
Access to all articles, new health classes, discounts in our store, and more!
Vitamin U Therapy of Peptic Ulcer
Presented before the Section on General Medicine at the 80th Annual Session of the California Medical Association, Los Angeles, May 13-16, 1951. Published in California Medicine, Vol. 77, No. 4, October 1952.
* * *
[Dr. Cheney’s manuscript is not printed here in entirety. Tables giving details of clinical and roentgenographic observations in each of the 100 cases were deleted to save space. The more detailed information will be included in reprints of the article, available from the author.]
Vitamin U, administered as raw cabbage juice to 100 patients with peptic ulcer, was apparently effective in promoting the rapid healing of uncomplicated peptic ulcers. The evidence of therapeutic benefit was (1) the rapid relief of the symptom, pain, without the use of any set plan of symptomatic treatment, and (2) ulcer crater healing time (determined roentgenographically) considerably shorter than in groups of cases, reported in the literature, in which “standard” types of diet and drug therapy were employed.
Results of a number of animal experiments carried out in the medical research laboratories at Stanford University School of Medicine in the past ten years1,2,3,4 indicate that a dietary factor plays some role in the etiology of peptic ulcer. Certain raw foods, particularly green vegetables, contain some substance, termed vitamin U, which prevented the development of histamine-induced peptic ulcers in guinea pigs. This substance is readily destroyed by heat, and may be rapidly destroyed by oxidation. The therapeutic use of vitamin U in the form of cabbage juice in the treatment of a group of thirteen patients was reported in 1949,5 and a further report dealing with the clinical use of this form of therapy was made in 1950.6 The present report consists of an analysis of the therapeutic effect of vitamin U in cabbage juice on the healing of peptic ulcer in 100 patients (including the 13 originally reported upon) who were treated in a period of two and one-half years.
Selection of Patients for Treatment
At first only patients were accepted for this form of treatment who had a readily demonstrable ulcer crater and who were free from such complications as recent bleeding, pyloric obstruction and long-standing symptoms suggesting extensive cicatricial changes. Since many patients who did not meet these qualifications requested cabbage juice therapy, it was decided to accept all patients for vitamin U therapy who had a clearly established diagnosis. In accepting a number of patients with complications, it was recognized that some patients in this group might not be expected to respond satisfactorily to any form of medical therapy, and that operation might be necessary.
Also it was obvious that improvements in the patient’s condition as measured by the time required for an ulcer crater to heal as observed in serial x-ray studies5 would not serve as a satisfactory criterion in all cases because a crater in the duodenum could not always be demonstrated clearly and the progress of a complicated case could not always be followed a sufficient length of time to judge crater healing time accurately. Consequently in a number of cases symptomatic relief of ulcer pain had to serve as the sole criterion of improvement.
As most patients were hospitalized during the first seven to fourteen days of treatment, bed rest alone may have contributed to the development of wellbeing in some instances. Each patient received only cooked (heated) food in the diet during the period of experimental therapy6 and no routine standardized administration of drugs was permitted. However, in the first few days of treatment, drug therapy was used when absolutely necessary for relief of pain or restlessness. Relief of abdominal pain by vitamin U therapy was only judged to have occurred when the use of symptomatic drug therapy was not required and when pain no longer appeared spontaneously. All patients were required to take one quart of fresh raw cabbage juice daily, in four or five divided feedings,6 or a dehydrated form of cabbage juice. Fifteen patients received the dried material which was prepared by lyophilization and assayed for antipeptic ulcer potency.4 It was mixed with enough water (one-half the original bulk of fresh juice) to permit complete solution. A few patients were unable to take large amounts of fresh juice consistently. Juice therapy was continued until pain was relieved and the ulcer crater as observed in x-ray studies (when available) had completely disappeared. In some instances the period of therapy was one week, in most 10 to 21 days.
Whenever possible x-ray examinations to determine ulcer crater healing time were carried out at 7 to 14-day intervals. However, some patients with clearly demonstrated ulcer craters declined follow-up x-ray studies when they were symptomatically relieved. If an interval of a month or more elapsed between x-ray examinations, it is obvious that crater healing time could not be accurately calculated. Ideally x-ray studies should be done weekly. In all cases, blood examinations (cell count, Kahn test and sedimentation rate determination), stool examination, and fractional alcohol gastric analysis were carried out. Some of the patients with gastric ulcer were also examined with a gastroscope.
Analysis of 100 Patients
All but five of the 100 patients either were under the care of the author or were treated under his direction and all records were available to him. There were 74 men and 26 women 21 to 78 years of age and the average age was 49.5 years. Seventy-two patients were hospitalized for treatment and 28 were treated at home. Twenty-five patients treated at home were ambulatory, the majority of them working.
The location of the ulcer was in the stomach in 25 cases, in the duodenum in 71 cases and in the jejunum (marginal or submarginal) in 4 cases. In 55 cases there were enough satisfactory roentgen films to permit determination of ulcer crater healing time. In 17 of these cases the lesion was in the stomach, in 36 in the duodenum and in 2 in the jejunum. In one case there was a peptic ulcer crater in both the stomach and the duodenum. In 17 cases in which the diagnosis of duodenal ulcer was established by clinical and x-ray observation no constant ulcer crater outline could be demonstrated. Ulcer craters that were visualized by x-ray in profile as a niche were measured in their greatest diameter and in their maximum depth. Ulcers that could be visualized only en face were measured in their greatest diameter. Lesions varied in diameter from 0.2 cm. to 3.0 cm. and in depth from 0.3 cm. to 1.5 cm.
Results of Vitamin U Therapy
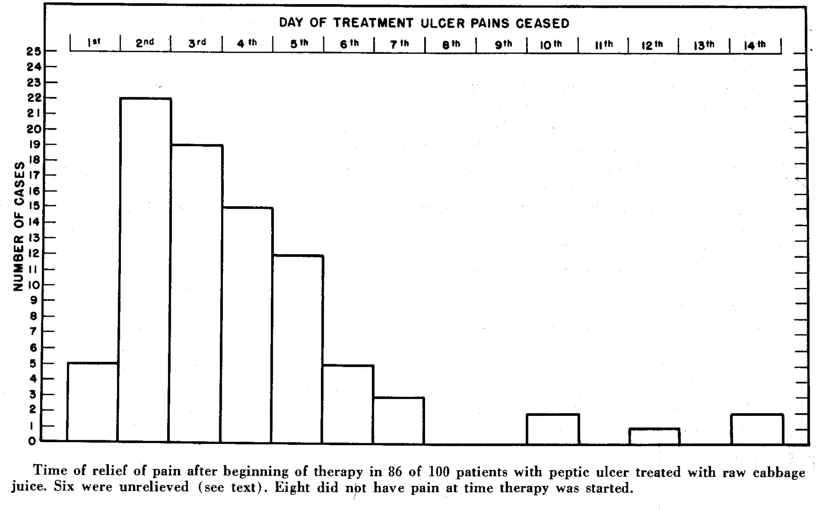
Appraisal of improvement was based first on relief of pain, and second on ulcer crater healing time. As eight patients were pain-free at the time therapy was begun (these patients had ulcer craters clearly visible by x-ray examination), there were 92 patients suitable for study of pain relief. Eighty-six of them (95.9 per cent) were pain-free within two weeks, and 81 per cent of the total were symptom-free within one week. The day of pain relief for the 86 patients is shown in Chart 1. Sixty-one of the patients were pain-free within four days. The average time from beginning of therapy to relief of pain in the 86 cases was 3.92 days.
Chart 1
In 19 cases no ulcer crater could be clearly demonstrated. In 17 of those cases a diagnosis of duodenal ulcer was established and in 2 a diagnosis of jejunal ulcer. Twenty-six of the 81 patients with clearly demonstrable ulcer craters could not be sufficiently well followed to determine crater healing time. In the remaining 55 cases crater healing time was determined.
In the 17 cases of gastric ulcer in which healing time was determined, it varied from 6 to 27 days; the average time was 14 days.
As to the eight cases in which crater healing time could not be calculated by x-ray examination: Three patients had no follow-up x-ray study after 6 days, 7 days, and 21 days of therapy. However, the first and second of the patients were operated upon promptly and in both instances after gross and microscopic examination the gastric ulcers were described as benign and healing. The third patient was symptom-free after the third day. In five cases there was no significant reduction in size of the ulcer after 5, 8, 9, 10, and 29 days of treatment. One of the five patients had polycythemia vera, and, in examination of sections of the stomach in the region of the ulcer crater removed at operation, extensive thrombotic changes of the vessels which apparently reduced the blood supply to the involved area were noted. Inadequate circulation could easily have retarded healing. In another case, in which operation was done on the tenth day after treatment was started, a large benign ulcer had perforated into the pancreas. In a case in which the ulcer crater was 1.0 cm. by 0.3 cm., the lesion was observed to be healed when x-ray examination was carried out three months after treatment ceased, but as the last preceding roentgen study had been done on the sixteenth day of treatment, the crater healing time could not be estimated. It was somewhere between one and four months. A patient in whom no reduction in the ulcer niche was observed upon x-ray examination after eight days of therapy, was operated upon on the eleventh day and at that time epithelialization of the ulcer was noted. A patient with a pyloric lesion and partial obstruction was under direct observation for only ten days, but was known to be improved and working one year later.
Although there were 54 cases of duodenal ulcer with crater in the series, only 36 of them were suitable for analysis of crater healing time (Chart 2), including one case in which the crater was no longer visible in the only follow-up x-ray study, 32 days after the beginning of therapy. Another case was not included because the patient was chronically ill and had a lesion in the pancreas. Although no definite crater was observed in this case at an x-ray examination after 72 days of therapy, upon subsequent x-ray examination six months later a large crater in the duodenal cap was noted; and, at operation, penetration of the ulcer into the pancreas and a localized small chronic pancreatic abscess were observed. For the 36 cases of duodenal ulcer in which healing time was determined, it varied between 6 and 32 days and averaged 12.9 days.
Chart 2

In seven of the seventeen cases in which crater healing time could not be calculated there was no satisfactory follow-up x-ray examination. Six of the seven patients felt well and declined further x-ray study. Improvement was noted in four patients who were last examined by x-ray after nine to ten days of treatment, but the crater was still present. All four were symptom-free. One patient who still had an ulcer crater eighteen days after therapy was started was operated upon, and a duodenal ulcer perforating into the pancreas was observed. In two cases in which ulcers still were present, as determined by roentgen study after ten days of treatment in one instance and after 21 days in the other, the patients apparently had not been adequately treated: they had received a preparation of lyophilized cabbage juice which, when it was fed to guinea pigs that received repeated injections of histamine,4 gave little prophylactic protection against peptic ulcer. Late follow-up studies of three patients with unhealed ulcers could not be obtained.
Seventeen patients with duodenal ulcer without crater all had a “typical deformity” of the duodenal cap with tenderness and irritability of the cap. Three of them were pain-free at the time they were treated, but 12 of the 14 with pain became symptom-free. The two who did not were treated for such short periods (three days and five days) that satisfactory therapeutic results could hardly be expected. In five cases no follow-up x-ray studies were made, including the two cases mentioned in the preceding sentence. In the other three of the five cases symptomatic relief occurred within two days of the beginning of cabbage juice therapy. In eight of twelve cases, improvement in the “indirect findings” of duodenal ulcer was noted in follow-up roentgen studies, and in four there was no change. Two of the latter four patients were originally pain-free, and the other two became pain-free during therapy. As far as can be judged from the data presented, this group of seventeen patients did as well as could be expected from any known form of medical treatment.
In considering the therapeutic results in the four cases of jejunal ulcer, it would appear that this type of peptic ulcer would benefit from vitamin U therapy. A favorable result might be expected on the basis of the generally accepted concept that the mucosa of the small intestine (jejunum and ileum) is lacking in some factor which normally affords a high degree of resistance to acid-pepsin digestion of the gastroduodenal mucosa. This expectation seems to have been borne out, as the average crater healing time in the two cases of jejunal ulcer adequately studied by x-ray was 10.1 days. The average healing time for the total series of 54 cases with demonstrable peptic ulcer craters which could be satisfactorily followed by periodic x-ray examinations was 13.1 days, or just under two weeks.
Discussion of Therapeutic Results
The results of treatment of 100 patients with peptic ulcer indicate that therapy with vitamin U in the form of cabbage juice deserves careful consideration and further study. Although an exactly comparable series of cases for a comparative analysis was lacking in the present study, it should be taken into consideration that 84 per cent of the patients treated had had symptoms of peptic ulcer for one month or longer before receiving cabbage juice and that at the time vitamin U therapy was begun nearly all of them were under some form of treatment which had already proven unsuccessful as regards sustained symptomatic relief. A number of the patients, and 21 additional “control patients” that were given “standard” treatment for ulcer had been examined initially by x-ray and again thirty or more days later without demonstrating disappearance of an ulcer crater. Consequently, although ulcer crater healing time could not be accurately calculated in these cases, it could be said that it exceeded one month in all instances, and was considerably longer than the average time of 13.1 days obtained in the series of patients treated with vitamin U.
In considering that the symptom of pain was relieved in 86 per cent of the patients treated with cabbage juice, and that the average length of time from beginning of therapy to relief of pain was four days, it might well be stated that in this series the interval before relief of pain was similar to that which has been reported for almost all other forms of therapy, nearly all of which involve the use of a bland diet, alkalis, sedatives, antispasmodics and, not uncommonly, a variety of old or newly introduced drugs. By that standard alone, the best that could be said for the effectiveness of vitamin U therapy in relieving pain is that it is only as good as many other forms of treatment. However, there is a very important and significant difference. Relief of pain occurred in this series of cases without the continued use of any form of drug therapy and without frequent feedings of food. This is in sharp contrast to experience in the usual series of peptic ulcer cases reported in which the symptoms are obliterated or masked by the frequent and continued use of drugs and food and it cannot be determined when pain would have spontaneously ceased. For example, when Banthine® bromide is used in the treatment of peptic ulcer, pain often is quickly relieved and the patient may remain pain-free during months of Banthine therapy. However, when treatment with this drug is stopped, pain may rapidly recur and a follow-up x-ray examination show that the ulcer crater demonstrated at the onset of Banthine® therapy remains unaltered. Symptomatic relief of pain by drugs or by food cannot be justly compared to absence of pain when no symptomatic treatment is administered. With this difference in mind it would appear that the high incidence of symptom relief which tends to develop rapidly in patients treated with vitamin U is a real and important indication that this form of treatment is effective in promoting the healing of peptic ulcers.
In considering normal standards of ulcer crater healing time, it must be stated that so far an insufficient number of detailed x-ray studies of large series of cases of peptic ulcer have been published. The control series of 68 cases used for a comparison with the present series of 54 cases (Chart 2) was published in 1946.7 In the total series of 69 cases studied there were six cases of gastric ulcer with an average healing time of 42 days, and 63 cases of duodenal ulcer (one of these was omitted from the calculations because of a greatly prolonged healing time) with an average healing time of 37 days. Chart 2 clearly shows a greatly shortened healing time for the patients treated with vitamin U; and the rapidity of healing is emphasized when the average healing times of 14 days for gastric ulcer and 12.9 days for duodenal ulcer are compared with the 42 days and 37 days cited from the literature. In 1947 a large series of cases of benign gastric ulcer was reported with a healing time similar to that reported in 1946.8 In a recently published report, ulcer crater healing time was completely studied in 31 cases of gastric ulcer,9 and the time was shown to have varied between 2 and 15 weeks, with only eight cases in which there was complete healing in less than 4 weeks. The average healing time for the 31 cases was not stated, but from the data presented it can be calculated as 6.93 weeks. This healing time of slightly less than 7 weeks is comparable to that reported by Cummings and co-workers7–42 days (6 weeks).
References Cited:
- Cheney, G.: “Effect of diet and cinchophen on production of experimental gastric ulcers in chicks,” Proc. Soc. Exper. Biol. & Med., 45:190, 1940.
- Cheney, G.: “Cinchophen gastric ulcers in chicks,” Arch. Int. Med., 70:532, 1942.
- Cheney, G.: “Prevention of histamine-induced peptic ulcers by diet,” Stanford M. Bull., 6:334, 1948.
- Cheney, G.: “The nature of the antipeptic-ulcer dietary factor,” Stanford M. Bull., 8:144, 1950.
- Cheney, G.: “Rapid healing of peptic ulcers in patients receiving fresh cabbage juice,” Calif. Med., 70:10, 1949.
- Cheney, G.: “Antipeptic ulcer dietary factor,” Amer. Diet. Assn., 26:9, Sept. 1950.
- Cummings, G. M., Jr., Grossman, M. L., and Ivy, A. C.: “A study of the time of ‘healing’ of peptic ulcer in a series of 69 cases of duodenal and gastric craters,” Gastroenterology, 7:2037, 1946.
- Pollard, H. M., Bachrach, W. H., and Block, M.: “The rate of healing of gastric ulcers,” Gastroenterology, 8:435437, 1947.
- Steigman, S., and Shulman, B.: “The time of healing of gastric ulcers: implications as to therapy,” Gastroenterology, 20:20, 1952.