
Access to all articles, new health classes, discounts in our store, and more!
Report of Dietary Observations Carried on at Ewa Plantation 1932-1933, Bulletin No 1
Published by Hawaiian Sugar Planters’ Association, Ewa Plantation Co., and The Queen’s Hospital. H.S.P.A. Research Health Project report. Dated 1932-33.
* * *
Foreword
It is believed that the publication of this Second Annual Report of the Health Clinic conducted jointly by the Hawaiian Sugar Planters’ Association, Ewa Plantation Co., and The Queen’s· Hospital will be of interest and advantage to those having to deal with questions of public health and dietetics discussed in this Report.
It is also hoped that the publication of this information will be welcomed by many others who are not engaged directly in health work, but are interested to learn more about the developments on Hawaiian Sugar Plantations in the field of general welfare and betterment of the health of employees.
For the benefit of those who do not understand the system of medical supervision and the care of health on Hawaiian Sugar Plantations, the following outline is submitted:
Sugar Plantation Medical Service
All employees on Hawaiian Sugar Plantations are given employment throughout the year, there being no seasonal work; even during the “off-season” the employees are retained on the plantation pay rolls and kept busy.
As an incident of employment, all sugar plantation employees are given either a house suitable to the family requirements or, if unmarried, living quarters suitable to the individual, and this housing is furnished without charge to the employees.
Certain other perquisites of employment are furnished free, namely–fuel, water, and medical attention. These last free perquisites go to all employees whose pay is $100.00 per month or less. All wages are paid in cash.
The medical attention furnished by the Hawaiian Sugar Plantations is perhaps unique in the extent of the field covered by this free perquisite. In general, each plantation maintains a hospital for the benefit of its employees; it has at least one regularly employed physician, and such nurses and visiting nurses and such staff of attendants as is made necessary by the numbers dealt with on each plantation. Regular dispensaries for minor ailments are operated daily. A baby clinic and prenatal advice for mothers are institutions in vogue on most of the plantations.
The service rendered by this medical staff without cost to the workers includes all physical ailments regardless of whether or not they originate as a consequence of employment. It, of course, includes the care of any employee for any injury as a result of industrial accident. It, however, goes further than this and includes the complete medical care of the employee even though he should be injured as the result of an automobile accident on the highway, when visiting a ball game on Sunday, or any other such accident. Free hospitalization and attention is given to all the employee’s family under similar conditions. Childbirth, tonsil operations, appendectomy and other surgical work, for any member of the family, are handled without charge in the plantation hospital.
There are 25 Hospitals, maintained by 38 sugar plantations, some of the plantations combining to use one community hospital for two or more plantations, and in other cases plantations located close to the cities may use the principal private hospital in the city for their hospital cases, paying the hospital for such services.
There is a total of 30 doctors employed by the plantations; in one or two cases a single doctor may serve two plantations. There are 64 graduate nurses employed in hospitals or as visiting nurses.
The equipment of all the plantation hospitals is of a creditable standard to meet the necessities, and in a few cases the equipment and facilities are equal to or better than many private hospitals in cities of the mainland where the population may exceed 50,000 or 100,000 people. A number of the hospitals are equipped with X-ray machines for bedside use.
Dr. Hoffman of the Prudential Life Insurance Company, eminent health statistician, said in an address in Honolulu on March 5, 1915:
“The health progress of Hawaii is of exceptional scientific interest as perhaps the most conspicuous modern illustration of successful tropical adaptation and race progress.”
“It has been my privilege to examine personally perhaps half of the labor camps on the principal islands, and, broadly speaking, their conditions conform as nearly as possible to a reasonable ideal as could be expected in the case of a population largely of Oriental, or otherwise Asiatic, origin. It is something very considerably to the credit of the Hawaiian sugar planters that in this respect they should have set an example of humanitarian consideration and conformity to the exacting principles of sanitary science far in advance of most of the plantation housing conditions in the southern states of the mainland, or of Cuba and Puerto Rico. It is even more to their credit that they should have provided better hospital facilities and free medical aid to a relatively low class of Oriental or Filipino labor on the Hawaiian sugar plantations than is available at the present time to most of the agricultural population, rich and poor, white and black, on the mainland of the United States. Such hospitals as are to be found on the island of Kauai at Lihue and on the island of Maui at Puunene challenge comparison with any similar institution as regards the equipment, nursing care, medical supervision, and even the keeping of card records, on the mainland. It is primarily due to the persistent efforts on the part of the planters to improve sanitary and housing conditions, hospital facilities, and provide food at reasonable prices for plantation laborers, combined with adequate wages, free fuel, pure water, etc., and the hearty cooperation of an efficient and thoroughly well-organized Territorial Board of Health that such far-reaching sanitary results have been achieved in recent years.”
Again in an article published in Stone & Webster Journal for December 1929, Dr. Hoffman recorded his impressions of another visit to Hawaii and an inspection of Hawaiian Plantations, as follows:
“The labor welfare policy of the Hawaiian sugar planters may be briefly summarized in essential points as follows: The planters provide in the first place free medical, surgical and hospital service to all laborers and their families. Each plantation has adequate hospital facilities, and the number of beds averages at least one bed to each 100 persons housed on the plantation. Thirty competent surgeons are employed by the planters, serving, as has been pointed out, a total plantation population of about 101,000.
“As regards sanitation, it may be said that all sanitary services are furnished free, including street cleaning, garbage removal, etc. The majority of villages are provided with sanitary sewerage systems, each family being provided with a separate toilet, wash and bath house. Housing is free and all buildings are kept in repair by the plantation. The general housing rule is, one family to a house of the bungalow type. Each house is provided with running water and sanitary facilities. All potable water supplies are approved by the Board of Health. The houses have enough space around them for a garden, which is cultivated for domestic use. There is an abundance of flowers everywhere and most of the houses are surrounded by hedges of flowering plants, giving them a neat and homelike aspect. Fuel is furnished free, but a small charge is made for electric lights, as a safeguard against excessive electricity consumption.
“The best test of a labor and welfare policy is, after all, the general death rate. The latter; of course, is to a certain extent conditioned by the birth rate. This in 1928 on Hawaiian sugar plantations was 30.25 per 1,000 and the evidence of an abundant crop of children was to be seen everywhere all over the plantations. The general death rate in 1928 was only 8.51 per 1,000, which compares with a general death rate for the Territory of Hawaii for the same period given as 11.70.”
As to the results of this system, it can be said that the health of workers on Hawaiian Sugar Plantations has been maintained at a high level, and that increasing efficiency and general. beneficial results are being secured by constant studies (the present pamphlet being a progress report of one such study). The splendid aid and assistance of physicians outside of· plantation employment who are themselves interested in research and the development of community health is gratefully acknowledged. Dr. N. P. Larsen and those mentioned in the paper here published have rendered a distinct and valuable community service.
Although the work covered by this report on the H. S. P. A. Health Project was originally begun as a research dealing with the decay of teeth, it has rapidly proven that its principal accomplishment will result from the studies of diet of children and the effect of a proper diet not only upon teeth but on the general bodily development and the prevention of disease in other organs.
It is in the belief that the success in the reduction of tooth decay and infant mortality, and the remarkable increase in bodily development and weight resulting from proper diet and attention, are matters which are of interest to everyone that this report is published.
Hawaiian Sugar Planters’ Association.
Honolulu, January 20, 1934.
Second Annual Report of the Directors of the H. S. P. A.-Ewa Plantation Health Project
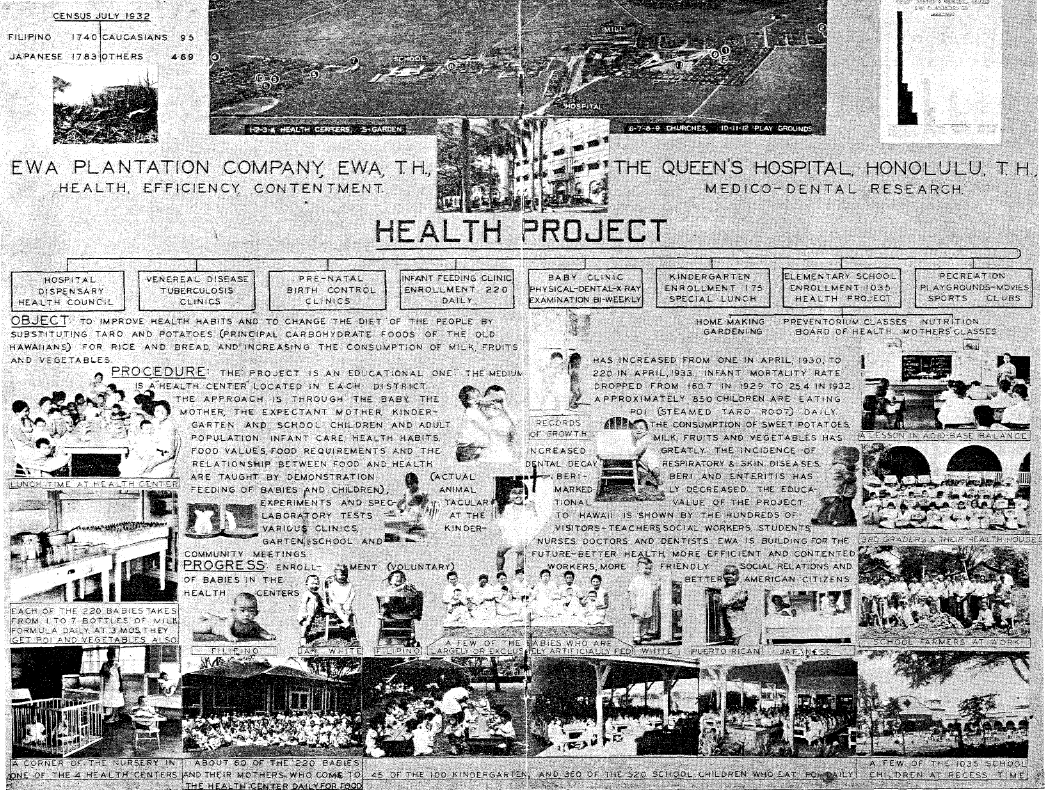
May 31, 1933, marks the close of the second year of the plantation “Health Project” which has been conducted jointly by the Ewa Plantation Company, the Hawaiian Sugar Planters’ Association, and the Research Department of the Queen’s Hospital, Honolulu. A brief review of the activities undertaken and accomplishments to date is herewith submitted.
Infant Feeding Clinics
In July, 1932, “health centers” were opened in “C” and “Lower” Villages, making a total of four “centers” which cover the entire plantation. All cooking is done in one center and the milk formulas and other foods–ready to be served–are delivered to the other centers where the babies living in the surrounding districts are brought once daily and fed. Formulas for other feedings are taken home.
Enrollment of babies in the Health Center is voluntary with parents and they pay a flat fee of $1.00 per month for each child. An additional charge is made for extra food over the amount allowed for the $1.00 enrollment fee. During the past year the receipts from parents covered approximately three fourths of the cost of food.
Enrollment and attendance:
Number of babies enrolled June 30, 1933: 225
Percent enrolled of those eligible (birth to two years of age): 92
Daily attendance (percent of those enrolled): 85
The age limit of two years for enrollment in the feeding clinic was removed during the year. When there is one child enrolled in the Health Center, parents, in general, object to enrolling the new baby unless the older one is discharged. The excuse is invariably “expense.” The need for increasing the age limit for enrollment is shown in the marked reduction in growth rate and increase in dental decay in those children who have been discharged at two years of age. Few parents know what constitutes normal development in babies and children and they accept poor posture, sunken chests, flat heads, thin bodies, bowed legs, diseased tonsils, decayed and abscessed teeth as inevitable and with little or no concern. Those babies who have been largely or exclusively fed on food provided by the Health Center are outstanding in physical development, as is shown in Chart I, page 8.
Physical and Dental Development of 117 Babies 12 to 15 Months of Age on Different Types of Diets
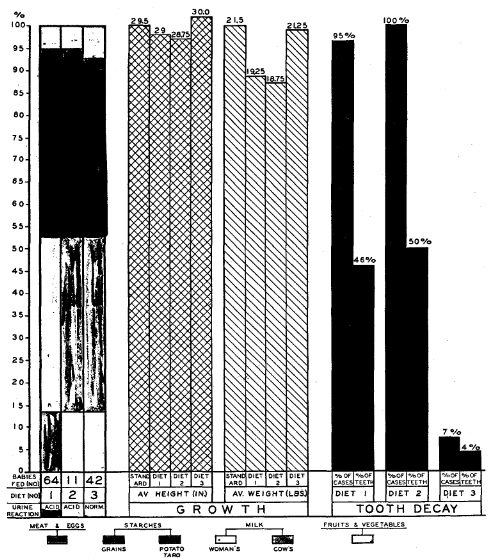
Chart I
Morbidity
General:
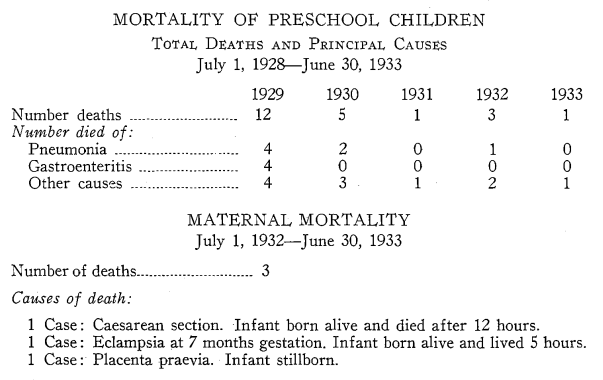
Infant health has improved, as has that of the preschool children. There have been few cases of pneumonia, with only two deaths (one infant with whooping cough and one preschool child following measles) in more than two years. There has been no death from diarrhea and enteritis since the health project was started and no case among infants that warranted hospitalization in more than a year. Mothers have learned how to prevent beriberi, and there has been no case which could be diagnosed clinically during the past year. The incidence of impetigo, pink eye and ear infections has been comparatively low. Illness is to a large extent restricted to the children of noncooperative mothers.
Whooping Cough:
Whooping cough and measles seem to strike the majority in alternate years. Measles swept the plantation in the late fall of 1931 and continued through the winter months of 1932. Subsequent complications resulted in three deaths. Whooping cough started in Ewa School in the early fall of 1932 and threatened to reach epidemic proportions. There were 36 more or less severe and protracted cases, with one death. Prophylactic treatment was given to more than 100 contacts. This, with other preventive measures energetically enforced by the medical and health center staffs and the greater resistance to disease of the babies due to improved physical condition, combined to prevent the spread and to lessen the intensity of the disease.
Venereal Disease:
As was reported previously, there are a number of families on the plantation, various members of which show clinical or other evidence of syphilis. Eight of the nine Filipino women thought to be diseased, whose record of 81 pregnancies has already been cited, have given birth during the past year or are now pregnant. There are six living babies, all of whom received some antisyphilitic treatment. The expectancy of life in all cases is good; nevertheless, two of this number already show marked clinical evidence of the disease. They are all offspring of alien parents, most of whom are too ignorant or indifferent to practice birth control. It is doubtful whether permanent cures are ever effected in syphilis, and in all probability, some, if not a considerable number, of this group will eventually become public charges.
Tuberculosis:
Ewa has 12 cases of tuberculosis at Leahi. Four have died during the past year. There are at least 75 suspected or arrested cases and known contacts now on the plantation. Two tuberculous families, both of which had babies enrolled in the Health Center, were returned to the Philippines during the past year.
In order to stop the spread of tuberculosis every case should be investigated with the object of determining, if possible, the source of the disease. The removal of the infected person from the premises is not enough. Tubercle bacilli live for long periods of time protected by a covering of sputum. It is perfectly possible for an entire household to become infected by living in a contaminated house. A policy, rigidly enforced, not permitting any person to occupy a contaminated house until after it has been thoroughly disinfected, would, it is believed, do much to improve the situation, as would also a special tuberculosis educational campaign carried out in the school, the various clinics, and particularly in the homes of the suspected cases and contacts.
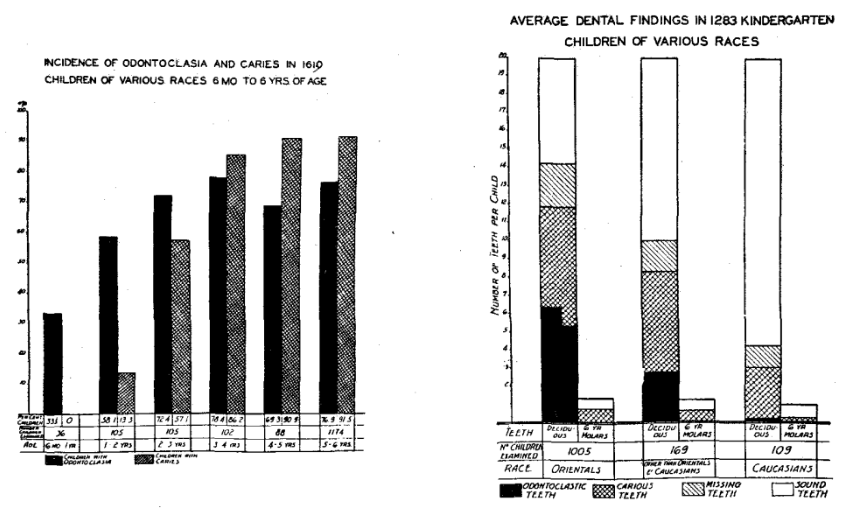
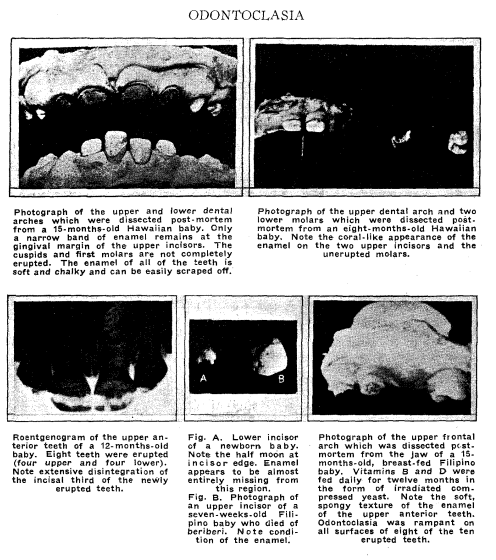
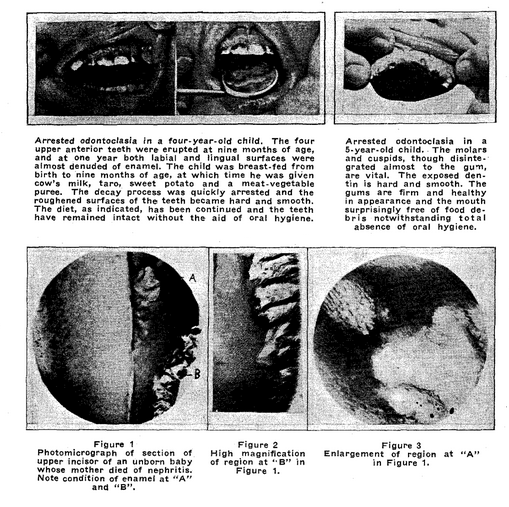
Dental Decay:
Dental decay is a systemic disease. “Odontoclasia,” a type of dental decay which is ravaging the teeth of the babies and young children of Hawaii, is a sensitive, and probably the best, indicator of community health. It is associated with high infant mortality, diseased tonsils, stunted growth, susceptibility to disease and abnormal development of the jaws, nasal and other facial bones which often lead to a succession of ills which persist throughout life.
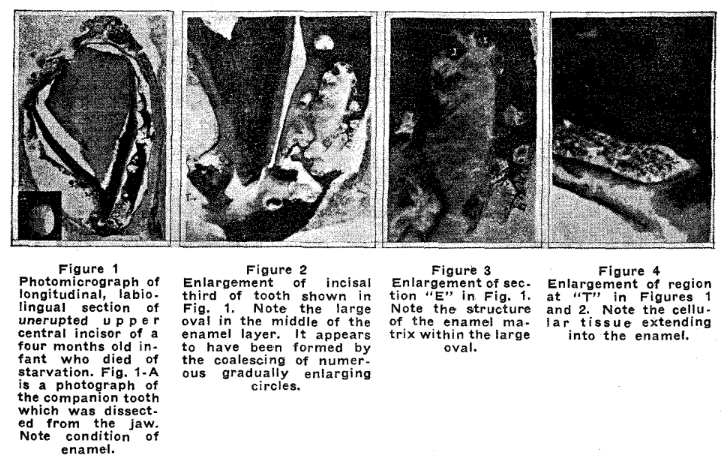
Odontoclasia has its beginning in prenatal life. It may occur in unerupted teeth and even in the teeth of the unborn. In a group of 50 Ewa Plantation Oriental babies studied before the health project was started, 40 had decayed teeth at 1 year of age, and 49 at 2 years. Odontoclasia can be prevented and arrested by diet–and apparently in a very simple way–the substitution of taro and potatoes for grain foods.
Concomitant with the tremendous and continuous reduction in infant mortality and morbidity on the plantation during the past 3½ years, there has been a parallel reduction in the incidence of odontoclasia, as is shown in Chart I.
Infant Mortality–Ewa Plantation, Ewa District (Exclusive of Ewa Plantation) and Honolulu City, July 1, 1928-June 30, 1933
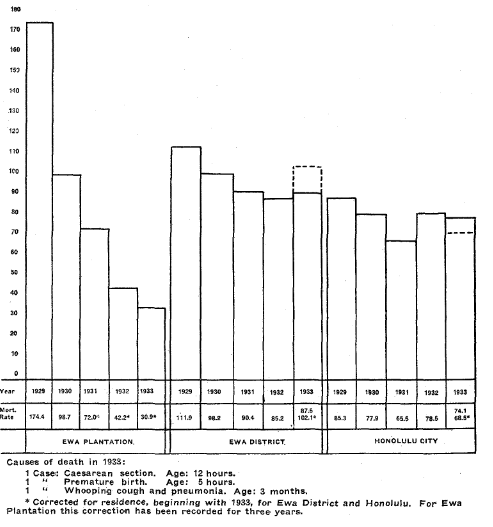
Chart II
Infant Mortality Filipinos and “Others,” Ewa Plantation, July 1, 1928-June 30, 1933
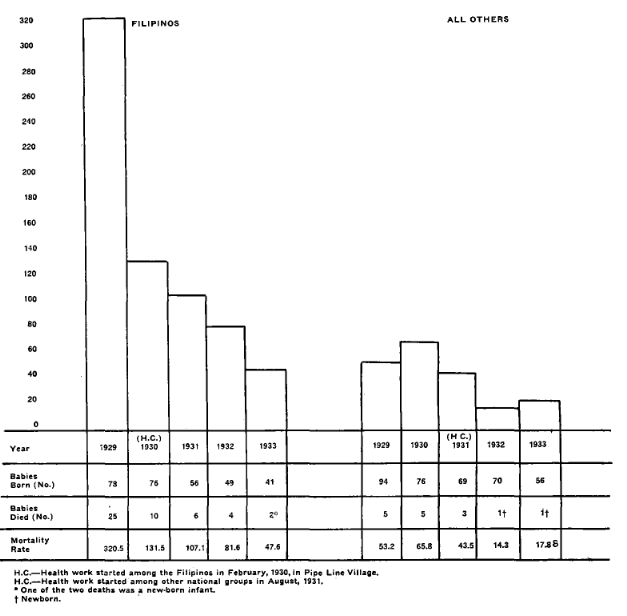
Chart III
Education
Infant and child care, prevention of infectious and contagious diseases, food values, food requirements and the relationship between food and health are being taught to the entire community through the various clinics, kindergarten, school, special meetings and classes for adults. Teaching is done by demonstration, spectacular tests and rat experiments showing the differences in food values and their effect upon the body. When the Health Center was first opened, a reward in the form of a savings bank was offered to all babies who attained the physical standard of the average white baby on his first birthday. This included 21 pounds in weight, good muscle tone, normal chest and head development, straight legs and sound teeth. It was about one year before the first baby qualified for the reward. Since then one or more babies have attained the requirements almost every month, and a number have exceeded them. The concept of the community of what constitutes normal babies and children is rapidly changing. It is difficult to get mothers whose babies are under par to bring them to the clinic for examination. Those who have fine healthy babies rarely miss the clinic and watch the growth records with keen interest.
Baby Conferences:
In addition to the feeding clinic which is held daily, conferences with mothers during which each baby is weighed, measured, examined and his teeth charted are held biweekly. In addition to advice as to general care, mothers are instructed in regard to the kind and amount of food needed for their babies. An effort is made to examine all babies under one year of age at least once each month.
Prenatal Clinic:
Mothers are being taught by means of X-rays of the bones of new-born babies and other tests that the diet of the mother during pregnancy has a marked effect upon the bone and tooth development of her child. They have learned something of the anatomy of their own bodies, how the fetus grows, and the principle of birth control. As a result, the babies are being born with a better start in life. Fewer babies were born the past year than in any preceding year–97 as compared with 119 in 1932. The figures for the various national groups are as follows:
Births by Nationality
| Filipino | Japanese | Others | |
| Number born alive 1932
Number born alive 1933 |
49
41 |
60
40 |
10
16 |
Birth rates have not been determined, because population figures are not yet available. It appears that the birth rate for the Japanese has dropped appreciably, but probably not for the Filipinos, since a number of women, some of whom were known to be pregnant, returned to the Philippines.
Kindergarten:
The kindergarten children were weighed and measured each month during the school year by the Health Center staff and their minor ailments cared for by the plantation nurse. The percentage of children who are 7% or more under average weight is very high–more than double the number of such children in the free kindergartens of Honolulu. The incidence of dental decay is 100 percent. It is exceedingly difficult, if not impossible, to overcome by diet the effect of toxin produced by infectious processes in the body. It cannot be expected that much can be done in a nutritional way with the kindergarten children as a group until the abscessed teeth are extracted and diseased tonsils removed.
A lunch consisting of milk, poi and fruit was prepared daily by the Health Center staff and served to the kindergarten children at a price of 75 cents per month per child. Enrollment for the lunch was voluntary. On June 1st 101 of the 175 children enrolled in the kindergarten were taking the lunch. The cost of food and incidentals was covered entirely by receipts for the lunch.
School:
The Ewa School Staff, under the leadership of the principal, Miss E. Kellogg, has shown unusual interest in the Health Project, and has given generous and untiring cooperation in the extension of the work through the school. A new system of record keeping was developed–each child’s health record for the entire year being recorded on a single card.
Findings were compiled monthly for each class and for the entire school. During the past year a homemaking class was started for the 8th grade girls, and a garden project, made possible by the plantation management, by the Smith-Hughes and 8th grade boys. A series of illustrated talks on nutrition and health were given to the school children of the five upper grades by the health project director, and special talks and demonstrations to the senior girls. Dr. Muriel Cass gave two talks to the 8th grade girls on the problems of girls. She received from them in writing more than 100 questions, which she attempted to answer.
A “preventorium” class made up of the under-par children from the first three grades was organized in March. They receive special food and rest. One class was formed entirely of first grade children. They had the benefit of the services of the school dentist, who removed all their abscessed teeth. Their improvement as a group even in the short period of time was most extraordinary. It is planned that the school will be classified first of all on a health basis and preventorium classes formed in as many grades as possible next year. A self supporting dental clinic is also being arranged for next year.
Adult Classes:
It was planned that the mothers of the children in the preventorium classes should be kept informed of the progress made by their children, and mothers’ meetings were held in the school auditorium each month. Talks and demonstrations and cooking lessons were given. These classes were conducted by the home-making teacher and health project director. A cooking class for adults (Filipinos) was organized and is being conducted during the summer months by the home-making teacher under the auspices of the Smith-Hughes work. Two illustrated talks were given to the mothers of the kindergarten children by the health project director.
Summer “School”:
The sharp setback that health work almost invariably experiences during the vacation prompted the continuation of the “preventorium” classes during the summer months. Children in these classes and the kindergarten children who desire to do so go to the school daily and eat their lunch. They are then told a story and after that allowed to sleep for an hour. The school cooperates by permitting the use of cafeteria equipment. The cost of food is borne by the children. Local teachers volunteered services.
Ewa Health Center–A Demonstration Center for Health Education in Hawaii:
Visitors to the Health Center became so numerous that it was decided to devote one day each week to educational work for schools and other organizations of Honolulu and Oahu. Since January 1st a formal demonstration and health talk has been given each Wednesday by the health project director at the Health Center. The following schools and organizations have sent representatives:
McKinley High School: Teachers
Washington Intermediate School: Teachers
Kalakaua Intermediate School: Teachers
Central Intermediate School: Teachers
Leilehua Intermediate School: Teachers
Kamehameha Girls School: Teachers and senior students
Ewa School: Entire teaching staff and senior students
Kawananakoa School: Teachers
St. Mark’s Mission: Teachers
School for Deaf and Blind: Teachers
Board of Health (Territorial): Public Health Nurses
Palama Settlement: Nursing staff
Queens Hospital: Supervisors and senior student nurses
Free Kindergarten Association of Honolulu: Superintendent and principals of kindergartens
University of Hawaii: Home Economics students and others
Junior League of Honolulu
Dental Hygienists of the public schools.
In addition to the demonstrations and talks given at the Health Center, the director was invited to address groups in Honolulu and other parts of the island on various aspects of the health project. Since January 1, 1933, talks have been given before the following groups and organizations:
Annual meeting of the Territorial Medical Association (with Drs. Larsen and Pritchard).
Annual meeting of the Territorial Nurses’ Association.
Annual meeting of the Free Kindergarten and Children’s Aid Association.
McKinley High School faculty.
Kawananakoa School faculty.
Kamehameha School faculty and students (two talks).
August Ahrens and Waipahu Schools Parent-Teacher Association.
Palarria Settlement nursing staff.
Queen’s Hospital nursing staff.
Pan-Pacific Club (two talks).
Pan-Pacific Women’s Association.
Lions Club.
Filipino Club.
Exhibit:
An exhibit of the Ewa Health Project showing both the scientific and clinical aspects of the work was prepared for the Centennial Dental Congress which is to be held in Chicago, August 7-12. This meeting is international in scope and the largest undertaking of its kind ever attempted. Illustrations of some of the charts and posters prepared are included herewith (pages 21, 22, 23, 24). In addition, plaster models of the mouths of about 90 of the plantation kindergarten and school children, which were prepared by Drs. Hoey and Pritchard of Honolulu, who are collaborating on the scientific aspects of the work, were sent. These show in a striking manner the kind and extent of tooth decay and mutilation of jaws suffered by the children. These models (about 150 prepared to date) are of very great scientific value and will serve not only as a permanent record of conditions, but as a “yardstick” by which progress may be measured.
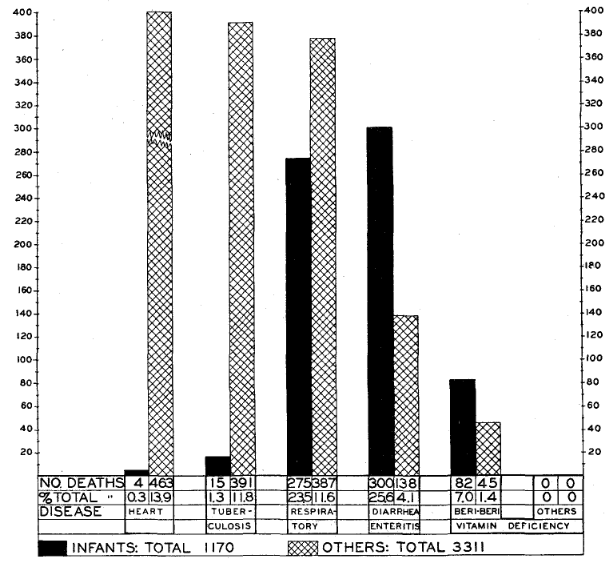
Mortality From Certain Diseases, Territory of Hawaii
Visitors:
There have been more than 450 visitors to the Health Center during the past year. All the islands of Hawaii have been represented, as well as many states on the mainland and foreign countries. Perhaps the best known visitors were Dr. and Mrs. George Bernard Shaw. Much favorable publicity was given the project by their account of it which was reported from Hilo in one of the Honolulu papers. Considerable interest in the project has been shown by the Army and Navy people. Among the more prominent who visited the Health Center were Mrs. Watts, wife of Admiral Watts, and Mrs. Mallison, wife of Commander Mallison.
Publications:
In addition to the four papers published previously, three have appeared recently in the following scientific journals:
Journal of the American Medical Association, November, 1932.
American Journal of Diseases of Children, April, 1933.
Journal of the International Association for Dental Research, June, 1933.
Several other papers are in the course of preparation.
Correspondence:
The director of the Health Project serves as project director for a study of food in relation to teeth and health of peoples throughout the Pacific area under the auspices of the Pan-Pacific Women’s Association, and through this medium has correspondence and contact with many organizations. It is expected that conferences at which the work in Hawaii will play a conspicuous part will be held in various cities throughout the mainland during the trip of the director, which has been planned primarily for the Centennial Dental Congress to be held in Chicago in August.
Economic and Other Aspects of the Health Project:
“How much more does the present system cost the Plantation Company than the old one, disregarding benefits?” is a question that is frequently asked, and is of importance to those contemplating similar undertakings. To arrive at such a figure it would be necessary to include all expenditures of the present project and deduct from same the salaries of the three nurses who previously worked outside the hospital; the wages of matrons and maintenance costs of the day nurseries; a considerable portion of the doctor’s time which was formerly devoted to clinics and care of sick children and other medical services and supplies which are now not required.
The cost of sickness to the plantation is difficult to evaluate in dollars and cents. It is infinitely more than appears in the cost of medical service. Sickness of any member of the family, from the baby to the mother, usually means days of labor lost by the father. To take care of a certain percentage of days of labor lost because of illness, the plantation must necessarily house and maintain a larger number of laborers. A death means a funeral and many days of labor lost on the part of relatives and friends. A baby dead of beriberi means that every member of the family is probably under par physically. Money that is needed for food is spent for funeral services. Rice is cheap and the family eats more of this and less of the more expensive protective foods. The efficiency of the father and the family income decrease. Sickness and discontent increase. A new baby arrives and perhaps there is another funeral. The cost of housing the family and of medical care overbalances the value of the few days of labor the father is able to render. The plantation cannot afford to keep them. They are a problem and ultimately become a burden on the community. Records already available will show many such family histories in Hawaii. If an effort were made to analyze and interpret such records in the light of present-day knowledge, it is more than probable that health education on the plantations of Hawaii would rate as one of the greatest labor and money-saving devices.
Food Costs:
The question of the cost of food that is served the kindergarten children and health center babies is a frequent one. The lunch consisting of poi, canned milk and fresh fruit which is served the kindergarten children on school days (five days a week) costs approximately 75 cents per month per child. This expense is covered entirely by parents. The per capita cost of food furnished the babies enrolled in the Health Center has averaged approximately $2.00 per month, of which parents have paid $1.50. The cost of food could have been appreciably reduced with little or no reduction in quality by using canned milk entirely, instead of half fresh and half canned as was done. Approximately $1,500.00 could have been saved in this way and the total cost of food reduced from $4,300.00 to $2,800.00 (roughly). In other words, with canned milk at the present price, fees paid by parents would cover the entire cost of food and half the wages of the matrons.
Milk:
Interesting and probably significant facts have been brought out by the health project in regard to the use of cow’s milk in infant feeding. It contains three times as much calcium and seven times as much phosphorus and more vitamins–the factors that are claimed by many to determine the quality of the tooth structure–as normal woman’s milk, yet cow’s milk in abundance, in the cases studied, did not increase the growth rate, or decrease incidence of tooth decay when grain foods were used as the carbohydrate supplement. When poi and sweet potato were used instead of grain foods to supplement the cow’s milk, there was an increase in growth accompanied by a sharp drop in the incidence and extent of tooth decay. See Chart I. The high incidence of tooth decay in certain groups who use cow’s milk in generous amounts, and the freedom from decay of the Samoan babies and children who use none at all, show clearly that it will not solve the problem of dental decay in Hawaii. The value of cow’s milk as a food is unquestioned. It is superior in infant feeding to an inferior quality of woman’s milk. Canned milk is cheap, compared with the price of fresh, and is entirely satisfactory as it is used at the Health Center. Orientals and Filipinos who have never been accustomed to use milk, as a rule, prefer the canned to the fresh.
Taro and Sweet Potato versus Grains in Hawaii:
For hundreds of years taro and sweet potato were the principal carbohydrate foods of the people of Hawaii. They were famed for their large stature, their splendid physique and beautiful teeth. Grain foods were introduced by visitors and during the past 50 years have gradually replaced taro and potato in the diet of the native people. Associated with this change is marked physical deterioration; high infant mortality; high susceptibility to disease of all kinds and teeth ravaged by decay. In 1932, the people of Hawaii consumed 94,305,472 pounds of rice, in addition to 27,628,959 pounds of wheat and other grains. About 3,350,000 pounds of rice were grown locally. Millions of dollars are going out of the Territory annually for food–a food which, according to all available evidence, is a prime factor in undermining the health of the people. What would it mean to the Territory if one third of the rice now consumed could be replaced by potato and taro which are “home grown”? It would create a new industry; give employment to the people; keep more money in circulation at home; improve community health and decrease welfare expenditures. Every potato eaten in Hawaii not only helps the individual who eats it but the community. Ewa Plantation Company is in a position to stage a demonstration, the economic and social value of which to the entire Territory, as well as to its own people, cannot be estimated.
It was said two years ago that it was impossible to teach Orientals and Filipinos to eat poi. Our answer to that is that there are now more than 850 children at Ewa who eat poi every day. The demand for sweet potato exceeds the supply.
The “Health Council”:
It is impossible to make a radical change in the habits of a community unless those who contact the people in an official capacity have a sympathetic understanding of what is being attempted, and throw the weight of their influence on the side of the change. It is only by studying situations, determining facts, analyzing and discussing findings with a view to improvement that progress can be made. With this in mind, the plantation “health council” consisting of the manager, doctor, project director, nurses, social worker, school principal and kindergarten director from the plantation, and Dr. N.. P. Larsen, representing the Queen’s Hospital, was planned. One meeting has been held. A smaller group, consisting of the plantation doctor, project director and nurses, planned to meet once each week.
The “Research” Council:
Regularly, since the project was started more than three years ago as a research undertaking under the auspices of the Queen’s Hospital, weekly conferences have been held at “The Queen’s” by Dr. N. P. Larsen, Dr. George Pritchard and the project director. As facts are obtained, the figures are compiled. An effort is made to analyze the findings; to make corrections where they seem to be indicated, and to apply the results, where possible, to community problems. In this way, the returns from “research” are immediate and exceedingly practical.
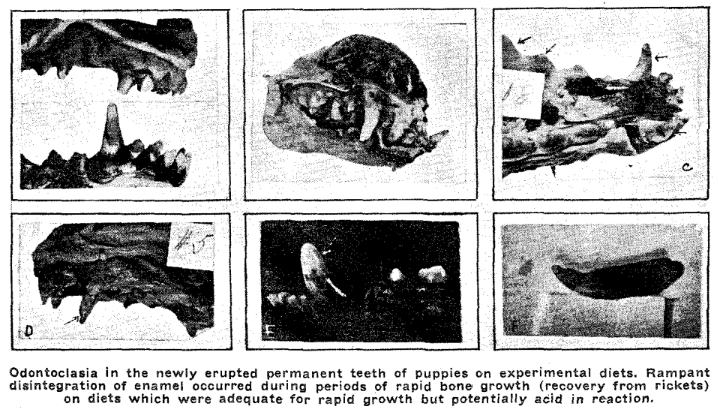
Medico-dental-social-economic Research:
The Ewa Health Project is the clinical application of at least twelve years of medico-dental research. Its ramifications include already social and economic aspects which may be far-reaching in significance. An analysis of conditions as they used to exist in Hawaii and as they are today and the interpretation of the findings in the light of scientific knowledge and animal experiments lead to the conclusion that a return to the type of diet employed by the ancient Hawaiians will automatically solve many of the economic-health-social problems of the community. A basic principle of nutrition which has to do not only with health, but life itself, is involved.
Can grain-eating people from foreign lands be induced to eat native foods–particularly taro and sweet potatoes? They have to be taught. When doctors, nutrition teachers, cafeteria directors, social workers and those who have to do with the feeding of others accept the fact that taro and potatoes have a very special value in the diet in the tropics and are not interchangeable with grain foods, much progress will be made. It is a new idea and has to be demonstrated. Ewa is staging the demonstration, and is doing it in an ideal way–the people making the demonstration pay and profit; the plantation profits; the community profits; the world and the millions of people yet to be born will profit.
Acknowledgments:
Many people have had a part in the making of the Ewa Health Project. The success to date is due in a large measure to the interest and cooperation of the plantation management and medical staff. The innovations started in the Ewa School succeeded as they did because the school principal, Miss E. Kellogg, Theodore R. Rhea, director of health education, Territorial Public Schools, supported by many of the teachers, “put it over.” Special mention should be made of the Health Center workers, whose interest in the work is a genuine one, and who leave nothing undone that might help to advance it.
Martha R. Jones, Ph.D.
Editor’s note: Since the era in which this article was written, society’s understanding of respectful terminology when referring to ethnic and cultural groups has evolved, and some readers may be offended by references to “Orientals” and other out-of-date terminology. However, this article has been archived as a historical document, and so we have chosen to use Jones’ exact words in the interest of authenticity. No disrespect to any cultural or ethnic group is intended.