
Access to all articles, new health classes, discounts in our store, and more!
The Special Nutritional Qualities Of Natural Foods
Published by Lee Foundation for Nutritional Research, July 1942. Co-Author: Jerome S. Stolzoff
* * *
There are certain basic facts relating to human nutrition that we believe are self-evident at this time. We offer them as follows:
- The refining and processing of foodstuffs that has become so universal in all civilized countries has been done to improve the appearance, keeping qualities and competitive salability of foods without any regard to nutritional values. As a result of our high per capita use of such foods, we have a high incidence of certain deficiency diseases that are almost non-existent in countries where such food denaturation is not prevalent. (A list of such diseases is indexed in the chart following this article,)
- Because of modern mechanized methods of food production, basic food commodities are today apparently far cheaper than they have been at any time in human history.
- Because of the denaturation of foods, by refining and processing, we are over-eating of the fattening and energy-producing components, and literally starving for the vital vitamin and mineral factors in foods, (no less necessary to life than the fats, carbohydrates and proteins), which have become far scarcer and more difficult to obtain than at any time in the history of the human race. Actually our diets are excessively rich in the ‘fuels’ necessary for good health, but lack the ‘spark’ in the form of vitamins and minerals necessary to properly utilize them.
- These vitamin and mineral elements are so complex and multiplex that their nutritional importance has been invariably discovered only by investigating the symptoms of physical degeneration and functional failures in animal and human subjects who were supplied with food lacking some of these essential elements. Further investigations have always shown that the lost material was so complex in its organic nature as to defy artificial substitution, if complete, restoration was to be attempted. Where less than complete restoration was attempted, the results have been extremely unsuccessful.
- Natural foods also are characteristic in being more satisfying to the appetite and are self-limiting in preventing a tendency to overeat. Honey is a good example; children crave sweets and will invariably overeat if given artificial sweets such as commercial candy, but if given honey they will automatically limit their intake to that which is safe. In the case of devitalized or artificial foods there is either a total loss of appetite for the food in question after its use for a period of time, as has been noted in the case of butter substitutes, or on the other hand, the substitute fails to satisfy the natural craving and overeating and obesity is the natural result.
- Each animal species has its preferred and most favorable specialized food, to which it has become adapted over ages of experience. Therefore, no new food product or vitamin concentrate should be sold or recommended for human use until a background of experience has been accumulated by clinical tests or carefully observed use by competent investigators, to determine its specific nutritional values and effects. Violation of this cardinal principle has resulted, in some cases, in the creation of new pathological conditions more serious than the ones that were being ‘cured.’1
The inevitable conclusion after the acceptance of the foregoing is that:
- No food is safe, unless it is fresh enough to have retained most of its perishable vitamins. Spinach may lose all of its vitamin C in a week;2 oranges in three months.3
- No food is safe, unless it has incurred no processing that would remove or impair its vitamin and mineral content. This eliminates pasteurized milk,4 white sugar,5 synthetic syrups, bleached flour, and practically all packaged cereals, shortenings, fats, etc.
- No food is safe, unless it is free of any kind of synthetic adulteration, representing crude attempts to replace valuable organic constituents lost in processing. Wherever this has been attempted, the result has been found futile, and has proven to be actually dangerous. Tests made on dogs with white flour fortified with synthetic vitamins demonstrated that the fortified flour killed dogs quicker than the old white flour, unfortified.6 That is why Canadian laws now prohibit the adulteration of bread or flour with synthetic materials of any kind. If the vitamin content is to be raised, it must be done by retaining the original factors, not by adding new ones of unknown effect.
- No food is safe, unless it has a background of experience behind it establishing its value to the human family. Animal tests should be considered only as preliminary and suggestive indications of possible value.1
The situation, no doubt, calls for some kind of legislative action to protect the public health. It also calls for a campaign of education on the part of makers of natural foods to call the attention of the public to the real facts, and to show the housewife how to get the most for her money in buying foods–not the most pounds of commodity but the most nutritional value for the money.
Wheat, rice, and oatmeal have been selected as preferred cereals for human food. It is, no doubt, more than a coincidence that these grains are the highest in vitamin content. The food products richest in vitamins, over the ages, seem to have appealed most to our taste sense. The modern method of processing these cereals, however, has deprived us of the benefit of this long-established preference. It has cheated us by giving us the bulk food components–the starches and proteins of the cereals, without the vitally essential vitamins and minerals. As a result we may become obese, lowered in vitality and resistance to disease, lazy, and mentally and morally deficient.
Today we find that even insanity is a possible end result of extreme deficiency of the vitamin B complex.1 Before the discovery of the far-reaching and socially devastating effects of nutritional deficiencies the above statement would have appeared to be an exaggeration.
The commonest and most universal effect of vitamin B deficiency is the heart degeneration that in civilized countries kills more people than any other disease. In creating this effect, vitamin C deficiency is an able partner, for in that case the heart is overworked because the capacity of the blood to carry oxygen is impaired materially, requiring a more rapid circulation.7 The biochemistry involved in these destructive forms of starvation is now fairly well known.
Dental caries, or tooth decay, has long been suspected of being a universal sign of vitamin and mineral deficiency, resulting from our excessive use of denatured cereals and refined sugar. Further proof of the deficiency theory as the cause of caries came last year, with the discovery that caries was practically non-existent in a county in west Texas where the wheat flour made from locally grown wheat was found to contain six times the ‘normal’ phosphorus and calcium content. This is evidence that wheat we have heretofore accepted as ‘normal’ wheat was in reality starved wheat, and in turn what we have termed as ‘normal’ children with many carious teeth, were really starved children.
Maybe this object lesson in our own back yard will produce more interest in Dr. Weston A. Price’s remarkable book, Nutrition and Physical Degeneration. Outstanding is his description of the high valleys in the Swiss Alps, where, before improved transportation brought in refined foods, such diseases as tooth decay, tuberculosis and cancer were unknown. After the use of refined foods became common, the incidence of these diseases became as high as in other countries where such foods are used.8
The Superiority of Whole Wheat Bread
The public has, in the last twenty years, become educated in a considerable degree as to the dangers of eating an excess of white flour products, and the per capita consumption of white bread has been constantly dropping, with an attendant increase in the use of whole wheat bread. Practically none of the whole wheat bread available, however, is made from freshly ground unbleached flour. Many kinds of mixtures of bleached white flour with bran and other wheat byproducts are being sold as whole wheat flour. The reason is that real whole wheat flour has such short keeping qualities because of its high vitamin content, thus attracting insect life, that it cannot be practicably distributed. One milling expert may be quoted as saying that “real whole wheat flour is practically as perishable as milk.”
It should be pointed out here that the whole wheat product is, undoubtedly, not the most perfect way to prepare a wheat flour. The bran or fiber content is not particularly desirable as it detracts from the workability of the flour in its baking qualities, as well as being irritating to many digestive systems. The secret of the success of the roller mill was that it made possible the rejection of the germ of the wheat along with the bran (the rejection of the germ being important to prevent insect infestation, and to prevent the development of rancidity of the germ oil in the flour that would take place if it were present).
The presence of the germ in the flour also drastically darkened it, and the public was taught to prefer bleached flour. The bleaching in reality was essential again to improve ‘keeping qualities,’ for it destroyed most of the remaining vitamins left after removal of the germ.
An ideal flour, that has an exceptional flavor, and a higher vitamin content than whole wheat, is made by grinding wheat in the old-fashioned way with stone buhrs, to as fine a degree as possible, then sifting out the major part of the fibrous remainder that is too tough to become comminuted. This retains the complete germ portion of the wheat, and rejects only the most woody elements of the bran. Unless this coarse bran is taken out of the flour, the average baker or cook finds it absolutely necessary to add some commercially bleached white flour to the whole wheat to get satisfactory working qualities for the practical manipulation of the flour either in bread making or other use. Rather than to add the nutritionally valueless white flour, the logical procedure is to take out some of the bran. As above stated, the remaining product then contains more, instead of less, of the vitamin values of whole wheat.
Such a flour would require distribution in vacuum-packed tins, or shipment in small lots directly from the mill to the consumer at short intervals, and to be kept under refrigeration except when actually in transit to prevent a definite progressive deterioration in flavor.
Is all this trouble worth while? Well, once it was not thought worth while to keep typhoid out of our drinking water, nor to test our milk cows for tuberculosis. Perhaps in time public opinion will force new reforms that will make it easier to escape the various forms of death that are hidden in denatured foods, and outlaw the sale of food products that have been so refined as to completely destroy their capability of supporting life.
Because bread forms a major part of the American dietary, the general public’s acceptance of devitalized white bread has formed a definite threat to the nation’s health standards. Drummond9 has pointed out that the introduction of the roller mill has converted the British dietary, based, much as ours, on white flour from one “reasonably compatible with well-being, into one definitely dangerous to health. There is no cheap source of vitamin B1 other than wholemeal bread, and if efforts to make it inaccessible continue, the gravest consequences will result.” The simple addition of synthetic B1 fails to completely answer this problem. McHenry10 has shown the commercial logic, but nutritional folly of fortification when he commented:
“Because of the public desire for white bread, a number of attempts have been made to restore to it part or all of the nutritive value lost in milling. Vitamin B1 (thiamin) is readily available as a pure substance and the addition of it to white flour has been recommended. This would only supply one of the vitamins lost in milling. Attention has been fostered upon thiamin with a consequent neglect of the other B vitamins because thiamin is easily measured and because it is readily available commercially.. Experimental evidence indicates that B vitamins are jointly needed for metabolic processes and that they should be supplied in balanced amounts. It is difficult to see the wisdom of removing eight or more needed vitamins and then only adding one to make good the loss.”
The failure of synthetic vitamins to replace the B complex vitamins lost in milling and bleaching of flour, has also been commented on by John F. Murlin, who, while addressing the National Nutritional Conference for Defense, May 26, 1941, expressed reluctance in accepting the program for fortification of bread. He noted that experiments in his laboratory had shown that dogs placed on a diet deficient in the B complex, failed to recover when fed the six commercially available synthetic fractions, but returned to normal when fed a natural source of the B complex in the form of yeast. He further stated that he was greatly reassured when he learned that the committee was going to attempt to gradually extract more and. more of the nutrients from the wheat itself.11
The consequences of this loss of the B complex assume staggering proportions when one realizes the prevalence of vitamin B complex deficiencies, and the number of conditions ascribable to B deficiency. Balfour,12 believes that not one person in ten receives an adequate supply of the B complexon a so-called standard diet. Neither is it easy to overlook the wide variance between the minimum (the amount needed to prevent clear-cut clinical deficiency syndromes) and the optimum (the amount needed to promote fullest health). While there are comparatively few cases of beriberi, or pellagra, there are vast numbers of conditions now believed to be sub-clinical manifestations of a B complex deficiency. Some of these conditions are outlined in the appended list.
There is an inter-dependence among these various factors of the B complex. Diets deficient in one fraction of the B complex are invariably deficient in other factors of the B complex.
The direct relationship between heart diseases and vitamin deficiencies has been clearly pointed out.13,14,15 Certainly we cannot explain the paralleled rise of white flour and heart diseases as coincidental. The fact that many forms of heart disease are recognized as vitamin B deficiencies, and that white flour has lost most of the B complex content, would appear to have a direct relationship. This outstanding rise of heart disease has been pointed out by Dublin,16 who showed that the rate of coronary disease among millions of industrial policy holders has risen from 4.7 per hundred thousand in 1930 to 24.9 per hundred thousand in 1935–an increase of more than 500 per cent in five years.
Quigley17 stated, “That this is a dietary error seems to be pretty well proved by the experiments of Langsworth, Harris, Sansum, and many others who find that quite advanced cases of high blood pressure improve in a very decided manner when treated only by putting patients on a corrected diet and having them avoid all foods containing white flour, refined sugar and other refined, devitaminized, and devitalized carbohydrates.” We might well remove the term ‘heart disease’ and supplant it with ‘white flour disease.’
The Problems of Whole Wheat
Unfortunately, the problem of bread does not end by simply saying, “make it whole wheat” rather than white bread. First, the type of whole wheat bread commonly sold, is made of bleached whole wheat flour (bleached to destroy the vitamins that make it perishable). Secondly, there is a wide variance in the desirability of whole wheat grown in various sections of the country. Lastly, centralized milling makes fresh flour unavailable for most of us.
We have already mentioned the outstanding example of wheat grown in Deaf Smith County, Texas, where an analysis of the flour made from this wheat showed that it contained six times the usual content of calcium and phosphorus, Mineral tests on the soil showed (as was to be expected) that the soil itself was many times richer in these minerals. Since the same varieties of wheat are grown here as elsewhere, the only logical answer is that this soil more nearly approaches the maximum nutritional requirement of wheat. Along this same line of reasoning, is it not fair to assume that all other, or at least most other wheat, is actually failing to receive the maximum amount of essential minerals it needs? Are we not then being fed on cereals which in most cases are actually starving for these vital factors? This is shown more clearly when one travels through most grain growing sections in the country. Too often the grain is so weak, that the field is a maze of plants almost doubled over, actually lacking in minerals to such an extent that it cannot support its own weight.
We attempt to offer no solution to this situation. It may be one of educating the public to buy only high mineral content wheat, or it may be one of better fertilization, but nevertheless from the viewpoint of the person interested in nutrition, it is a serious problem of no small consequence. The far flung effects of taking wheat which first of all does not contain as much of the vital factors as it possibly could, then bleaching it, thereby destroying the vitamins, and finally serving it in one form or another as a major part of the diet, reflects a trend in foods that is not only unsound, but which can be classed only as dangerous to the health of the persons who depend on their common foods to provide the proper nutrition which their body demands.
It is a problem which the Canadian Government has attempted to answer, by prohibiting the fortification of foods with artificial vitamins, after the removal of the natural ones. It is a problem which the United States has ignored for a long period of time. The action of the President in calling the National Nutritional Conference in Washington in 1941 showed that work shall be done. With the growing realization that proper nutrition is the only basis of sound health, perhaps the accumulated information on deficiency diseases so long in the background will be given a chance to receive some deserved publicity.
The Unique and Indispensable Place of Butter in the Diet
Since the discovery of the fat-soluble vitamins and their paramount importance in foodstuffs, the uses of various special sources of these vitamins and their concentrates have been widely investigated and vast sums have been spent in the study of their nutritional effects. Butter, however, the most extensively used and by far the most important source of these vitamins has been rather neglected from a scientific standpoint. The commercial opportunities have been far more attractive in the fields of recovery of the fat-soluble vitamins from cod and other fish liver oils and their advertisement has to a great extent overshadowed the fact that most people had-been and were now getting these vitamins from their butter.
The vitamins from such other sources represented in many cases a salvage of value from otherwise wasted byproducts, and afforded a liberal profit permitting an extensive expenditure for the advertising of the essential nature of the vitamin involved; whereas, butter is a product produced upon a scant margin of profit at best and represents, no doubt, one of the highest values in food products obtainable, considering the number of man-hours per dollar of the consumer’s money that is used in its production.
It is important to guard against measuring our foods by false nutritional standards in which foods are judged by energy values, which serve only to put on weight, instead of by vitamin and mineral values which serve to promote vitality and resistance to disease. In this connection we recall the experience of an institution for the blind, during the last war, in which butter substitutes replaced butter without the knowledge or detection of the inmates. Though they could detect no difference in flavor, after a few months they lost their taste for ‘butter’, and invariably would eat their bread plain. Apparently, the vital substances and not just the fats themselves satisfy our appetite for butter. These vital substances give butter its special nutritional value. If we are after only the fats and calories, there are many substitutes far cheaper than butter. Measured by accurate nutritional standards, butter is an inexpensive, irreplaceable dietary constituent. These special nutritional values of butter are responsible for its use as an important dietary factor in the treatment of certain diseases.
The Vitamins in Butter
Butter is rich in vitamins A, D, E, and F.
One author has called butter “the nation’s best source of vitamin A.”19 Butter contains both vitamin A and pro-vitamin A (carotene).20 It is important to note that these identical values cannot be produced in other fats merely by adding a high unitage of carotene. Many persons lack the ability to convert carotene into vitamin A.21 Among those able to convert it, there is a wide variance in the percentage of carotene which is utilized.21 Being a natural food, butter contains all of the associated factors necessary for the maximum vitamin effect.
Taken the year round, butter contains enough vitamin D to be considered a preferred source of this vitamin. The natural vitamin D found in one pound of butter is equal to that found in ten quarts of milk.22
Little has been said in the past of the vitamin E content of butter, but it appears to be present in significant quantities. On a diet in which all vitamin E-containing substances, except butter, were removed, test animals continued to reproduce23 and did not otherwise exhibit symptoms of vitamin E deficiency. The removal of butter from the diet, however, saw the cessation of all reproductive powers.23 The presence of butter in the diet of persons receiving no other supply of vitamin E, when furnished in amounts up to 10 per cent, assures not only reasonable success in reproduction, but is followed by notable success in lactation.24 Other authors have also pointed out the need for butter fat, if reproduction powers are to remain normal.25
Recent work has shown the necessity of an adequate amount of vitamin F (unsaturated fatty acids) in the diet. Hart and Cooper26 have shown it to be a successful curative agent in the treatment of prostate disorders. As far as they are known, the history, uses, and chemical properties of vitamin F, have also been reported.27 Though vitamin F will still bear much investigation, from the list of conditions responding to it (including certain skin conditions, prostatic hypertrophy, failure of reproductive powers), it may be assumed that vitamin F may soon take its place as one of the important factors in the vitamin category.
The most potent form of vitamin F is known to be associated with arachidonic acid.27 Arachidonic acid is found to be present in butter.28 Normal patients fed 100 gms. of butter (slightly more than a normal day’s supply) showed an immediate increase in the unsaturated fatty acid content of the blood.29
Attempting to measure the vitamin content of butter in terms of units, fails to indicate the true potency of the substance. These factors modify and enhance one another, and unless they are all present, as in natural foods, maximum effectiveness cannot be obtained.
Fraps and Kemmerer, of the Texas Agricultural Station, found that unit for unit the vitamin A in butter was three times more effective than the vitamin A in cod liver oil.30 This probably accounts for the results discussed later in treating vitamin A deficiencies by adding substantial amounts of butter to the diet.
One must bear in mind the apparent fallacy of measuring the vitamin D potency of butter in terms of units alone. Actually, it has been found that a unit of natural vitamin D is 100 times more effective in preventing rickets in children than a unit of irradiated ergosterol 1 (synthetic vitamin D).31
Other Properties of Butter
Of importance is the physical structure of butter. Because it is found in free-floating globules, butter is easily acted upon by the body enzymes. It is partially because of this that butter is the most digestible and easily tolerated of the fats.32
An added advantage of butter fat is the relative stability of the vital factors. Subjecting butter to steam for several hours failed to materially alter its growth-promoting qualities.33 While butter is not high in mineral content, it is rich in the fat-soluble factors which must be present for proper mineral ingestion.8
Butter is also enhanced by the presence of approximately 140 gms. of lecithin per pound. The phosphorus associated with lecithin is of importance. Much publicity has been given to calcium in the past few years, and while there is, undoubtedly, a calcium deficiency in the average dietary, an adequate intake of phosphorus is also important, and ofttimes lacking in the diet. In the diagnosis of rickets, for example, it has been found that rickets is more often caused by a deficiency of phosphorus than a deficiency of calcium.34 The lecithin content of butter assumes further significance, when we realize that the phosphorus in lecithin is the form most readily utilized.
Therapeutic Values of Butter
The real value of butter in the diet is its use as a protective agent against certain nutritional deficiency diseases. Butter has been used on occasion, however, as a therapeutic agent in the treatment of these deficiency diseases. Notable in this field has been the work of Dr. A. B. Grubb, who has used butter as a dietary agent in the treatment of psoriasis, xerophthalmia, tuberculosis, dental caries and rickets.
Dr. Grubb recently commented:
“Unfortunately, the public which loves to suffer and suffer long prefers ‘shots’ for their deficiency diseases to actual wholesome food. The author has lived about ten miles from a community which has had more than its share of eye troubles and even blindness. This condition has existed, from what I have learned from old people, at least seventy-five years. The diagnosis made by the ophthalmologists who have seen these cases has been trachoma and so far as I can learn they have been treated mostly with application to the lids. Originally the community was a poverty stricken community. Marriages were practically always among kin folk. Everyone was poor and on a terribly deficient diet, and the soil was sandy and deficient in lime, etc.
“Several years ago I put a girl on cod liver oil, with marked improvement…One large family moved away to a dairy farm of an Englishman and had plenty of milk and butter. I was told by their friends that the change in their eyes was so great within a short time that they hardly knew them. The red eyelids were gone, and the lacrymation and the characteristic manner of holding the hands over the eyes to keep out the light were gone too. It appears that it was a wonderful transformation, all due to diet. There were others on whom I prescribed a butter diet with improvement in spring conjunctivitis and xerophthalmia.
“The following is a typical case: A sixteen year old boy from the same community was visiting his sister when seen last May. His eyelids were swollen and red, lacrymation and photophobia annoying, and this condition had existed for a long time. I urged that he eat two pounds of butter a week with no other treatment. All symptoms were gone when I saw him in August.” (Grubb, A. B., “Butter Fat in Trachoma,” Medical Record, 154, 9:351, November 5, 1941)
Some cases of diarrhea may be little more than the result of failing to receive a proper fat intake, since it has been pointed out that butter fat is essential in producing stools of proper consistency.35
Dramatic proof of the growth promoting properties of butter was shown in a test in which a 78 per cent increase in weight in young animals was produced by the addition of but 5 per cent of this amount of butter fat.36
Superiority of Butter Over Substitutes
Basically butter is a natural carrier of vital food factors. Butter substitutes are not. Attempts to fortify other products and make them the nutritional equal of butter fall far short of the mark for two reasons: (A) The action of any single fractional vitamin is enhanced by the presence of all of its naturally occurring associated factors. Butter, being a natural food and natural carrier of these vital substances, contains all of the factors essential to fullest utilization. The cooperation of vitamins D and F is an outstanding example. Vitamin D raises the blood calcium and vitamin F diffuses it through the capillary wall to its destination–the cell. Without the vitamin F the possibility of vitamin D toxicosis is present, as increasing the calcium of the blood to an excessive level is dangerous, and is characterized by the symptoms of sun stroke–a case where the victim may even die–really from vitamin F deficiency, which, if present, would nullify the effects of the excessive sunlight in creating vitamin D. (B) Previous to fortification, other fats admittedly are lacking in almost all of the nutritional fractions necessary to sustain life. Obviously then, any attempt to add but one or two fractions cannot put any other fat on a nutritional par with a food known to contain a balance of vital factors.
Other workers have substantiated these findings. It has been found that substituting vegetable oils for butter causes a decalcification of bones, resulting in their fragility (36). This may well be a result of a vitamin F deficiency, since Zeithraus and associates found that margarine was inferior to butter in calcium resorption even on a full diet of the other vitamins.37
The nutritional inferiority of butter substitutes is reflected in their inability to promote growth, or even sustain reproduction in test animals. A series of animal tests25 placed half the rats on a diet including vegetable oils, and the other half received a diet in which the vegetable oils were replaced with butter. The group on vegetable oils had a lower growth rate. They also tended to have a lower birth rate, and produced unsatisfactory offspring. A third group was placed on a diet which excluded butter, and their weight slumped one third. The replacement of milk and butter in the diet promptly returned their weight to normal.
One author36 finally concluded that the exclusion of butter from the diet in favor of vegetable oils or butter substitutes can result in poor health or even premature death. Neither can we forget the tragic story of the first world war, when Denmark exported most of its butter, and then as an economic measure replaced it with butter substitutes. The result was a tragically high incidence of children becoming blind. “Their eyesight was sold abroad along with the butter.”1 The story of butter is not distinctive in the field of nutrition. It is the oft repeated tale of an artificial food being unable to replace a natural one.
The story will continue, unless some day we either completely master every slightest detail of the workings of nature, or else manage to establish in the mind of the public the fact that natural foods are undeniably superior, and, as a democratic nation, call upon our legislators to frame some common-sense laws to stop the unwarranted and, in some cases, the unconscionable meddling with naturally nutritional foods.
The Difficulties of Combating Commercial Interests
“The machinery for government regulation of foods was devised to prevent the sale of spoiled, adulterated, or misbranded foods. With notable exceptions in certain bureaus of the Department of Agriculture, little attention has been given to the nutritive qualities of human foods. The interest in general has been more in protecting pocketbooks than health. Also unhappily some food legislation has discriminated in favor of special interest groups with large political influence to the detriment of the public at large.” (Wilder, R. M., Professor of Medicine, The Mayo Foundation, Rochester, Minnesota, Speech before the National Nutrition Conference, Washington, D. C., May, 1941)
Perhaps the field of nutritional science which we have reviewed in this paper is new to an extent, but the ideas are neither radical, nor contrary to the fundamentals of good nutrition. Most nutritional workers have long recognized that the foods we consume in the greatest amounts, are not always those foods most beneficial. Recent years have seen a marked tendency to stray far from the path of sound nutrition. Why then, has the public in general failed to properly receive the knowledge so vital to its very existence?
America’s food industry is built to a large extent on foods which would ordinarily be highly perishable. Rather than finding methods of efficient distribution, it has been easier to simply devitalize the food. Foods which have had their vital factors removed will fail to sustain life for insects, molds, and microbes, consequently they can be easily shipped over long distances, and simply stored over long periods. Unfortunately foods which will not sustain other forms of life, will not satisfactorily sustain human life.
The problem can no longer remain one which is merely a question of commercial expediency. The reason for the inability of any educational program to take hold, has been mainly a financial one. Commercial propaganda is profitable, financially self-sustaining; education is not.
Legislation is vitally necessary to correct this picture of malnutrition in a land of plenty. Manufacturers of devitalized foods will defend their position to the last inch. They defend it by propaganda, corruption of political parties, control of medical societies, financial inducement of professional men to create pseudo-scientific evidence to favor their products, or any other means which they can find to perpetuate their existence. They, too, realize that we are entering into the final stage of a battle that will find either our health standards destroyed, or the devitalized food manufacturer destroyed (the latter by legislation, the former by malnutrition).
It is impossible, for example, for centralized flour milling to continue if we were to leave in the flour the valuable factors now removed. Such flour cannot be distributed over long periods of time without excessive loss due to insect infestation, mold, and spoilage.
This is not an attempt to answer the problems of such foodstuffs. American ingenuity has found the answer before when forced to. Under the present laws there is no incentive to arrive at methods of distributing foods in their most nutritive state. Canada’s solution to this problem seems to be our solution to it. Legislation is the most expedient method of stamping out the dangers of malnutrition which we are now faced with. Because the people of the nation are not strapped to their beds, doesn’t mean that this problem should not be taken seriously. The reduction in efficiency measured in man-hours would, undoubtedly, present a staggering figure if it could be accurately measured. A generation brought up on devitalized foods has accepted a poor dietary as a standard dietary.
Sound nutrition, like charity, “must begin at home.” It is the choice of foods by each individual person, today, that will determine to a large extent his physical condition tomorrow.
As sources of information for a detailed study of this subject, the following books are suggested:
For a scientific approach:
Nutrition and Physical Degeneration, W. A. Price, D. D. S., Paul H. Hoeber, Inc., New York, 1939, $5.50.
Physiology and Chemistry of the Vitamins, H. R. Rosenberg, Interscience Publishers, New York, 1942, $12.00.
For practical information useful to the lay reader:
Diets for All Ages, R. M. Field, M. D., Doubleday, Doran and Company, Inc„ Garden City, New York, 1942, $2.50.
Man Alive, D. C. Munro, M. D., Bartholomew House, Inc., New York, 1940, $2.00.
The National Malnutrition, D. T. Quigley, M. D., F. A. C. S., Lee Foundation for Nutritional Research, Milwaukee, Wisconsin, 1943, $1.50.
How to Regain and Retain Health, Joseph H. Maassen, Health Publications, Los Angeles, California, 1942, $3.00.
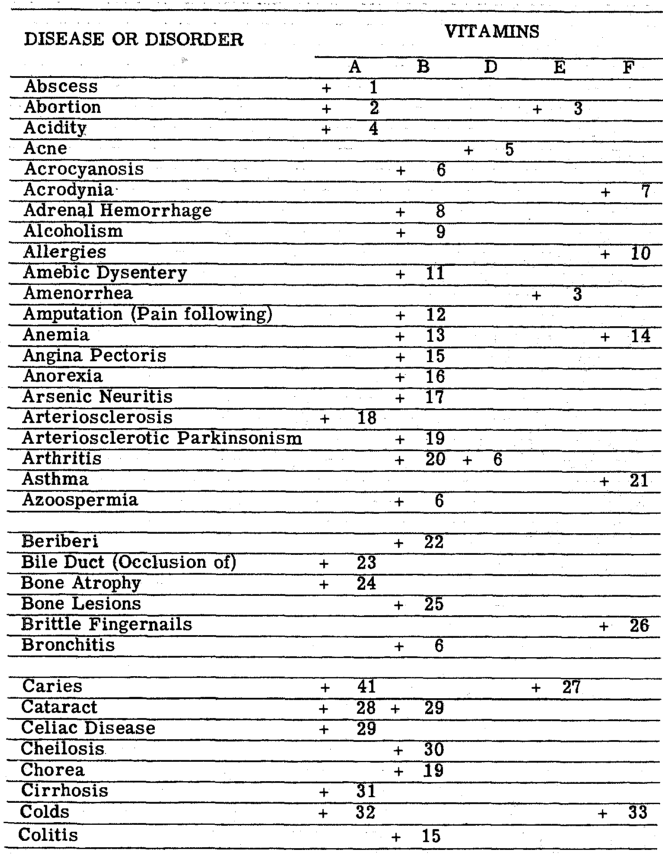
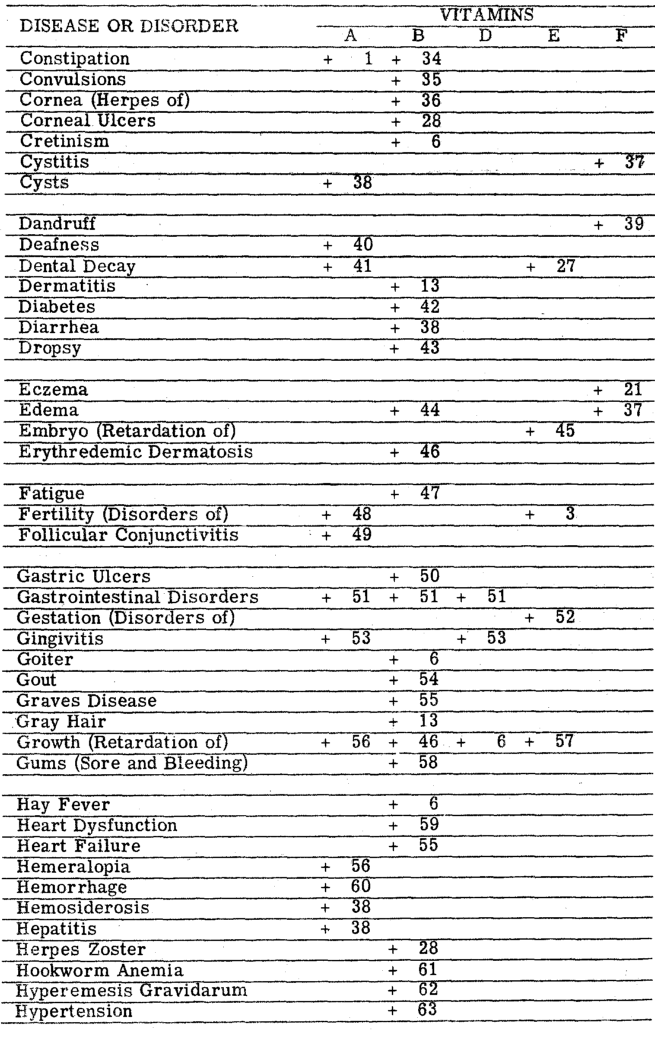
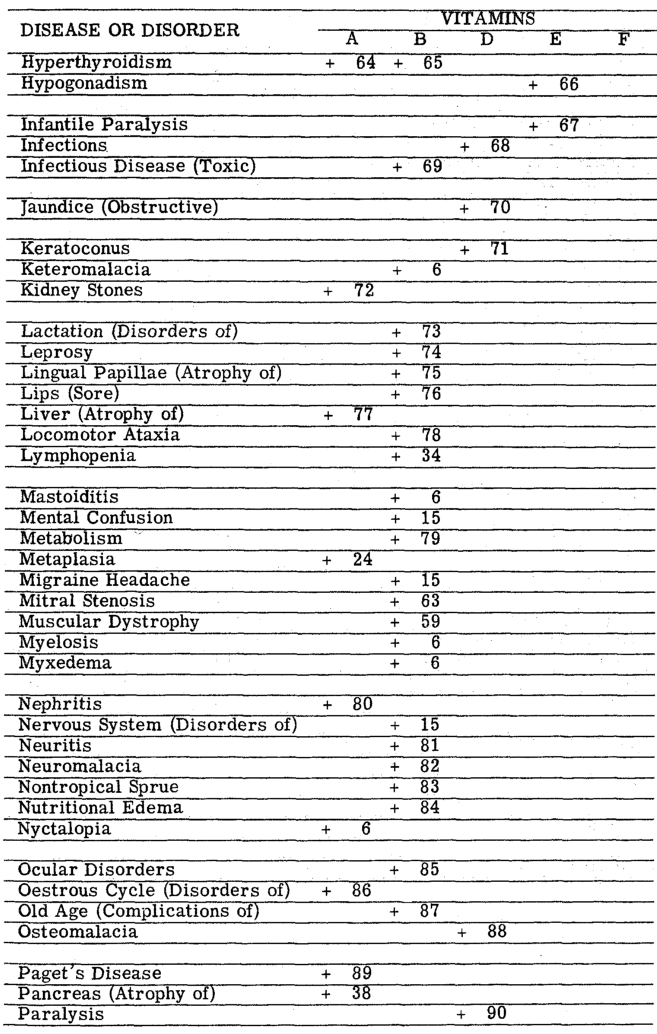
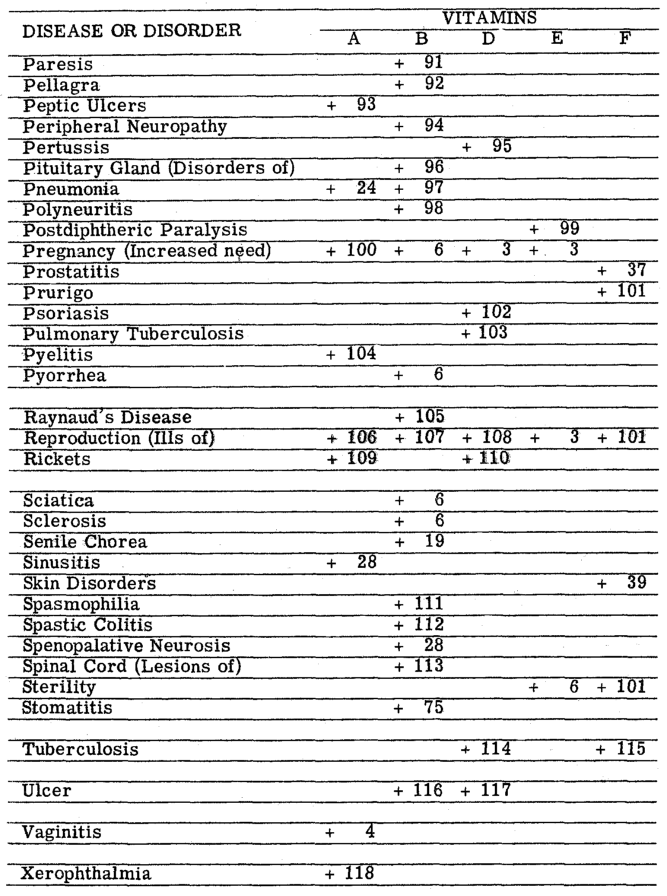
Bread and Butter Chart
The bodily disorders and diseases listed below have been reported in the literature as aggravated by a deficiency of the vitamins normally found in butter, and whole wheat.
(The numbers in this chart refer to the Bibliography for Disease Appendix below)
 }
}
References Cited:
- United States Department of Agriculture Yearbook, Food and Life, pp. 12, 268, 151, 705, Government Printing Office, Washington, D. C., 1939.
- Eddy and Dalldorf, The Avitaminosis, p. 171, Williams and Wilkins, Baltimore, 1937.
- Roberts, J. A., “Vitamin C in Citrus-Juice Beverages and Canned Grapefruit Juice,” Food Research, 2:331-337, 1937.
- Jordan, E. O., A Textbook of General Bacteriology, Twelfth Edition, p. 691, W. B. Saunders Company, Philadelphia, 1938.
- Lewis, L. R., “The Relation of Vitamins to Obstetrics,” Am. J. Obstetrics and Gynecology, 29, 5:759, May, 1935.
- Morgan, Agnes Fay, Science, March 14, 1941.
- Peterson, J. M., “Vitamin Enables Animals to Use Less Oxygen,” Science News Letter, 40, 9:137, August 30, 1941.
- Price, W. A., Nutrition and Physical Degeneration, pp. 34,291, P. B. Hoeber, Inc., New York City, 1939.
- Drummond, J. C., “The Place of Bread in the National Diet,” J. Roy. Inst. Pub. Health Hyg., 2:441-450, 1939.
- McHenry, E. W., “Observations on the Nutritive Value of Bread,” Can. Pub. Health J., 31:428-432, September, 1940.
- Proceedings National Nutrition Conference for Defense, pp. 25-26, Government Printing Office, Washington, D. C., 1942.
- Balfour, M., “Nutritional Therapy During Pregnancy,” J. Proc. Roy. Soc. Med., 31, 2:911-914, June,1938.
- Keefer, C. S., “The Beriberi Heart,” Arch. Int. Med., 45, 1:1-22, January, 1930.
- Dustin, Weyler, and Roberts, “Electrocardiographic Changes in Vitamin B Deficiency,” New England J. Med., 220:15, 1939.
- Marvin, H. M., “The Therapy of Dropsy,” J. A. M. A., 114, 9:757- 763, March 2, 1940.
- Dublin, L. I., Correspondence–Metropolitan Life Insurance Co., New York City, 1941.
- Quigley, D. T., Notes on Vitamins and Diets, p. 74, Consolidated Book Publishers, Inc., Chicago, 1933.
- Taylor, E., “Preliminary Studies on Caries Immunity in the Deaf Smith County (Texas) Area,” J. Am. Dental Association, 31:428-432, September 1940.
- Shrader, J. H., Food Control, pp. 168-9, John Wiley and Sons, New York, 1939.
- Gillam, A. E., and Ridi, M. S., “The Carotene of Milk Fat (Butter),” Biochem. J., 1937, 31:251-253.
- Palmer, L. S., “The Chemistry of Vitamin A and Substances Having a Vitamin A Effect (Carotene),” J. A. M. A., 110, 21:1748-1752, May 21, 1938.
- Boer, J., “Antirachitic Action of Butter,” Acta brev. neerl. Physiol., 8:121-123, 1938.
- Osborne, T. B., and Mendel, L. B., “The Influence of Butter Fat on Growth,” J. Biol. Chem., 16:423-437, 1914.
- Sure, B., J. Biol. Chem., 74:1, 71-84, July, 1927.
- Schantz, E. J., Elvehjem, C. A., and Hart, E. B., J. Dairy Sci., 23:181-189, 1940.
- Hart, J. P., and Cooper, W. L., Vitamin F in the Treatment of Prostatic Hypertrophy, Lee Foundation for Nutritional Research, Milwaukee, Wisconsin, Report No. 1, November, 1941.
- Perlenfein, H. H., A Survey of Vitamin F, Lee Foundation for Nutritional Research, Milwaukee, Wisconsin, Report No.3, February, 1942.
- Turpeinen, O., “Arachidonic Acid for Fat Deficiency,” Proc. Soc. Exptl. Biol. Med., 37:37, 1937.
- Idovina, R., Graziano, C., Arch. Fisiol., 36:167-177, 1936.
- Fraps and Kemmerer, Tex. Agr. Exptl. Bul., 560, April 20, 1938.
- Supplee, G. C., Ansbacher, S., Bender, R. C., and Flanigan, G. E., “The Influence of Milk Constituents on the Effectiveness of Vitamin D,” J. Biol. Chem., 141, 1:95-107, May, 1936.
- Lorand, A., Health and Longevity Through Rational Diet, pp. 183-184, F. A. Davis Company, Philadelphia, 1912.
- Osborne, T. B., and Mendel, L. B., “The Stability of the Growth Promoting Substance in Butter,” J. Biol. Chem., 24:37-38, 1936.
- Morgareidge, K., and Manly, M. L., “Simultaneous Appearance of a Positive Line Test and Radioactive Phosphate Deposition in the Rachitic Rat Metaphysis,” J. Nutrition, 18, 4:411-421, October, 1939.
- McLester, J. S., Nutrition and Diet in Health and Disease, p. 242, W. B. Saunders Company, Philadelphia, 1940.
- Moore, C. U., Northwestern Medicine, XXVI, 1:30, January, 1927.
- Zeithraus, G. H., Neymark, M., and Widmark, E. M., “A Comparative Investigation of the Influence of Butter and Margarine on the Calcium Assimilation of Growing and Full Grown Rats in Full Vitamin Supply,” Contrib., 50, 9:32, 1939.
Bibliography for Disease Appendix
- Gutman, J., Medical Record, 146, July 21, 1937.
- Cova, “Congress of Obst. and Gyn.,” Journal of the American Medical Association, 110, 19:1618, May 7, 1938.
- Booth, M., and Hansen, A., Journal-Lancet, 57, 12:531, December, 1937.
- Sydenstricker and Wilson, Nutritional Disease Bul., Univ. Hosp. of Augusta, Georgia, February, 1940.
- Maynard, M., California and Western Medicine, 49:127, August, 1938.
- Stepp, W., Kuhnau, J., and Schroeder, H., The Vitamins and Their Clinical Applications, pp. 31, 101, 6, 10, 80, 90, 14, 28, 34, 29, 35, 27, Milwaukee, Wisconsin, 1938.
- Quackenbush, F., and Steenbock, J., Journal of Biological Chemistry, 123, 3:xcii-xcvii, May, 1938.
- Daft, Sebrell, Babcock, and Jukes, Public Health Report, 55; 1333, July 26, 1940.
- Romano, J., American Journal of Medical Sciences, 194:645, November, 1937.
- Pacini, A., Health Culture, 42-43, page 61, March, 1936.
- Baserga, A., Journal of the American Medical Association, 110,. 4:320, January 22, 1938.
- Sliosberg, Presse. Med., 58:906-909, December 8, 1939.
- Hospital Topics and Buyer, XVI, 11:30, November, 1938.
- Adamstone, F., Archives of Pathology, 31:603-612, 1941.
- Munro, D. C., Man Alive, pp. 100, 96, Bartholomew House, Inc., New York City, 1940.
- Hughes, E., abstr. by Chemical Abstracts, 33, 16:6393, August 20, 1939.
- Vilter, R., Aring, C., and Spies, T., Journal of the American Medical Association, 115:209, July 20, 1940.
- Bernheim, A., and London, I., Journal of the American Medical Association, 108:25, 2102-2109, June 19, 1937.
- Baker, A., Journal of the American Medical Association, 116, 22:2484, May 31, 1941.
- Steinberg, C., American Journal of Digestive Diseases and Nutrition, 3:765=786, December, 1936.
- Cornbleet, R., Archives of Dermatology and Syphilology, 31:224-226, 1931.
- Jolliffe, N., and Goodhart, R., Journal of the American Medical Association, 111, 5:380-381, July 30, 1938.
- Pray, R., Journal-Lancet, 58, 11:492, November, 1938.
- Eddy, W., and Dalldorf, G., The Avitaminosis: The Chemical, Clinical and Pathological Aspects of the Vitamin Deficiency Diseases, p. 52, Williams and Wilkins Company, Baltimore, 1937.
- Shipley, McCollum, and Simmond, Journal of Biological Chemistry, 49:399-410, 1921.
- Shepherd, M., Survey of Vitamin F in Cosmetics, p. 3, Pharmaceutical Spec. Company, Chicago, 1936.
- East, V., American Journal of Public Health, 28, 72-76, January, 1938.
- Koepke, G., Journal-Lancet, 57, 10:460, October, 1937.
- Langston, W., Day, P., and Cosgrove, K., Archives of Ophthalmology, 10:508-514, October, 1933.
- Smith, and Martin, Proc. Soc. Exptl. Biol. and Med., 43:660-663, April, 1940.
- Hecht, and Mandelbaum, Journal of the American Medical Association, 112:1910-1916, May 13, 1939.
- Quigley, D., Notes on Vitamins and Diets, pp. 15-17, Consolidated Book Publishers, Inc:, Chicago, 1933.
- Boyd, E., and Connell, W., Journal of the Canadian Medical Association, 37:38-41, July 19, 1937.
- Musser, J., Journal of the Medical Association of Alabama, 6:33-41, August, 1936.
- Jukes, T., Proc. Soc. Exptl. Biol. and Med., 42:180-182, October, 1939.
- Rattner, H., Harvey, C., Journal of the American Medical Association, 112, 25:2585-86, June 24, 1939.
- Hart, J., and Cooper, W., Report No. 1, Lee Foundation for Nutritional Research, Milwaukee, Wisconsin, November, 1941.
- Wilbur, D., American Journal of Digestive Diseases, 6, 610-617, November, 1939.
- Burr, G., and Burr, M., Journal of Biological Chemistry, 82:345-367, May, 1929.
- Mellanby, E., Journal of Physiology, 94:380-398, 1938.
- Shibata, M., Jap. Journal Exptl. Medicine, 9:21, 1939.
- Labbe, Nepveux, and Gringoire, Bul. Acad. de Med., Paris, 109:689-702, May 23, 1933.
- Marvin, H., Journal of the American Medical Association, 114, 9:757-763, March 2, 1940.
- Luckner, Zeitschrift f. d. ges. experimentelle medizin, 103~563, June 25, 1938.
- Mason, K., American Journal of Anatomy, 52, 153, March, 1933.
- Booher, L., Journal of Biological Chemistry, 119, 1:223-231, June, 1937.
- Jolliffe, Clinical Medicine and Surgery, 46, 12:501, December, 1939.
- Howell, W. A., Textbook of Physiology, Twelfth Edition, pp. 968-969, W. B. Saunders Company, Phiiladelphia, 1933.
- Sandels, M., Cate, H., Wilkinson, K., Graves, L., American Journal of Diseases of Children, 62:101-114,July, 1941.
- Cowgill, The Vitamin B Requirement of Man, Yale University Press, New Haven, 1934.
- Simpson, V., Tri-State Medical Journal, 12:2381-2387, November, 1939.
- Branch, A., Canadian Medical Journal, 41, 292-293, September, 1939.
- Journal of the American Medical Association, 113, 1:83, July 1, 1939.
- Vorhaus, M., his work reviewed in Science News Letter, July 3, 1937.
- Means, J., Journal of Clinical Medicine and Surgery, 44, 8 353, August, 1937.
- Mathews, A., Principles of Biochemistry, pp. 416-417, William Wood and Company, Baltimore, 1936.
- Stone, S., Journal of Pediatrics, 18.310, March, 1941.
- Becks, H. B., and Morgan, A. F., Journal of Periodontology, 18-30, January, 1942.
- Marvin, H., Journal of the American Medical Association, 114, 9:757-763, March 2, 1940.
- Richards, M., Brit. Medical Journal, 1:99-102, January 19, 1935.
- McKenzie, A., abstr. by Journal of the American Medical Association, 113, 8:723, August 19, 1939.
- Guhr, G., Journal of the American Medical Association, 112, 19:2001, May 13, 1939.
- Moia, B., and Batele, F., abstr. by Journal of the American Medical Association, 113, 23:2009, December 2, 1939.
- Wohl, M., Feldman, J., Endocrinology, 24:389, March, 1939.
- Means, J., Hertz, S., and Lerman, J., Annals of Internal Medicine, 11:429, September, 1937.
- Nacca, R., Reprint from Druggists Circular, July, 1935.
- Pacini, A., Wheat Germ Oil, Vitamin E, page 15, American Physician, Inc., First Printing, New York, 1935.
- Sure, Barnett, Vitamins in Health and Disease, page 187, Williams and Wilkins Company, Baltimore, Maryland, 1933.
- Willie, Southern Medical Journal, 33:1056, 1940.
- Boys, F., Surgery, 2:817-822, 1937.
- Knapp, A., Journal of the American Medical Association, 110, 24:1993-1994, June 11, 1938.
- Osborn, and Mendel, Journal of the American Medical Association, 69, 32, 1917.
- Modern Medicine, Editorial Section, 10, 2:122, February, 1942.
- Lamb, A., Journal of Biological Chemistry, 109, May, 1935.
- Schradt, E., Art. Med. Scandic., 84:456-495, 1935.
- Sebrell, W., and Butler, R., Health News, 7, 3:11, February 10, 1939.
- Pillat, A., and Chang, H., Chinese Medical Journal, 46.254, March, 1932.
- Reese, H., and Hodgson, E., Urologic and Cutaneous Review, 43:56-58, 1939.
- Spies, T., Vilter, R., and Ashe, W., Journal of the American Medical Association, 113, 10€931-937, September 2, 1939.
- Berglund, Medes, Huber, Longcope, and Richards, The Kidneys in Health and Disease, pp. 147-149, Lea and Febiger, Philadelphia, 1935.
- Fantus, B., Journal of the American Medical Association, 115, 6:450, August 10, 1940.
- Phillips, P., and Engel, R., Poultry Science, XVII, 6, November, 1938.
- Davis, T., Virginia Medical Monthly, 64:26, April, 1937.
- Luckner, Journal of the American Medical Association, 11, 9:879, August 27, 1938.
- Sydenstricker, Sevrell, Cleckley, and Kruse, Journal of the American Medical Association, 114:2437-2445, June 22, 1940.
- Sherwood, T., et al., Journal of Nutrition, 14:481-486, November 10, 1937.
- Druggists Circular, 84, 4:38, April, 1940.
- Meulengracht, E., Journal of the American Medical Association, 111, 25:2344, December 17, 1938.
- Schneider, E., and Widmann, E. Klin. Wchnschr., 14:1786, 1935.
- Joer, J., Arons, and Van Der Rijst, Archives, Neerland, Physiol., 22, 594-600, 1938.
- American Academy of Ophthalmology and Otolaryngology, paper read before meeting, October 9, 1939.
- McLester, J., Journal of the American Medical Association, 112, 21:2110-2114, May 27, 1939.
- Van Meeteren, Genessk. Tydschr. Nederland. Indie, 80, 2405-2431, 1940.
- Fein, Ralli, and Jolliffe, Journal of the American Medical Association, December 7, 1940.
- Hanson, F., Jahrbuck for Kinderheilkuncle, Basel, 151:136, April, 1938.
- Rubin, D., Endocrinology, 29, 2:281-287, August, 1941.
- Science News Letter, February 7, 1942.
- Jolliffe, Colbert, and Joffe, American Journal of Medical Science, 191, 4:515, April, 1936.
- Butturina, U., Giornale di Clinica Medica, 22:249-324, March 20, 1941.
- Richelts, American Journal of Obst. and Gyn., 38:487, 1939.
- Annual Review of Biochemistry, Stanford University Press, Stanford University, California, 4:371, 1935.
- Brunsting, L., Proc. Staff Meeting Mayo Clinic, May 4, 1938.
- Zondek, H., and Weiser, J., Wien. klin. Wchnschr., 50:63-64, January, 1937.
- Walker, K., Medical World, 57, 7:447-448, July, 1938.
- Modern Medicine, Editorial Section, p. 128, January, 1942.
- Sherman, and Smith, The Vitamins, Second Edition, Monograph Series, page 326, Chemical Catalog Company, Inc., New York, 1939.
- Department of Agriculture Yearbook, Food and Life, page 116, Government Printing Office, Washington, D. C., 1939.
- Kozelka, Hart, and Bohstedt, Journal of Biological Chemistry, 100:715-729, May, 1933.
- Desanctis, A., and Craig, J., New York State Journal of Medicine, 34:712-714, 1934.
- East, B., Journal of Medicine, 15:418-422, October, 1934.
- Drug and Cosmetic Industry, 41, 5:701, November, 1937.
- Sokoloff, F., Clinical Medicine and Surgery, 46, 12:478-481, December, 1939.
- Phillips, P., and Engle, R., Journal of Nutrition, 18, 227, 1939.
- Getz, H., Badger Quarterly, January, 1939.
- Perlenfein, H., A Survey of Vitamin F, Report No. 3, Lee Foundation for Nutritional Research, Milwaukee, Wisconsin, February, 1942.
- Modern Medicine, p. 90, April, 1940.
- Driver, Binkley, Sullivan, Clinical Medicine and Surgery, 45, 9:445, September, 1938.
- Krues, H., et al, work reviewed in Drug Trade News, 16, 15:34, July 28, 1941.