
Access to all articles, new health classes, discounts in our store, and more!
Why Dental Caries With Modern Civilizations? VI. Practical Procedures for the Nutritional Control of Dental Caries
Published in The Dental Digest, August 1933, Volume 39, Number 8.
* * *
This was the sixth in a series of field studies by Dr. Weston A. Price that were published in The Dental Digest during the 1930s. This article appeared in the August 1933 issue (Volume 39, Number 8). Please see the editor’s note regarding language usage at the end of the article.
In the five preceding communications reports have been given of field studies conducted in Switzerland and the Outer Hebrides, which consisted of an interpretation of clinical and chemical data. In this communication data are given on the practical application of the information developed in these investigations of the problem of the control and prevention of dental caries and associated degenerative processes.
It is important that some of the general physical differences be observed in two groups, one reared on the kind of nutrition used by its ancestors, and the other reared on the nutrition provided by modern civilizations, which is almost universally attended by dental caries and often in severe form.
In Fig. 1 will be seen a group of girls and boys who live in the Kyle of Scalpay, Isle of Harris in the Outer Hebrides. Their nutrition has consisted largely of oat products and sea foods as previously outlined. Their physiques are excellent and they have a very high immunity to dental caries. The symmetry of the arches is relatively perfect, the nostrils broad and the middle third of the face is well developed in proportion to the remainder of the face. In this group only one tooth in each one hundred teeth examined has ever been attacked by dental caries. In the June installment of this series I compared the incidence of tooth decay in this group with those of Tarbert, about ten miles distance, in which 32.4 teeth out of every hundred examined had been attacked by tooth decay. Tarbert, it will be recalled, is a port with access to modern foods and has a modern bakery.
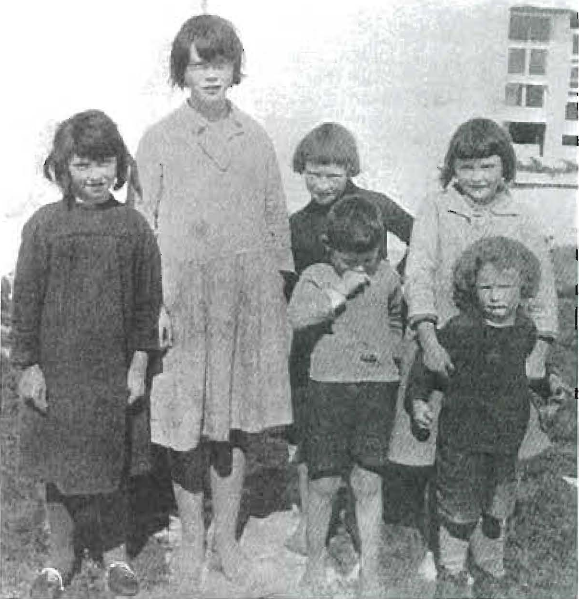
Fig. 1 – A group of children in the Outer Hebrides, reared on primitive foods. Note the splendid facial development. They have high immunity to dental caries.
In comparison with Fig. l one sees at once on studying Fig. 2 that in all of the children in this group of four photographed on the Island of Bardsey off the northwest coast of Wales, where they were living on modern foods and were suffering a definite and serious lack of development of the middle third of the face, tooth decay was rampant–27.6 teeth out of every hundred teeth examined among the growing boys and girls had already been attacked by caries. Even children 3 years of age were found with tooth decay. It will at once be seen that these children have already suffered a handicap that cannot be estimated nor can it be entirely overcome. All of these children are mouth breathers. This greatly increases the predisposition of infection of the air passages and to disease in general. All of these older children have rampant tooth decay and accordingly focal infection with its resulting suffering and injury. Irregularities of the teeth are common accompaniments to the type of facial deformity present in this group; mastication is also interfered with and accordingly digestion is disturbed. They are partly doomed before they have gone far on life’s journey since they cannot hope to compete with the physically fit. I have referred to the fact that this island was largely repopulated less than a decade ago.
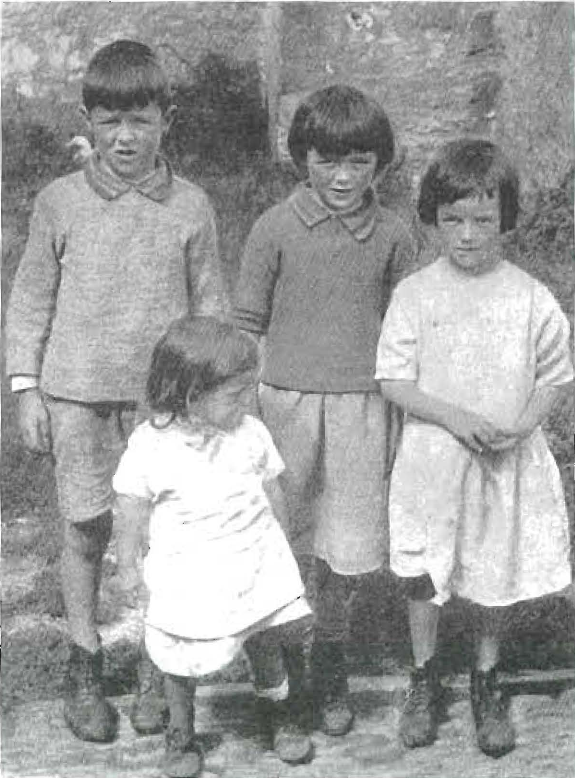
Fig. 2 – These children of the Isle of Bardsey had modern foods and active caries. All are mouth breathers. Note the lack of development of the middle third of the face.
In the technical textbook to which this series is complementary I have discussed the mechanisms that are involved in this deformity and traced its cause directly to the absence of activators and minerals in the foods.
It can readily be anticipated how these two serious disturbances of dental caries and facial deformity can occur in the same persons as parallel symptoms of a common group of causative factors, all of which are to be found in the food intake. It impresses one profoundly who has been trained to study faces critically, to note the striking differences in the physiognomies of two groups of the same stock separated by only a few miles in physical distance but living on different nutritions. In one group were found large numbers of persons with irregular teeth and serious facial deformities urgently needing the services of orthodontists. In the other group, in practically no case was there need for the orthodontist’s services among those receiving an adequate nutrition of minerals and vitamins.
If the data I have presented are correctly interpreted as indicating that white flour products and the foods that are associated commercially with them so distinctly lower the effect of the body factors that provide defense and immunity, it should be possible to produce different effects in animals by simply modifying the nutrition in the general way that I have outlined. In order to study this phase of the problem I presented in my paper before the American Dental Association meeting at Buffalo, September, 1933, the results of placing fifteen pens of rats on fifteen diets that are similar in all respects except the form and kind of cereal products used. Three of these modifications of nutrition are shown in Fig. 3, in which will be seen a comparison of the distribution of the minerals of the cereal part of the ration when different forms of wheat were used; associations and comparisons were made with the physical development of the rats. The three forms of ground whole wheat used were whole wheat, white wheat flour, and bran and middlings mixture. In the first column it will be noted that the rat that has been feeding on the entire wheat product in connection with the stock diet which was the Mellanby1 ration as modified by Hoppert, Webber and Canniff2 and which consisted of cereal 66, whole-milk powder 30, alfalfa meal 3, sodium chloride 1, is in excellent physical condition and is much larger than the other two. The one in the center receiving the white wheat flour as the cereal part of the ration has shaggy hair, is extremely nervous, underdeveloped and emaciated. The third rat receiving the bran and middlings mixture, while much better than the second, lacks a great deal of being equal in physical efficiency to the first rat. While there was a decided difference in the physical appearance, the difference in the nervous reaction was even more striking. The rats fed entire wheat were active, had good disposition and could be handled even roughly with impunity. The rats of the second group were irritable and nervous, even treacherous. They would jerk involuntarily at a mere snapping of fingers in front of the cage. The rats in the third group were listless, undersized and evidently subnormal when compared with the rats in the first group.
DISTRIBUTION OF MINERALS IN RED CROSS WHEAT

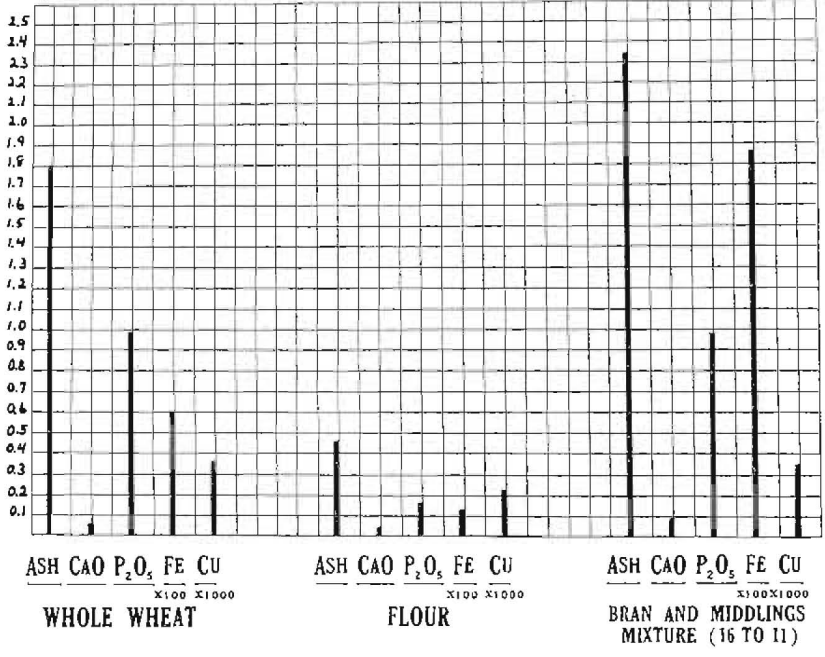
Fig. 3 – The nutritional effects produced by three diets differing only in the wheal product factor of the ration. Note the marked difference in the chemical content of white flour and whole wheat, particularly in the phosphorus. The middle rat on a flour diet had dental caries.
Since all factors in the nutritions were the same except the cereal factor it is important to note some of the principal differences in the mineral content. The phosphorus content of the ration of the group receiving entire wheat was 0.97 as compared with 0.16 in the rats fed the white flour. The mineral content of the group receiving the bran and middlings mixture, while higher than for the rats receiving entire wheat, did not produce so good a physical efficiency as the entire wheat product.
In the extended text I have prepared I present the chemical analysis of the blood of these various groups of rats in comparison with one another and note those characteristics that were most significant in association with the diets used. It is important to note that the activator other than that in the cereal was the same for all the animal groups, and also that the calcium content of the cereal did not differ greatly in these three groups, while the phosphorus markedly differed in the white flour group.
If the data I have presented in preceding research reports and in the communications preceding this in The Dental Digest are correctly interpreted, it should be possible to modify the severity of dental caries in any group of human beings or experimental animals. It should also be possible to prevent dental caries or even check it if already active by the addition to the nutrition of the affected group of those substances present in the food of the immune group. I have interpreted these variations to be related to a difference in the quantity of fat-soluble activators in the nutrition and a difference in the quantity of minerals, chiefly phosphorus, and also in the chemical form of the minerals, particularly phosphorus. This is not a new or recent procedure for me because it has been a progressive development and in continued successful operation since 1922, and under study for five years previous to that date with regard to its being related to radiant energy and its products. I have published many reports in the meantime showing progress in the development of this phase.
At this time the practical application of this procedure by the selection of rampant cases of dental caries among children in two missions of Cleveland will be discussed. I have selected these children on the basis of the urgency of their need as indicated by the extent of dental caries and evidence of its activity. Three clinical groups have now been run in Cleveland, two in the same place during two different years. There are two groups in the Broadway Mission and one in the West Side Community House. In the former place the selected group received as special reinforcement one meal a day for six days a week for about four months of the winter and spring, from February to June, 1932. The present group in this institution receives similarly one reinforced meal a day for six days a week from November to June, 1933.
The group at the West Side Community House received one reinforced meal a day for five days a week from March 30 to July 1, 1933. Wherever possible the children selected had cavities in which the decalcification extended to or near the pulp, as evidenced by the roentgenograms, but the teeth were known to be still vital. Pulpless teeth were extracted. Similarly the teeth with serious pulp involvements were extracted. As an experimental procedure many teeth were retained in which there was little possibility that the pulps could be prevented from progressive degeneration ultimately requiring the extraction of the teeth.
A considerable number of the teeth were purposely left without restorations, particularly those in which there was no danger of mechanical pressure causing pain or injuring pulp tissue. In my hundreds of clinical cases extending over the past decade, it has frequently been noted that hypersensitive teeth rapidly lose their abnormal sensitivity and become normally comfortable. In many cases in which the decalcification had approached the pulp, the odontoblastic layer of the pulp had been induced under the nutritional program to lay down a protective layer of new dentine at the point where dental caries was approaching. This, however, was done on three reinforced meals a day inasmuch as the instructions regarding the selection of the nutrition involved all the meals and the activators were used in all three meals. In these three groups neither the children nor their parents had instructions as to what to eat during the other fifteen or sixteen meals of the week which they had at home, nor did they have any special reinforcement of vitamins or activators to use with home meals.
The quantity of activators given in the one meal a day was approximately that which would ordinarily be distributed through three meals, but it would not be possible similarly to increase the food eaten during the meal since presumably children would eat until their hunger was satisfied at each meal. An effort was made, however, to select the foods for the special meal so as to provide a reinforcement of the minerals, particularly by the addition of the factors that are present in liberal quantities in the foods of modern civilizations. Specifically, this consisted of changing the white bread products to entire cereal products, thus reducing the calories content in proportion to the mineral and activator content and providing every day one of the natural sources of the fat-soluble activators that are available for the primitive group.
Roentgenographic studies were made in all cases of molars and bicuspids and in other teeth in which caries had occurred. Samples of saliva were taken for chemical analysis, detailed records were made of the positions of the cavities, height and weight and general physical conditions and special factors were recorded with each case, including photographs of the face in special cases. Additional roentgenograms are made on an average of every sixty days to check the change in the dental conditions, particularly for comparison with earlier and later records.
A typical striking illustration of what has occurred is seen in Fig. 4, in which is shown four views of the same tooth enlarged to reveal the detailed structure of the interior of the teeth and the supporting bone. It will be seen in the first view that the decalcification had apparently reached the pulp. The debris was removed by washing, and such of the carious matter as could be dislodged easily without danger of exposing the pulp was removed by instrument. As in such advanced cases of dental caries, a protective temporary restoration was placed to protect the pulp. It will at once be seen that in the period of thirteen months between the first and last views the pulp has laid down a well organized layer of dentine providing complete protection. There is no doubt that this procedure continued to make this tooth fit for service. However, it is important to consider what might happen if the service was not continued.

Fig. 4 – Four stages representing caries of the lower first molar. Note the new protecting wall of dentine built over the pulp as a result of a special nutritional program.
The change that occurred during the period that the child was given the reinforced nutrition is illustrated in the difference between the first two views which represent this period. The first roentgenograms were made on March 5, the second on July 12, 1932. The nutritional reinforcement was discontinued during the summer and was not taken up again in the fall partly because the patient moved to another community. It is of interest that the reparative process progressed favorably beyond what it was in July, as evidenced by the roentgenograms made on December 17, 1932. Another roentgenogram made on April 22, 1933, shows little change in the extent of the new wall of dentine built over the pulp. However, the decalcification that had begun on the proximal surface and had become inactive has now become active so that a new cavity is developing in this tooth because of an inadequate intake of something that had been made adequate during the early period.
Several cases of this type are shown in Fig. 5, in which the following details should be noted: In number 1 is shown a carious cavity with decalcification extending close to the pulp. In the second and third views there is disclosed a progressive decrease in the size of the pulp chamber, with a progressive thickness of the zone of protection and an increased factor of safety for the preservation of the pulp. This total change has occurred in six months under the nutritional program.
In number 2, eleven months later, the first four months of which the patients were on the special defensive program. The condition is similar to number 1.
In number 3 the occlusal caries had decalcified to the distal horn of the pulp. Nature has built in a protecting zone as well as mineralized the decalcified dentine such that in five months an excellent factor of safety has been established. In the first and third cases protective temporary restorations were placed to prevent pressure from disturbing the pulp.
In number 4 no protection was used, and it will be noted that the caries has not extended in the six months while on this nutritional treatment, and a fine zone of protection has been built over the pulp with an increase in mineralization of the entire tooth, including the decalcified dentine.
Numbers 1, 3 and 4 are in the group receiving a reinforced nutritional program from November, 1932 to June, 1933. Number 2 was in the group that received a reinforced nutritional program from February to June, 1932.
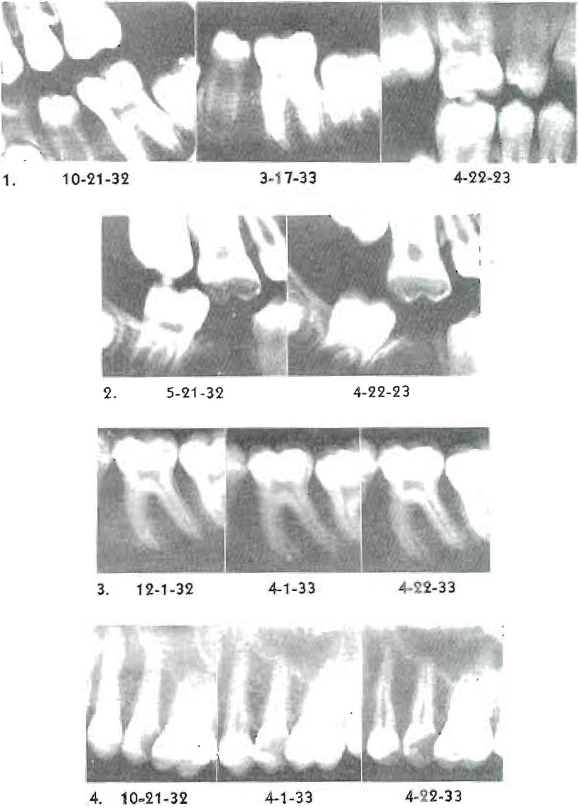
Fig. 5 – Typical examples of the building in of a protecting wall of new dentine within the pulp chambers and the mineralization of decalcified dentine under nutritional treatment for the control of tooth decay.
It was gratifying to see the appreciation of the children for the benefit they were receiving from this nutritional program. They seldom missed a meal, and many of them changed from being children difficult to manage to affectionate and cooperative boys and girls under the direction and efficient supervision of Miss Ruth Flaherty.
The physical changes that occurred in these children were marked. There was a general gain in weight and in growth. In the first group eight children gained on an average of 7 pounds each in fifteen weeks. Most striking of all was the difference in their dispositions and sense of well being. One boy gained 7 pounds in four weeks. He had been a frail invalid owing to lack of nutrition, and it was a question whether he should walk the two blocks to come to the mission for his meal. In a month he was able to play basketball and he soon played as hard as the other boys.
The improvement in school work was so striking that on two occasions teachers came to me to inquire what l had done to create so marked a change in the children, who had progressed from among the poorest in the class to the best. In my private practice one boy’s grades improved from 55 in mathematics to 97 and there also was an excellent change in his physical well-being and general disposition.
The following is the nutritional program provided:
As the children come from school to the church for their noonday meal for six days of the week, they line up and take from a spoon a mixture of half and half high vitamin butter concentrate and high vitamin cod liver oil. The butter vitamin concentrate was chiefly made from butter produced by cows fed a rapidly growing wheat or rye. The quantity of butter vitamin concentrate taken is usually 4 cc. daily and in some instances 6 cc. (One teaspoonful is 4 cc.) This was followed by fruit or tomato juice. They then proceed to the table to eat a luncheon in which the fluid parts are largely milk or the juices of meat and vegetables. On some days is served a pint bowl of a thick vegetable soup and meat broth made from bones and meat, into which is added not the meat in which the material had been cooked but some chopped fine grade meat that has been broiled in the pot to retain all its nutrition. The vegetables are selected on the basis of mineral content as outlined in detail in my textbook. In addition, a cooked fruit, not highly sweetened, and special entire wheat muffins are served. The muffins are spread liberally with high vitamin butter produced from cows pasturing on rapidly growing young wheat and rye. Each child drinks a pint of milk with each meal. The children are allowed as many helpings as they desire.
The fat-soluble activators in the form indicated and the high vitamin butter are furnished by me. The other foods are provided by a special fund under the management of the church staff. The concentrate was prepared from the best butter products that could be found in various parts of the country and some from other countries.
lt is of interest in this connection that over 75 per cent of all the butter that I have found to be sufficiently high in vitamins for my use has had to be shipped a thousand miles or more and often duty must be paid as well as expressage. This, as I have shown in my textbook, is entirely unnecessary since the product can be produced in any place with the proper nutrition of the cattle. The ration of butter allotted provides an adequate supply of vitamins for twenty-four hours and usually approximately enough minerals to carry the child through the day while supplying both the energy and reparative factors.
The striking effects obtained in some cases by this procedure is shown in the two following cases: I was called on the telephone one day by the Reverend Edwin A. Brown, Pastor of the Broadway Methodist Episcopal Church which is located in a mission district. A large number of the workers in that vicinity are engaged in the steel mills which have been shut down during an extended part of this industrial depression. The Reverend Brown reported to me that he had just been called to a home to baptize a small child for burial, and while he was extremely ill with a broken leg that had not united and was suffering from repeated convulsions, the Reverend Brown believed that the child might be saved. He thought the cause was largely nutritional and asked if I would see the child. He was a frail little lad, aged 3 years, and had had his leg in a cast about two months. The convulsions were becoming progressively more severe and more frequent and had already extended over a period of six or eight months. The child was carried by his grandmother on a pillow on the back seat of an automobile to the office. He had broken his leg as he fell during one of his convulsions while walking across the kitchen floor. The boy had been living on bread and milk. Ordinarily, bread and milk is considered a pretty good diet. Had he been getting bread and milk in the Alps in the communities in which l found high immunity to dental caries, he would not have had this accident, but he was living in a modernized, so-called civilized community. The bread he was eating was white bread and the milk was skimmed milk.
It is important to note that the calcium and phosphorus are as high in skimmed milk as in whole milk; however, this child’s body could not maintain the minerals in the blood on this nutrition and he was compelled to borrow from his skeleton, thus undermining his bones from the inside. The only changes that were made in his diet were the following:
The child was fed rolled whole wheat, which I keep on hand to give to patients (not for sale) as a part of an educational program. They are taught several ways of using it. The instructions to the boy’s grandmother were to cook the cereal for a couple of hours in a double boiler with plenty of water, five or six times as much by volume as was used of the cereal.
This was to be strained through a piece of cheese cloth to take out the coarse bran if it was found to be irritating. Muffins were to be made a little later of the same material, some of the cooked cereal to be used as a binder instead of a white flour binder. The child was to have all the whole milk he could use, and in addition have put into his milk each time it was served to him warm some of the high vitamin butter concentrate which I gave them in little vials. Some of this butter concentrate was also to be put over his porridge. It was of interest that the boy has not had a single convulsion since he took his first meal, immediately on his return home, containing this high vitamin butter concentrate and fresh whole milk which the Reverend Brown had supplied to him every day. In one month’s time the broken femur was united as shown in Fig. 6. The roentgenogram was made thirty days after the boy started on this nutritional program and after the removal of the cast. The view shows the bone condition both before and after treatment. Dental caries which had been rampant ceased to be active.

Fig. 6 – Healing of Ununited fracture in thirty days with the aid of butter vitamins.
About sixty days after the boy was first brought to me the Reverend Brown called at his home to see how he was progressing, and his mother stated that he was in the yard playing. They both went out to find him but because he was afraid he was to be punished for something he ran and climbed over the back fence. He had had an attack of infantile paralysis in infancy, which was largely blamed for the symptoms he later developed but apparently have been outgrown. This boy is a brother to the one whose teeth are shown in Fig. 4. They are two of a large family. The mother’s teeth were wrecked with caries, for clearly she had to pay the price of frequent pregnancies and poor nutrition. She, too, was provided with additional vitamins since another pregnancy was in progress. On measurement she asserted that she had lost 4 inches in height during her periods of child-bearing.
Another case that illustrates an important problem that is associated with modern civilization is arthritis. As I have previously noted, I found its occurrence rare in the communities with high immunity to dental caries both in the Outer Hebrides and in the physically isolated districts in the Alps. This is in strong contrast with an American mountain community where modernized living conditions have been in use for many generations. In one of the eastern states of the United States, I found a community where every fifth house had a severe case of arthritis. Arthritis is usually associated with adults, particularly with the aged. In that community I found children bedridden with arthritis as I made a door to door inspection in studying the nutrition and its effects. The case reported here is in an adjoining state.
The mother solicited my assistance, reporting that her boy, aged 5 years, had been in bed most of the time, in hospitals for two and a half years with rheumatic fever, arthritis, and acute heart involvement. She reported to me that she had been told that her boy could not recover, so severe were the complications. She requested that if that is true she be privileged to take him home and enjoy him as long as he lived since he was her only comfort. As is so generally the case with children with rheumatic fever and endocarditis, this boy had suffered severely with rampant dental caries. It is important to keep in mind that according to the data of the American Heart Association, 75 per cent of all cases of heart involvement begin before 10 years of age. My studies have shown that in more than 95 per cent of these cases there is active dental caries. This case was typical in this regard. In addition to the nutritional factors outlined in the previous case reported, the mother was provided with a rubbing oil for the affected joints. This consisted of the same material that was in the capsules, with the exception that it had been exposed for ten minutes to sunshine in an open dish as an activating process. The fat-soluble activators were given as a mixture of high vitamin butter concentrate and high vitamin cod liver oil in equal parts. This was placed in naught size capsules of 0.6 Gm. in each. The boy took three of these capsules with each meal. His nutrition consisted chiefly of entire grain cereals freshly ground and entire grain breads, a liberal use of whole milk supplemented with vegetables and fruit, with fish and a limited amount of sweets. This patient is shown in Fig. 7.
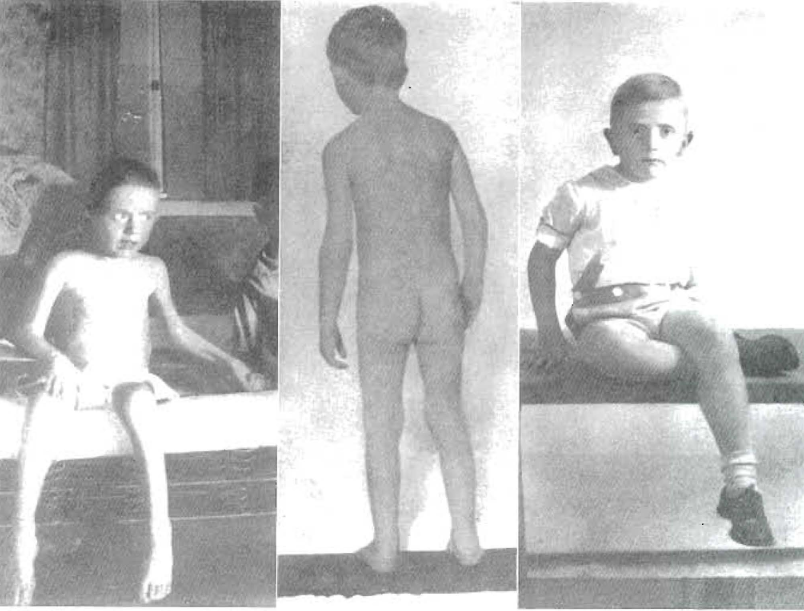
Fig. 7 – Multiple arthritis and heart involvement following rheumatic fever. Approximately six months elapsed between first and second and second and third views.
It is difficult to realize the great change in the physical condition which occurred. The distressing and acute pain rapidly subsided; the boy’s appetite improved; he slept soundly and gained in weight rapidly. In the first six months he had changed to the condition shown in the second view and in the second six months to the condition shown in the third view. The ankylosed condition of the spine, including the neck, has cleared, and the boy has full use of his hands, legs and feet.
In the light of our newer knowledge as illustrated by these investigations, which include a large number of cases of arthritis, several of which I have previously reported, it seems clear that skeletal degenerations as expressed in arthritic processes are often largely and probably always in part due to mineral metabolism disturbances which have their origin largely in nutritional deficiency. It is easy for focal infection from teeth, tonsils, or any other source, including epidemic infection, to become planted in the joints where an abnormal state has been established through nutritional stress. Indeed, many of the disturbances in the soft tissues as so-called organic diseases, including heart involvement, such as endocarditis, may have the soil prepared in large part by a disturbance in activator and mineral intake.
As I dictate this, the data are just coming through on a second blood test for a woman, aged 72, who has been another of the unfortunate elderly people to have a broken hip. She is in a hospital in another city, and when my assistance was solicited by the physician in charge of the case, his prognosis was bad since there was already a rise in temperature, the patient was coughing and the dread pneumonia that so often involves these cases was greatly feared. A chemical analysis of the blood and saliva showed chemical factors that would preclude the possibility of healing fractured bones. A check on the saliva in ten days after the new nutritional program was established shows a remarkable improvement. Another sample of blood has been brought one month after the first, and the patient’s physical improvement checks with the improved blood picture, for now she and all concerned are hopeful and confident of her recovery. Her physician and her son both report that she is physically in better health now than before her accident. Pain was relieved rapidly. The following will illustrate the changes:
The product of calcium and inorganic phosphorus of the blood serum, which is normal at about 40 and which for normal repair of bones should be at or above 0, was in the case just cited down to 17.3. It is exceedingly difficult if not impossible for broken bones to unite if this factor is below 25. In one month’s time this factor has changed to 28.9. The inorganic phosphorus of the serum was at 1.75 and this has increased to 3.03. Similarly, the solubility factor of the blood for phosphorus was previously abnormal, such that whereas the inorganic phosphorus of the blood serum should normally be decreased in the presence of powdered bone by a process of absorption, in this case it was seriously abnormal. The inorganic phosphorus passed from the powdered bone to the blood serum to an amount equal to 46 per cent of the serum inorganic phosphorus. This factor has changed so that now 17.5 per cent of the inorganic phosphorus of the blood serum passes to the powdered bone. This makes bone healing favorable. The following changes have occurred in the saliva. Before treatment the inorganic phosphorus of saliva passed from the powdered bone to the saliva to an amount of 13 per cent, which is in the wrong direction, and in ten days moved liberally from the saliva to the powdered bone by a process of absorption.
While this series of articles herewith concluded has been in process of preparation and publication, the material has been almost completed for a textbook in which the discussions are more technical than in this series and in which probably most of the questions prompted by the reports of these investigations have been answered. Fortunately, Nature has provided us a magnificent control in this big human experiment in that the primitive people of many lands have been relatively immune to dental caries until they have been reached by modern civilization and its commercial foods. While this is being put in type I will be searching for bands of primitive Eskimos and Indians in Northwest Canada and Alaska to learn their lessons to help us with our problems. These field investigations will include studies of the chemical characteristics of the blood and saliva and their relation to the level of immunity to dental caries and other degenerative processes, such as irregularities of the teeth and facial deformity and arthritic processes. These blood and saliva studies will be compared with more than 2000 blood analyses of persons in modern civilizations and nearly an equal number of saliva analyses for modernized subjects.
It is important that these new principles be made available for practical application as rapidly as possible. For this purpose I have prepared data for a textbook including the following: detailed procedures for diagnosis and treatment, chemical procedures for analysis of blood and saliva, testing of foods, their preparation and selection of high vitamin products, and details for clinical application. The text is designed to anticipate the scientific and practical needs of dentists, physicians, and other health workers.
References Cited:
- Mellanby, Mav: Diet and the Teeth, Brit. J. Dent. Science 64: 70.81, 1921.
- Hoppert, C. A.: Webber, P. A. and Canniff, T. L.: The Production of Dental Caries in Rats Fed an Adequate Diet, J. Dent. Research 12, February, 1932.
Editor’s note: Since the era in which this article was written, society’s understanding of respectful terminology when referring to ethnic and cultural groups has evolved, and some readers may be offended by references to “primitive” people and other out-of-date terminology. However, this article has been archived as a historical document, and so we have chosen to use Price’s exact words in the interest of authenticity. No disrespect to any cultural or ethnic group is intended.