
Access to all articles, new health classes, discounts in our store, and more!
Additional Light on the Etiology and Nutritional Control of Dental Caries With Its Application to Each District Showing Immunity and Susceptibility
Read at the Seventy-Fourth Annual Session of the American Dental Association, Buffalo, N.Y., September 15, 1932. Published in The Journal of the American Dental Association, Vol. XX, September 1933, pp. 1648-1679.
* * *
An experimental basis for a new theory regarding the phenomena of dental caries has recently been presented.1 The data presented provide an explanation of many conflicts in interpretations made from available clinical and experimental studies and provide a bridge between the two main opposing views. The first, growing out of the work of Miller, Black and Williams, placed the responsibility on the action of bacteria as a controlling factor in the environment of the tooth and, hence, on the need for oral hygiene. The second placed the responsibility on metabolic processes, and hence was interpreted to be largely of nutritional origin. This theory has been supported by the work of McCollum, Mellanby, Price and others. A harmonization of these two theories is needed for practical progress in the control of dental caries, which is apparently on the increase in most of the civilized world.
The experimental and clinical data reported in the two communications referred to above can be summarized as follows: The routine chemical analyses of the blood from 400 successive cases revealed that when powdered bone chips were placed in blood serum or plasma, there was, in normal cases, a movement of calcium and inorganic phosphorus from the blood serum to the bone chips, but that, in certain pathologic conditions, frequently the movement of inorganic phosphorus and occasionally that of calcium was in the opposite direction; namely, from the bone chips to the blood serum or plasma. For sixty successive cases, it was found that, in fifty without marked evidence of decalcification of the skeleton, there was a reduction of 27 per cent in the calcium of the serum and 18 per cent in the inorganic phosphorus. In the ten others of this group, all of which were characterized by marked decalcification, the calcium moved from the blood serum to the bone chips in an amount of 24 per cent of the serum content, while the inorganic phosphorus moved in the opposite direction; namely, from the bone chips to the blood serum in an amount equal to 28 per cent of the inorganic phosphorus content of the serum. Studies were made on the effect of treatment through reinforcement of the nutrition with high mineral carrying foods and fat soluble activators, the latter as provided in exceptionally high vitamin butter and high vitamin cod liver oil. In two of the patients of the decalcifying group, one presented spontaneous fracture in which, before treatment, the inorganic phosphorus moved from the bone into the serum in the amount of 35 per cent of the total, and after treatment it moved in the other or normal direction in the amount of 15 per cent. Roentgenographically, the bones showed an increased density, with progressive calcification. In the other case, one of degenerative arthritis with marked decalcification in which, before treatment, the inorganic phosphorus moved from the bone chips to the serum in an amount of per cent, after treatment with nutritional reinforcement with high mineral carrying foods and fat-soluble activators (the latter as provided in exceptionally high vitamin butter and high vitamin cod liver oil), the inorganic phosphorus now moved in the other or normal direction in the amount of 34 per cent.
Since dental caries presents so much evidence of being influenced by the environment of the tooth, large numbers of saliva samples have been studied by this same procedure to ascertain the effect of the solubility factor of the saliva for calcium and phosphorus on susceptibility to dental caries and whether this factor may be a controlling one in the environment of the tooth which determined the level of immunity. The clinical and experimental results of this study have revealed that, in immunity to dental caries. the inorganic phosphorus and calcium moved from saliva to hone chips and that, in active dental caries, the inorganic phosphorus and sometimes the calcium (either or both) moves from the bone chips to the saliva instead of from the saliva to the bone chips. The discovery of this physicochemical condition immediately threw light on many of the clinical observations; for example, the progressive hardening of the surface of crowns of teeth for several months after eruption, and also on observations regarding the change in density of tooth structure under such stresses as pregnancy, wasting disease and rapid growth of childhood. These conditions are also favorable for the development of caries. The findings are very important, if they are found to prevail.
As a means for critically checking the application of these new principles, several groups of patients have been investigated. One, a large group, has consisted of clinical patients who had been studied carefully by roentgenographic examination, clinical examination (by instrument) and by chemical analysis of the saliva. Another group consisted of forty children from the Broadway Mission selected because of very rampant dental caries, their nutrition being very bad owing to the stress of the industrial depression. Many of these children had caries extending to the pulp chambers, though the pulps were still vital. The pulps were protected in most of these teeth with temporary fillings, and careful clinical inspection was made together with roentgenographic studies. These children received as treatment one well balanced meal a day especially reinforced in mineral carrying foods and high vitamin butter. This meal was commenced by each child in line taking a half a glass of tomato or citrus fruit juice and a teaspoonful of half and half of a high vitamin cod liver oil and high vitamin butter concentrate mixture provided by me. They then proceeded to the table and had a large bowl of vegetable and meat soup containing a varied assortment of vegetables and chopped meat prepared as stew. Many of the children took a second liberal helping of soup. For the next course, they had sliced canned peaches and delicious rolls made of freshly ground whole wheat to which had been added, on some occasions, an additional small quantity of fresh wheat germ. (This has been discontinued.) The whole wheat was ground in a motor driven coffee mill and prepared freshly from day to day. These rolls were spread liberally with an extra high vitamin butter, which had been produced by cows while pasturing on green wheat. Each child had also one or two glasses of milk. This meal was varied from day to day, but so designed as to maintain these high levels of fat-soluble activators, minerals and grain embryo. The children received six meals a week. The source of vitamin C was varied. Carotene was reinforced by adding to the vegetable soup finely ground small carrots of a deep yellow. These and the wheat germ were added to the vegetable soup after it was removed from the stove but still hot, to avoid the high temperature and long cooking, which would injure the activator content. This meal provided 1.48 gm. of calcium and 1.28 gm. of phosphorus in a single helping.
A third study group consisted of patients selected by groups of dentists in about a dozen cities each providing a patient with a history of marked susceptibility to dental caries. Control of the condition was undertaken by sending to these selected patients some high vitamin product and instructions relative to the reinforcement of the daily nutrition with high mineral carrying foods. In all of these groups, the average movement of inorganic phosphorus was in the wrong direction before treatment and in the right direction when the second sample of saliva was procured one or two months later. Additional roentgenograms were made from time to time, and in only one case was dental caries reported to be in progress.
In many cases, in all three groups, there was marked roentgenographic evidence of improvement in the density of the teeth, in reduction and size of the pulp chamber and in the building in of protective walls underneath the caries. Illustrations of these structural changes have been presented.¹
These and other data have suggested the urgent need that these new principles be checked in each group of individuals living in natural conditions which provide immunity and other groups living in conditions providing susceptibility, if such could be found living under very exacting nutritional conditions and where the diets could be studied and analyzed. This cannot be done with diets of those earlier civilizations and primitive people whose skeletons reveal complete absence of dental caries. This has constituted an important part of the new investigations, a preliminary report of which is included in this paper and a brief résumé of which has been made of studies conducted by me in Switzerland in 1931.
Since human nutriment in various parts of the world has contained a few principal food factors, there has been need for more detailed information regarding the variations in the mineral content of the same foods produced under different conditions and in different localities. This has been done both by chemical analysis of the foods and by studying the effect of these variations on experimental animals when detailed analysis could be made of the chemical content of tissues as well as minor and gross structural changes. This will throw light on the dietary studies of the experimental groups and will be presented first.
It will assist in visualizing the problem if we will first state briefly the principal factors that have seemed to be established. Arthur D. Black,2 in summing up the work of W. D. Miller, J. Leon Williams and G. V. Black, says:
“In brief, the facts are: 1. The structure of the tooth, except in gross defects such as pits and fissures, has little or no relation to the occurrence of decay…2. Caries always begins on the surface of the tooth or in a defective pit or fissure in the enamel and gradually progresses inward. 3. Caries practically always begins in certain protected spots and spreads on the surface within definite limits which are exactly definable as the area of liability for each surface. 4. Caries practically never begins elsewhere on the surface of a tooth, and the dentin is never involved until the enamel has been penetrated. 5. The dissolution of the structure of the tooth is caused by an acid formed by micro-organisms which are protected by a gelatinous plaque in such a way that the acid is confined to the particular spot and not allowed to become dissolved in the saliva. 6. The acidity of the saliva has nothing to do with the occurrence of decay.”
Robert Kesel3 summarizes past and present theories as follows:
“From a review of the past experiments and observations, what do we actually know about this disease, dental caries? We possess these facts:
- Primitive people both ancient and modern, living in their native environment, developed little decay.
- With the advancement of civilization with the refinement of food and living conditions, dental caries has markedly increased.
- Caries is, as a rule, most active during childhood and adolescence; that is, during the growth period.
- Metabolic disturbances produced by such conditions as pregnancy and diabetes seem to increase susceptibility to caries.
- The disease has never been produced outside the oral environment.
- It stops with the extraction of the tooth and ceases with the death of the individual. Teeth and skeletons are not subject to proteolytic decomposition as is the rest of the body.
- The crowns of extracted teeth mounted on artificial dentures and worn in susceptible mouths sometimes develop caries.
- Caries is confined largely to so-called areas of susceptibility. These are more or less protected areas, where there is opportunity for stagnation and the collection of foreign material. The more exposed areas, such as prominent angles and cusps, are immune.
- Caries does not begin or extend under healthy gum tissues.
- Aciduric and acidogenic bacteria can be found in the active carious cavity.
- These organisms can be cultured from the saliva of the susceptible individuals, yet not all susceptible areas in the mouth become carious, although exposed to the same bacteria. Of two approximating teeth, one may be destroyed by the carious process and the other not even be affected.
- The caries lesion, although developing in a susceptible area, may become arrested and remain so indefinitely.”
It is of interest that both of these reviewers refer to the available information as they have summarized it as “facts.”
Many investigators have laid much stress on the hardness or softness of foods, assuming that the former is necessary, yet large immune groups have existed whose diets have consisted of very soft and sticky foods. Hoppert, Webber and Canniff4 have recently presented data which they interpret to indicate that the coarseness or fineness of the cracked corn in an otherwise similar diet has made the difference between a very high and a very low incidence of dental caries in rats. Klein and McCollum,5 in discussing previously presented data, including that of Hoppert, Webber and Canniff, have interpreted the controlling factors as being involved in the levels and ratio of calcium and phosphorus as concerned in the development of dental caries in rats. They say:
- “Estimations of the phosphorus content of diets reported to produce caries in rats indicate that rations containing 0.4802 gm. of phosphorus per hundred grams of diet, or less than 0.4802 gm. of phosphorus per hundred grams of diet, tend to induce dental caries in rats if Ca intake is 0.3424 per cent.
- Estimations of the phosphorus content of diets reported to produce rats immune to dental caries indicate that such diets contain 0.5282 or more grams of phosphorus per hundred grams of diet and 0.4012 or less grams of calcium per hundred grams of diet.”
During the past decade, I have been making a study of the effect of various modifications of nutrition on the incidence of dental caries. The results have been presented in many reports.6 These have been reviewed in an article entitled “Control of Dental Caries and Some Associated Degenerative Processes Through Reinforcement of the Diet with Special Activators.”7 Data are there presented indicating that dental caries has been controlled by these procedures to about 90 per cent by reinforcing the nutrition with fat-soluble activators in natural form and high mineral foods in natural form. Many cases were reported in which, before treatment, there were as many as two or three dozen cavities, and after or during treatment with reinforced diet, they had either no cavities or one or two a year.
These studies have presented much evidence that phosphorus is a mineral that is frequently needed in larger amounts and, further, that its shortage in easily available natural foods is in part associated with and in part apparently controlled by the exhaustion of phosphorus in the soil. This latter phase has been discussed in another communication.8
An important phase of my investigations has been concerned with the variation in levels of natural food vitamins with the seasons and as influenced by geographic location, climate, altitude, etc. Seasonal cycles seem to have an important relationship to the seasonal incidence of many diseases, including dental caries. They further indicate that the vitamin levels of the butter-fat of milk as produced in various countries in the world and which show a seasonal cycle are directly related to the type of food being eaten by the cows, goats and other dairy animals. Among the foods found to be most favorable for the production of high vitamin levels have been rapidly growing young green wheat and rye.
The investigations herewith reported will accordingly cover (1) comparative levels of minerals in different cereal foods and the same cereal foods as produced in different places; (2) results from feeding fifteen different diets to fifteen groups of rats; (3) structural changes produced in human teeth by reinforced diet and (4) results of field studies of districts providing immunity and districts providing susceptibility to dental caries including chemical analyses of saliva.8
Experimental Data
1. Comparative Levels of Minerals in Different Cereal Foods and the Same Cereal Foods When Produced in Different Places.–Since different sections of the earth provide conditions which are especially suitable for certain cereal plants and unsuitable for others, the available food of different districts is essentially different, the people living in those communities being limited to that particular cereal. It is important that we know the mineral content of the cereals used in the animal experiments to be reviewed presently.
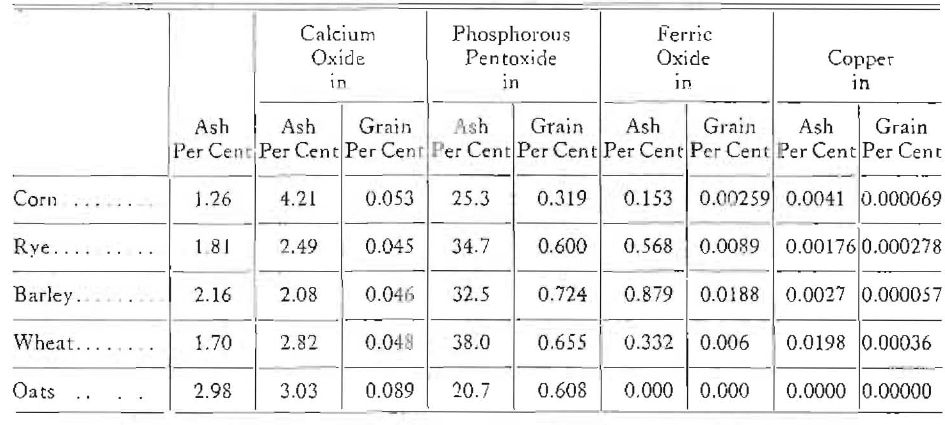
Data presented in Table 1 represent the averages of a number of determinations for each of the five cereals, corn, rye, barley, wheat and oats. Only the calcium, phosphorus, iron and copper content is shown in this table. It will be seen that the calcium level shown as the percentage of calcium oxide in grain is highest in oats, but the percentage in ash is highest in corn. The phosphorus as pentoxide percentage in grain is the highest in barley and more than twice as high as in corn. Indeed, the phosphorus of the corn is only about half as high on an average as in each of the other four cereals. This table may be very misleading unless we consider carefully the variations that can take place in the different samples of the same cereal which have grown in different places at the same time, the controlling factors being local.
Table 1. Comparison of Mineral Content of Different Kinds of Grain
A study, for example, of nine samples of wheat obtained on the market showed a variation in phosphorus content of over fourfold. So great a variation as this is not common. Through the assistance of the department of agriculture in Canada, I have received samples of the same marquis wheat grown in about twenty places in Canada. Data on seventeen of these are reported in Figure 1. The places are shown below each mention of calcium, phosphorus, potassium, magnesium, iron and protein. This is helpful in several ways, showing at a glance the relative amount of these minerals and the protein in wheat and, by the difference in the height of the columns, the variations that were found by growing this sample of wheat in seventeen places. At once we see that wheat carries a high percentage of phosphorus in comparison with the other minerals, particularly as compared with calcium. The animal body’s need for iron is imperative. The greatest variation of the minerals disclosed in the chart is found in the iron. The difference in the iron content in the last two samples of wheat is a little over fifteenfold. The significance of this will be discussed later. Further data will be presented on the mineral content of different diets containing cereals under the next heading.
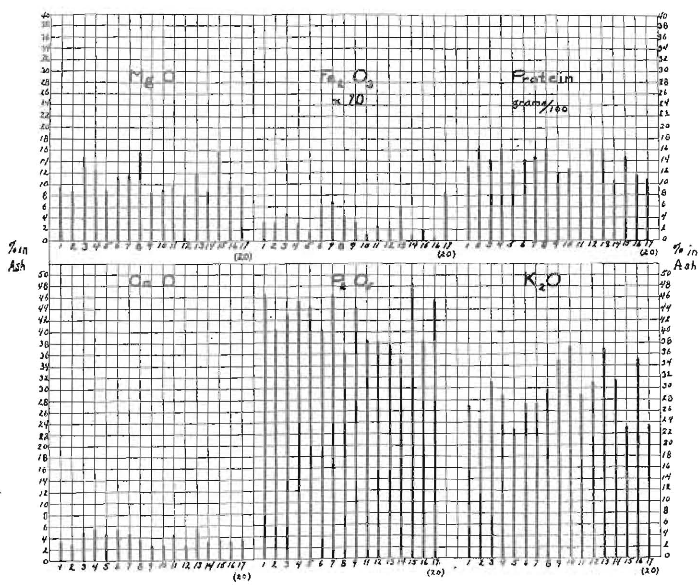
Fig. 1. Variations in mineral and protein content of the same Marquis wheat grown in seventeen different places in Canada, in 1929. The seventeen experiment stations of the department of agriculture were: 1, Brandon, Manitoba; 2, Swift Current. Saskatchewan. 3, A 12, Plot 13, Swift Current, Saskatchewan; 4, A 12, Plot 14, Swift Current, Saskatchewan; 5, Fredericton, New Brunswick; 6, Lacombe, Alberta; 7, Fort Veinillion, Alberta; 8, Indian Head, Saskatchewan; 9, Ste.-Anne-De-La-Pocatiere, Quebec; 10, Nappan. Nova Scotia; 11, Cap Rouge, Quebec; 12, Agassiz, British Columbia; 13. Scott, Saskatchewan; 14, Charlottetown, Prince Edward Island; 15, Rostheru, Saskatchewan, 16, Invermere, British Columbia; 17, (20), Kapuskasing, Ontario.
2. Results from Feeding Fifteen Different Diets to Fifteen Groups of Rats.–These diets have been planned on a basis that would make possible the comparison of the same cereals obtained from two different sources; namely, two kinds of corn and two kinds of wheat, and a modification of diets built on these cereals with activators and with different parts of the grain. It has been deemed important to make this study in order that detailed chemical analyses might be made of blood and other body tissues, as well as a study of the teeth for dental caries.
In planning this series of animal investigations, the following factors have been deemed important: (a) A comparison of different sources of the same food. For this, a feed corn of cheaper market value and a seed corn of a higher market value have been used. The wheats used were grown in two different localities. (b) A consideration of the relation of the coarseness and fineness. The corn factors used were on the same basis of separation with a twenty mesh screen as suggested by Hoppert, Webber and Canniff. (c) The influence of activators of different sources. (d) The use of inorganic tricalcium phosphate. (e) Comparisons of the different wheat products as provided in the whole wheat, the flour, the bran and middlings mixture. For these studies, fifteen groups of rats were provided consisting of from four to seven rats each. These were obtained from four different places in order to get as large a number of rats of approximately the same age. Each of these sources was represented in each of the first ten groups in one series and in each of five groups in a second series. The rats in these two groups differed in age, the first group averaging 8 weeks of age and the second group averaging 4 weeks of age at the beginning of the test. The feeding program for each of the fifteen groups was as follows. The variable factor was added as 69 parts to a basic diet of wheat gluten, 20 parts, whole milk powder, 5 parts, crisco, 5 parts, and sodium chloride, 1 part, as used by Hoppert, Webber and Canniff.
Group 1 received cracked feed corn, which included both the coarse and fine, with the following distribution of particles, 45 per cent remaining on a 20 mesh screen as used by Hoppert, Webber and Canniff. Group 2 received the fine corn, which went through the 20-mesh screen; Group 3, the coarse particles, which remained on the 20-mesh screen; Group 4, freshly cracked whole wheat with the mill at the same set; Group 5, the same as Group 1, namely, both coarse and fine corn meal plus a high vitamin butter ad libitum; Group 6, the same as Group 1, namely, both the coarse and fine corn meal plus 2 per cent of a mixture of a high vitamin butter and a high vitamin cod liver oil; Group 7, coarse and fine corn meal as in Group 1, plus 2 per cent of a mixture of high vitamin butter and a high vitamin cod liver oil and 10 per cent of wheat germ; Group 8, coarse and fine feed corn meal as in Group 1, plus 10 per cent wheat germ; Group 9, whole wheat plus 10 per cent wheat germ; Group 10, coarse and fine corn meal plus 10 per cent of dicalcium phosphate. The rats in Groups 11 to 15 inclusive were as stated younger than those in Groups 1 to 10 inclusive. Number 11 received the coarse screenings of a better grade of corn, sold as seed corn, otherwise corresponding with Group 3 plus the basic diet. Group 12 had fine screenings from seed corn as in Group 2. Group 13 received cracked Red Cross whole wheat. Group 14 received Red Cross flour and Group 15, received a Red Cross bran and middlings mixture as separated from Red Cross flour; all in addition to the basic diet. One hundred pounds of wheat was said to produce 73 pounds of flour, 16 pounds of bran and 11 pounds of middlings. (The miller’s report.)
The last three groups have been particularly interesting because of the need for the greatest possible efficiency in the planning of dietaries during this strenuous industrial depression. These three groups will be reviewed first.
The percentage gain in weight of these three groups after seven weeks of the feeding program was 154 per cent for Group 13, receiving the cracked whole wheat ration; 89 per cent for Group 14, receiving the flour of the wheat, and 112 per cent for Group 15, receiving the middlings and bran mixture. There was a great difference in the appearance of the animals, particularly in the fur coat which is illustrated in Figures 3 and 4. As is readily seen, the fur of these rats in the flour group came out in patches and looked very bad and they lacked the “pep” and energy of those in the other two groups. When a finger was snapped or any other sudden noise was made, rats on the flour jumped perceptibly as an involuntary reaction. This did not occur with either of the other two groups.
The mineral content of the Red Cross wheat, flour and bran and middlings, which were furnished to me by a miller who ground the wheat for the Red Cross, is presented in Table 2.
Table 2. Mineral Content of Red Cross Wheat, Flour and Bran and Middlings
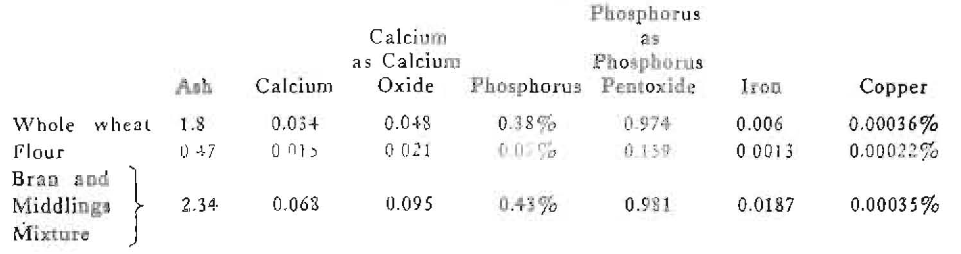
It is of interest to note that four fifths of the ash went with the middlings and bran. There was 2.26 times as much calcium and 5.26 times as much phosphorus provided in the whole wheat of a given weight as in the flour of that weight. The bran and middlings mixture provided 4.53 times as much calcium for a given weight as flour and 6.1 times as much phosphorus. These data are shown graphically in Figure 2, with the photographs of a typical rat from each of the three groups; namely, those receiving whole wheat, those receiving flour and those receiving bran and middlings mixture as a supplement to the basic ration. This chart should be read vertically. It is important that these figures and their significance be kept in mind, since it is not easily possible under ordinary conditions for most people to eat enough additional white flour products as a means of obtaining their required minerals to make up what has been lost by the removal of the bran and middlings. That this is true for the experimental animals used is emphasized by the fact that those receiving foods low in minerals, the flour mixture, ate less food instead of more. The physical differences which are so strikingly brought out in the photographs in Figures 2 and 3 were associated with a very marked difference in the structure of the various organs and tissues, including the teeth and their supporting structures. A detailed study of these seems to throw important light on the problems of the etiology and control of dental caries. The mineral content of diets 13, 14, and 15 is shown in Figure 2, for comparison. Note the wide variation.

Fig. 2. Distribution of minerals in Red Cross wheat. The rats were fed on these three different wheat products. Four gave marked evidence of lack of minerals.
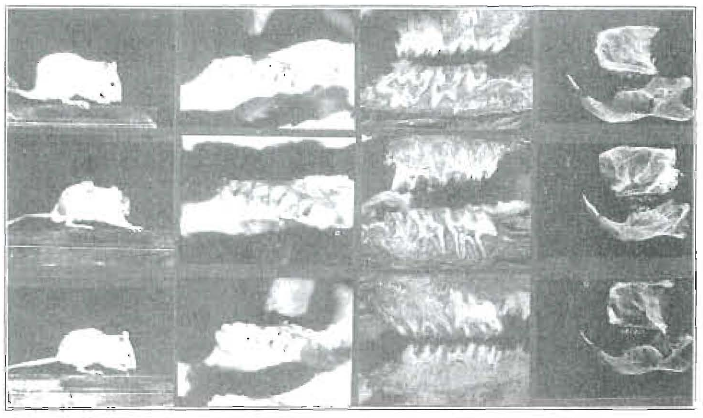
Fig. 3. Red Cross wheat studies. Above: Group 13, fed stock diet plus whole wheat (all of minerals); center: Group 14, fed stock diet plus wheat flour (one-fifth of minerals); below: Group 15, fed stock diet plus bran and middlings (four-fifths of minerals). The teeth of the rats on the wheat flour supplement showed active caries.
A series of studies of the teeth and their supporting structures are shown in Figure 3. In this chart, the data for each group are arranged horizontally. The first column shows another typical view of the rats of the three different groups. The second column shows photographs of the occlusal surface of the teeth. In these, it will be seen that the crowns are well formed in all three series. The second group, those on the white flour, show cavities extending into the teeth on the occlusal surfaces. The sulci of rats’ teeth are normally quite deep. The third column shows photographs of the ground sections of the teeth of each of the three groups. The second group shows marked destruction by caries of the crowns, approaching the pulp in some of the cavities. The first and third group are practically normal. The fourth column shows roentgenograms of the teeth which were prepared by first soaking the specimens in silver nitrate, a 10 per cent solution, for a few hours, then exposing them to light. In this condition, decalcified tooth structure which would normally be quite transparent to the roentgen-rays, becomes more opaque owing to the presence of metallic silver.
In Figures 2 and 3, I have shown the relationship between the physical conditions of the rats in the different groups, this depending on whether they received whole wheat, flour or the bran and middlings mixture. The difference in content of some of the chemicals in each of these three forms of wheat cereal and a comparison of the structure of the teeth of the rats fed on these three diets has been shown. These studies have also included a comparison of the levels of several of the minerals in the blood of rats on different diets with the difference in the levels of the minerals in the different diets. This is illustrated in Figure 4.
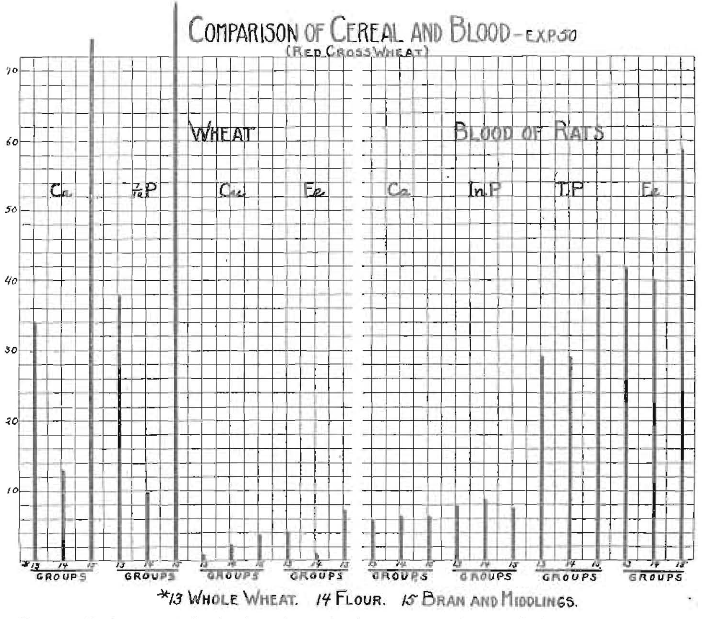
Fig 4. Deficiency of food minerals again demonstrated in chemical content of blood of rats.
It will be noted that the calcium and inorganic phosphorus of the blood is nearly the same in all three groups. There is a marked difference in the total phosphorus of the blood, it being much higher in Group 15 than in Group 13 or 14. The total phosphorus in the wheat is also much higher in Group 15, which is the bran and middlings mixture, than in the whole wheat group, and very much higher than in the flour group. The most striking difference is in the iron content of the three foods and the three specimens of blood, it being much lower in the flour than in either the whole wheat or bran and middlings mixture and much higher in the blood of the rats in this group and lower in the wheat flour group than in the whole wheat group. The significance of these data will be much more apparent when we come to the discussion of this summer’s studies of human beings showing immunity or non-immunity to dental caries.
The foregoing data have related to the last three groups of rats in the series of fifteen diets previously outlined. Several chemical factors in addition to these here presented have been determined on the blood of the rats of these fifteen series. This has been done by pooling the blood of the different rats in the groups. The levels of the various chemicals are shown in parallel columns for comparison in Figures 5, 6, 7 and 8. The remarkable influence of diet on some of the blood chemical factors is immediately made apparent by a comparison of the different heights of the columns.
In Figure 5 are shown the levels of each calcium, the percentage of change in calcium when powdered bone chips were added to the blood serum and percentage of calcium in the cells. Diets 1, 2 and 3, representing the feed corn, fine feed corn and coarse feed corn, respectively, are of special interest and should be noted in these various data because of the suggestion that the coarseness of the corn was the cause of decay in the series reported by Hoppert, Webber and Canniff.4 The blood serum calcium was slightly higher in the group of rats receiving fine feed corn. The percentage change of calcium plus bone was lowest in the group receiving the coarse feed corn, and the percentage of calcium in the blood cells highest in the group receiving the whole corn (both fine and coarse), and lowest in the group receiving the coarse feed corn. These changes were not nearly so great as the changes produced by some other factors, as, for example, the effect of adding dicalcium phosphate to the diets in Group 10 and an excess of wheat germ in Group 7.
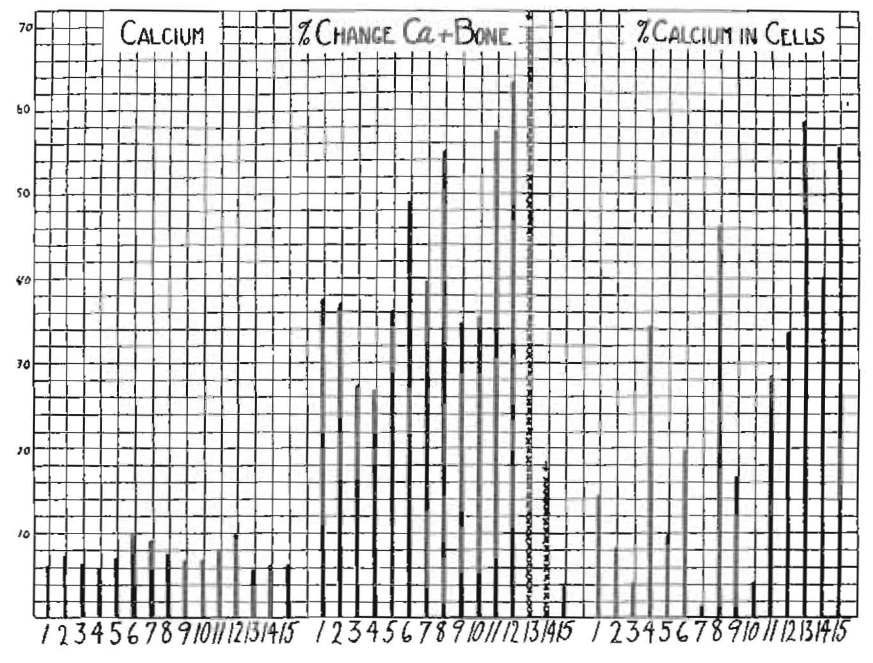
Fig. 5. Blood chemical changes of fifteen diets Comparisons in three blood factors calcium, percentage of change of calcium of serum plus bone and percentage of calcium in cells of rats fed on fifteen different diets. The crosses indicate a reverse direction of movement of calcium in the center group. The diets were: 1, fine and coarse feed corn; 2, fine feed corn; 3, coarse feed corn; 4, fine and coarse whole wheat; 5, No. 1 plus high vitamin butler; 6, No. 1 plus 1 per cent of cod liver oil and of high vitamin butter; 7. No. 6 plus 10 per cent wheat germ; 8, No. 1 plus 10 per cent wheat germ; 9, No. 4 plus 10 per cent wheat germ; 10, No. 1 plus dicalcium phosphate; 11, coarse seed corn; 12, fine seed corn; 13, Red Cross fine and coarse whole wheat; 14, Red Cross flour; 15, Red Cross bran and middlings.
Figure 6 shows, for comparison, the inorganic phosphorus, the per cent change in inorganic phosphorus when powdered bone chips were added to the blood serum and the percentage of phosphorus in the cells. In observing these different levels, it is important to observe that two different kinds of corn, one a low grade commercial feed corn (used in diets 1, 2 and 3), the second a high grade commercial seed corn (used in diets 11 and 12); also wheat from two different sources, one used in diet 4, and the other in diet 13, produced quite different effects when fed; which suggests that it would not be justifiable to apply these readings for interpreting data presented by other workers using another sample of corn or wheat. It should be noted particularly in Figure 6 that the phosphorus of the blood cells was exceedingly low in rats from Group 14 receiving the white flour and high in Groups 13 and 15, receiving the whole wheat and the bran and middlings mixture. The phosphorus of the cells of the groups receiving the fine siftings of feed corn has the highest level. The percentage change in inorganic phosphorus when bone chips were added to the blood serum will be discussed later.
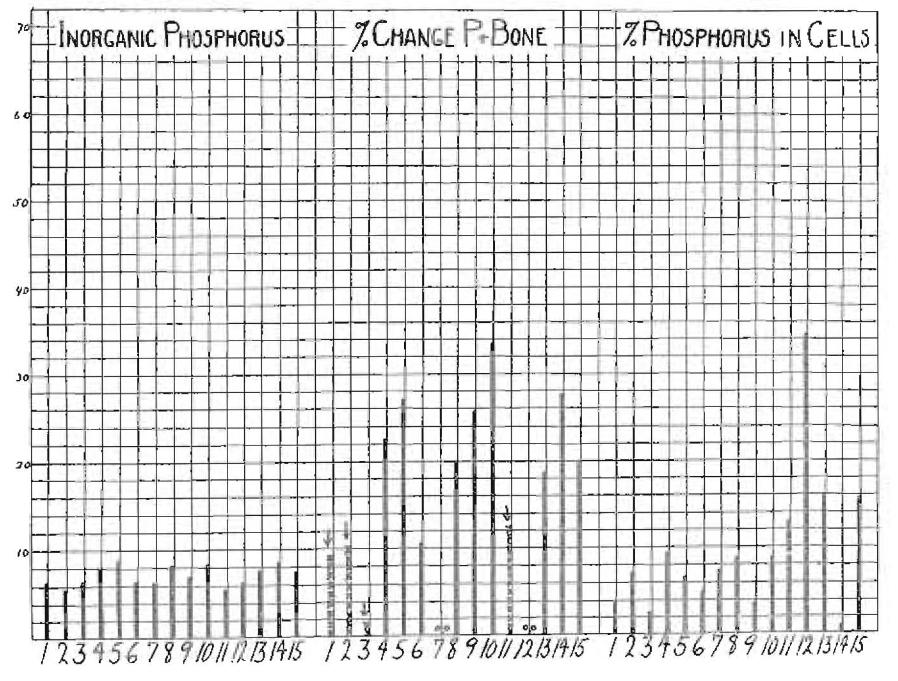
Fig. 6. Blood chemical changes on fifteen diets. Comparisons in three blood factors: inorganic phosphorus, percentage of change of phosphorus of serum plus bone and percentage of phosphorus in cells of rats fed on fifteen different diets. Crosses indicate a reverse direction of movement of phosphorus in the center group. The diets were: 1, fine and coarse whole feed corn; 2, fine feed corn; 3, coarse feed corn; 4, fine and coarse whole wheat; 5, No. 1 plus high vitamin butter; 7, No. 6 plus 10 per cent wheat germ; 8, No. 1 plus 10 per cent wheat germ; 9, No. 4 plus 10 per cent wheat germ; 10, No. 1 plus dicalcium phosphate; 11, coarse seed corn; 12, fine seed corn; 13. Red Cross fine and coarse whole wheat; 14, Red Cross flour; 15, Red Cross bran and middlings.
In Figure 7 will be seen a comparison of the levels of potassium, iron and total phosphorus for the different groups. It should be noted that the comparison of the level of potassium with that of iron and of phosphorus in this chart requires the explanation that the potassium columns are one-third their proper height as shown because of the large amount of potassium in comparison with other minerals. This does not change the significance of a comparison of the potassium in the blood of each of the fifteen groups of rats, which shows a difference of over 100 per cent between Group 4 and Group 12. There is also a marked difference in the level of the iron and total phosphorus in the blood of the different groups.
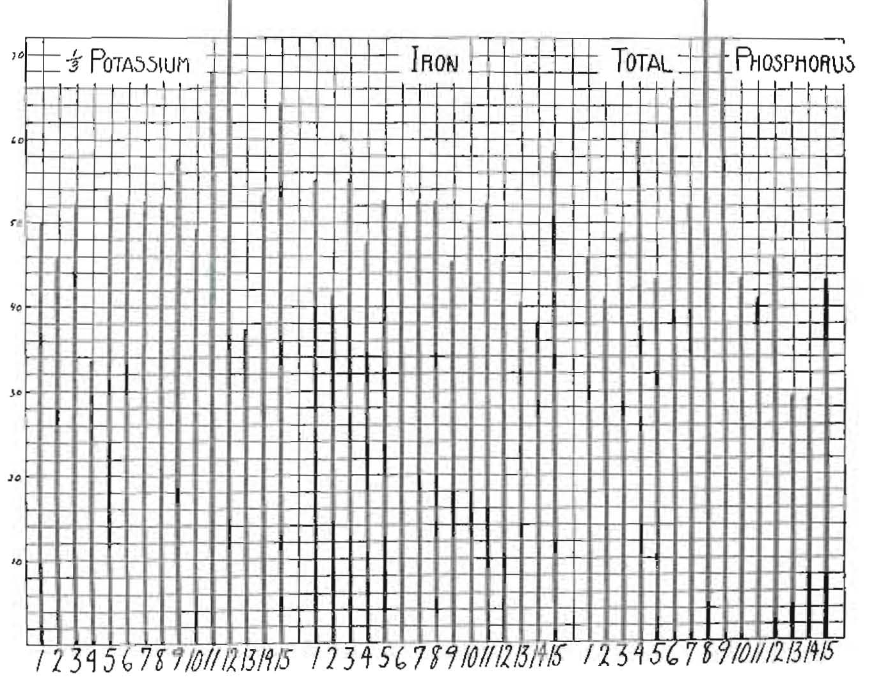
Fig. 7. Blood chemical changes on fifteen diets. Comparisons in three blood factors: potassium, iron and total phosphorus of rats fed on fifteen different diets: 1, fine and coarse feed corn; 2, fine feed corn; 3, coarse feed corn; 4, fine and coarse whole wheat; 5, No. 1 plus high vitamin butter; 6, No 1 plus 1 per cent each cod liver oil and high vitamin butter; 7, No. 6 plus 10 per cent wheat germ; 8, No. 1 plus 10 per cent wheat germ; 9, No. 4 plus 10 per cent wheat germ; 10, No. 1 plus dicalcium phosphate; 11, coarse seed corn; 12, fine seed corn; 13, Red Cross fine and coarse whole wheat; 14, Red Cross flour; 15, Red Cross bran and middlings.
In Figure 8 will be seen a comparison of the cell volume, the hemoglobin and the gain in weight of the different groups. As already stated, the rats in the last five groups, namely, 11, 12, 13, 14 and 15, were younger than those in the first ten groups and show a more rapid growth than those in the first ten groups. The rate of growth progressively lessens with increasing age. The greatest gain in weight occurred in the rats receiving whole wheat in the second series, and the lowest gain in weight in the first series in the rats receiving fine feed corn. It is important to observe that the two different grades of wheat used in Groups 4 and 13 produced very different growth characteristics. The hemoglobin of the blood shows a marked variation in different groups and will be seen to vary in almost exact relation to the iron of the feed as shown in Figure 2. I have previously shown that in Groups 13, 14, and 15, the iron of the bloods was in direct proportion to the iron in the food of the different groups.
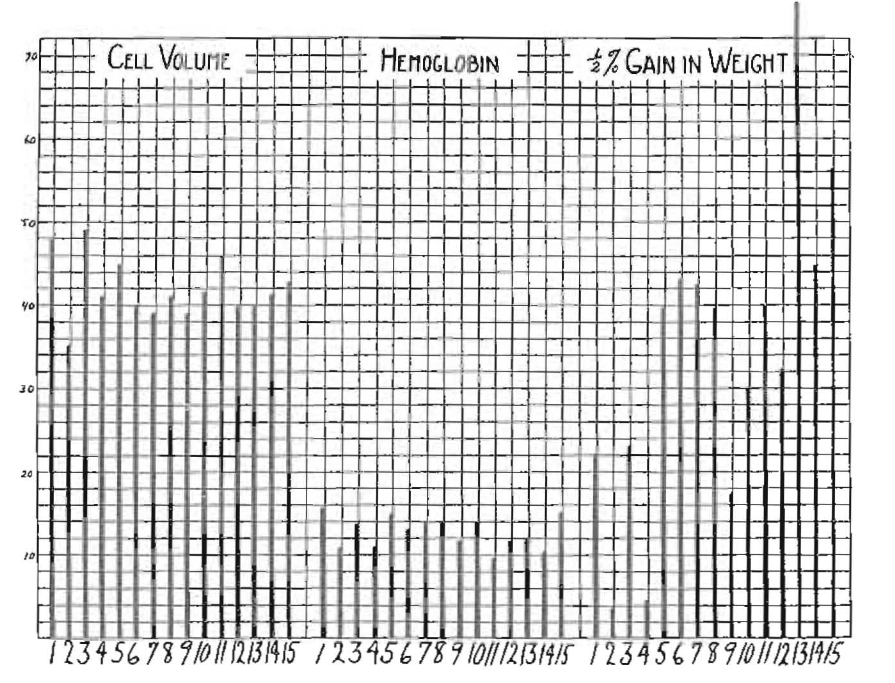
Fig. 8. Blood chemical changes on fifteen diets. Comparisons in two blood factors, cell volume and hemoglobin, and gain in weight of rats fed on fifteen different diets: 1, fine and coarse feed corn; 2, fine feed corn; 3, coarse feed corn; 4, fine and coarse whole wheat; 5, No. 1 plus high vitamin butter; 6, No. 1 plus 1 per cent of each cod liver oil and high vitamin butter; 7, No. 6 plus 10 per cent wheat germ; 8, No. 1 plus 10 per cent wheat germ; 9, No. 4 plus 10 per cent wheat germ; 10, No. 1 plus dicalcium phosphate; 11, coarse seed corn; 12, fine feed corn; 13, Red Cross fine and coarse whole wheat; 14, Red Cross flour; 15, Red Cross bran and middlings.
An important phase of this study of the effect of fifteen different diets on the groups of rats has related to the incidence of dental caries. It is difficult to compare the data provided by different workers, chiefly because of different procedures of study. The results that are shown in Figure 9 represent cavities per rat. When staining methods and histologic sections are used, the microscope will reveal structural changes in very minute proportions, which cannot be observed or estimated by less exacting procedures. I am not reporting the data obtained with the assistance of the high magnification microscope. Cavities that were sufficiently large to be seen with the naked eye or with the low power of the microscope are indicated by the column. The number of cavities per rat which had entered into the pulp chambers is indicated by a cross line with a letter P. It will at once be seen that there is a marked difference in the number of cavities produced in the rats on these different diets, and it is of particular interest that the data produced by these studies have not developed the same proportion of cavities whether in the groups eating coarse corn or in those eating fine corn, as reported by Hoppert, Webber and Canniff. The significance of these data will be discussed presently. It is important to note that Groups 4, 5, 6, 9 and 15 had no caries and Group 13 almost complete immunity. The role of the activators in conjunction with the mineral-carrying foods is strikingly indicated in Groups 5 and 6.
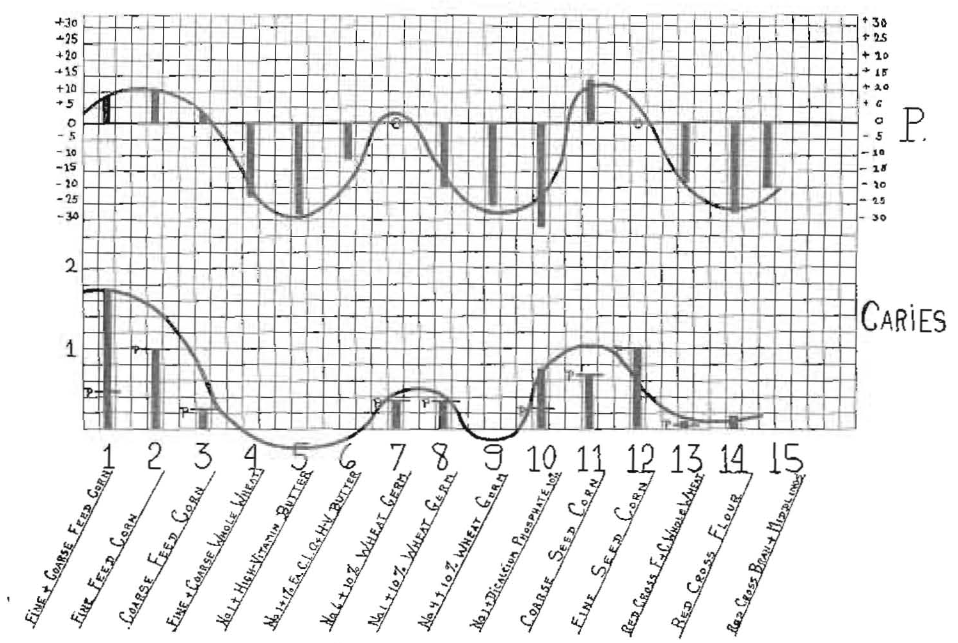
Fig. 9. Dental caries in rats on fifteen diets (below); solubility factor of blood for phosphorus (above). The inorganic phosphorus of the blood serum of normal animals moves to bone chips. The tendency to follow the incidence of caries is shown below for the different diets.
3. Structural Changes Produced in Human Teeth by Reinforcement of the Diet.–If dental caries is fundamentally controlled in its major aspect by physicochemical factors of the saliva, which, in turn, are controlled by nutrition, it should be possible to produce changes in caries cavities, even after they have been established, by nutritional means. In Figure 10 will be seen two teeth, both deciduous molars. The one to the left was removed from a child with active dental caries, without treatment. After extraction, the tooth was immersed in a 10 per cent solution of silver nitrate for several hours, then placed in sunlight. The ground surface reveals that the soft caries portion has been completely saturated with silver nitrate. Other parts of the tooth have not been penetrated, except a small proximal area of caries on the opposite contract. The tooth to the right shows a similar tooth which was left in the mouth during twelve weeks of treatment, being a tooth from one of the children of the Broadway Mission group. This tooth was treated similarly to the one at the left, and it is important to note that the silver nitrate had not penetrated the carious structure much more than the enamel surfaces of the tooth. To the point of a sharp instrument such as an explorer, this surface was glassy hard. It is routine practice to leave many such teeth unfilled for critical examination. The result shown in this tooth is typical of large numbers so examined.

Fig. 10. Left: Tooth showing silver nitrate saturated to depth of carious dentin; from a patient without treatment. Right: Tooth showing caries controlled. The silver nitrate has not been able to penetrate much if any farther than into the enamel surface of the tooth.
An opportunity for a more severe test is provided in teeth where the decalcification of large occlusal and proximal cavities has reached the pulp, and where it would be expected that toxic material, if not actual bacterial invasion, had already entered into the pulp tissue. Such a case in which a large area of dentin over the pulp had been decalcified is shown in Figure 11. Without removal of the carious dentin, a temporary cement filling was placed in the cavity to prevent pressure and packing of foods The patient was one of the Broadway Mission group receiving one reinforced meal a day. The condition at the beginning is shown to the left, and on the right is seen the result after about twelve weeks on the reinforced diet. The coronal aspect of the pulp has now been protected by a deep layer of newly laid down dentin. The exposed pulp is no longer exposed. Of twelve teeth with far advanced dental caries apparently involving the pulp as in the case here presented, two became abscessed and ten showed marked structural change by building in of dentin in the pulp chamber to provide a protecting wall. In some cases the teeth were purposely left without fillings and the caries did not proceed with a breakdown of the pulp tissue.

Fig. 11. Control of dental caries under nutritional treatment with building in of new pulpal wall
4. Results of Field Studies of Districts Showing Immunity and Districts Showing Susceptibility to Dental Caries, Including Chemical Analyses of Saliva.–An explanation of the phenomena of dental caries, to be adequate, must stand testing by application to areas of immunity and areas of susceptibility. Areas in which the people will generally be found to have lost their immunity are very numerous and very easy to find; not so with areas of immunity.
I have reported efforts made last year to find groups with immunity in the high Alps of Switzerland and particularly one large group with a high level of immunity. Accordingly, much effort has been expended during this summer of 1932 in search of groups with high immunity living under quite exacting conditions, where the controlling factors would be relatively similar for large groups. Extended correspondence relative to different countries led to the decision in favor of Switzerland and the Inner and Outer Hebrides as important fields for this study. In all, about twenty different districts were studied in most of which, in addition to a detailed and clinical study of the mouth and living habits, a sample of saliva was obtained, cultures were made of the flora with special consideration of the acidophilic group and the bacterial growth of the saliva was controlled by the addition of formalin. One hundred and seventy-one samples of saliva were forwarded or brought by me to my laboratories for chemical analysis and arrangements were made for study of other samples in provided containers. In all about forty items of information were obtained for each patient. In addition, twenty chemical factors were provided in the salivary analysis.
The first place studied this summer was the Loetschental Valley, which has an altitude of from 4,000 to 6,000 feet for different parts of the principally occupied valley. These people have had a forced isolation owing to the high snow-capped mountain ranges surrounding the valley, with the only entrance a dangerous one owing to the presence of treacherous avalanches in the narrow gorge. Recently, the opening of the Lotschberg tunnel, the second longest in Europe, made a doorway for these people to the outer world, and also permitting the accompaniments of modern civilization to have access to the valley. Even since last year, I have found evidence of modernization both in dress and in foods available. A modern white flour bakery, built within the year, is rapidly influencing the dietary. Compared with most communities, they still have high immunity to dental caries.
This valley has four principal villages connected by a footpath on which the post mules carry the government mails. The transportation of the valley is largely by human beings. All of the farming and local industrial work is done by human power. Sojourns were made to other districts for carrying forward the clinical examinations and obtaining saliva samples for chemical analysis. Studies were also made in districts in the lower plains country of Switzerland. Switzerland, an inland country, provided a different environment from that near the sea. I, therefore, also made studies in the Inner and Outer Hebrides, north Scotland, Wales and England.
A group of nine places in which the incidence of dental caries was very low are shown in Figure 12 (below, left). To the right are shown seven places where the incidence of dental caries was very high. In both groups are included places representing characteristic types of environment with regard to altitude and climatic conditions. For each place, three factors in dental caries are shown graphically by the columns. The first column from the left represents the percentage of teeth that have been involved by dental caries during the individual’s entire lifetime as far as could be determined by either the presence of cavities or fillings or missing teeth in the case of young people, or where the history of the patient, if older, could decide one that the tooth had been lost by caries. The second column for each place represents the percentage of people who do not have a history of complete immunity from dental caries for their lifetime, which I will refer to as “total individual susceptibility.” The third column represents the percentage of individuals who, at the time of the examination, were free from active dental caries, which I have referred to as “present susceptibility.” The first two towns or villages, Ferdon and Kippel, are in the lower part of the Loetschental Valley nearest to the tunnel and railroad station and have an altitude of about 4,000 feet. The second group, Wiler and Blatten, having an altitude of about 5,000 feet, are farther up the valley nearer to the glaciers. Ayer, with an altitude of 4,800 feet, is in the upper part of the Anniviers Valley, and Grachen, with an altitude of 5,000 feet, is on the mountain side well toward the glacier in the Natervisp Valley. Vispertiminen is high up the mountain side in the Visp Valley. Vissoie is in the Anniviers Valley, 5 miles down the valley from Ayer. Zinal is in the same valley as Vissoie. Zinal is populated in the summer by families from Vissoie. St. Moritz, the famous winter and summer health resort, is in the Oberengadin Valley and is among the streams forming the headwaters of the Danube. Herisau is in the rolling low country of Switzerland near Lake Constance. Lewis is the most northerly island of the Outer Hebrides off the northwest coast of Scotland. Tarbert is the principal port of call for boats in the Isle of Harris. Scalpay is in the Isle of Harris south of the Lewis Island. Airth of Sleat is on the island of Skye. Bardsey is an island off the west coast of Wales. In Figure 12, these are shown in the two general groups marked “low caries districts” and “high caries districts,” respectively. In the former, 4,080 teeth were examined, of which only 145 had ever been attacked by caries, an incidence of 3.4 per cent on the basis of the number of teeth. In the “high caries districts,” 2,063 teeth were examined, of which 516 were attacked by caries, or 25.5 per cent. An effort was made to obtain groups as nearly typical and comparable as possible. For this reason, this study was largely limited to children under 15 years, in whom the stress period of natural growth would be common.
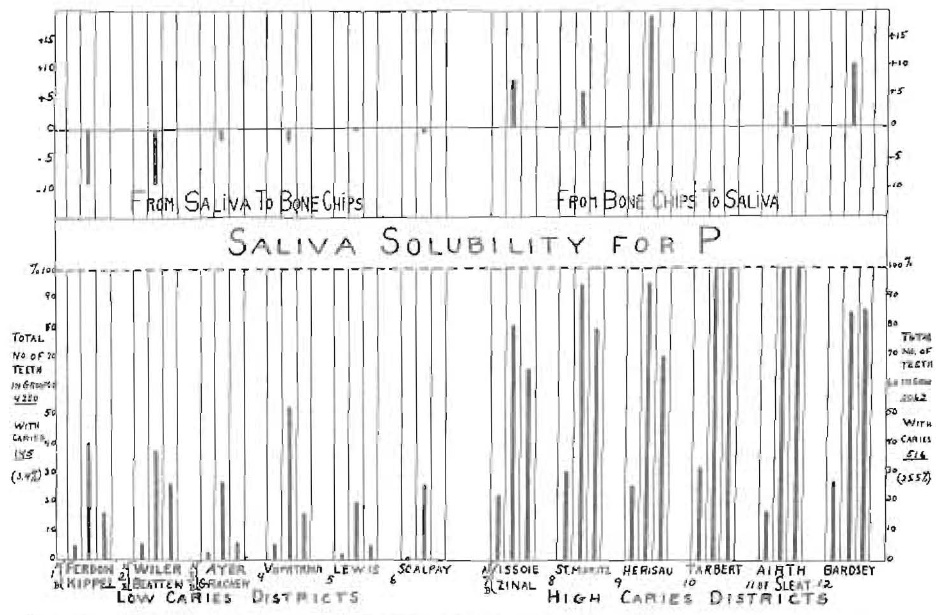
Fig. 12. Results of field studies both in districts showing immunity and in those showing loss of immunity to dental caries. Above is shown the behavior of the serum inorganic phosphorus, which moves in the normal direction in groups with low caries incidence and in the wrong direction in the groups with a high incidence.
In Group 1, Ferden and Kippel, in every hundred teeth examined, an average of only 4.8 were found to have been attacked by dental caries (shown in the column to the left). In Group 2, Wiler and Blatten, the average was 5.9, in Group 3, Ayer and Gracken, it was 2.3, and in Group 4, Visperterminen, it was 5.2. In the Isle of Lewis area, Group 5, the average was 1.3, and for the Scalpay group number 6, it was 1.0. The general average for the “low caries districts” was 3.4. In the “high caries districts,” the percentage of teeth attacked by caries is in Group 7, Vissoie and Zinal, an average of 22.0 per cent; in Group 8, St. Moritz, an average of 29.8 per cent; in Group 9, Herisau, an average of 24.7 per cent; in Group 10, Tarbert, an average of 32.4 per cent; in Group 11, Airth of Sleat, an average of 16.4 per cent, and in Group 12, Bardsey, an average of 27.6 per cent. The general average in this “high caries group” was 25.5 per cent.
The middle column in each group represents “total individual susceptibility”; that is, the percentage of individuals who did not have a perfect history of immunity as indicated by either teeth with caries, filled teeth or missing teeth. For Group 1, this was 40.4 per cent; Group 2, 37.8 per cent; Group 3, 26.6 per cent; Group 4, 35.0 per cent; Group 5, 19.0 per cent; and Group 6, 35.5 per cent; an average for this group of 32.2 per cent. For the “high caries district,” this factor was in Group 7, 90.0 per cent; Group 8, 95.8 per cent; Group 9, 96.0 per cent; Group 10, 100 per cent; Group 11, 100 per cent; Group 12, 84.6 per cent; an average for this group of 94.4 per cent.
The third column in each of the groups of three factors indicates the “present susceptibility” to dental caries. This was determined by the absence of active caries. For Group 1, this factor was 17.0 per cent; Group 2, 27.0 per cent; Group 3, 6.6 per cent; Group 4, 16.2 per cent; Group 5, 5.0 per cent; and Group 6, 0.0 per cent; that is, no teeth with active caries were found in this last group. The average for the series was 11.9 per cent. In the districts with high dental caries, the figures were: Group 7, 66.0 per cent; Group 8, 78.9 per cent; Group 9, 68 per cent; Group 10, 100 per cent; Group 11, 100 per cent; and Group 12, 84.6 per cent. The average for the series was 82.9 per cent.
An important phase of the special field studies conducted the summer of 1932 has included the securing of samples of saliva for chemical analysis. For this, 171 specimens were shipped or carried to my laboratories for study. In most cases, cultures were made in a special medium in order to study the incidence of the acidophilic organisms. This bacterial phase will be discussed later. Among the factors determined are total calcium, inorganic phosphorus, total phosphorus, solubility of the saliva for calcium, solubility for phosphorus and the ratio of calcium to inorganic phosphorus. The factor with which we are primarily concerned in this discussion is the behavior of the salivas when powdered bone chips are added to them. This is shown for inorganic phosphorus in Figure 12, above. In this connection it should be noted that while summer conditions in many districts on the whole are more favorable than winter, in some other districts they are distinctly less favorable. There are reasons that conditions were distinctly unfavorable at the time the saliva samples were taken. In high Alpine Valleys where they are dependent on dairy products as one of two principal sources of nutrition, they may suffer shortage because, in the summer, the dairy cows, and in some places also the goats, are sent to the high ranges to permit the harvesting to be done without their presence in the community (which is largely without fences), and, further, to permit the animals to have the advantage of the superior qualities of pasturing near the snow line; in other words, on the rapidly growing young plant life, which is in a very clear atmosphere, rich in ultraviolet rays, the conditions being responsible for the characteristic abundance and brilliancy of the flora of those regions. These valuable nutritive factors are placed in the milk by the cows. The milk in turn is made into cheese containing all the butter-fat and this cheese is stored for winter use. In the absence of the cows in summer, the nutrition of the children is greatly handicapped. Favorable results are obtained in spite of this disadvantage relating to the time the saliva samples were taken.
I have presented data indicating that the condition of immunity to dental caries is associated with physicochemical states of the saliva in which the inorganic phosphorus of the saliva passes from the saliva to the bone chips and that, in the condition of loss of immunity to dental caries, the movement is in the opposite direction; namely, from the bone chips to the saliva. One of the purposes of the different expeditions this summer was to obtain samples of saliva for checking these factors. To the left in Figure 12 are shown six groups with high immunity to dental caries, only 3.4 per cent of the teeth being affected in these six districts. Above is indicated the movement of the inorganic phosphorus in the saliva samples obtained as representative of these groups and all are shown to move downward in the direction indicating a movement out of the saliva to the bone chips. In the six groups on the right, in which 25 per cent of all the teeth studied were now carious or had been so, the movement of the inorganic phosphorus is shown to be upward in the opposite direction; namely, from the bone chips to the saliva. At the time of this dictation, the chemical analysis of these saliva samples is still in progress and a further report will be presented later dealing with the behavior of the calcium and other chemical factors.
While it is impractical to make estimations on the saliva chemical factors of the rats, a study of their blood has afforded important data as presented in Figures 4, 5, 6, 7 and 8. In Figure 10, the incidence of dental caries in the rats of the different groups has been shown on the basis of the average number of cavities per rat in each group. These show highest incidence in Groups 1, 2, 3, 7, 8, 10, 11 and 12. If reference will now be made to Figure 6, showing the percentage change of inorganic phosphorus plus bone, it will be observed that, in Group 1, 2 and 3, the inorganic phosphorus of the blood moved in the wrong direction, namely from the bone chips to the blood serum, as indicated by the crosses instead of the solid lines. In Group 7, this factor was reduced to zero. In Group 11, it was also in reverse phase, and in Group 12, reduced to zero. For those who are concerned with the changes in the blood which are likely to be responsible for the changes in the saliva, this will doubtless be significant.
An important phase of the collection of data this summer included the making of a record of the principal factors of nutrition in the various localities, the form in which the food was eaten, the obtaining of samples for chemical analysis and the ascertaining as nearly as possible of the percentage of certain foods used in the diet. Since cereals are, in all of these places, found to be an important factor, the particular cereals used and the form in which they were used were given detailed attention. One of the principal differences in the form in which cereals were used consisted of the method of preparation. In some districts studied, the cereals were made into porridges and breadstuffs from powdered whole grains. In some of these, small quantities of modified grain meals were in use, this usage extending to white flour and even bleached white flour. In some districts, practically all white flour was used. The proportion of these two for each place was studied and data were recorded. When the individuals for all the groups are arranged in progressive order on the basis of the ratio of white grain breads and its dilution with white flour to 100 per cent white flour, and with the incidence of dental caries plotted with these percentages, we have the information revealed in Figure 13. It will be seen that in the individuals, regardless of the group and regardless of the other factors entering into the nutrition, but who were using all the minerals of the grain, the number of cavities as shown at the left was 0.3 cavity per person. When this whole grain bread was diluted with 25 per cent white flour, the cavities increased to 1.5 cavities per person. With the use of 50 per cent each of whole grain breads and white flour breads, the data reveal that there were about 2.3 cavities per person. With further increases in the proportion of white flour, the curve of incidence of dental caries goes up more rapidly, so that at 75 per cent white flour, there were 5.3 cavities per person, and with 100 per cent white flour breads, the data revealed seven cavities per person. When we use the data obtained by an analysis of a number of whole wheats and flours, we should find the phosphorus factor of the cereal at about 0.9 per cent in the whole grain breads and about 0.2 per cent in the white flour products. If we use the data provided in the table in Figure 2, we find that these figures are about 0.97 for the whole grain meal and 0.16 for white flour. The latter curve is shown in the continuous line. The phosphorus content of the different cereals and products is shown at the left.
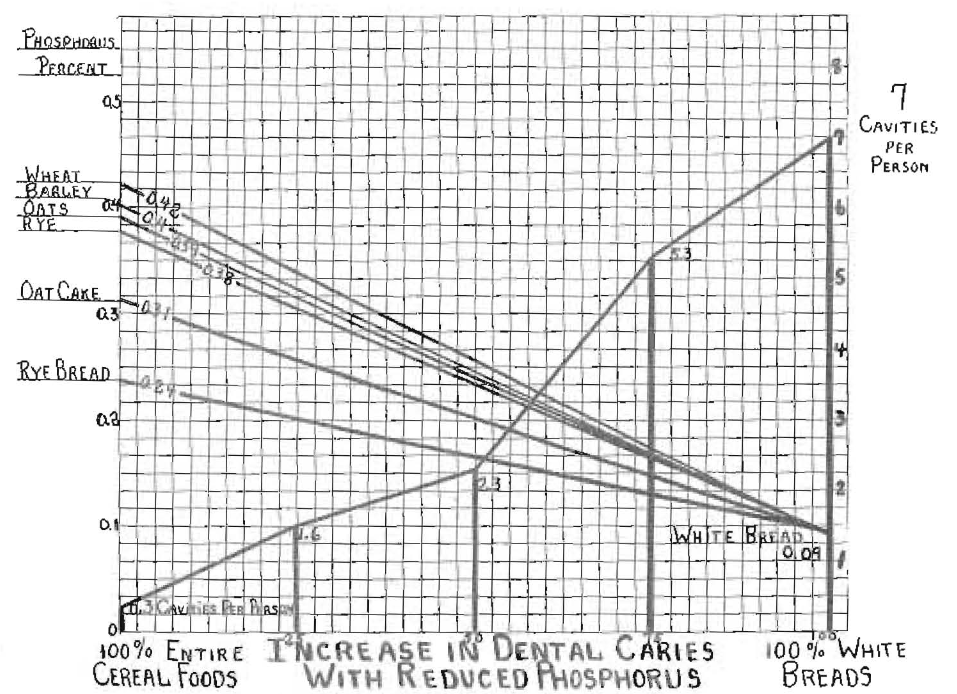
Fig. 13. Incidence of caries in relation to mineral content of one important food.
Even without the data obtained from a quite detailed study of the diets of the people living in districts of immunity and of susceptibility, it becomes possible to interpret the factors in these phenomena. Since body building and repair require an adequate amount of foods to be ingested which carry with them minerals and other chemicals including the activators, sufficient to meet the body’s demands, and since Nature has constructed seeds of plants so that they provide these various factors, any nutritional program which seriously modifies these balances becomes deficient. This relates equally to minerals and activators, including the known vitamins. When the individuals in the high valleys, which formerly provided immunity, were satisfying all of their hunger demands for various stages and conditions of life by eating foods very high in both minerals and activators, conditions were provided for both good growth and a good defense, against natural or unnatural overloads. Where less efficient foods are provided such as prevail in modern procedures of preparing and selecting foodstuffs, the factor of safety is so greatly reduced that these people living under primitive conditions rapidly change physically, and dental caries and other degenerative processes develop. Specifically, the change in the nature of the cereal factor of their foodstuffs, the total quantity of dairy products eaten and the reduction of the butter-fat intake in each of the general regions studied have apparently been largely responsible for the change from immunity to susceptibility to dental caries, and this handicap has not been compensated for by the increase in the variety of foods, including marked increase in the availability of fruits and vegetables. In the districts where immunity to dental caries existed not only for the present generation examined, but also for preceding centuries, there was also a marked absence of irregularity of the teeth. On the contrary, those areas with high susceptibility, or with even recently acquired loss of immunity, showed much deformity of the arches and irregularity of the teeth, expressing itself in even a single generation and indicating that the stress existed all through the developmental and growth periods.
Comment
An interpretation of the various factors in order that they may be applied to the districts in which field studies were made requires that some further data be in mind. In the high Alpine valleys, rye constitutes the principal locally produced cereal. Usually, the only other grain that is grown is barley, and it is very limited in use in comparison with the rye. In the Outer Hebrides, practically no rye or wheat is locally produced, the locally grown cereal being very largely oats with a small amount of barley. Wheat does not readily ripen in either of the above mentioned places. In the Island of Bardsey, wheat is grown easily, as are also rye and oats. Corn was not an important factor of diet in any of the communities included in this study. Where wheat was imported, it was very largely imported as white flour. It is also important to note that white flour was available in every place where transportation facilities made its shipment easily possible. The only areas found where white flour was not easily available either as flour or as white bread and white flour products were places where it could not readily be delivered. It was frequently possible to go from an area of very high immunity to dental caries to one of very low immunity in one hour or, at the most in a few hours. In Switzerland this usually meant climbing down from a place of difficult access to one more accessible.
The geographic positions of the places studied are presented in Figure 14, the white pins indicating places from which I have been receiving butter samples during the past year, usually every two weeks, for analysis of the vitamin levels. The black pins indicate the districts in Switzerland which were studied last summer. In order to check the role of altitude, since the districts of immunity were all found from about 4,000 to about 6,000 feet, care was taken to study places with comparable conditions. It is of interest that Ferdon, Kippel, Wiler, Blatten, Ayer, Gretchen and Vispertiminen, which were places with high immunity or a low incidence of dental caries, are all situated in high districts in the Alps. In none of these places did we find evidence of a program of prophylaxis or any evidence of oral hygiene. Indeed, it is doubtful that many of the people studied in these districts even owned or ever saw a toothbrush. St Moritz represents a comparable climate and altitude to all of the places just mentioned. Its fame is world wide as a health resort, both winter and summer. Every child studied in St. Moritz showed evidence of an efficient program of prophylaxis and all had been taught oral hygiene in the public schools, yet almost every child had suffered severely from dental caries at some time and 78.9 per cent had active dental caries at the time of the examination. Examination revealed that 29.8 per cent of all teeth had been attacked by dental caries. This, of course, occurred in spite of an excellent prophylactic program. Similarly, isolated districts in the Isle of Lewis, in The Outer Hebrides, and in Kyle of Scalpay in the Isle of Harris are shown to have a very low incidence of dental caries. These are at sea level. There was little if any evidence that oral hygiene had ever been taught or practiced. The locations of the places studied in the Outer and Inner Hebrides and other parts of the British Isles are shown in Figure 15, by the dark pins.
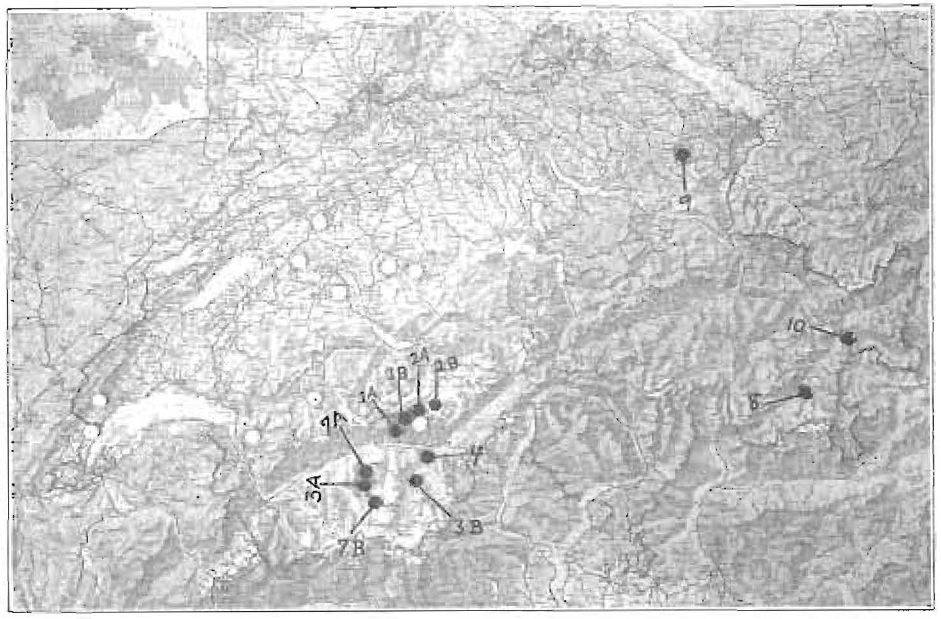
Fig. 14. Districts in Switzerland where special field studies were made of the incidence of dental caries: 1a, Ferdon; 1b, Kippel; 2a, Wiler; 26, Blatten; 3a, Ayer; 3b, Grachen; 4, Visperterminen; 7a, Vissoie; 7b, Ziral; &, St. Moritz; 9, Herisau. Butter samples have been received regularly from the places indicated by white dots.
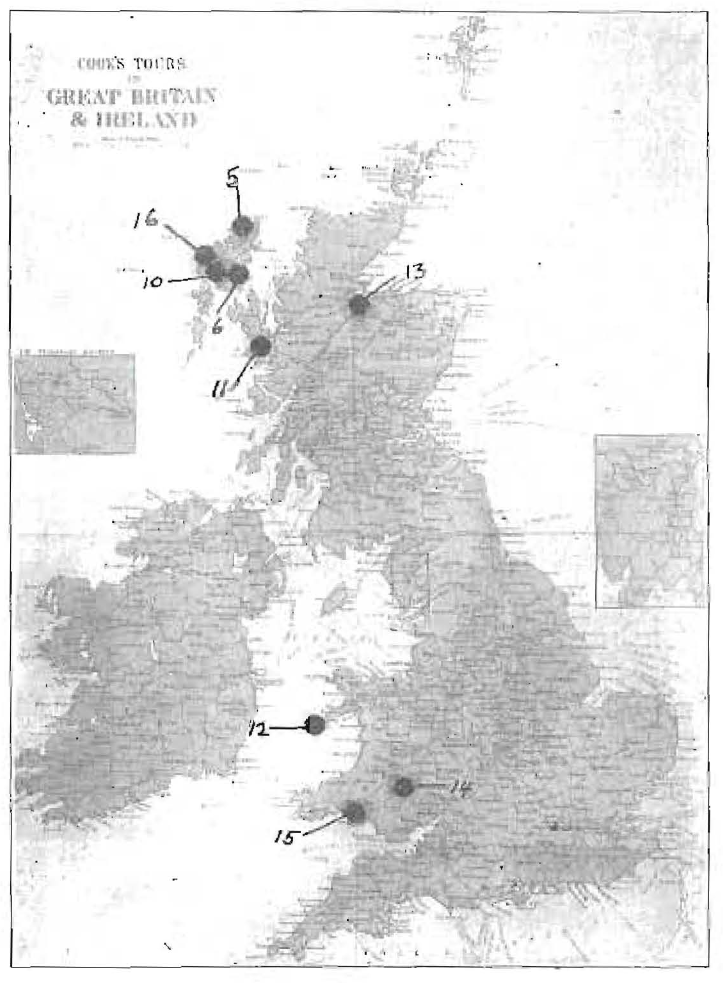
Fig. 15. Districts in the British Isles where special field studies were made of incidence of dental caries: 5, Lewis; 6, Kyle of Scalpay; 10, Tarbert; 11, Airth of Sleat; 12, Bardsey.
As we proceeded in Switzerland to Herisau, a thriving modern city in the plains district near Lake Constance in the northeastern part of Switzerland, we again found boys and girls with much evidence of home care and careful teaching in methods of oral hygiene; yet 24.7 per cent of all teeth showed caries; 89 per cent of individuals had had dental caries, and 68 per cent had active dental caries at the time of the examination. This is most significant as a commentary on the inefficiency of prophylaxis as a means of control of dental caries.
The data here presented relative to the kind and form of cereals used indicate strongly that it does not matter so much what the kind of cereal used or the form in which it is used, provided all of the natural mineral content of that cereal is made available. This is also emphasized in the group of studies presented under “Results from Feeding Fifteen Different Diets to Fifteen Groups of Rats.” The question of the form of the units of food that are taken, whether soft or hard, coarse or fine, does not seem to have been the determining facIn the series obtaining the whole corn, there was a higher percentage of cavities than in either of those groups receiving the fine or coarse corn. Those receiving the fine corn had more cavities than those receiving coarse corn. This is not in accordance with the data presented by Hoppert, Webber and Canniff. I would emphasize that the fine feed corn group (2) and the fine seed corn group (12) each had more cavities than the coarse feed corn group (3) and the coarse seed corn group (11). Since none of these had so many cavities as Group 1, receiving both the fine and coarse corn, though all had liberal caries, it is suggested that we should not put too much emphasis on the coarseness or fineness of the food.
It is important to note, particularly for those who would put great emphasis on the hardness of the food eaten as a means of muscular exertion for the development of the bones of the face, that the people living in the high Alpine districts that were found to have a high immunity to dental caries were eating a hard bread usually weeks old, sometimes several months old and dried out until it required much effort for its mastication, while the people in the Outer Hebrides who also were found to have high immunity to dental caries were using a large part of their cereal in the form of soft porridge. True, the oat cake is crisp, but it is thin and relatively more easily masticated than the Swiss dark whole grain bread. The evidence does not support the view that the texture of the food is a determining factor.
The matter of the availability of the various vitamins has been studied and further data will later be presented. Some factors can be determined readily from a study of local conditions. In none of the immune districts included in this study were citrus fruits available. Many of the immune individuals in both the high Alpine valleys and the interior of the Isle of Lewis have probably never eaten an orange or grapefruit and in neither district were wild berries provided as a native food. Some citrus fruits come into Switzerland from Italy and Spain, but they reach only communities provided with adequate means of transportation. No district was found with immunity where imported fruits were available. This would seem at once to exclude the possibility of vitamin C being a controlling factor in these districts. The inhabitants of Vispertiminen had vineyards down the mountainside. Since there are many places where immunity to dental caries existed a few years ago and where that immunity has been lost coincidentally with the opening up of means of easy transportation of foodstuffs, it has not, of course, been the introduction of citrus fruits to formerly immune areas which has contributed to the loss of immunity. It is also significant that in no place was immunity to dental caries found where there was not a bountiful source of fat-soluble vitamins in a natural food product, which my investigations have demonstrated to constitute a principal controlling factor in dental caries in many individuals and in many districts. For the Inner and Outer Hebrides, fish products are available and are used liberally. A particularly favored dish in the Isle of Lewis consisted of cod’s head stuffed with a mixture of oat meal and chopped cod livers and baked. Heads with large muscles were selected and the brains left in position. This would furnish vitamin D and phosphorus besides the minerals in a readily available form. Of course, no fish were available for providing vitamins in the isolated high Alpine valleys. Probably many of those individuals have never seen a fish. Their source of fat soluble vitamins is primarily from the dairy products used as milk, cheese and butter. The cheese contains the full butter-fat. With the introduction of contact with the outside world by means of transportation, easy access is had to markets for dairy products. These markets are generally utilized as a means of obtaining ready money for the purchase of machine made clothing and canned foods and flour. In the Hebrides, the thatched roof that covers the family covers the cows and goats. The walls were built of stone and many of the homes were without windows and chimneys. The thatched roof has two purposes, protection from the weather and the preparing of a special fertilizer for the soil through the burning of the peat for most of the year. The few trees on the Isle of Lewis have been planted in chiefly one place, near the coast. The island is largely covered with peat from a few inches to 20 feet in depth, except for the areas covered with bald rocks. The geologic form is granite of the oldest type. The mineral calcium is very scarce. The plant that is seen most everywhere is purple heather, as is also true in much of north Scotland. About the only animals on the island are the domesticated black face sheep and a few highland cattle or mixed breeds of highland with others. These animals are very hardy and can live out through the winter. The little pasture grass that these animals can pick up enables them to collect the plant calcium and phosphorus and make these minerals available in the very limited dairy products which were part of the former primitive diet and still is for a few people living in a primitive manner. Eggs are also used. With the introduction of modern foods in condensed form and generally low in minerals, this important source of nutrition is rapidly dwindling in the districts having contact with commerce, with the result that passing from an immune area to the principal seaport of Stornoway, out of 100 people between the ages of 16 and 35 (estimated), there were found twenty-five wearing artificial teeth, and about an equal number showed that they had lost many teeth or parts of them from caries. All the people speak the same language, Gaelic. Some of them speak English. The breakdown was so rapid and clear cut that people from 50 to 80 years of age still had most or all of their teeth without evidence of active caries. These people were insisting on having their original diet. The younger generation which had access to the modern diet had rampant dental caries. In some districts, 60 per cent of the people between 20 and 60 years of age were wearing artificial dentures, often both upper and lower. This condition of increase of dental caries was reported in many districts as being progressively more severe. An analysis of these diets and of living conditions will be presented in another communication.
In further consideration of the role of activating substances, including the known vitamins, important data are provided in Figure 9. In this, fifteen diets were used, with the same basic ration for all, the modification being chiefly in the kind or form of the cereal factor. A glance at the chart reveals at once that dental caries was particularly high in Groups 1 and 2, moderate in Group 3 and completely absent in Group 4, who received wheat instead of corn; also absent in Group 5, who received fine and coarse feed corn as provided to Group 1 plus all they wished to eat of high vitamin butter. In Group 6, receiving the same as Group 1 plus 1 per cent high vitamin butter and 1 per cent high vitamin cod liver oil, there were no gross cavities but several small ones. In group 7 receiving the same as Group 6 plus wheat germ, there were moderate carious cavities. In Group 8, receiving the diet of Group 1 plus wheat germ, there was moderate caries. In Group 9, receiving the wheat of Group 4 plus wheat germ, there was no caries. In Group 10 receiving the diet of Group 1 plus dicalcium phosphate in an inorganic form, there was considerable caries. In Group 11, receiving coarse siftings of a seed corn differing from that employed in Group 1 only in kind of corn, there was considerable caries. Group 12, receiving the diet of Group 1 plus the fine siftings of seed corn, had very active caries. Group 13, receiving the Red Cross whole wheat, had no caries; while those in Group 14, on Red Cross four, had much caries. This group received not only less minerals but also less of the activators that would have been provided in the wheat embryo. Group 15, receiving the Red Cross bran and middlings mixture, had no caries. It is at once seen that something was provided in the butter that was made available with the diet in Group 5, which otherwise corresponded with Group 1, and which was capable of changing that diet so that it provided complete immunity to dental caries. The very small amount of butter and cod liver oil furnished to Group 6 reduced caries to a very low level. That the activators provided in wheat germ are more efficient when used to supplement wheat rather than to supplement corn is suggested by the complete immunity of Group 9 as compared with Group 8.
An important new light on the relation of the phosphorus of the blood to dental caries susceptibility and immunity is provided by shaking powdered bone into the blood serum and noting the change it produces in the level of inorganic phosphorus, which is shown in Figure 9 to follow the caries susceptibility for these different groups.
If we review the summaries of accumulated facts as provided by Arthur D. Black2 and Robert Kesel,3 we note that the evidence stresses the necessity that caries shall begin on the outer surface of the tooth, and then usually only in protected areas, never involving deeper structures until the external surfaces had been penetrated, and that it is initiated and accompanied by a decalcifying process in which acid-producing microorganisms seem to have a part. These phenomena are apparently not related to acidity of saliva, but are related to its buffer capacity. All of these conditions could be provided by variation in physicochemical characteristics of the fluid bathing the external surfaces of the tooth, provided it could be shown that it contained forces which could progressively carry minerals in most minute form either into the tooth surface by absorption or out of the tooth surface in accordance with changes in that fluid. The information given here of an increase or decrease in the inorganic phosphorus of the saliva in accordance with whether that individual was found to show immunity or susceptibility to dental caries is presented in support of this premise. The data provided in the illustration of the teeth before and after treatment (Fig. 10) show the difference in the penetration of silver nitrate, and Figure 11 shows the actual building of new tooth structure when the blood and saliva are put in such condition that minerals are deposited rather than taken up. Many additional data are available on this point. That this change in the chemical aspect of the saliva can be produced by nutritional changes is supported by the evidence presented here and in former communications as reviewed in the introduction. When these interpretations are applied to the review of fundamentals as presented by Kesel, we find why both ancient and modern primitive people living in their native environment develop little decay. We find supporting evidence in these studies of districts of immunity or susceptibility. When we apply these principles to the phenomena associated with periods of physical stress, the active growth of childhood and adolescence, pregnancy and disease, we find much evidence that the need of the body for the minerals and activators with which body tissues are built and repaired incident to those overloads prevents the development of a normal saliva for the environment of the tooth. The reason that decay of teeth ceases even though the bacteria are still present, and even though culture mediums suitable for their needs are provided, now becomes apparent. We also see why crowns of teeth when mounted on artificial dentures and worn in the mouth can also be attacked by dental caries as though in their normal position. When we apply this view to the areas of susceptibility which have been indicated to be vulnerable areas owing to the collection of foreign material in any location where the saliva cannot, particularly when its factor of safety is low, maintain a margin of safety, because the physical environment prevents its ready access, we see why saliva with a low but positive factor of safety can maintain immunity on surfaces that are liberally exposed. This provides an explanation for the observation that small proximal cavities or caries under fillings may progress; whereas, if the cavity is opened so that saliva has free access, so long as its margin of safety, even though small, exists, caries is inhibited. In the protected areas, a very high state of defense in the saliva would have to be provided in order to maintain immunity. Further, when we consider the problem of the progressive softening of teeth in cases of rampant caries, as in pregnancy and some other conditions and later the hardening of these teeth, we find not only an adequate explanation, but also a physical condition which we have demonstrated on teeth removed from the mouth and which shows not only change in structure on the basis of hardness, but also a change in chemical content varying in amount and in chemical expression. In most cases, a greater reduction in phosphorus than in calcium occurs. In some cases, there is a reduction in calcium. In a later communication, these data will be presented and will be shown to have a direct relationship to the nutritional deficiency and also to the nature of the local expression in both the teeth and their supporting structures.
Summary and Conclusions
- Supporting data are presented for a new interpretation for the phenomena of dental caries based upon a physicochemical state of the saliva which provides and largely controls the immediate environment of the tooth.
- These new interpretations have been supported by data provided from the study of both experimental animals and human beings, the latter living under both primitive and modern social conditions.
- The specific requirements indicated by past investigations regarding the etiology of dental caries can be largely if not completely explained on the basis of these physicochemical qualities of the saliva.
- People living under modern conditions which provide either immunity or susceptibility reveal physicochemical conditions of the saliva apparently competent to create the clinical dental conditions found in those individuals.
- A new theory for the phenomena of dental caries has been provided supported by clinical data which furnish the basis for a program shown to be competent not only to prevent the development of dental caries but also to control it after it is established.
- Data are presented which provide an explanation not only for the general immunity of wild animals from dental caries but also for the immunity of primitive peoples, both ancient and modern.
- Light is thrown on many degenerative processes of both hard and soft tissues also resulting from the accumulated effects of faulty nutrition and means are indicated for the reduction of their severity and incidence.
Editor’s note: Since the era in which this article was written, society’s understanding of respectful terminology when referring to ethnic and cultural groups has evolved, and some readers may be offended by references to “primitive” people and other out-of-date terminology. However, this article has been archived as a historical document, and so we have chosen to use Price’s exact words in the interest of authenticity. No disrespect to any cultural or ethnic group is intended.
References Cited:
- Price, W. A.: “New Light on Etiology and Control of Dental Caries,” J. D. Res., abstr. 12:540 (June) 1932. “Experimental Basis for New Theory of Dental Caries with Chemical Procedures for Determining Immunity and Susceptibility,” D. Cosmos, 74:1139 (Dec.) 1932.
- Black, A. D.: “Future Practice of Operative Dentistry,” J.A.D.A., 19:1213-1221 (July) 1932.
- Kesel, Robert: “What Do We Know About Dental Caries? (A Critical Review of Recent Investigations),” J.A.D.A.. 19:908-917 (June) 1932.
- Hoppert, C. A.; Webber, P. A., and Canniff, T. L.: “Production of Dental Caries in Rats Fed Adequate Diet,” J. D. Res. 12: 161-173 (Feb.) 1932.
- Klein, Henry and McCollum, E. V.: Science, 74:662 (Dec. 25) 1931.
- Price, W. A.: “New Light on Some Relationships Between Soil Mineral Deficiencies, Low Vitamin Foods and Some Degenerative Diseases Including Dental Caries, with Practical Progress in Their Control,” Bull. Indiana D. Soc., September, 1932;
Footnote 1;
“Are Activators Revealing Nature of Life in Health and Disease Including Dental Disease?” Ohio D. J., August-November 1932;
“New Light on Cause and Prevention of Dental Caries and Other Degenerative Diseases,” Proc. Eighth Internat. D. Cong., Paris, 1931. - Price, W. A.: J.A.D A., 19:1339 (Aug.) 1932.
- Footnote 6, first reference.