
Access to all articles, new health classes, discounts in our store, and more!
Predictive Medicine IV. The Gradation Concept
Published in Journal of The American Geriatrics Society, Vol. 19, No. 6, 1971.
* * *
ABSTRACT: In the traditional philosophy of medicine, a diagnosis usually is made only when a set number and constellation of signs and symptoms prevail. Hence, when there is a long and tortuous incubation period, clinically and biochemically, the disease may remain either undiagnosed or labelled as an ill-defined psychologic syndrome. Sensitivity to clinical and biochemical changes is an integral part of predictive medicine.
“Health and disease are not absolutes, but occur in a spectrum ranging from perfect health to death.” “The time has come to speak in terms of percentage of disease.” – T. S. Danowski
Among the unique features of predictive medicine are the recognition of the multifactorial nature of health and disease and the identification of the factors which contribute to host resistance and susceptibility.1 This report concerns another singular feature of predictive medicine, i.e., that health and disease, which may be pictured in an achromatic series as white and black, are limiting poles; an infinite number of shades of gray are interposed between the limiting endpoints. It is in this gray area that predictive medicine finds justification in the anticipation rather than simply the identification of disease.
The Course of Disease
All disease is preceded by an incubation period. In acute mechanical trauma (e.g., an automobile accident), the incubation time is brief and not too important. In acute infection (e.g., measles), the incubation period is somewhat longer (approximately ten days) and somewhat more significant from a prognostic standpoint. In chronic disorders (e.g., myocardial infarction, cerebrovascular accident, rheumatoid arthritis, periodontal disease), the incubation time extends over months, years or decades. The longer the incubation period, the greater the opportunity to anticípate the end-problem and to abort the process. Primary prevention (prevention of occurrence) requires analysis of the sequence of events in the development of classical disease syndromes.
Initially, the patient notes only a few, seemingly unrelated findings. There may be irritability, for example associated with leg cramps. Because these apparently unrelated symptoms and signs do not fit any textbook description of a particular disease, the complaints are either ignored, assigned a meaningless label, or regarded as a minor psychic problem. The latter diagnosis is frequently made by exclusion, i.e., failure to relate the signs and symptoms to classical disease nomenclature. At this stage, as shown in Figure 1, the clinical picture is represented by the form on the left.
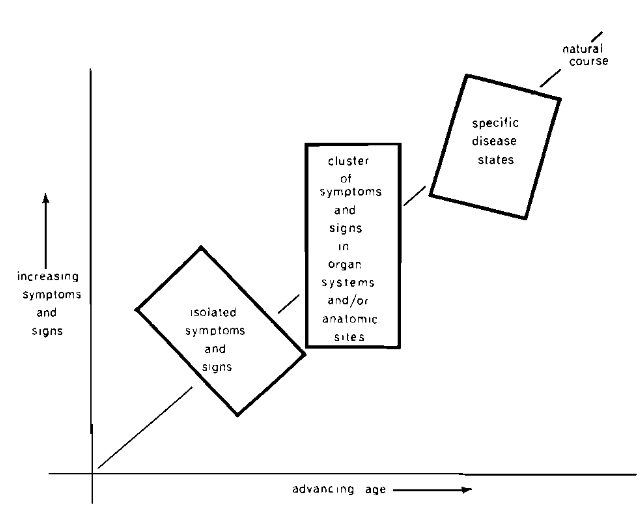
Fig. 1. The clinical sequence of events in chronic disease. At first, there are few and diverse symptoms and findings (left box). With time, the findings become more numerous and localized in a system or organ (middle box). Finally, the clinical evidence fits the textbook picture of a particular disease or syndrome (right box).
If the situation continues, then the symptoms and signs multiply. Sooner or later, they become referable to systems, organs or localized sites. For instance, the subject may have several gastrointestinal complaints (e.g., indigestion, anorexia, and hemorrhoids). At this stage, the constellation is still not classifiable according to textbook terminology. Hence, treatment is usually symptomatic, or the patient is simply placed under observation. If many organ systems and/or anatomic sites are involved, the diagnosis may be “psychologic disturbance,” as represented by the center form in Figure 1.
When, however, the syndrome can be clearly identified in terms of its classical description, then the illness is assigned a label (represented by the form on the right in Figure 1). Even at this stage, the interrelationships between several existing diseases are frequently overlooked.
The Clinical Course
The foregoing picture can be simply demonstrated.2 Twelve hundred twenty-four presumably healthy female subjects completed the Cornell Medical Index Health Questionnaire.3 Section D, consisting of 23 questions, relates to the gastrointestinal tract. Figure 2 shows age in relation to reported gastrointestinal symptoms and signs (Cheraskin and Ringsdorf, unpublished data). Four points warrant special attention. First, with advancing age, the mean number of gastrointestinal findings increased (2.9 to 3.2 to 3.5). Second, in the oldest age group (70-89 years), the mean number of findings declined (3.5 to 3.1). Third, with advancing age, the variance widened in general. Fourth, in the oldest age group, the variance shrank.
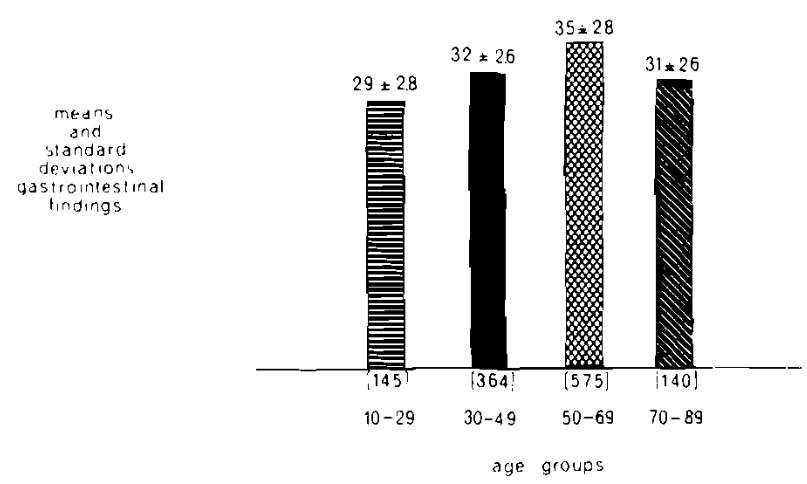
Fig. 2. The relationship of age (abscissa) to the frequency of reported gastrointestinal findings (ordinate). With age, up to a point, the mean number of symptoms and signs increased. After age 70 (the present life expectancy of man), the number of findings declined. With age, up to a point, the variance widened. After the age of 70, the variance declined. (Cheraskin and Ringsdorf, unpublished data.)
These findings are the clinical expression of the pattern in Figure 1 showing the usual course of events in the development of disease states. Initially, the symptoms and signs are relatively few and usually so diverse that the total picture does not lend itself to classical textbook diagnosis (e.g., peptic ulcer). As time passes, the signs and symptoms increase in number and begin to localize in systems and sites. Finally, the constellation fits the classical requirements for a particular disease tag.
The gradation concept is an important and integral part of a predictive medicine program. Awareness of the course of events means that effort can be directed at an early stage to the number and pattern of symptoms and signs, without waiting for the identification of a specific disease syndrome.
The usual graphic portrayal shows that, with advancing age, there is a progressive increase in symptoms and signs (Fig. 3). However, it is usually not emphasized that, with time, there is an increase in variance (the gray area in Fig. 3). Some relatively older people are afflicted with fewer symptoms and signs than other relatively younger subjects. This suggests that the frequent increase in clinical symptoms and signs is not an inevitable part of the aging process. Thus in a predictive medicine program it is important to recognize that much of the clinical picture heretofore ascribed to the physiologic aging process is simply an expression of disease and, in many cases, early pathosis. Moreover, since the course of events is not physiologic, it may be slowed, stopped, reversed, or even completely prevented (Fig. 4). Prevention of occurrence, however, must begin early in life. In reality, most chronic diseases begin in childhood.
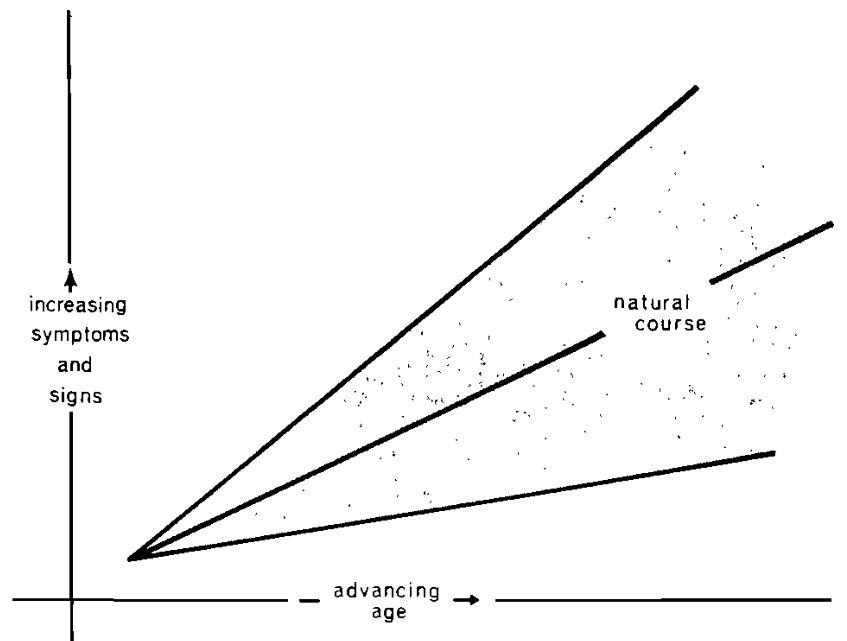
Fig. 3. The usual clinical sequence of events. With time, there is a progressive increase in symptoms and signs (rising center line). However, with advancing age, there is also an increase in variance (widening gray area).
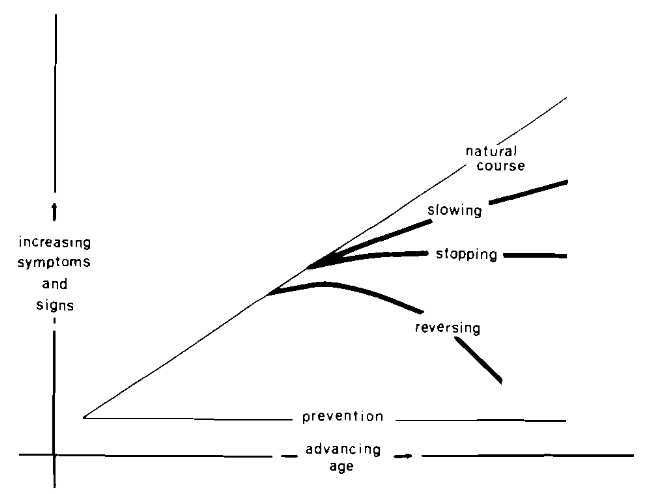
Fig. 4. Five possible clinical events are shown: 1) the clinical course is unchanged: 2) it is slowed; 3) it is stopped; 4) it is reversed; or 5) it is prevented. The ideal is to subtend an angle of zero with real primary prevention (prevention of occurrence).
It is noteworthy that, in the eighth and ninth decades of life (the time beyond the current life expectancy of three score years and ten), both the mean number of findings and the variance decline. This is because those who are still living are the heartiest subjects (survival of the fittest). The very ill have succumbed.
Awareness of this pattern plays a significant role in the philosophy of a predictive medicine program. The healthy young together with these elderly living subjects, representing success, can be employed for the development of norms and standards of health.
The Biochemical Course
The clinical pattern just outlined is not unique. When other indicators of health and disease are examined, the pattern is similar. Figure 5 is a summary of blood glucose values (Dextrostix method) in 6143 presumably healthy female subjects.2 With advancing age, the mean blood glucose scores slowly but progressively rose. Moreover, with time, the variances continued to increase. This suggests that some elderly persons have lower blood glucose levels than have younger people, However, in the very elderly, (as with clinical symptoms and signs), the variance begins to shrink.
Thus, norms established from the healthy young and aged can play a cardinal role in the philosophy of a predictive medicine program. The fact that, in healthy people, biochemical values change very little from birth to death, re-emphasizes the importance of the healthy aged as a group.
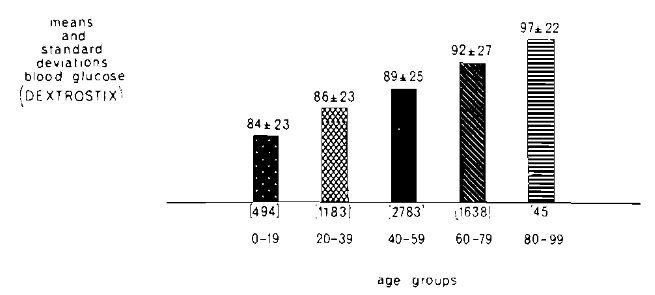
Fig. 5. The relationship of age (abscissa) to the blood glucose level, Dextrostix method, (ordinate). With advancing age the mean values continued to rise. With advancing time, the variances increased. However, in the oldest subjects, the variance declined.
Comment
Sensitivity to clinical and biochemical events is an integral part of predictive medicine. As Danowki and Moses4 so aptly pointed out, it is time to think in terms of 20 per cent of disease X and 40 per cent of disease Y. This approach not only invites the earlier identification of disease but, more importantly, its anticipation and thus an earlier start of therapy for primary prevention.
A report to follow5 will consider another special characteristic of a predictive medicine program.
References Cited:
- Cheraskin, E., and Ringsdorf, W. M., Jr.: “Predictive medicine: III. An ecologic approach.” J. Am. Geriatrics Soc. 19: 505 (June) 1971.
- Cheraskin, E., and Ringsdorf, W. M., Jr.: Unpublished data, Department of Oral Medicine, University of Alabama Medical Center, Birmingham, Alabama.
- Brodman, K.; Erdman, A. J., Jr., and Wolff, H. G.: Cornell Medical Index Health Questionnaire. New York, Cornell University Medical College, 1949.
- Danowski, T. S., and Moses, C., Jr.: “Cholesterol levels reduced by hormone ‘replacement doses,’” J. A. M. A. 181: 17 (Sept. 1) 1962.
- Cheraskin, E., and Ringsdorf, W. M., Jr.: “Predictive medicine: V. Linear versus curvilinear function,” J. Am. Geriatrics Soc. 19. (in press) 1971.