
Access to all articles, new health classes, discounts in our store, and more!
Epilepsy and the Cortisone Glucose Tolerance Test
Published in The Journal-Lancet, Vol. 83, No. 6, June 1963.
* * *
The justification for the study of carbohydrate metabolism in epileptic patients has been described by many investigators and is succinctly summarized in the following quotation:1
“…The possibility that there may be abnormality in carbohydrate metabolism in persons subject to convulsive disorders is suggested by the fact that convulsions and increased irritability of nerves accompany hypoglycemia produced by insulin in animals, by the reported marked diminution in glycogen content of the brain accompanying convulsions, and by the occasional clinical reports of patients who seemed to be better or worse following variation in the carbohydrate content of the diet.”
The lack of a significant relationship between carbohydrate metabolism and convulsive seizures is summarized in the following statement:2
“… Aside from variability of results in initial and also in repeated measurements, it seemed that glucose played only a passive role with respect to convulsions. Among some 100,000 total admissions to Harriet Lane Home in Baltimore, there were only 15 with convulsions ascribed to hypoglycemia. Three were diabetic and two had adenoma of the islet. None of the 3,000 epileptic children whose blood sugar was measured had hypoglycemia.”
It might well be that there is no cause-and-effect relationship between carbohydrate metabolism and convulsive seizures. On the other hand, significant relationships may indeed exist which have not been demonstrated for one or more reasons. First, most of the presently published studies have assumed that the present ranges for physiologic blood sugar and blood glucose are correct. This may well be a source of error since there is some evidence to indicate that physiologic blood sugar and glucose may embrace a much narrower range than is presently held.3-6 Second, different results may be obtained through different methods for measuring carbohydrate metabolism. For instance, blood sugar and glucose may be determined fasting, postprandially, or under tolerance conditions.
There are recent reports which claim that the cortisone-glucose tolerance test may be a more delicate barometer of carbohydrate metabolism than any of the presently employed procedures. By this means, the prediabetic subject may be more readily detected than by the classical glucose tolerance procedure.7-8 Epilepsy has been studied in terms of fasting blood sugar and the classical glucose tolerance test.1 No published reports are available to show the diagnostic utility of the cortisone-glucose tolerance test in the detection of early or subtle hypoglycemia, or both. Also, as far as possible, there appears to be no report on the relationship of the cortisone-glucose tolerance procedure and convulsive seizures.
This report, therefore, is designed to outline the cortisone-glucose tolerance test findings in comparable groups of unequivocally epileptic (grand mal) versus nonepileptic patients.
Method of Investigation
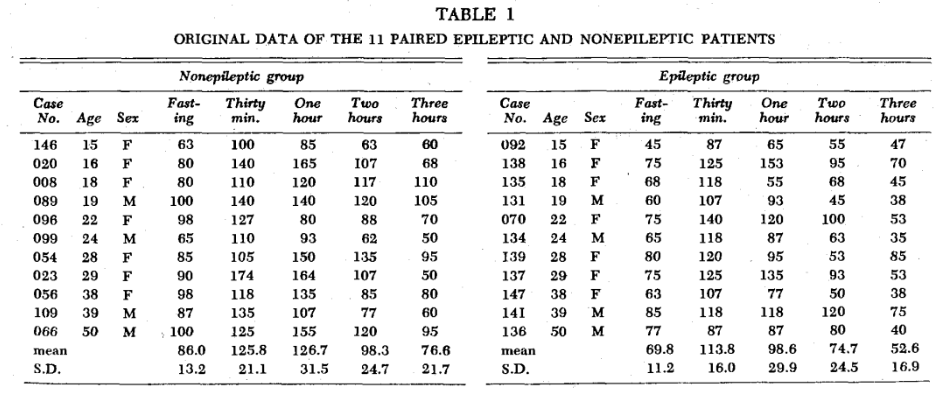
During the course of study of the correlation of stomatologic findings and the cortisone-glucose tolerance test in 170 subjects,10 11 confirmed epileptic patients from the Department of Neurology of the University of Alabama Medical Center were examined. These subjects ranged in age from 15 to 50 and included 4 men and 7 women. It was possible to pair each epileptic patient with a nonepileptic subject of the same sex and age (table 1). The cortisone-glucose tolerance test was performed according to the Conn technic.11
Results
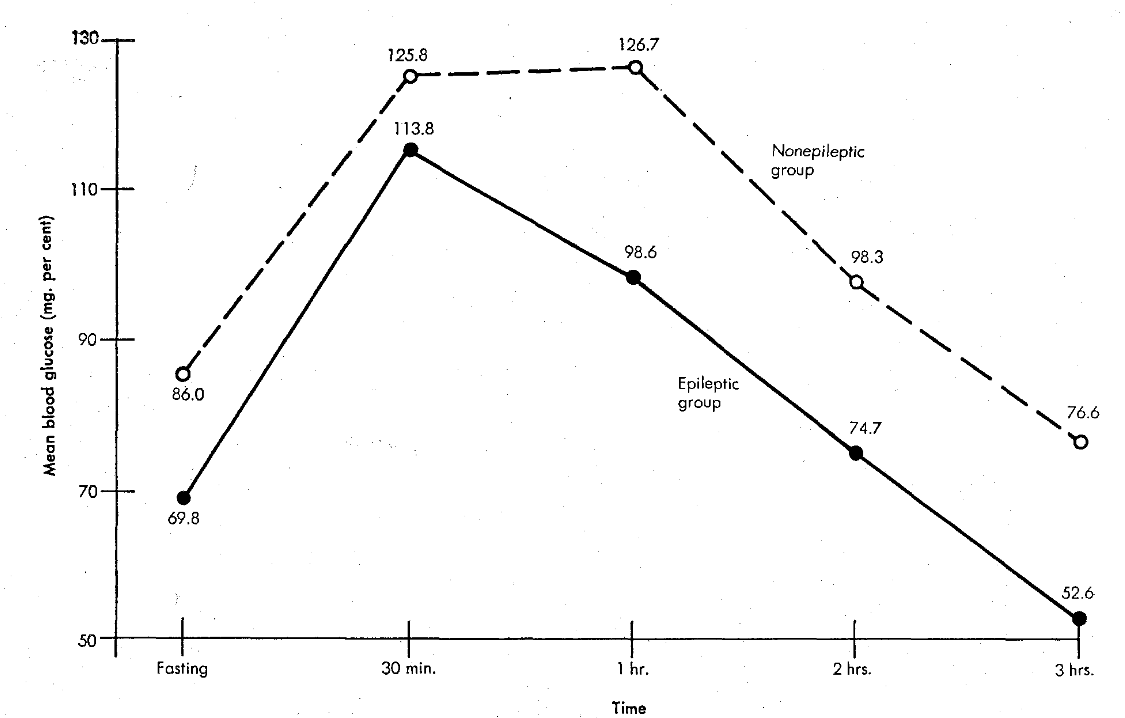
Table 1 summarizes the data obtained for the 2 groups. The figure shows in graphic form the mean blood glucose levels, initially, at thirty minutes, and at one, two, and three hours. It is noteworthy that, at every temporal point, the mean blood-glucose scores were lower in the epileptic group. The differences of the means at each temporal point are significant in every case but the thirty-minute determinations:
| P | |
| Fasting
Thirty minutes One hour Two hours Three hours |
<.01
>.10 <.05 <.05 <.01 |
Comparison of cortisone-glucose tolerance test in 11 paired epileptic and nonepileptic patients
Discussion
There are 3 points which deserve special consideration. First, there is every reason to believe that, if the cortisone-glucose tolerance test is a more delicate barometer of hyperglycemia, then it might also be a sensitive indicator of hypoglycemia. At least, in the light of present information, there is nothing to negate this hypothesis. For this reason, it was thought of interest to study the cortisone-glucose tolerance pattern in patients with and without convulsive seizures. Second, regardless of the standards accepted for the physiologic range for blood glucose, the cortisone-glucose tolerance pattern in the epileptic and nonepileptic patient is significantly different.
All that has been demonstrated here is a statistically significant correlation. True, variable A (blood glucose) is related to variable B (epileptic state). This cannot be interpreted to mean that A causes B. It is just as possible that B causes A. Or, it is likely that both A and B may be the result of a third variable (C).
An attempt is now being made to determine whether a cause-and-effect relationship exists by subjecting patients with convulsive seizures to a diet (low refined carbohydrate, high protein) known to produce a more physiologic carbohydrate metabolic state.12
Summary
The general consensus, at the present time through studies of fasting and nonfasting blood sugar and blood glucose, is that there is no relationship between carbohydrate metabolism and epilepsy of the convulsive type.
As far as can be determined, no study of carbohydrate metabolism in the epileptic patient has been done by means of the cortisone-glucose tolerance test.
This study consists of an analysis of the cortisone-glucose tolerance test findings in 22 patients paired with respect to age and sex and including 11 epileptic and 11 nonepileptic individuals.
The findings show significantly lower blood glucose levels at every temporal point except the thirty-minute determinations in the epileptic group.
References Cited:
- Lennox, W. G., and Bellinger, M.: “Studies of metabolism in epilepsy. The blood sugar curve.” Arch. Neurol. Psychiat. (Chic.) 18:395-413, 1927.
- Lennox, W. G., and Lennox, M. A.: Epilepsy and related disorders. Boston: Little, Brown & Co., 1960, vol. 2, p. 643.
- Ringsdorf, W. M., Jr., and Cheraskin, E.: “Physiologic fasting blood glucose: range or point?” Dent. Med. 16:96-99, 1961.
- Cheraskin, E., and Ringsdorf, W. M., Jr.: “Stomatology and clinical chemistry.” Dent. Rev. 9:1-8, 1961-1962.
- Ringsdorf, W. M., Jr., and Cheraskin, E.: “Physiologic glucose tolerance test.” Progr. 2:281-284, 1962.
- Ringsdorf, W. M., Jr., and Cheraskin, E.: “Physiologic cortisone-glucose tolerance test.” Med. Ass. Ala. 31:359-362, 1962.
- Conn, J. W.: “The prediabetic state in man.” Diabetes 7:347- 357, 1958.
- Fajans, S. S., and Conn, J. W.: “The early recognition of diabetes mellitus.” N.Y. Acad. Sci. 82:208-218, 1959.
- Lennox, W. G., O’Connor, M., and Bellinger, M.: “Studies of metabolism in epilepsy. II. The sugar content of blood.” Neurol. Psychiat. (Chic.) 18:383-394, 1927.
- Ringsdorf, W. M., Jr., Cheraskin, E., and Keller, S. M.: “The physiologic cortisone-glucose tolerance pattern: the development of blood glucose by an analysis of oral symptoms.” Dent. Res. 41:833-839, 1962.
- Fajans, S. S., and Conn, J. W.: “An approach to the prediction of diabetes mellitus by modification of the glucose tolerance test with cortisone.” Diabetes 3:296, 1954.
- Page, M. E., Ringsdorf, W. M., Jr., and Cheraskin, E.: “The effect of a low-refined-carbohydrate high-protein diet upon nonfasting blood sugar.” Revy 12:1-24, 1961.