravenously. In some instances a like dosage of the growth in this medium from single colonies in blood-agar plates was given. The animals were observed at least twice daily, and leukocyte counts were made before and after injection and after death in many instances; postmortem examination was made as soon after death as possible. Smears of cultures were made as a routine of the blood from the heart and of fluid from the pleural cavities of the mice and rats and of pipettings of the cerebrospinal fluid and of the brain and lungs of the rabbits.
Results of Cultures
Blood-agar platings from the suspensions of the nasopharyngeal swabbings revealed a variable usually large and predominating, number of green-producing colonies of streptococci in each of the groups of cases studied. The moist, markedly green colonies of streptococci isolated during the first wave of the highly fatal pandemic of influenza of 1918 and 19194 were not found in any of the cases of influenza in this study, as was also the case in the studies of Falk and his co-workers. They were not encountered in the cases of colds or in cultures from normal persons but were found in several cases of influenzal bronchopneumonia. Indifferent and slightly hemolytic colonies of streptococci were found in variable, usually small, numbers in cultures from the throats, but they were often numerous in platings directly from the milk. Typical colonies of hemolytic streptococci were found in primary platings in only a small number of swabbings from the throats and almost never in the milk. The incidence of their isolation was highest (30 per cent) in swabbings of the throats of persons with colds at an orphanage (chart 1), next highest in the patients with influenza (4 per cent) and lowest in the patients with common head colds and in normal persons. Colonies of staphylococci were found in varying, sometimes in large, numbers in from 30 to 60 per cent of cases in the different groups.
Bacillus influenzae was rarely encountered. During the epidemics of influenza, control platings were made on chocolate-agar to make certain that the horse blood-agar used was favorable for the growth of this organism. In practically all cases, if the chocolate-agar revealed colonies of B. influenzae the corresponding plating on horse blood-agar also revealed the typical colonies, and in about the same number. B. influenzae was isolated together with green-producing streptococci in about 5 per cent of the cases of influenza during the height of epidemic waves, but this organism was almost never encountered otherwise.
Platings of the primary cultures in dextrose-brain broth of nasopharyngeal swabbings revealed an even greater preponderance of green-producing streptococci than the direct platings. In most instances only green-producing colonies of streptococci grew, sometimes even when the inoculum contained large numbers of hemolytic streptococci as revealed by direct plating on blood-agar. In some instances the reverse was found; the change from hemolytic to green-producing streptococci occurred more often in inoculated animals than in cultures in dextrosebrain broth. This instability of streptococci was more marked in strains isolated in studies of influenza during these epidemics, just as was the case with the strains that I isolated in the pandemic of from 1918 to 1920.4b
Results of Studies of Cataphoresis
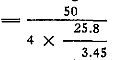
The results obtained in a study of the cataphoretic time and velocity of the streptococci isolated from the nasopharynx of the same person while well, during an attack of the common autumnal cold associated with bronchitis and persistent cough and again while well are shown graphically in chart 1. Cataphoretic time and velocity of the streptococci while the patient was well in August, 1931 (chart 1, A), and those in March and April, 1932 (chart 1, E), were similar and normal except that an unusually large number of streptococci having neurotropic time and velocity were isolated during August. The average distribution curve of cataphoretic time and velocity for five swabbings made while the subject was suffering from a cold and resultant persistent cough was very different but typically pharyngotropic, characteristic of the autumnal common cold (chart 1, B), and as recovery ensued in October the curve became more nearly normal (chart 1, C). The cataphoretic time and velocity while the patient was well in February (chart 1, D), at the height of an epidemic of influenza, were abnormal and resembled somewhat the slow velocity of the streptococcus associated with this disease (charts 2, 5, 6, 7, 8, 9 and 10). The patient had been immunized shortly before with a vaccine prepared from the streptococcus of influenza and remained free from symptoms of influenza throughout the epidemic.
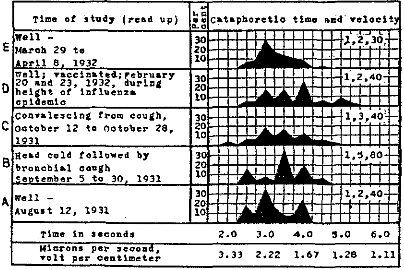
Chart 1.—Cataphoretic time and velocity of streptococci isolated from the nasopharynx of the same person while well in August, February and March and during and following an attack of the common cold and severe cough.
The changes in cataphoretic time and velocity of streptococci noted on isolation from persons at different times during attacks of respiratory infection appear to be not haphazard but determinative, for they often can be correlated with clinical manifestations.5 This was strikingly true in one case of the following study of two cases of the common cold occurring in a family. The cataphoretic time and velocity of the streptococci isolated from the nasopharynx in these two cases as the patients were recovering and from the raw milk and cream supply are summarized in chart 2. There was a marked, characteristic preponderance of streptococci having rhinopharyngotropic velocity both before and after animal passage in each of the cultures, except the one after animal passage in one of the cases (chart 2, B). The person whose streptococci retained rhinopharyngotropic time and velocity through animal passage made an uneventful recovery. Owing to the marked shift into neurotropic cataphoretic time and velocity (4 seconds; 1.67 microns per second, volt per centimeter) on animal passage in the case represented by B in chart 2, inquiry was made, and it was found that instead of the patient’s recovering in the usual manner, there developed, the day after the first swabbing, not an exacerbation of the former symptoms but severe headache, nausea and vomiting, diarrhea associated with fever and marked exhaustion. The second swabbing was made four days after the first, as the patient was recovering from this attack. Streptococci were isolated which had chiefly neurotropic time and velocity, exactly like those of strains injected into the animals, a property so firmly fixed as to be retained through animal passage (chart 3, B). This question was studied further, and it was found that an identical shift in cataphoretic time and velocity occurred in the streptococci grown in dextrose-brain broth obtained at the first swabbing, which were preserved in the refrigerator in gelatin-Locke’s solution, and in those isolated from the patient’s throat and from the inoculated animal. The neurotropic type of velocity was retained through animal passage (chart 3, C), through three rapidly repeated subcultures in dextrose-brain broth (chart 3, E), through one blood-agar plating and two rapidly repeated subcultures in dextrose-brain broth and again through animal passage (chart 3, F). This shift from predominating pharyngotropic to neurotropic velocity did not occur in the subculture of the primary culture of the first swabbing in dextrose-brain broth which had been kept at room temperature (chart 3, D). The cataphoretic velocity of the streptococci of the third swabbing, made eleven days after the first and six days after the second, before and after animal passage (chart 3, G) was again chiefly pharyngotropic, like that of the streptococci from the first swabbing, whereas the velocity of the organisms from the fourth swabbing, made fourteen days after the first, before and after animal passage (chart 3, H), approximated that of streptococci from the nasopharynges of well persons in nonepidemic times.
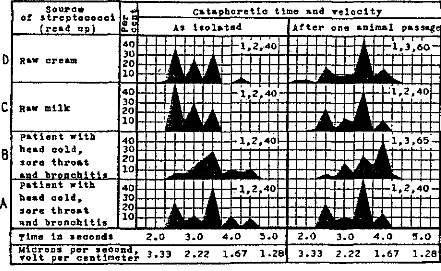
Chart 2.—Cataphoretic time and velocity of streptococci from the nasopharynges of two persons (of one family) who had sore throat, head cold and bronchitis and from the raw milk and cream supply.
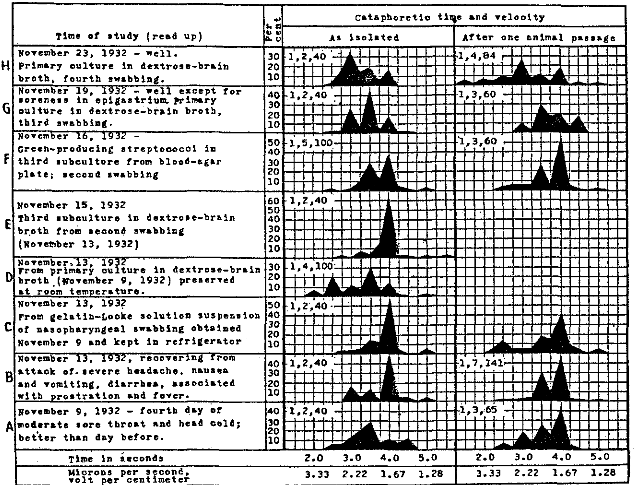
Chart 3.—Cataphoretic time and velocity of streptococci isolated in dextrose-brain broth from the nasopharynx of a patient with sore throat and a head cold and from the blood, lungs, pleural fluid and brains of animals that succumbed to injections of the streptococci.
In order to understand better the significance of the changes in the streptococci that were noted in the case under consideration, I determined the average distribution of cataphoretic time and velocity of all cultures injected into animals, of all cultures isolated from the animals that succumbed and of all cultures isolated from the brain, from the pleural fluid and lungs and from the blood. The average distribution curves of cataphoretic time and velocity of the streptococci injected and of those isolated from all sources in animals that succumbed to injection were almost identical, being chiefly pharyngotropic and neurotropic. In sharp contrast, a high incidence of streptococci having almost pure neurotropic cataphoretic time and velocity was found in the strains isolated from the brain, and a high incidence of organisms having pharyngotropic or pneumonotropic cataphoretic time and velocity was found in the strains isolated from the lungs and pleural fluid of animals that succumbed. The distribution of cataphoretic time and velocity, as determined directly in distilled water, of the streptococci from nasopharyngeal swabbings during and following the attack and from pleural exudates of the animals that succumbed corresponded closely with that of the streptococci from the respective primary cultures in dextrose-brain broth.
The results summarized in chart 4 were obtained from cultures of nasopharyngeal swabbings of patients in the hospital of an orphanage and of the milk supply during two waves of respiratory infection in the early and later parts of October, 1931, coincidental with the occurrence of one case of poliomyelitis during each outbreak.6 The symptoms, such as fever, rhinitis, sore throat and cough, and the physical findings were relatively mild and of short duration during both outbreaks studied, but were more marked, more bronchial and of longer duration during the second wave. High fever, marked prostration and bronchopneumonia did not develop in any of the cases. There was the usual number of cases in which gastro-intestinal symptoms were more pronounced than symptoms referable to the respiratory tract. Raw milk obtained from Holstein cows at the dairy owned and managed by the orphanage was used. Six cultures from a composite sample were studied during the first outbreak, on October 8, and twenty-seven cultures from twenty-five samples obtained chiefly in a sterile manner from individual cows were studied during the second outbreak three weeks later, on October 29. It will be noted that the cataphoretic velocity of the streptococci isolated during the first outbreak was considerably greater than that of streptococci from the throats of normal controls at the orphanage and markedly less than that of streptococci from the throats of normal persons remote from the epidemic, and that with the greater severity and the more bronchial type of the symptoms presented by those ill during the second wave three weeks later, the velocity of the streptococci was much less, approaching the influenzal type (chart 7). The similarity in type of the distribution curve of cataphoretic time and velocity of the streptococci, from the milk and of those from the nasopharynges of patients in both outbreaks was striking. Raw milk was used. Milking was done by hand. The refrigeration and the technic of handling the milk appeared satisfactory.
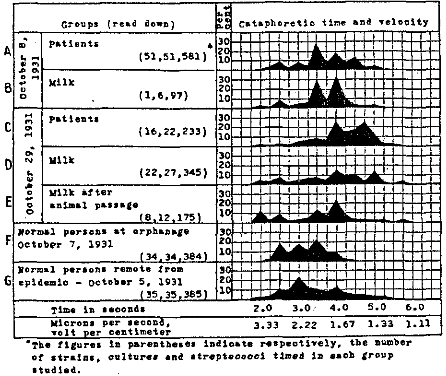
Chart 4.—Cataphoretic time and velocity of streptococci isolated from the nasopharynges of patients and from the raw milk supply at an orphanage during epidemics of sore throat.
The results obtained in a study of the cataphoretic time and velocity of the streptococci isolated repeatedly from the nasopharynges of two persons while well and during attacks (1) of the common cold, (2) of influenza-like infections of the respiratory tract and (3) of arthritis (in one patient) are summarized in charts 5 and 6. The shift in cataphoretic time and velocity from the normal values to those characteristic of the disease in question and back to normal after recovery is strikingly shown. On the second and third days (Dec. 3 and 4. 1931) of the attack of influenza in the case summarized in chart 5, the cataphoretic time and velocity were typically influenzal. With marked improvement of symptoms following administration of the influenzal streptococcic vaccine four days later (December 8) the cataphoretic time and velocity had changed materially toward the normal, but there was a preponderance of streptococci with neurotropic time and velocity. The patient felt well but was still easily exhausted. With the development of a dry, irritating cough, the cataphoretic time and velocity of the streptococci had become (December 10) markedly pharyngotropic (3.5 seconds). On April 18, 1932, during a bronchial cold without much aching, the time and velocity of the streptococci were again slow, but not as slow as during the attack of influenza. Recovery was complete following this attack and concomitantly the cataphoretic time and velocity of the streptococci from the nasopharynx became like those for well persons in nonepidemic times. This person remained well until November 7, when she contracted epidemic sore throat associated with a persistent, dry cough. The cataphoretic time and velocity of the streptococci were markedly pharyngotropic. Again, with recovery from symptoms the cataphoretic time and velocity of the streptococci isolated became normal. On December 16, symptoms of acute rhinitis, without constitutional reaction, developed, and the streptococci isolated from the nasopharynx had markedly “rhinotropic” cataphoretic time and velocity (2.5 seconds; 2.66 microns per second, volt per centimeter). Recovery from this attack was prompt. The cataphoretic time and velocity of the streptococci isolated from the nasopharynx again returned to normal, resembling the values obtained while the patient was well, on April 19, 1933.
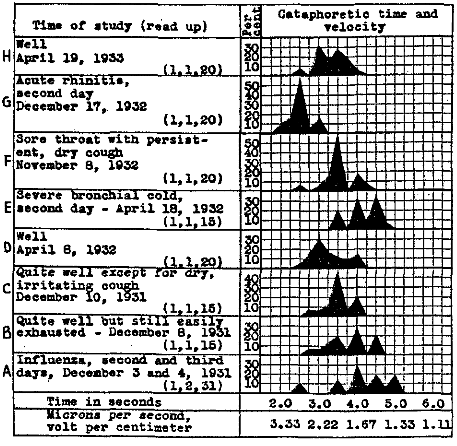
Chart 5.—Cataphoretic time and velocity of streptococci isolated from the nasopharynx of the same person during one attack each of influenza, bronchial cold, sore throat and acute rhinitis and while well.
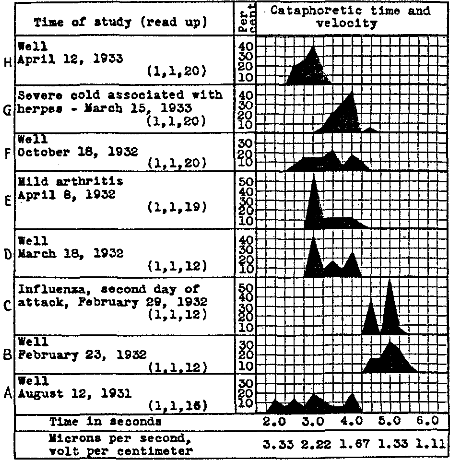
Chart 6.—Cataphoretic time and velocity of streptococci isolated from the nasopharynx of the same person while well and during one attack each of influenza, mild arthritis and a severe cold associated with herpes.
In the case summarized in chart 6 the cataphoretic time and velocity were normal while the patient was well, on Aug. 12. 1931 (chart 6, A), except that too many organisms had neutrotropic velocity, but this was found at the same time in other normal persons and was in accord with the fact that several cases of poliomyelitis in which the streptococci were markedly neurotropic had occurred in the surrounding community at the time. On Feb. 23, 1932, at the height of an epidemic of influenza, while the patient was well and not knowingly exposed to influenza, the cataphoretic time and velocity of the streptococci from the nasopharynx resembled those of streptococci in cases of influenza (chart 6, B). This person had not been vaccinated. Six days later he had an attack of influenza, and concomitantly the velocity was markedly influenzal (chart 6, C). On March 18, while the patient was well, the cataphoretic time and velocity were approximately normal (chart 6, D), but on April 8, at about the time when there was a general increase in arthritis in the community, coincidentally with a great increase in the number of streptococci derived from the nasopharynx and from milk having arthrotropic velocity (chart 8, E and F), and several days after he had had a slight sore throat, the patient underwent an attack of acute, although mild, arthritis, and concomitantly the cataphoretic time and velocity of the streptococci from his nasopharynx were markedly arthrotropic (chart 6, E). On April 18, he had recovered from the arthritis and the cataphoretic time and velocity again approached normal values for that time of the year. On Oct. 18, 1932, while the patient was well, but during an epidemic of the common cold, the cataphoretic time and velocity of the streptococci from his throat were normal. The number of streptococci having pharyngotropic time and velocity was higher than for normal persons in nonepidemic times (chart 6, F). On March 15, 1933, on the third day of a severe cold associated with marked herpes of the lip, the incidence of streptococci from his nasopharynx having pharyngotropic and especially neurotropic cataphoretic time and velocity was high (chart 6, G). The patient recovered promptly from this attack, and twenty-eight days later, on April 12, the cataphoretic time and velocity of the streptococci approached the normal (chart 6, H).
The two epidemics of influenza, the studies of which are summarized in chart 7, occurred in February, 1931 and 1932, at a college in a small city 60 miles from Rochester, Minn. The disease was of moderate severity in both epidemics. The attacks of influenza were characterized by a variable degree of headache, pain back of the eyeballs, photophobia, prostration, pain in the muscles of the back and the extremities, moderate fever and often moderately dry cough which was associated with pain in the throat and the anterior part of the thorax. The face was flushed, the conjunctivae were congested, the tongue was coated and the soft palate and pharynx were hyperemic; the uvula was hyperemic and edematous in the more severe cases. Tenderness and pain over the scalp, usually limited to one side, and other manifestations referable to the nervous system were more common during the epidemic of 1932 than during that of 1931, and concomitantly, the incidence of isolation from the throat of streptococci having neurotropic velocity was higher during the epidemic of 1932. The acute stage lasted usually for from three to five days. Following this there were prostration and exhaustion, often directly proportional to the severity of the attack; these features were more common and more marked during the epidemic of 1932. It is estimated that during each of the epidemic waves about one fourth of the student body had some sort of respiratory infection and about one tenth had attacks justifying the diagnosis of influenza. Bronchopneumonia developed in a number of cases during both epidemics; one student died of this complication in the epidemic of 1932. Only pasteurized milk was used. At the height of the epidemic it was easy to make a differential diagnosis between, on the one hand, ordinary head colds or rhinitis, more severe colds associated with cough and evidence of involvement of the pharynx or bronchi but with only slight fever and aching and simple pharyngitis and, on the other hand, true influenza. This differentiation, as is usual in community epidemics, became increasingly difficult as the epidemic ran its course and as milder cases occurred. The type of cataphoretic velocity of the streptococci isolated in each of these three groups of cases was fairly distinctive, but as the symptoms and findings became atypical the cataphoretic velocity was likewise not typical of any of these groups.
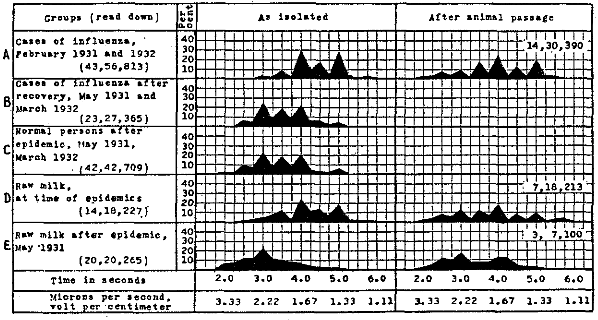
Chart 7.—Cataphoretic time and velocity of streptococci isolated from the nasopharynx and from raw milk in studies of two epidemics of influenza that occurred at a college.
As shown in chart 7, the velocity of the streptococci from the patients’ throats and from raw milk before, and less so after, one animal passage at the time of the epidemic was much less than that of the streptococci isolated from the patients after recovery and from the throats of normal students and from the milk of cows from one to two months after the epidemic had subsided. Cultures made from the pasteurized milk used during these outbreaks sometimes yielded streptococci, but the organisms usually had a normal type of velocity and only rarely the velocity characteristic of streptococci from influenza.
The patients who had influenza and the normal persons studied, as summarized in chart 8, were chiefly persons residing permanently in Rochester, Minn., and persons who had come to the Mayo Clinic for diagnosis and treatment. All were adults. There was marked similarity of the distribution curve of the velocity of the streptococci derived from these patients with influenza in 1931 and that of the streptococci found in the cases that occurred at the college and in Rochester in 1932. Streptococci having slowed velocity were found in greater number than that which obtains in the throats of normal persons in nonepidemic times in the two groups of normal persons at the time of the epidemic of 1932 (chart 8, Band C). As the velocity of the streptococci from the same group became more nearly normal one month after the epidemic of influenza had subsided, the incidence of streptococci of neurotropic velocity became abnormally high (chart 8, D), and as the distribution curve four months after the epidemic had disappeared became still more like that which obtains among streptococci from throats of well persons in nonepidemic times (chart 8, G), the incidence of streptococci having arthrotropic velocity became exceedingly high (chart 8, E). This was true, also, of the streptococci from the raw milk supply and other dairy products isolated four months after the epidemic had subsided (chart 8, F). Concomitantly with this marked increase in streptococci having arthrotropic velocity, several of the persons whose throats were swabbed repeatedly had symptoms of mild arthritis (as many as three of the group on the same day), and the general incidence of arthritis and myositis in Rochester noticeably increased. A distinct epidemic occurred among patients, nurses and attendants at the Rochester State Hospital; this was associated with a very high incidence of streptococci having arthrotropic velocity and virulence isolated from the nasopharynges of those ill. From two brands of cheese consumed generally in the hospital there were isolated pure, or nearly pure, cultures of streptococci having arthrotropic velocity and virulence. The epidemic subsided promptly after the use of these dairy products was discontinued.
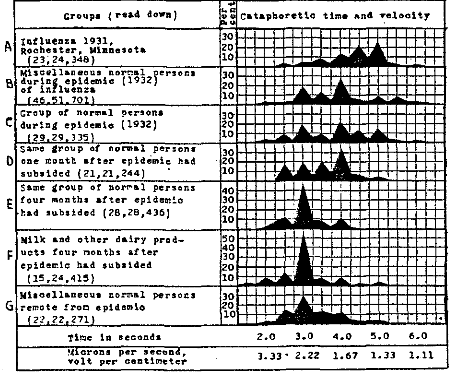
Chart 8.—Cataphoretic time and velocity of streptococci isolated from the nasopharynges of patients having influenza and of normal persons and from raw milk remote from an epidemic of influenza.
The cataphoretic time and velocity of the streptococci isolated in the cases of influenza, of postinfluenzal exhaustion and of contact with influenza that were encountered in Rochester during 1932, together with the time and velocity of the streptococci from normal controls, from milk and from other dairy products, are summarized in chart 9. The cataphoretic time and velocity of the streptococci, especially those isolated in the cases of influenza, were similar to the values which obtained during the outbreaks at the college, but were decidedly more neurotropic (28 per cent, chart 9, A) than those of the streptococci isolated during the epidemic at Rochester in 1931 (13 per cent, chart 8, A). Evidence of involvement of the nervous system in patients during and following attacks of influenza and in members of the population generally was correspondingly greater during and following the epidemic of 1932 than during the milder epidemic of 1931. There was marked similarity in type of velocity between the streptococci isolated from patients with influenza and those obtained from persons who had had contact with influenza (chart 9, D). The cataphoretic time and velocity were more nearly normal, but there was an abnormally high incidence of streptococci having neurotropic velocity among the organisms isolated from persons convalescing from influenza (chart 9, B) and from persons suffering from postinfluenzal exhaustion (50 per cent, chart 9, C), as well as a moderately high incidence among the streptococci isolated from normal persons during the latter part of the epidemic (32 per cent, chart 9, E), from normal persons soon after the epidemic had disappeared (28 per cent, chart 9, F) and from raw milk and other dairy products during the latter part of the epidemic (23 per cent, chart 9, G).
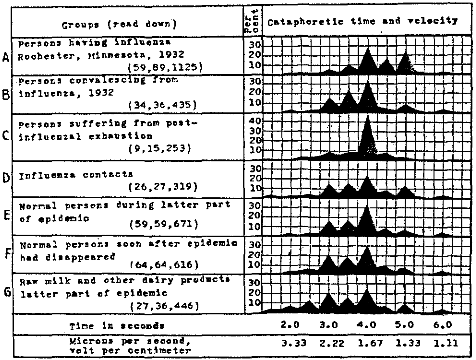
Chart 9.—Cataphoretic time and velocity of streptococci isolated from the nasopharynges of persons at the height of attacks of influenza and during convalescence of normal contacts and of well persons and from raw milk during and following an epidemic of influenza in 1932.
The striking similarity of the curves of distribution of cataphoretic time and velocity obtained with streptococci isolated from raw milk and from Streptococcus lacticus “starters” to those for streptococci isolated at the same time from the nasopharynges of persons suffering from the common cold and influenza during epidemics of these diseases and from well persons following epidemic influenza is strikingly shown in chart 10. This was also true of the streptococci isolated from the animals that succumbed to injections of the respective streptococci.
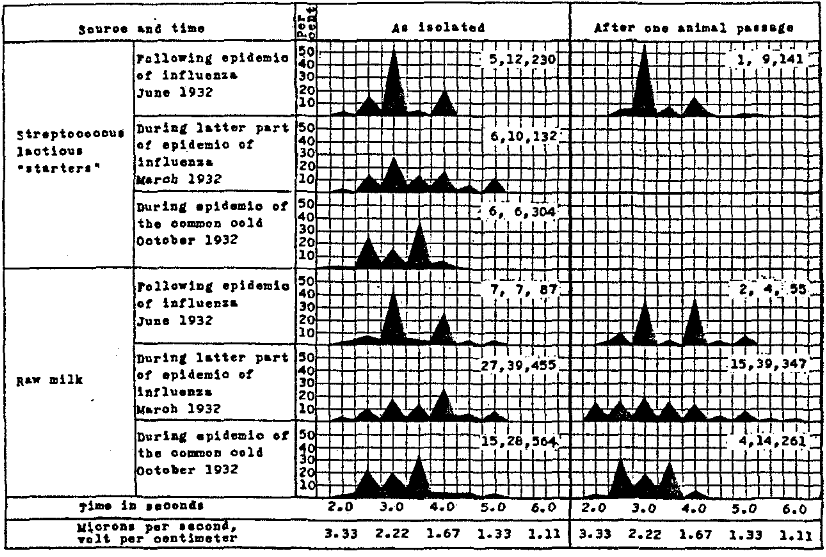
Chart 10.—Cataphoretic time and velocity of streptococci isolated from raw milk and Streptococcus lacticus starters during an epidemic of the common cold and influenza and following influenza.
In chart 11 are summarized graphically the results obtained in a study of the cataphoretic time and velocity of streptococci isolated from the nasopharynges of persons suffering from the common cold and from influenza and from the nasopharynges of well persons during epidemics of the common cold and influenza during three consecutive years, from 1930 to 1933. It will be noted that the average distribution curve of cataphoretic time and velocity is most constant and most distinctive in the different groups of cases of undoubted respiratory influenza, irrespective of season, year or epidemic prevalence. A high incidence of streptococci having cataphoretic time of 4, 4.5 and 5 seconds was found in each group, and a marked shift to neurotropic time (4 seconds) occurred in March, 1932, as the epidemic of influenza subsided, resembling the distribution curves for streptococci isolated during convalescence from influenza (chart 9). In general, the more severe the case, especially during the early part of an epidemic, and the more severe the outbreak, the more numerous were the streptococci that had particularly slow velocity.
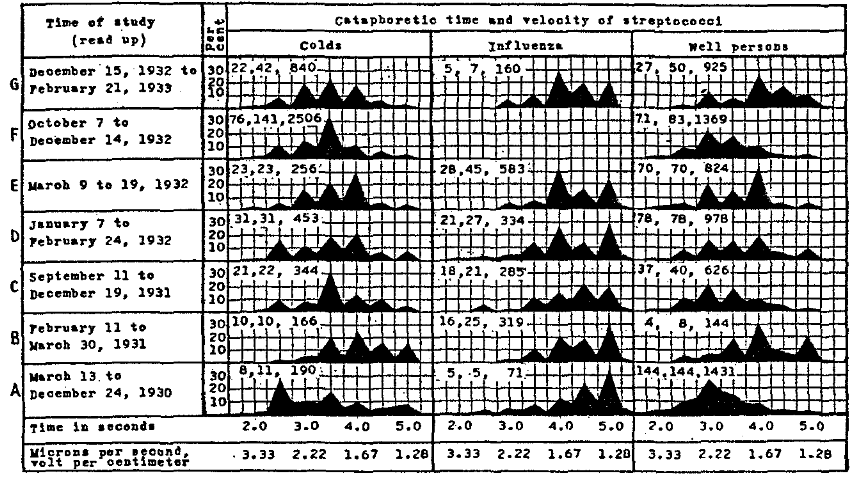
Chart 11.—Cataphoretic time and velocity of streptococci isolated from the nasopharynges of persons suffering from the common cold and influenza and of well persons.
The average distribution of cataphoretic time and velocity of streptococci isolated from the swabbings of the nasopharynges of persons suffering from the common head cold or sore throat during the autumn of the three consecutive years was much alike (chart 11, A, C and F, first column) and, at the same time, distinctly different from that for the streptococci from well persons and from patients considered to have influenza. Differential diagnosis between the common cold and influenza, from the clinical standpoint, as a rule was easily made. Rhinotropic and pharyngotropic cataphoretic time and velocity (2.5 and 3.5 seconds; 2.66 and 1.9 microns per second, volt per centimeter) predominated in each consecutive group of cases. With the approach of winter and a concomitant increase in the severity of the respiratory infections, differential diagnosis became more difficult on clinical grounds, and in studies of cataphoresis of the streptococci isolated from the nasopharynx, a slower, more “influenzal” type of cataphoretic time and velocity was found each winter among persons considered to have simple head colds and sore throats (chart 11, B, D and G, first column) while epidemics of influenza occurred.
Likewise, the average distribution of cataphoretic time and velocity of streptococci isolated from well persons was similar during the autumn of each consecutive year, arthrotropic cataphoretic time and velocity (3 seconds; 2.22 microns per second, volt per centimeter) being the highest in each group (chart 11, A, C and E, third column). Each winter, while respiratory influenza was prevalent, a slower, more “influenzal” type of cataphoretic time and velocity of streptococci isolated from the nasopharynges of well persons (chart 11, B, D and G, third column) supervened.
Through the cooperation of different members of the Section on Dental Surgery of the Mayo Clinic I have had an opportunity to study the cataphoretic time and velocity of streptococci isolated from the apexes of pulpless teeth. As shown in chart 12, the streptococci isolated from the apexes of infected pulpless teeth of persons suffering from different diseases reveal similar changes according to season and according to whether epidemic respiratory infections are present. It will be noted that the distribution curve of cataphoretic time and velocity of streptococci isolated from persons with encephalitis (chart 12, A, column 1), arthritis (chart 12, B, column 1), ulcer of the stomach and duodenum (chart 12, C, column 1) and iridocyclitis and uveitis (chart 12, D, column 1) remote from epidemics of influenza was characteristic of each of these diseases. The cataphoretic time and velocity of streptococci isolated from the persons having diseases not suspected of being due to streptococci were like the values for streptococci isolated from well persons remote from epidemic influenza (chart 12, E, column 1). However, in all of these groups the cataphoretic time and velocity of the streptococci isolated in studies made during the winter as epidemic influenza was occurring resembled (chart 12, A, B, C, D and E, column 2) more or less the values for streptococci from patients with influenza (chart 12, F, columns 1 and 2).
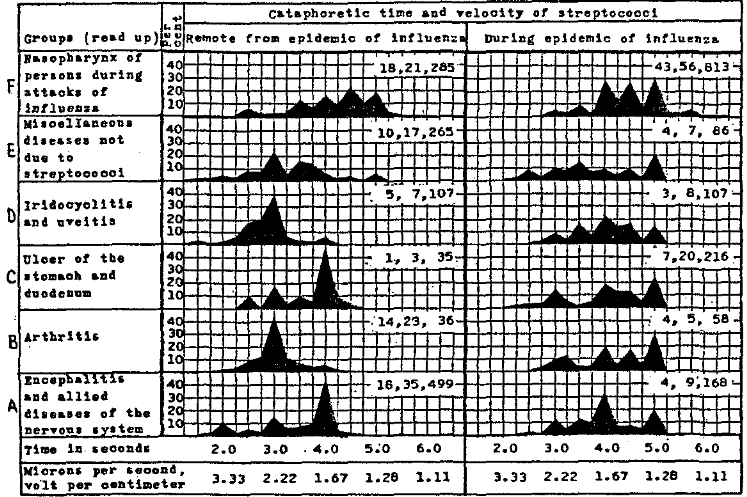
Chart 12.—Cataphoretic time and velocity of streptococci isolated from the apexes of pulpless teeth of persons suffering from different chronic diseases remote from and during epidemics of influenza.
As shown in chart 13, the distribution curve of cataphoretic time and velocity of streptococci isolated from infected teeth of well persons during the summer of 1932 (chart 13, A) was strikingly similar to that of streptococci isolated from the nasopharynges of well persons remote from regions of epidemic respiratory infections (charts 4 and 8). On the other hand, the distribution curve of cataphoretic time and velocity of streptococci isolated from the teeth of well persons during the autumn of 1932 resembled that of the streptococci isolated from the nasopharynges of well persons during the same season for each of three years (chart 11, C and F) and in each instance resembled most that of the streptococci isolated in cases of the common autumnal cold. The streptococci isolated from the infected teeth of persons suffering from neuritis, multiple sclerosis, herpes zoster, postinfluenzal exhaustion, dementia praecox and certain forms of psychosis during the summer months, when infections of the respiratory tract were largely absent, had chiefly neurotropic cataphoretic time and velocity, while those isolated from a patient with syphilis of the central nervous system had a very different but normal distribution curve of cataphoretic time and velocity.
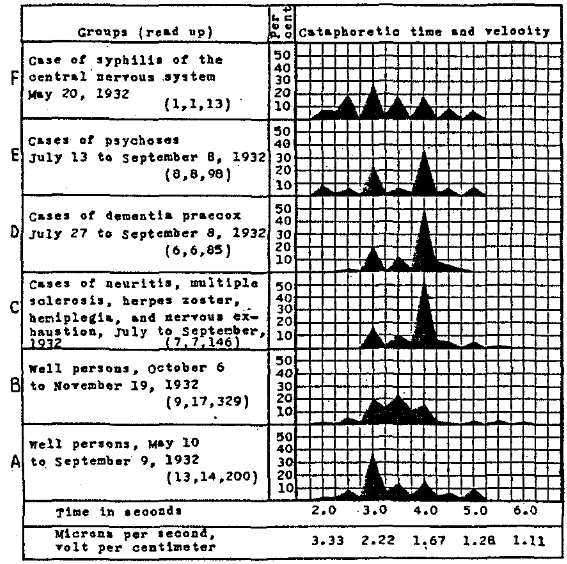
Chart 13.—Cataphoretic time and velocity of streptococci isolated from infected teeth of well persons and of persons suffering from diseases of the nervous system.
Through the cooperation of members of the diagnostic staff and the Division of Pathology of the Mayo Clinic, of Dr. F. G. Carter, Superintendent of Ancker Hospital, St. Paul, and of Dr. G. E. Fahr, of the Minneapolis General Hospital, I have had the opportunity of making a similar study of pneumococci and streptococci isolated from the nasopharynges and sputum of persons with lobar pneumonia and bronchopneumonia during epidemics of the common cold and influenza.
The distribution of the velocity of pneumococci isolated from the nasopharynx in cases of lobar pneumonia during influenza and during epidemics of the common cold, in contrast to that of pneumococci or streptococci obtained from the nasopharynx at the height of attacks and during convalescence in cases of common cold, influenza and bronchopneumonia, is summarized in chart 14. In the cases of lobar pneumonia, the velocity of the pneumococci from the nasopharynx in primary cultures was extremely high, and that for the pneumococci from the nasopharynx in subcultures and for those from the sputum in cultures and subcultures was greatly reduced (chart 14, B). After animal passage the velocity of the pneumococci from the nasopharynx in cases of lobar pneumonia was scattered (chart 14, A). The velocity of the streptococci isolated in cases of common cold, greater at the onset than during convalescence both before (chart 14, C and D, first column) and after animal passage (chart 14, C and D, second column) occupied a position between the values for pneumococci from lobar pneumonia and those for streptococci from influenza. During the acute stage of cases of influenza the velocity of the streptococci was the lowest yet studied (chart 14, E). During convalescence the velocity, instead of being less, as during convalescence from common cold, was greater (chart 14, E, first column). This was true also of these strains after animal passage (chart 14, E and F, second column).
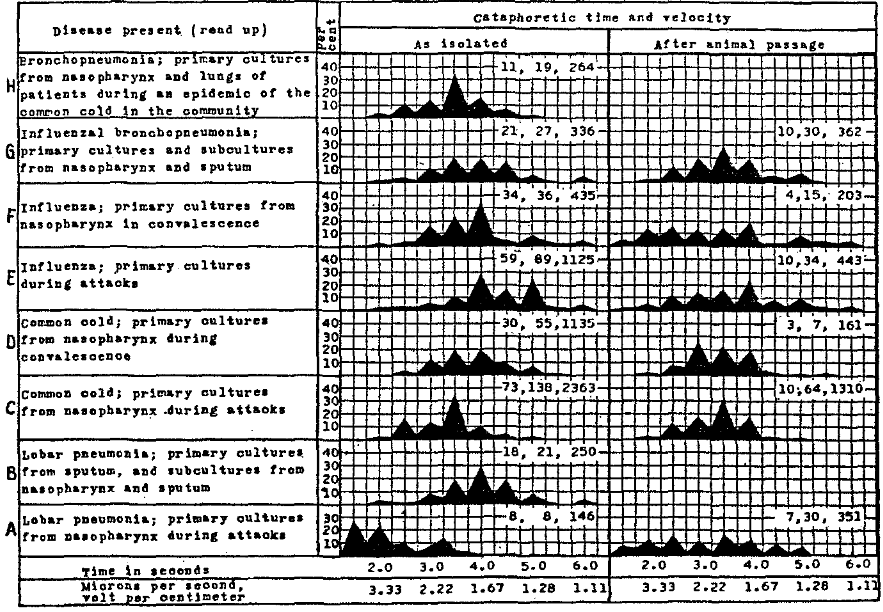
Chart 14.—Cataphoretic time and velocity of streptococci and pneumococci isolated from patients with lobar pneumonia, the common cold, influenza and bronchopneumonia.
The cataphoretic velocity of streptococci from the nasopharynx and sputum in cases of influenzal bronchopneumonia was identical. It resembled most that of the streptococci from uncomplicated cases of influenza but was distinctly greater, both before and after animal passage, than that of the streptococci isolated during the primary phase of influenzal infection (chart 14, G). The cataphoretic velocity of the streptococci isolated from the nasopharynx and lungs in the cases of bronchopneumonia that occurred during epidemics of the common cold (chart 14, H) resembled closely the velocity of the streptococci in the cases of uncomplicated common cold (chart 14, C).
The cataphoretic velocity of streptococci isolated in cases of acute sinusitis and otitis media, as a rule, was like that noted in the epidemic in which these conditions were complications. If the sinusitis or otitis occurred during an attack of the common cold, or of the bronchial type of cold, the velocity of the streptococci isolated from the pus, like that of those isolated from the nasopharynx, was chiefly pharyngotropic. If the sinusitis or otitis occurred during an attack of influenza, the velocity, like that of the streptococci from the nasopharynx, was usually influenzal. This was generally true also of streptococci isolated from the exudate or secretions from the infective processes in more remote parts of the body, as in the prostate gland and the seminal vesicles and in the uterine cervix. In cases of chronic sinusitis, prostatitis and endocervicitis, the cataphoretic velocity of the streptococci isolated was usually like that of the organisms from the nasopharynx and teeth, and in nonepidemic times was usually characteristic of the disease from which the patient was suffering.
The distribution curves of cataphoretic time and velocity of the hemolytic streptococci isolated from the nasopharynx in cases of acute follicular tonsillitis and of septic sore throat were very different from those of the hemolytic and green-producing streptococci sometimes isolated in cases of influenza and of the common cold. In harmony with the common occurrence of arthritis during and following attacks of follicular tonsillitis and especially of septic sore throat, the curves resembled closely that of streptococci isolated in cases of arthritis, organisms having arthrotropic time and velocity predominating.
Serologic Studies
The results summarized in table 1 are illustrative of a large number of experiments performed with the serums of patients having influenza and of controls and with streptococci isolated in studies of influenza and other diseases. As shown by the dilution method, the serum of patients during attacks of influenza develops a marked increase in slowing power over the streptococci isolated as recovery ensues. This action is largely specific. The serum of the patient with encephalitis following influenza and of the patient with transverse myelitis following mumps during an epidemic of influenza developed increased slowing power over the streptococci of influenza as well as over the streptococci from cases of encephalitis. The cataphoretic time and velocity of streptococci isolated from the former patient were influenzal during the antecedent attack of influenza and markedly neurotropic during the attack of encephalitis. From the results given in table 2 it is evident that the streptococci associated with epidemic influenza are much alike but not wholly identical serologically in different epidemics of this disease of varying degrees of severity.
Table 1.—Increased Slowing Power of the Serum of Persons Convalescent from Influenza on the Streptococci Isolated in Studies of lnfluenza
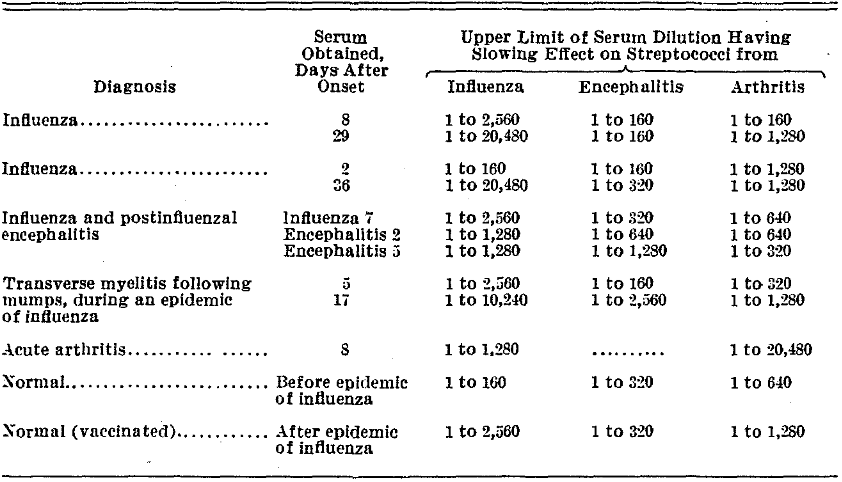
Table 2.—Slowing Effect of the Serum of a Patient During and After an Attack of Influenza on Streptococci lsolated in Studies of lnfluenza
*After an institutional outbreak of Influenza.
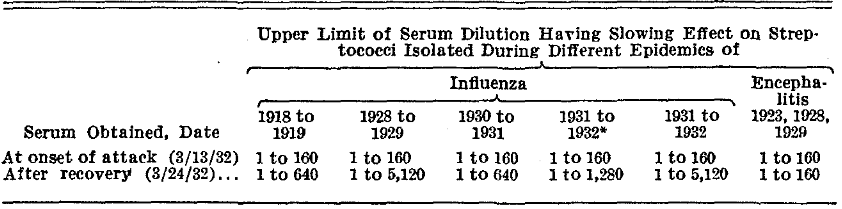
The slowing action of serum taken during and following colds and influenza in one dilution (1 to 200) over streptococci isolated in studies of these diseases is given in table 3. The three experiments, it is thought, suffice to illustrate, in general, the results obtained by this method. The figures in the body of the table, except those giving the average cataphoretic time, indicate the percentage of slowing action of the serum over the velocity of the streptococci in the sodium chloride solution controls. The respective serums and suspensions, each consisting of 3 cc., representing a 1 to 200 dilution of the serum and a density of streptococci equal to about one-half that of a broth culture, were incubated at 35 °C. for one and a half hours and then placed in the refrigerator over night. The tubes were then inspected for agglutination and centrifugated, and the sedimented streptococci were suspended first in about 2 cc. of distilled water and then in from 15 to 17 cc. The material was poured into the cataphoresis cell, and the migration rate of twenty organisms in each suspension, including the salt solution control suspension, was determined immediately as in the case of cultures. It will be seen that the serum from patients convalescent from colds or from influenza develops an increased power to slow the cataphoretic time and velocity of streptococci isolated in cases of both the common cold and influenza. The action was generally greatest on the streptococci characteristic of the disease. The serum of patients with influenza usually had a greater action on the streptococci isolated in cases of the common cold than had the serum of patients with the common cold on streptococci from influenza.
Table 3.—Slowing Action of Cold and Influenza Convalescent Serums on Cataphoretic Time and Velocity of Streptococci
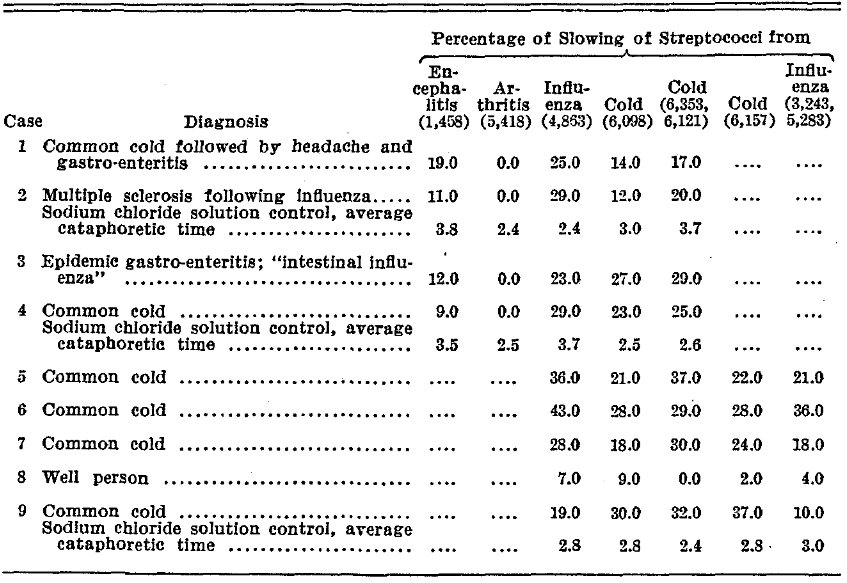
In experiments on a biologic method for the standardization of antiserums prepared in the horse with green-producing streptococci isolated in studies of poliomyelitis, encephalitis, ulcerative colitis and other diseases, it was found that in general the greater the cataphoretic slowing action of the serums in the different dilutions tested on the respective streptococci, the quicker was their destruction on intraperitoneal injection into mice. This reaction was found to be highly specific with the higher dilutions of the serums. The method is now being used to determine more precisely, if possible, the etiologic relation of streptococci having elective localizing power to the diseases in which they have been isolated. The results of two experiments on the cataphoretic slowing and antibody action of pooled serums from well persons and from persons recovering from colds and from influenza, respectively, on the streptococci isolated in these diseases will suffice to illustrate the results obtained along this line (table 4).
Table 4.—Cataphoretic Slowing and Antibody Action on Streptococci of the Serum of Persons Recovering from Colds and lnfluenza
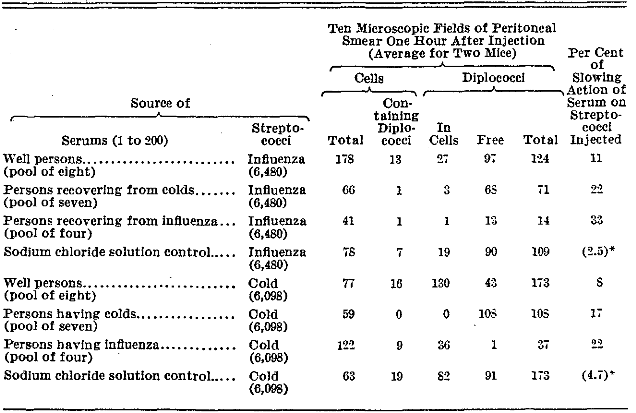
*The average cataphoretic time of the streptococci in the sodium chloride solution control suspension.
The suspensions of streptococci were made in duplicate, one for cataphoresis and one for intraperitoneal injection, and represented a 1 to 200 dilution of the respective serums, containing about 1,000,000,000 streptococci per cubic centimeter. The streptococci derived from patients with colds had been preserved in the dense glycerin-salt solution menstruum for nine months; those from patients with influenza, for fifteen months. Both revealed large numbers of viable streptococci on plating. The diluted suspensions were incubated at 35 °C. for an hour and a half; they were then put in the refrigerator over night, after which readings and injections were made. One and five-tenths cubic centimeters of each was injected intraperitoneally into a mouse, and small amounts of peritoneal fluid were withdrawn with a small Pasteur pipet drawn to a fine point after one, four or seven and sixteen or twenty-four hours. In some instances smears were made also of scrapings of the peritoneal linings in mice killed with ether. Smears of the same size, of like amounts, were made on glass slides stained by the Gram-safranin stain and examined microscopically. The total number of cells, the number of cells containing diplococci, the number of diplococci in cells, the number free and the total number in ten oil immersion fields were determined as a routine. The results recorded in table 4 represent the average of findings on two mice one hour after injection. It will be noted that the rate of destruction of streptococci following treatment in the different serums and following intraperitoneal injection into mice was roughly proportional to the degree of cataphoretic slowing action, that normal serum had no effect or only a slight effect, that convalescent “cold” serum had a moderate effect and that convalescent influenza serum had a marked effect. The cells in the exudate were chiefly polymorphonuclear leukocytes. Evidence of lysis was found both within and without cells; it was most marked in the smears that contained the fewest organisms. There was no striking evidence that the more rapid disappearance of the organisms previously acted on by the convalescent serums was due to phagocytosis by the fixed cells of the peritoneum. It seemed clearly to be due to the intracellular and extracellular lysis in the peritoneal exudate. The findings in the smears made after one hour were usually representative of those made later. Smears made after twenty-four hours were nearly always free from streptococci if derived from mice previously treated with convalescent serums and showed a small and a moderate number, respectively, if derived from those treated with normal serum or from those given injections of sodium chloride solution as controls.
The cataphoretic slowing and antibody action of the convalescent cold and influenza serums, crosswise, on the respective strains of streptococci is to be expected, considering the close relationship of the clinical manifestations in some of the cases, and the close resemblance cataphoretically of the streptococci isolated during colds, especially during the late stages, to the streptococci isolated during influenzal attacks. In order, however, to be certain regarding this point, I determined the average cataphoretic time and velocity of the streptococci isolated from the seven well persons, the eight who had colds and the four who had influenza whose serums were pooled. The distribution curve of cataphoretic time and velocity of the streptococci from the well persons resembled that of the streptococci of well persons during epidemics of respiratory infection; that of the streptococci from persons having colds and influenza was mainly characteristic of organisms found in the presence of these infections, but there was a large number of organisms the cataphoretic time and velocity of which were common to both conditions.
Comment
The cultures made from the nasopharynges of persons during attacks of common cold and of influenza, from the nasopharynges of well persons and from raw milk yielded a great preponderance of green-producing streptococci. Aerobic blood-agar platings sometimes revealed only a few colonies of streptococci and occasionally no growth at the very onset of attacks of acute rhinitis or head cold. This should not be interpreted as meaning that streptococci were not at hand, for abundant growth of streptococci having characteristic cataphoretic velocity and virulence occurred in the dextrose-brain broth, and in smears from the sediment of the gelatin-Locke’s solution washings of the swabbings, as in the cataphoretic cell, diplococci or streptococci were about as abundant as later in attacks. The streptococci seemed merely to be more sensitive in their growth requirements and more anaerobic at the onset of attacks. The streptococcic flora obtained on blood-agar in the different conditions studied, aside from the fact that streptococci were usually more numerous than in well persons, was not distinctive. The moist, encapsulated streptococcus commonly isolated early during the pandemic of influenza of 1918 to 1920,4 was encountered rarely during the several epidemics of influenza studied. This was true also of the influenza bacillus.
When the streptococci almost always predominantly present in the nasopharynx were studied cataphoretically, directly or after growth in dextrose-brain broth (other mediums do not suffice for routine work), distribution curves of cataphoretic time and velocity characteristic of the different epidemic diseases studied and of the associated complications were obtained with great regularity. This was true alike of the green-producing type of streptococci predominatingly present and of the hemolytic streptococci isolated less often. It was likewise true of the streptococci isolated from animals that succumbed to injections of streptococci shown to have characteristic cataphoretic time and velocity, and here too it made no difference whether they were green-producing or hemolytic on blood-agar. The curves of distribution of cataphoretic time and velocity were found to be most characteristic during the early stages of acute attacks, especially during the early stages of sharp epidemic waves. At the onset of attacks during the early stages of epidemics of the common cold there was usually a preponderance of streptococci having rhinotropic cataphoretic time and velocity (2.5 seconds; 2.66 microns per second, volt per centimeter). If rhinitis and sore throat occurred simultaneously in the same person in the early stages of epidemics in the autumn, the cataphoretic time and velocity were usually mixed rhinotropic and pharyngotropic, the former often predominating. Later in individual cases, and later in epidemic waves, when symptoms of sore throat and bronchitis and sometimes of bronchopneumonia supervened, there was usually a proportionately greater preponderance of streptococci having pharyngotropic cataphoretic time and velocity (3.5 seconds; 1.8 microns per second, volt per centimeter). Still later in epidemics, when the symptoms of the common cold had become more severe and involvement of the larynx, trachea and bronchi and sinuses was more common from the outset or became manifest during the course of attacks, there was a further shift toward the slower type of cataphoretic time and velocity characteristic of influenza. Finally, in cases of undoubted influenza, especially at the height of epidemic waves, characterized by a disproportionate constitutional reaction, “the cataphoretic time and velocity were slower than in any disease yet studied, the peaks in the curve occurring at 4, 4.5 and 5 seconds and 1.67, 1.48 and 1.33 microns per second, volt per centimeter. At the onset of attacks and epidemics severe general aching was usually associated with a particularly high incidence of streptococci having cataphoretic time and velocity of about 5 seconds and 1.33 microns per second, volt per centimeter —expressive, it would seem, of high toxigenicity. If manifestations referable to the nervous system, such as severe headaches or neuritis, were unusually marked in cases of influenza, the incidence of streptococci having neurotropic cataphoretic time and velocity (4 seconds; 1.67 microns per second, volt per centimeter) was often particularly high. Marked deviation from the usual cataphoretic time and velocity of the streptococci often occurred during the latter part of individual attacks, during late stages of epidemic waves and under unfavorable conditions for growth of the streptococci in vitro and in animals. Close correlation between the curves of distribution of cataphoretic time and velocity and the type of respiratory infection was possible, as a rule, only during the early stages of epidemic waves. After streptococci having peculiar epidemic characteristics had been generally prevalent for a time a general increase in resistance to epidemic strains of streptococci seems to have occurred, owing, it would seem, to mild and symptomless infections, and concomitantly there seemed to be a shift in cataphoretic time and velocity and a decrease in virulence of the streptococci. It was then not uncommon, especially in the spring (to mention only the most extreme discrepancy), to find streptococci having influenzal cataphoretic time and velocity, and less often influenzal virulence, in the nasopharynges of persons suffering from symptoms of a mild head cold, without aching or other constitutional reactions, instead of streptococci having chiefly rhinotropic and pharyngotropic time and velocity as in autumnal cold with like symptoms. The changes in the cataphoretic time and velocity of the streptococci appeared to be expressive of alterations in virulence or invasive power and of a protective mechanism for the survival of the micro-organisms in response to unfavorable or other conditions influencing growth. Evidences of exalted and peculiar invasive power were especially noticeable when the changes in cataphoretic time and velocity occurred suddenly, as at the outbreak of sharp epidemics and during the course of infections in individual patients and in inoculated animals.
The changes in the type of colony produced on blood-agar and in the cataphoretic time and velocity of the streptococci, especially in influenza, noted in this study in individual cases, on animal passage, on cultivation in vitro and during epidemic waves were similar to those noted during my studies of streptococci isolated in the pandemic of influenza of 1918 to 1920.7 The character of colony formation on blood-agar, the virulence on successive animal passage and the behavior in response to a hyperimmune serum prepared from one epidemic strain were the measures of change at that time.
The demonstrated prevalence in the nasopharynges of well persons of streptococci having characteristics like those of streptococci isolated from persons suffering from attacks of these diseases during epidemic waves, although the organisms occurred in smaller numbers and were of lesser virulence, is in accord with the general prevalence of the inciting agent assumed by epidemiologists in attempting to explain the rise and fall of epidemic waves of respiratory infection. However, the general prevalence of these streptococci is due, it would seem, to causes chiefly other than contact infection, because they are found widespread in the throats and teeth of well persons and in persons ill with chronic diseases without history of exposure and because streptococci from raw milk and strains of Streptococcus lacticus starters isolated at the same time revealed similar epidemic characteristics. A general influence seems to be operative, depending, it would seem, on changes in the weather or on some wholly obscure factor to which streptococci in throats, in the apexes of teeth and in more remote foci of human beings and in the udders and milk of cows respond simultaneously in a certain way. The shift in cataphoretic time and velocity during and after convalescence and following artificial cultivation to the values typical of streptococci in the nasopharynges of well persons in nonepidemic times and the concomitant loss of general and characteristic virulence indicate that the respective strains represent streptococci which are normally present in the respiratory tract but which have acquired temporary specific properties. The spread by contact of strains that have acquired exalted virulence and other peculiar properties and hence are a factor in epidemics is taken for granted. The results of my studies on cataphoresis are considered as corroborative of the work of others in this field,8 but are more precise because dextrose-brain broth was used to cultivate the streptococci.
The cataphoretic time and velocity of streptococci isolated from the nasopharynges of human beings in epidemics of the common cold and of influenza, respectively, were much alike for each of three consecutive years. Therefore, I have anticipated these infections among persons especially susceptible by prophylactic inoculation with the respective vaccines prepared from freshly isolated strains of the streptococci or from those preserved in dense suspensions of glycerin (2 parts) and sodium chloride solution (1 part) and shown to have characteristic cataphoretic time and velocity. The details of this study will be published later; suffice it to state that by the use of the cold vaccine in autumn and the influenza vaccine in winter and spring gratifying results have been obtained which were similar to those obtained during the pandemic of 1918 to 1920 with a similarly prepared vaccine.9
The incidence of streptococci having neurotropic velocity and virulence among persons convalescent from influenza and among well persons as epidemics of influenza subside is high. The high incidence of such streptococci is especially marked in cases attended by undue exhaustion. It is more marked in some epidemics than in others. This high incidence does not occur in connection with epidemics of the common cold. The foregoing facts may explain why epidemics of encephalitis and other diseases of the nervous system usually follow especially the more severe infections of the respiratory system commonly designated as influenza. The general presence in abnormal number of streptococci having neurotropic time and velocity in the throats of well persons during and after epidemics of influenza, which also varies with different epidemics and parts of epidemics, should lead to inquiry by clinicians in cases of encephalitis or other diseases of the nervous system, not only as to whether there was an antecedent attack of influenza but as to whether the symptoms began during or following an epidemic of this disease. The demonstrated slowing action of the serums of persons convalescent from the common cold and influenza on the cataphoretic time and velocity of the streptococci isolated in these diseases, and their antibody action on the respective streptococci, resulting in the accelerated destruction of the organisms following intraperitoneal injection into mice, indicate that the streptococci isolated in the common cold and influenza are closely related and that they have etiologic significance.
Conclusions
Streptococci and pneumococci isolated in studies of the common cold, influenza, simple bronchopneumonia, influenzal bronchopneumonia and lobar pneumonia have distinctive distribution curves of cataphoretic time and velocity on isolation. The serum during and following attacks of the common cold and of influenza contains specific antibodies (cataphoretic slowing power) for the streptococci of these diseases. The changes noted in the cataphoretic time and velocity of the streptococci during the rise and fall of epidemic waves of these diseases appear to be not merely coincidental but expressive of determinative properties. The etiologic importance of streptococci and pneumococci in these diseases is emphasized.
References Cited:
- Rosenow, E. C., and Jensen, L. B.: Staff Meet., Mayo Clin. 5:49, 1930; Infections of the Central Nervous System, an Investigation of the Most Recent Advances, Association for Research in Nervous and Mental Diseases, Baltimore, Williams & Wilkins Company, 1932, vol. 12, chap. 10, p. 208.
- Rosenow, E. C.: Infect. Dis. 50:377, 1932.
- Exper. Med. 40:453, 1924.
- (a) Mathers, George: Infect. Dis. 21:1, 1917. (b) Rosenow, E. C.: ibid. 26:469, 1920.
- Rosenow, E. C.: Staff Meet., Mayo Clin. 8:6, 1933.
- A. B. Stewart, Owatonna, Minn., gave me the opportunity to make these studies.
- Infect. Dis. 26:469, 567 and 597, 1920.
- Falk, I. S., and Jacobson, M. A.: Infect. Dis. 37: 507, 1925. Falk, I. S.; Jacobson, M. A., and Gussin, H. A.: ibid. 37:495, 1925. Jensen, L. B.: Proc. Soc. Exper. Biol. & Med. 23:783, 1926. Thompson, R. L.: Am. J. Hyg. 15:712, 1932.
- A. M. A. 72:31, 1919.