
Access to all articles, new health classes, discounts in our store, and more!
The Improvement in Renal Function Following EDTA Chelation and Multivitamin Trace Mineral Therapy: A Study In Creatinine Clearance
Published in Medical Hypotheses, Vol. 15, No. 11, pp. 301-304, November 1984.
* * *
Abstract
One of the most commonly alleged contraindications to the use of (ethylene diamine tetraacetic acid) chelation therapy is possible renal damage. In this experiment, 13 subjects with chronic degenerative disorders and with renal damage were treated with infusions that included EDTA, vitamins, minerals and oral supplements. Following 10 and 20 infusions, creatinine clearance significantly improved. This report adds credence to the findings of those physicians who have noted that EDTA is a safe and major therapeutic modality in the treatment of chronic cardiovascular diseases. The patients reported in this experiment represent a small part of a much larger group of several hundred individuals undergoing a series of tests to determine the utility of EDTA therapy in subjects with occlusive vascular disorders.
Introduction
The utility of chelating agents, and particularly EDTA, has been known for several decades. One of the major criticisms to its use has been the possible deleterious effects upon renal function. The purpose of this experiment is to examine the influence of EDTA plus supportive multivitamin-trace mineral supplementation upon kidney function in humans as judged through a study of creatinine clearance. A recent search conducted by Dialog Information Services showed no previous citations are present in the medical literature.1
More specifically, this study was undertaken to gather serial data on several hundred patients with occlusive vascular disorders who were undergoing chelation therapy. The data on creatinine clearance was gathered to ascertain the validity of the charges of critics regarding the alleged toxicity of EDTA. Their concern is based on reports in the scientific literature in the 1960’s when the dosage of EDTA was two or three times the 3.0 gm dosage recommended by the Food and Drug Administration in 1970.2 The toxicity issue has been largely an American one because EDTA has been widely used in Europe and Japan where over 18 million persons have been so treated.3
Reports in the United States literature by Emmerson,4 Casdorph5 and McDonagh, Rudolph and Cheraskin6,7 have shown that chelation therapy is not nephrotoxic but, in fact, improves kidney function. These reports have dealt with studies of creatinine clearance, serum creatinine, and blood urea nitrogen.
Despite such observations and the widespread use of the synthetic amino acid in other parts of the world, Jones of the American Medical Association stated recently: “It can cause renal tubular necrosis and renal failure) permanent renal damage…”8
Halstead has maintained in a critical review of the reports on nephrotoxicity both in experimental animals and humans that, in most cases, excessively high doses were used and concluded, “…when EDTA chelation therapy is properly administered by a well trained physician and nursing staff, it is one of the safest major therapeutic modalities available in the chronic degenerative disease armamentarium.”9
Materials and Methods
This ongoing study reports on the first 13 patients with poor creatinine clearance who completed 20 EDTA infusions and multivitamin-trace mineral supplementation. After developing a unique problem-oriented record system and establishing clinical protocols, tests were made at baseline and intervals following 10 and 20 infusions over a period of 90 to 160 days. A total of over 300 patients with a variety of occlusive vascular disorders are involved in this study. The 13 in this group are characterized by obvious poor creatinine clearance.
The most common vascular disorders classified were coronary artery disease and arteriosclerosis. The criteria used were established in 1980 by the United States Department of Health and Human Services, Public Health Service–Health Care Financing Administration.10
Our studies were designed to gather data consistent with the testing recommendations proposed for physicians who belong to the American Academy of Medical Preventics.11 In addition to the creatinine clearance, other serial observations are being prepared on blood pressures of arms and legs, exercise tolerance, and medication requirements. Treatment for this study consisted of providing 3 gm of EDTA plus multivitamin-trace minerals in an intravenous infusion that lasted approximately four hours and was given twice weekly. Daily oral vitamin-trace mineral support was given throughout the therapy. All patients were placed on a high bulk, nutritionally balanced diet.
Creatinine clearance tests were done by Metpath (Corporate Headquarters, One Malcolm Avenue, Teterboro, New Jersey 07608), a fully licensed federally-approved laboratory that conducts clinical pathology and chemistry testing in a large number of cities across the nation. Samples were obtained using the Metpath standard protocols.
Results
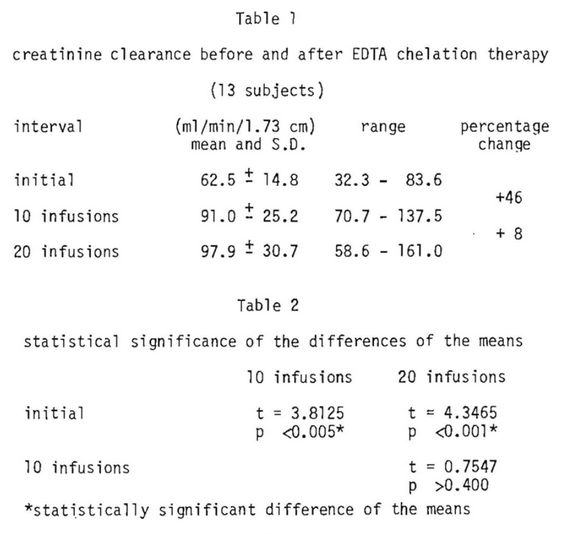
Table 1 outlines the mean and standard deviation for creatinine clearance initially and following 10 and 20 infusions along with the range of values and the percentage differences. It is abundantly clear that creatinine clearance improves significantly (a matter of 46 percent) following 10 infusions. Within the limits of this study there is an additional 8 percent increase in creatinine clearance between 10 and 20 infusions. The significance of this information is outlined in Table 2. There is a statistically significant difference following 10 infusions and more so following 20. There is no significant difference in observations made between the 10th and 20th infusions.
Discussion
Creatinine is an endogenous end product of muscle metabolism. It is generated at a fairly constant rate and is cleared primarily by glomerular filtration. Creatinine clearance is a practical measure of glomerular filtration readily available to the practicing clinician. Under presumably normal conditions, creatinine clearance is approximately 140 liters per 24 hours or approximately 100 milliliters per minute.12
Within the limits of this study, creatinine clearance approaches the optimal (100 ml/min/1.74 c.) following chelation therapy under the conditions outlined in this report. The findings are consistent with those of others who have examined the problem. Casdorph made the statement, “In fact, two patients have shown improvement in creatinine clearance during the course of chelation therapy, raising the possibility that this form of treatment may even improve renal function in some patients.”5
References Cited:
- Terrell, W., LINE, Inc., Personal Communication, December 1983.
- Federal Register, January 13, 1970, p. 586.
- Walker, M. Chelation Answer. 1982. New York, M. Evans. p. 89.
- Emmerson, BT. “Chronic lead nephropathy.” Kidney Int. 4: 1, 1973.
- Casdorph, HR. “EDTA Chelation Therapy II, Efficacy in Brain Disorders.” J. Hol. Med. 3: 115, 1981.
- McDonagh, EW., Rudolph, CJ. and Cheraskin, E. “The effect of EDTA chelation therapy plus supportive multivitamin-trace mineral supplementation upon renal function: A study in serum creatinine.” J. Hol. Med. 4: #2, 146-151, Fall/Winter 1982.
- McDonagh, EW., Rudolph, CJ. and Cheraskin, E. “The effect of EDTA chelation therapy plus supportive multivitamin trace mineral supplementation upon renal function: A study in blood urea nitrogen.” J. Hol. Med. 5: #2, 163-171, Fall/Winter 1983.
- Jones, RJ. “Chelation therapy.” JAMA 250: 672, 1983.
- Halstead, BW. The Scientific Basis of EDTA Chelation Therapy. 1979. Colton, California, Golden Quill Publishers, p.84.
- International Classification of Diseases, 9th Revision DHHS Publication Number (PHS) 80-1260. Superintendent of Documents, U. S. Government Printing Office, Washington, D.C. 20402.
- Clinical Protocols, Science Committee, American Academy of Medical Preventics. 6151 W. Century Blvd. Los Angeles, 1983.
- Frackelton, JW. Personal Communication., October 1983.