
Access to all articles, new health classes, discounts in our store, and more!
Eating Habits of the Dentist and His Wife: Daily Consumption of Vitamin E
Published in the Journal of the American Geriatrics Society, Vol. XXII, No. 8, August 1974.
* * *
ABSTRACT: An epidemiologic survey of the dietary habits of 369 dentists and 288 wives indicated that about 50 per cent of them consume suboptimal amounts of vitamin E, according to the conservative estimates of the Food and Nutrition Board of the National Academy of Sciences-National Research Council. By means of simple health education measures, it seems possible to increase significantly the consumption of vitamin E and, in association, to reduce reported cardiovascular findings.
There are at least two justifications for studying the dietary status of the dentist and his wife. First, since diet is related to health and disease, a knowledge of diet and its improvement should favor better health. This should be reflected in the dentist’s professional productivity and in the housewife’s general activity. Second, the average physician’s concept of who, among his patients, is overweight is directly related to his own weight. It follows that the dentist’s conception of his patient’s dietary habits and their relationship to general and oral health is likely to be influenced by his own dietary patterns.
This series of reports will analyze the diet of the dentist and his wife. In this study, consideration will be given only to the daily consumption of vitamin E. Particular attention will be paid to the following questions:
- What is the daily intake of vitamin E for the dentist and his wife?
- Can the daily intake of vitamin E be readily changed?
- What is the clinical significance of a change in vitamin E consumption?
Material and Methods
Initially, 369 dentists and 288 wives participated in this study. At present they are taking part in a multitest program conducted in Florida under the auspices of the Southern Academy of Clinical Nutrition, in Los Angeles under the sponsorship of the Southern California Academy of Nutritional Research, in Columbus (Ohio) under the aegis of the Ohio Academy of Clinical Nutrition, in Connecticut under the auspices of the Northeast Academy of Clinical Nutrition, and in the San Francisco Bay area under the supervision of the Northern California Academy of Nutritional Research.
The multitest program includes the periodic measurement of a host of clinical, oral, electrocardiographic, and biochemical factors. One of the unique features of the project is the inclusion of dietary evaluation. This is accomplished in two ways. First, each subject is required to record, according to stated instructions, all food consumed for a seven-day period. The data are subjected to computer analysis, and a printout is obtained showing the daily intake of the major foodstuffs, vitamins and minerals. Second, each participant completes a simple questionnaire based upon the frequency of intake of critical foods. This form is also sent for a computer analysis. A printout showing the daily intake of nutrients is returned. This paper concerns only the daily consumption of vitamin E, as judged by the food-frequency questionnaire.
The results derived were discussed with the membership. The group was shown the daily intake of vitamin E on an individual basis. Discussions were conducted regarding the relationship of health and disease to vitamin E consumption. Finally, the group was shown how to increase the intake of foodstuffs and supplements in order to attain an optimal level of vitamin E consumption.
About a year later, the dietary survey was repeated, as were the other measurements in the multitest program. This has been done on an annual basis, and the information now extends over a four-year period for the same group.
Results
Question 1: What is the daily intake of vitamin E for the dentist and his wife?
Table 1 summarizes the daily distribution of vitamin E in the male subjects at the time of the initial examination. The mean consumption of vitamin E was 67 International Units (I.U.), with a spread from 6 to 218 and a range of 212 I.U. It is noteworthy that 46 per cent of the group consumed less than 30 I.U. daily. According to the Food and Nutrition Board of the National Academy of Sciences,1 the recommended daily intake of vitamin E for the male is 30 I.U.
Table 1–Vitamin E Distribution in the Male Subjects (initial examination)
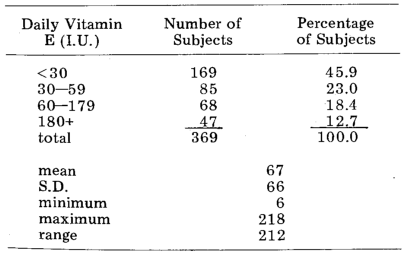
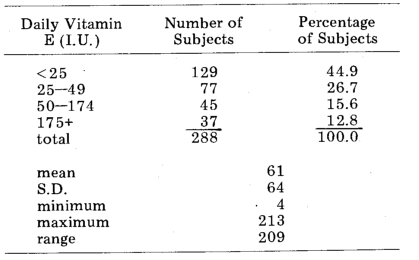
Table 2 summarizes the daily distribution of vitamin E in the female subjects at the time of the initial examination. The mean intake was 61 I.U., with a spread from 4 to 213 and a range of 209 I.U. Forty-five per cent of the group consumed less than 25 I.U. daily. According to the Food and Nutrition Board of the NAS,1 this is the minimal daily requirement for females.
Table 2–Vitamin E Distribution in the Female Subjects (initial examination)
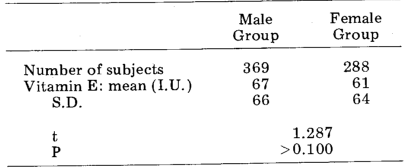
There was no statistically significant difference (t = 1.287, P > 0.100) between the sexes in terms of vitamin E consumption (Table 3).
Table 3–Vitamin E Distribution in Male versus Female Subjects (initial examination)
Comment: This presumably healthy population sample was characterized by persons with a broad range of vitamin E intake, and by a significant number who failed to meet the recommended daily consumption.
Question 2: Can the daily intake of vitamin E be readily changed?
A comparison was made between the intakes of vitamin E before and after the health education lectures. Table 4 shows the initial and the subsequent daily intakes in 84 paired subjects. There was a significant increase in the daily intake of vitamin E–from a mean of 21 I.U. initially, to 51 I.U. and 127 I.U. respectively at the times of the second and third annual examinations.
Table 4–Vitamin E Distribution in 84 Paired Subjects at Three Annual Visits, after Health Education Lectures
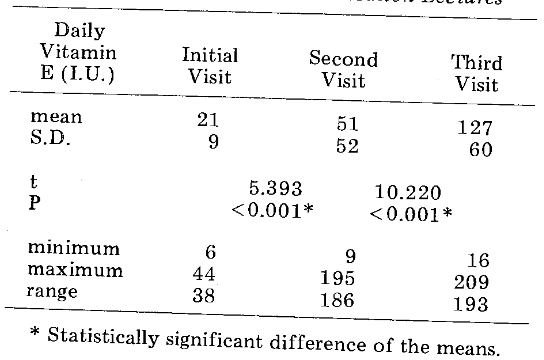
Comment: The daily intake of vitamin E can be significantly increased by the use of relatively simple methods of health education.
Question 3: What is the clinical significance of a change in vitamin E consumption?
Since the clinical and dietary states were re-examined annually, it was possible to compare the changes in cardiovascular symptoms reported on the Cornell Medical Index Questionnaire in terms of changes in the daily intake of vitamin E. It was found that 286 subjects increased their vitamin E intake, whereas 69 chose to decrease it. Figure 1 shows that in group 1 (increased intake) the mean daily consumption of vitamin E rose from 47 to 111 I.U.–statistically significant (t = 17.470, P < 0.001). In this same group, the mean number of cardiovascular symptoms decreased from 1.17 to 0.85–highly significant (t = 4.427, P < 0.001). Group 2 was deliberately selected as comprising those who decreased their vitamin E intake. Figure 1 shows the significant (t = 5.117, P < 0.001) reduction in vitamin E intake from 100 to 79 I.U. daily. There was no significant (t = 1.582, P> 0.100) reduction in cardiovascular findings (from 1.16 to 0.96).
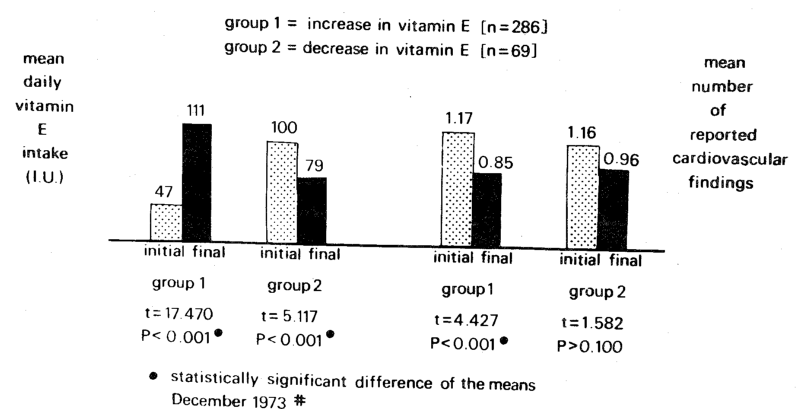
Fig. 1. Effect of changes in the daily intake of vitamin E in terms of changes in reported cardiovascular findings.
The effect of vitamin E seems to be partly a function of dosage. Figure 2 shows data on three groups of subjects. In group 1 the increase in vitamin E intake reached a level lower than 30 I.U. daily, in group 2 the level was between 30 and 60 I.U., and in group 3 it was above 60 I.U. In group 1, the significant increase in vitamin E from 17 to 22 I.U. was not paralleled by a significant decrease in reported cardiovascular findings (1.34 to 0.98; t = 1.826, P > 0.050). However, in group 2 there was a significant (t = 8.248, P < 0.025) rise in vitamin E intake from 23 to 36 I.U. daily, associated with a significant (t = 2.595, P < 0.025) reduction in cardiovascular findings from 1.27 to 0.62. In group 3 there was the most significant (t = 17.452, P < 0.001) rise in daily vitamin E intake from 52 to 150 I.U., and the most significant (t = 3.222, P < 0.005) decline in cardiovascular findings from 1.35 to 0.83.
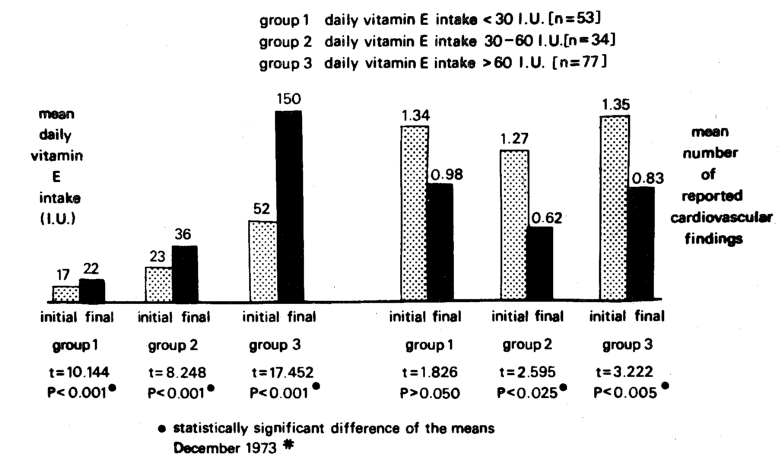
Fig. 2. Effect of changes in reported cardiovascular findings in terms of changes in the daily intake of vitamin E. (In group 1 the increase in vitamin E reached a level lower than 30 I.U., in group 2 it was between 30 and 60 I.U., and in group 3 it was over 60 I.U.)
Comment: Statistically significant parallelisms were observed between changes in the daily intake of vitamin E and reported cardiovascular findings. Moreover, these clinical changes appeared to be dose-dependent.
Discussion
As far as we can determine, this is the first time it has been shown that the dentist and his wife consume suboptimal amounts of vitamin E. The significance of these data remains to be clarified. At least they provide some evidence that cardiovascular status may be a function of the daily intake of vitamin E. Of particular importance is the observation that dosages twice as high as those recommended appear the most beneficial.
It is of interest that the Food and Nutrition Board of the National Academy of Sciences-National Research Council in 1973 further reduced the vitamin E requirements from 30 and 25 I.U. to 15 and 12 I.U. for males and females respectively.2
Our report showing suboptimal consumption of vitamin E is a companion article to an earlier report3 describing the relatively high intake of foodstuffs containing refined carbohydrates.
By simple health education measures, it seems possible not only to reduce the intake of refined carbohydrates, but to increase vitamin E consumption and, in association, to reduce reported cardiovascular findings.
References Cited:
- Food and Nutrition Board: Recommended Dietary Allowances. Publication No. 1694, 7th revised edition. Washington, D.C., National Academy of Sciences, 1968.
- Food and Nutrition Board: Recommended Daily Dietary Allowances, Revised edition. Washington, D.C., National Academy of Sciences-National Research Council, 1973.
- Cheraskin E. and Ringsdorf W. M. Jr.: “What does the dental family eat? A study of refined carbohydrate consumption,” J. Alabama Dent. A. 56: 32, 1972.