
Access to all articles, new health classes, discounts in our store, and more!
Study of an Abrams Demonstration
Published in The Journal of the American Dental Association, August 1924.
* * *
The following is a report of a study made of an instrument that was brought to me by the presumable owner, which, he stated, was a set each of the Abrams Diagnostic and Treatment Units, with the request that I investigate the instrument and his method of applying it, he having assured me that he had complete confidence in it. Knowing of the criticism of the instrument, he desired to leave it to my findings as to whether he was correct in his interpretations as to what the machine would do in his hands. He assured me that he would let my findings determine whether he should continue its use in the examination for and treatment of disease.
Dr. Blank and his assistant, who is his subject, arrived with the instrument on the afternoon of Tuesday, March 4, 1924. He selected a back room which could be darkened and which had water pipes conveniently near, where there would be maximum freedom from the contaminating influence of bottled pathologic specimens or sources of bacterial culture and bottled chemicals.
The diagnostic instruments were set up on a glass-top table, the plateglass of which was approximately three-quarters inch in thickness. Attachments were made to water pipes by placing the wires under the screw of the faucet, and wires were continuous metallic circuits from the instruments they were grounding, either by being continuous wires or by soft soldering. The subject, a man about 30 years of age, stood, with his shoes on, on a rubber mat (the subject is not the patient but is part of the examining equipment), and the examiner sat in a chair with his shoes removed and his feet on large zinc plates, which were grounded to the water main. To increase the conductivity of the water main, the water was turned on in it, at the request of the examiner. Great care was taken to see that all binding posts and plug contacts were making good contacts to insure perfect electrical connection. The instrument was thoroughly tested out by the examiner who was demonstrating it, to make sure that both the instruments and his subject were in perfect working conditions.
The first series of studies was made at night when there was a minimum of disturbance and distraction from outside the room. It was demonstrated to us that the subject must stand facing exactly due west. Otherwise, correct readings would not be possible. This was accomplished by means of a compass. The compass, however, was found to be in error, owing to the presence of a magnet, used for sterilizing various fields, which was lying in close proximity to the compass. It was explained that the adjustments of the instrument were so sensitive that all of these conditions, such as magnetic direction, must be observed.
The demonstrator requested me in advance to have ready for him samples of blood from cases to be diagnosed. The first used was that from a patient, aged 39, who had been severely crippled with arthritis and who had been greatly relieved by removal of dental infection, but was physically incapacitated because of extreme muscle atrophy resulting from anterior poliomyelitis (infantile paralysis), which she had suffered in childhood. We had assured her that this muscle atrophy would not now be subject to treatment. She reported to me, however, that she had been assured of great improvement if she would submit to treatment with the Abrams method by a local operator (not the demonstrator), and also advised me that she had paid more than $200 for the treatment, without apparent improvement. A reading was started on the blood from this case but was discontinued when the operator found that it had been in a room in which there was a milligram of radium, and in its place the reading was made from a sheet of filter paper on which she had been requested to write her name with a pencil with a metallic frame. An Eversharp, furnished by the demonstrator, was used. At the time the above mentioned sample of blood was taken, two other samples prepared in the same way were left on a lower floor of the building and were used later for making diagnoses.
A demonstration was made to show that the results were entirely different whether or not the subject faced some direction other than due west.
All of the blood preparations that we had in readiness for the tests had to be discarded because it was found by the demonstrator that the paper had been torn from a hemoglobin test book, which had a test chart in the front of it, showing the different shades of red, colors which were considered adequate to spoil completely our blood specimens, which had been made with great care and with much expenditure of effort, particularly in the preparation of the imitation bloods. This change in program necessitated some overtime work in preparation for the following day’s studies.
In order to remove, as completely as possible, the danger of my making wrong interpretations, I arranged to have from two to four assistants present practically at all times, an expert professor of physics part of the time, and both a physiologist and a clinical and tissue pathologist most of the time.
Details of Procedure
For the information of those not familiar with the detailed procedure required for making an examination, the following is a brief description. The specimen of blood, consisting of one medium size or, better, a large drop, soaked and dried into a piece of blotting or filter paper, or any white absorbent paper, is placed in the instrument called a “dynamizer,” which is shown both with the top off and on, in Figure 1. Inside the dynamizer will be seen two electrodes, which were attached to grounds extending to the water main. This dynamizer is connected to a box whose measurements were about 4 inches. This box, which is called an “intensifier,” is also shown in Figure 1. These two units are connected by a metallic wire, which passes through the lid of the dynamizer to an insulated metallic disk lying in close proximity to the piece of paper containing the blood. This is shown in the insert “Dynamizer open,” Figure 1. The intensifier is in turn connected by a metallic circuit, as shown in Figure 1, to the rheostat of the diagnostic unit, which consists of three units of variable resistance, one said to contain 50 ohms, another 10, and the third fractions of an ohm by division into twenty-fifths. (Two rheostats were used in series part of the time, as shown in Figure 1.) This instrument was connected through a single wire to the contact electrode, also shown in Figure 1, which was held in the hand of the subject, and in most of the procedures of the diagnosis, held by him against his forehead. This subject was clothed so that his body was exposed over the region of his chest and abdomen. The examiner or demonstrator sat on a chair, as stated, with his stocking feet on the grounded zincs, and was without connection with either the instrument or the subject except as the wires, passing from the instrument to the subject’s hand, passed across his neck, which was not part of the connection though it could become a means of conscious or unconscious recognition of the completion of movements on the part of the subject. It is not my opinion that this was used at all as a means of communication.
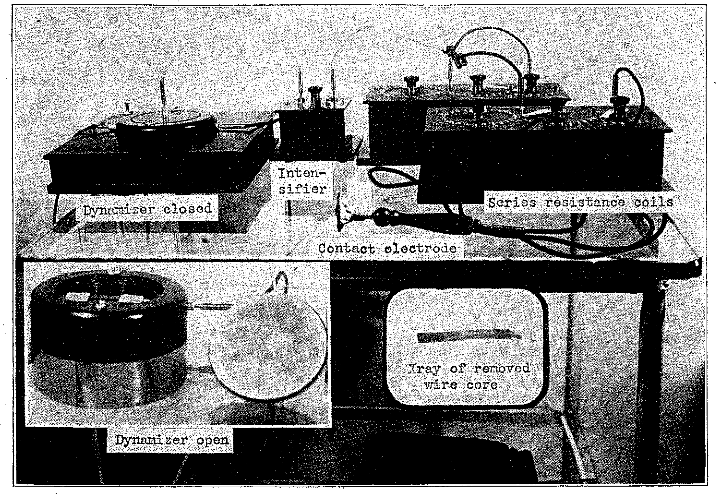
Fig. 1. Diagnostic Unit, Abrams.
The procedure consists in placing the paper containing the drop of blood, folded or unfolded, under the cover of the dynamizer; but before doing so, the dynamizer and its cover and the specimen of paper were each sterilized by making passes in front of them with a magnet. The top was then placed over the dynamizer.
Each disease is represented by a definite zone on the surface of the abdomen, not at all related to the organs in which the disease would occur. The cancer area, for example, is just to the right of the subject’s navel, which is at the demonstrator’s left as he faces him. The syphilis area is just above it; the streptococcus area at the left of the subject’s navel. A large number of diseases have their expression within a very small circumference around the navel.
The examiner placed his left hand on the bare surface of the abdomen and tapped with the second finger of his right hand on the second finger of his left hand. As he did so, there was always a dull note at the beginning. After from ten to twenty taps, the pitch of this tone sometimes raised, this constituting a positive diagnosis. The diagnosis was negative if the pitch of this tone remained constant. Having determined that any particular disease was present, its location could be established with considerable exactness, as will be shown presently. Since the percussing is done in many of the same or overlapping areas, the different diseases are distinguished by setting the rheostat so that a given number of ohms will be in series; as, for example, 32 for streptococcus, 50 for cancer, 57 for syphilis. Having determined that there was a disease somewhere in the body, let us say cancer, the location of the cancer was determined by placing on the subject’s head an elastic band carrying a contact, to which there was an extension, a single cable, insulated cord, to a handpiece ending in a point, which point was directed toward but not necessarily against, the surface of the body. If the tones came up strong when the point was pointing toward the gallbladder it indicated that the cancer was in the gallbladder; and similarly, other areas.
The severity of the affection was determined by measuring the fractions of an ohm on a scale which divided the same circuit into presumably twenty-five equal divisions, and the number of twenty-fifths of an ohm beyond the 50, say, for cancer, at which the tone came up best, determined the severity of the cancer. This point is important to remember in connection with the later part of this report.
A set of standards had been provided and were presented by the demonstrator, against which to check various affections or types of culture. These were in the form of bottles (Fig. 2) of about 2-ounce capacity, and were labeled “Staphylococcus, Streptococcus, Cancer, Gonococcus, Diphtheria, Tuberculosis,” etc. The demonstrator showed that if one of these bottles was put on the dynamizer and then the zone that corresponded was tapped, the tone would always come up unusually strong. Thus, the presence of a bottle containing the tubercle bacillus would make a very strong positive endpoint in the percussion tone as a sharp rise in pitch after from five to ten taps over the zone for tuberculosis. It was for this reason that the exhibition could not be made in the room containing the fixed pathologic specimens, which might contain influencing bacteria of the types concerned. (Our culture from the bottle marked “Streptococcus” grew only haybacillus).
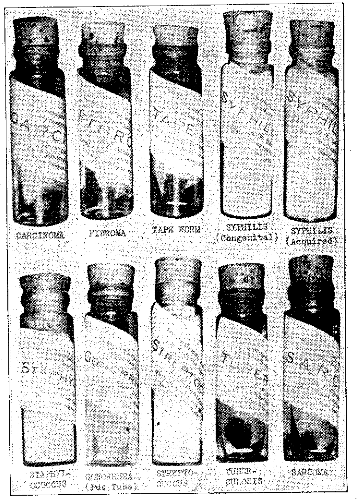
Fig. 2. Test specimens and cultures for checking diagnosis.
Experiments
Among the many specimens tested for us by him was one consisting of clippings from the lung of a rabbit that had just died from our inoculation with tuberculosis, belonging to a series, all of which have shown the same typical lung lesions, and demonstrated to contain the original and inoculated strain of tubercle bacillus. Blood specimens were included with it. The demonstrator knew that this material was taken from a rabbit that had just been subjected to postmortem examination, but did not know the source of the culture that was given to the rabbit or the type of lesion from which the rabbit died. He stated that from this he could tell the symptoms from which the patient was suffering. Notwithstanding the quantity and concentration of the involved virus, he was not able correctly to identify the infection.
Later, he tested the blood of this rabbit, as one of the blood specimens, thinking it was from a patient, and stated that, notwithstanding the fact that the patient had the following positive lesions: streptococci in the tonsils (the left one in particular) heart, right ear, bones; 30 ohms of acquired syphilis in the heart, nerves, brain, bones and joints; from 5/25 to 8/25 ohms of cancer which he did not locate, he did not have tuberculosis.
One of the specimens that I gave him was an artificial blood made by combining a water-color paint with argyrol. He found that this patient had the following diseases: streptococci in the ears, tonsils, heart, colon, and gallbladder; 30 ohms of congenital syphilis, affecting the nerves, brain, bones and joints, and digestive tract; and 7/25 ohms of cancer, located in the left breast and uterus.
Among the considerable assortment of blood specimens from which he made diagnoses were two taken from the first patient mentioned, who had previously suffered severely with deforming arthritis and has much muscle atrophy resulting from anterior poliomyelitis of childhood. The two specimens of blood, which were kept downstairs and were not, therefore, subjected to any undue influence from the machine or otherwise, were used, one following the other, in order to determine whether two specimens taken from the same patient, at the same time, under precisely the same conditions, preserved for twenty-four hours under the same conditions, and run one immediately following the other, with all conditions of the instrument, diagnostician and subject as nearly constant as could be, would give the same readings.
From the first test he found malaria, in the second, none.
Streptococcus and syphilis were found in both tests.
Carcinoma was not found in the first, but found in the second.
Tuberculosis was not found in either.
Streptococcus found in the tonsils both times.
Streptococcus was found in the fallopian tubes the first time, but not found in the second test.
Streptococcus was found in the genito-urinary tract the first time, but not found in the second test.
Streptococcus was not found in the heart the first time, but was found the second time.
Streptococcus in the teeth was not found at the first test, but was found at the second.
Streptococcus was found in the spine, fourth lumbar vertebra, in second test, but not in the first.
Syphilis of the heart was found the first time, but not found the second time.
Syphilis of the nervous system was found both times.
General paralysis was not found either time.
Syphilis of the bones and joints was not found the first time, but was found the second.
Syphilis of the ears, not found the first time, was found the second time.
Cancer of the breast was negative the first time, positive, the second.
Cancer of the lungs was negative the first time, positive the second.
Cancer of the gallbladder was negative the first time, positive the second.
From this, it will be seen that thirteen items of the diagnosis were different in these two diagnoses made within a few minutes of each other.
An important finding in the many diagnoses, and a great surprise and shock to us all, was that so many of the unsuspected individuals and rabbits, guinea-pigs and paint had syphilis. We therefore had arranged to use the blood of a male patient from a skin clinic, who had very positive and abundant signs of syphilis, as shown by the following facts: Internist’s report showed that the patient had syphilis in the third stage, with many scars on the chest, the result of syphilitic lesions of the second stage, and was a chronic alcoholic. The condition had been diagnosed in a local hospital clinic, and the treatment had been started but was discontinued by the patient. The diagnosis in this case showed this patient to have the following: 14/25 ohms streptococci; 2 10/25 ohms cancer, located in the uterus, breast and gallbladder. It will be noted that this is the only blood examined on the two different days that did not show syphilis, and yet this was the lesion that was fundamental in this individual.
I asked the demonstrator what percentage of people he found to have syphilis: whether the percentage would be as high as 75, and he stated that nearly all the people he examined had it, more than 90 per cent.
Treatment
As part of his equipment consisted of a treatment unit, which is shown in Figure 3, we asked him to demonstrate how it was used and what it would accomplish. He suggested that he take the blood from anyone in the room, and stated that he probably would find that the individual had syphilis; that he could treat the condition and cure it in about ten minutes, if it were not too far advanced, and that we would see immediately the difference in the reading, as expressed in the change in tone, by the improvement in the syphilitic condition of the patient. There were plenty of volunteers to furnish blood. The physiologist, whose health was excellent, was selected and was found apparently to have a very aggravated case of syphilis, 22 ohms, for which the demonstrator proceeded to give a treatment for ten minutes. I begged them to extend the treatment to make sure that it was a complete cure, so it was continued for twenty minutes, at which time the syphilis reading had reduced from 22 to 5 ohms, and he suggested that about two minutes more treatment would probably remove the balance.
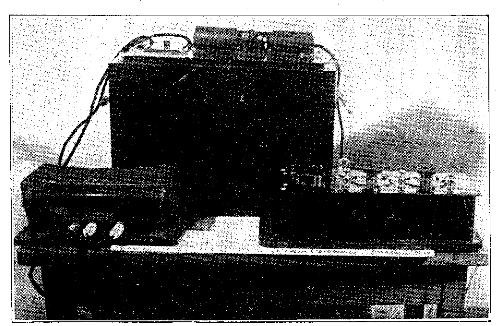
Fig. 3. Treatment unit, Abrams. The large box is the oscilloclast.
In receiving treatment, the patient held in his hand an electrode, ending in a disk about 3 inches in diameter, which was supposed to give off a potent but undetectable discharge, which passed readily through his clothing to cure his ailments. The large instrument on the table, furnishing this current, was called the “oscilloclast.” It has a rocking mechanism which breaks the circuit and probably introduces a little inductance, and is used through a box of series resistance. Eight patients can be attached to one oscilloclast, which makes an interesting noise like a metronome or a loudly ticking clock. This instrument was said to have the power of neutralizing the dynamizer and preventing its impulse to reach the subject. When this disk was brought near to the dynamizer, percussion on the subject’s abdomen gave a continuous tone without change of pitch. If it was taken a few inches away from the dynamizer, the tone became stronger and stronger. It became quite strong at a distance of 6 feet, but still had influence at 16 to 20 feet, and the operator demonstrated a difference in the tone, at even this distance, whether this disk was pointed toward the ceiling or toward the dynamizer.
Controls
During the progress of the many tests, I took occasion to remove plugs from contact points, where I could without being observed, for all of this work had to be done in very subdued light, and I could not tell any difference in the tone whether the circuit was complete or not. When I called his attention to this fact, the demonstrator informed me that my own handling of the apparatus would disturb its efficiency and that I should not do it. I therefore arranged to get the same result without touching it. While we were all dismissed for luncheon, I removed the connector between the intensifier and the rheostat, between the small instrument in the center and the one next to it, and, after taking off the plug, took the metallic core out of the center of the end of the wire for a distance of about three-fourths inch and filled it with a nonconducting hard wax, which gave the wire about its original stiffness. (Compare insert in Figure 1). The silk-covered wax cord connector was fastened into the metallic plug with some of the insulating wax and the connector was replaced. The instrument was again used in this way with all the precision and efficiency that had been used on the two previous sessions. In fact, the operator commented on the splendid working quality of all of the conditions.
I explained to the doctor and his assistant that, in all our research work, all our progress is based upon what we call “controls.” Conditions are set up in several different forms with only one variable factor at a time, and the presence or absence of this variable factor on repeated tests will be considered to be related to the change in result in proportion to the certainty that no other conditions have been changed and no new factors introduced besides the one being checked; that, accordingly, if I were to make a research problem of his instrument, as he had come a long distance especially to have me do, it would be necessary for me to proceed in this fashion, and suggested as a simple test that he tell us whether or not the blood of a given patient (and he might select his own specimen) was in the dynamizer or not, by the results he would get in percussing his subject. He readily acquiesced in this test, and in the first five times was in error four times. The specimen, not having been in the instrument at any time after its first removal, was given to one of the assistants who took it to a distance away from the instrument. He stated that this was not a fair test as he was mentally disturbed and distracted and not able to concentrate properly. I explained to him that there were certain tests that, because of this type of mental involvement, should be made without the knowledge of the operator, giving illustrations, and it was for this reason that I opened the circuit by removing the metallic core from the connector, as previously stated.
I asked him to give me a demonstration in which I would take part myself. To this he cheerfully assented, outlining the following procedure, which was carried out. He used as the patient his own case because he knew so well his own conditions. Instead of taking his own blood, he wrote at length on a piece of paper and placed this in the dynamizer. After setting the rheostat properly, he placed the double electrode on the subject’s head and the contact point from the diagnostic instrument was held by the subject against the bare chest. I was given the electrode that was connected to the subject’s headpiece. It was explained that the impulses would come from his brain through the 6 foot flexible, single strand cable to the handpiece electrode that I held in my hand, and I was to pass this up and down the back, limbs and fingers of the subject a few inches from the subject, but always holding the electrode at right angles to his body. When I came opposite the back of his leg, about half way between his knee and ankle, the pitch of the tone suddenly rose and indicated a very marked reading. The operator then exhibited his leg, which showed edema above the ankle and which he stated had previously shown cellulitis, which I had hereby diagnosed. In doing this, I disconnected the cable part of the time and the pitch went up the same when my other hand was opposite his shin, whether the circuit was connected or not.
I have previously referred to the method of determining the intensity or quantity of an infection or neoplasm of a given type by measuring the ohms and fractions of an ohm. It was demonstrated that he could read the ohmage to a twenty-fifth of an ohm on many occasions and go back to that same reading within one or two twenty-fifths every time, which was explained to me as one of the best proofs of the exactness and certainty of the process. While making the demonstration, I, without his knowledge, changed the position of his total ohmage lever and had him repeat the test, and the fraction came out exactly the same as previously. This is like using the ounce weights after having determined the total number of pounds in order to find the last fraction of a pound, and then making the scales balance after taking off one of the pound weights and balancing it with the same number of ounce weights that were used previously.
These results very definitely indicated to me that the matter was one consciously or unconsciously within the control of the demonstrator and his subject. I desired to test the effect of suggestion on the demonstrator, and I found that if I suggested that a sound was coming up clear and strong, on repetition it did come up clear and strong and made a positive reading; and if I would suggest that there was apparently nothing there, on a repetition there tended to be nothing there, and it was very easy for me to get the impression that I was influencing the demonstrator. I do not have any power to hypnotize and am sure that neither the demonstrator nor his subject were influenced in any of their other interpretations by any suggestion that came from myself or anyone else, for I did not make any suggestions during the major portions of the readings.
Summary and Conclusion
I told the demonstrator that I would send him this detailed written report, but before doing so I wanted to go over with him in detail, while all these witnesses were present, many things that had occurred. I showed him, for example, the specimen of blood which consisted of a water-color paint and argyrol, and reminded him of his reading, which indicated that this patient had streptococci in the ears, tonsils, heart, colon, and gallbladder; 30 ohms of congenital syphilis, affecting the nerves, brain, bones and joints, and digestive tract; and 7/25 ohms of cancer, located in the left breast and uterus; also, how the specimen of rabbit’s tissue, and, later, blood from this rabbit, which he was analyzing, was from a rabbit recently examined postmortem, which had died of tuberculosis of the lung, the culture of which we had inoculated, and how his statement was very positive that there was no evidence of tuberculosis indicated from this specimen; how he had given three different readings on the same patient, all very different; how his reading of the blood of the patient with syphilis indicated that that patient did not have the disease and that practically all the readings of other samples in the three sessions had shown syphilis; how, out of six trials that he had made to tell whether the specimen was in or out of the dynamizer, he had been in error five times, when, according to the law of chance, he should have been right half the time; and, finally, how he had worked for hours with his machine with his circuit interrupted by the removal of the core from the wire and placing wax therein, with conditions which he stated to be particularly satisfactory so far as the working of his instruments was concerned. I also showed him the insulating wax in the wire, which is so splendidly dielectric that it is used for insulation for high potentials. When he suggested that possibly this wax was a good carrier, I made a test of this by a very sensitive galvanometer with a high voltage, which would have completely ruined the instrument had there been good capacity for conduction. Indeed, this instrument would show a millionth of an ampere of current, and there was not the slightest deflexion; in other words, it had a resistance approximately equal to that of a telegraph wire reaching from the earth to the moon and back.
He assured me that he recognized that he had been mistaken, but that he had acted in good faith and never thought to make such tests for himself. It was mutually agreed that I would not publish his name but that he would write to the proper officers of his local society and explain that he had been mistaken, and that he would discontinue its use and use his efforts to have the practice discontinued by others in his community. He stated that I was privileged to publish this report, without his name.
The seriousness of this matter in the interest of humanity cannot be estimated. I have been told of a case of an unmarried woman who committed suicide after being told by this method of diagnosis that she had syphilis, and of a practitioner, who is probably only one of a great many, who is treating up to and exceeding 100 patients a day on the basis of $6 an hour, or $3 for half hour treatments. The demonstrator told of an operator who had made more than 7,000 blood diagnoses, a large part of the patients receiving treatments by him or by others, and that the average cost per patient for treatments would be about $100. We were advised by the subject that a customary charge for the time spent reading a patient’s blood was from $10 to $15 and that it took from ten to fifteen minutes, or a dollar a minute. He stated frankly that he was personally not interested in whether the instrument was efficient or not; that he was concerned and interested in the money that he got for acting as a subject, and that he had been serving as a subject for about five years. He cited cases where he thought cures had been made.
The operator and demonstrator made very elaborate comments and detailed explanations as the operations proceeded. These were taken by a stenographer and have been typed and are available, if desired, for elucidating this report.
We have made some tests to throw light on the nature and origin of the endpoint, which is a change in the tone of the percussion note. We are also testing the capacity of blood and such specimens as were used to discharge a very sensitive condenser. The evidence so far developed indicates that the presence or absence of a change in tone depends on the following factors: Under certain conditions of continued pressure and the stimulation of tapping, muscles go into slight rigidity, which raises the pitch of the percussion note. We noted that it took from ten to fourteen percussions to bring this change when the subject was first used and the muscles were therefore in their maximum tone. As he became more tired, the average time at which the endpoint appeared, extended to twenty percussions, and ultimately on some occasions to twenty-four. We have found, as was demonstrated by the operator, that it was necessary that he be very careful to tap the same place on his finger; that is, if he extended toward the nail the pitch went higher and would produce a false endpoint or positive reading. Similarly, we find that a considerable difference depends on the tension of the flexor muscles of the finger being tapped, since it is necessary to maintain pressure with that finger. Another variable, which relates to time, is the pressing of the blood and lymph out of the subcutaneous tissues over the abdominal muscles; and still another, which relates particularly to the percussions in those zones that are over folds of the small intestines, which seem to depend on the passing of a bolus of food or volume of air, and the same point on the abdomen will give quite different percussion tones over the intestines within a few minutes’ time. It seems a tragedy that so many variables should be entering into the endpoint on which the life and finances of so many individuals are being placed.
Owing to the length of the report, we have presented here only a part of the important data obtained.