
Access to all articles, new health classes, discounts in our store, and more!
The Relative Efficiency of Medicaments for the Sterilization of Tooth Structures
Read before the National Dental Association’s Twenty-First Annual Session, New York City, October 23-26, 1917. Published in The Journal of the National Dental Association, Vol. V, No. 3, March 1918, pp. 273-303. Co-Author: Matilda Moldenhauer Brooks, A.B., M.S.
* * *
Introduction.
The existence of bacteria was discovered by Antony van Leeuwenhoek as early as 1675 but it was not until 1860 that their importance as causes of disease was indelibly impressed upon the consciousness of mankind. This was the beginning of antiseptic surgery and the discovery that certain drugs may be used to kill bacteria.
Owing to this discovery, a great impetus was given to literature, not only in the medical profession but also in the dental field, and methods of treating putrescence in pulp canals began to be suggested. However, it was not until 1895, thru the brilliant researches of Miller, Black and Williams, and later Fletcher and many others, that the importance of dealing with root canals of teeth as possible causes of systemic diseases was brought forcibly to the attention of the scientific world.
The importance of this problem, namely, the relative efficiency of the medicaments for the sterilization of tooth structures, is much greater than has been suspected by either the laity or the members of the dental and medical professions, for the reason that medication has not been doing what we supposed it was. While this topic would include the sterilization of infected tooth structures involved in ordinary dental caries, we have limited the study in this paper to the sterilization of infected dentin and cementum as involved in root canal infection, following the death of the dental pulp. Incidentally, it should be recalled that infection of the dental tissues constitutes not only probably the most universal of all human diseases but by many authors considered the most far reaching in its effects by the production of pain, and primary and secondary lesions. Our problem even when limited to the infected root tissues of non-vital teeth concerns all the members of the dental profession, as well as the patients whom they serve. It should be borne in mind that infected dentin and cementum are the almost universal cause of chronic periapical abscess, and the ultimate cause of the loss of the involved tooth root. This condition of infected dentin and cementum, with or without the assistance of accumulated infection in unfilled root canals, constitutes a contributing cause of a large number of secondary infections and systemic involvements. This is one of the most important unsolved problems connected with the practice of dentistry of today.
It is an exceedingly difficult problem of research to establish means for the sterilization of tooth structures in a way that will be without injury to the surrounding tissues. Our profession has not recognized its failures for several reasons. In the first place the involved tissues are very inaccessible, the approach being thru a small opening which must be followed for considerable distance. The clinical evidence has been exceedingly misleading to both patient and dentist. The criterion of success has been the local comfort and serviceability of the involved tooth. We now understand that these symptoms are not dependable; that the organism which can produce a low grade secondary infection frequently, if not generally, does not produce a local irritation in the primary lesion when these tissues in question are involved; that this infection of the dentin and part of the cementum can exist without apparently influencing the strength of the attachment of the tooth, and indeed, may produce a condensing osteitis which will increase the rigidity of the infected tooth root rather than diminish it. Another difficulty in studying this problem is that of reproducing the conditions involved. This is an important reason why more dependable work has not been done. Observations have been made by many men, as recorded in the dental and medical literature. These have furnished the basis for dental practice. It is important that the literature be reviewed and summarized, which we have, accordingly, herewith, done quite fully.
Historical.
Dental literature contains innumerable articles on the importance of the root canal problem, and many methods for the sterilization or “near” sterilization of this field of infection. Necessary as those first efforts are, they merely approach the ideal. A few of the most important articles are quoted which lead to the present day status.
The first to demonstrate the presence of bacteria in dental tubuli were Miles and Underwood, followed by Miller, who reviewed the researches of the former investigators and corroborated their statements and Sewell in 18851 who wrote extensively on bacteria in dental tubuli. Ingersoll,2 Garretson in 1895,3 Williams in 1892,4 Kirk,5 Grieves,6 Buckley in 1911,7 Rhein in 1909,8 Barrett,9 Gorgas,10 Truman in 1896,11 Abbott,12 Ottolengui in 1914,13 and others are advocators of different methods of disinfection, while Thoma14 advises the use of mild antiseptics and urges the operator to perfect his technic.
So many so-called antiseptics, guaranteed to produce certain results, are in use by the dental profession today that no uniform standard is maintained. As a result of this diversity in the treatment of root canals, confusion exists and queries from ocean to ocean voice this sentiment. Many writers have seen the lack of standardization in the treatment of root canals, among whom Von Herff in 191515 in his short discussion of the action of the various medicaments used in dentistry, gives reasons for their lack of efficiency, concluding that such standard drugs as iodin, alcohol, bichloride of mercury, cresols and their compounds are all of no account as disinfectants.
Brophy in 188016 states that carbolic acid and creosote have antiseptic, but not disinfecting, powers. He does not quote researches as evidence of this fact, or any references to the effect that these researches have ever been accomplished. LeRoy in 189717 advised deliquescent crystals of carbolic acid in treatment of pulpless teeth.
The following will give a slight idea of the non-conformity to standard methods: Burchard18 mentions the use of thymol and menthol, dissolved in glycerine as a canal medicament. Bodecker in 1886,19 in discussing the relative merits of iodoform, makes the following statement: “I fill the pulp chamber loosely with a piece of cotton saturated with the iodoform solution, and temporarily seal it. This plug I allow to remain from three to five days, before I attempt to clean out either the pulp or the root canal.” The inefficiency of this method is proven by subsequent experiments in this present research. Rhein in 1897,20 in discussing the treatment of root canals in abscessed conditions, mentions pyrozone as possessing strong antiseptical properties in the treatment of root canals and canaliculi. An interesting quotation in this connection, contradicting Rhein’s statement, is hereby given from McCurdy.21 He ranks iodin, U. S. P., mercuric chloride, and phenol in order of strength and discredits the use of hydrogen peroxide, as the following quotation shows: “As a matter of fact, the moment the liquid becomes effervescent, its power to destroy bacteria is ended. As the gas thus produced must push out in every direction, it carries before it not a germicide but an inert bubble. Hydrogen peroxide should not be used in a cavity because of its effervescence, for it distends the tissue and the inert bubbles carry infective germs deeper into the tissues.” If experiments proving this point are true, it seems that hydrogen peroxide would then be placed in the rear rank in the dental profession. There are many other methods for root canal treatment which are too numerous to quote.
In order to produce the ideal state of sterilization, no irritation to the tissues must ensue. In this connection Frahm in 191422 claims that the use of solidified formaldehyd, together with a slight amount of cresol, sealed up in a tooth is an excellent method for the production of sterilization. He gives clinical evidence but no researches. But further investigations by Black23 have shown that formaldehyd and cresol, or any of their compounds, are very injurious to tissue. This suggestion would, therefore, not be an ideal disinfectant.
Dunning24 states that “complete sterilization is produced within the zone of action by the use of metallic sodium and potassium.” There are no proofs mentioned, feasible as this statement may be. This author appreciates the necessity of going further than the immediate zone of action. In this connection Callahan in 1914,25 says “We have the testimony of several investigators that it is possible to sterilize the root canal properly, but it is an impossibility to sterilize infected dentin of a tooth while it remains in the mouth.” Brophy16 also claims that carbolic acid and creosote must not be stronger than a five per cent solution on account of the therapeutic action of the drugs, at the same time realizing that these are not disinfectants.
The contributing factors provided by the saliva, which are directly related to. the growth of bacteria, have been investigated by Marshall in 191526 and Gies in 1915,27 in studies on the salivary factor with reference to caries, and Rickert28 and Bunting28 have made an extensive study of this factor, in which they give experiments on the structure of individual differences in the teeth leading to the production of caries.
Some writers call attention to the undue stress laid upon the essential oils as disinfectants. Daufresne in 191729 mentions the fact that, under certain conditions, “bacteria and antiseptic are covered with fatty material which isolates them from each other and permits the bacteria to multiply freely.”
There may be a relation existing here between the use of the essential oils as is customary in the practice of dentistry and the action of fat as mentioned above. Further inquiry into this field may elucidate this statement and prove of value in the explanation of the non-bactericidal action of these essential oils.
Boyd30 gives a complete statement of the present status of root canal problem, and Callahan in 190931 briefly summarizes the position of the treatment of root canals in the following quoted statement: “Dr. Broomell,32 of Philadelphia, has recently given us a most excellent and helpful book under the title of Practical Dentistry by Practical Dentists. Under ‘Root Canal Treatment’ we find fifty-one different procedures, any of which may be thought the best. Under ‘Root Canal Filling’ we find seventy-one methods for sealing canals and keeping them forever sweet and clean. And yet we are not happy! Under head of ‘Treatment of Pulps and Pulp Canals,’ miscellaneous, we have sixty-six preparations, each one more potent than its predecessor.” Including treatments not here quoted there results a “Total of two hundred and eighty prescriptions and procedures for one poor sick little tooth!” And this was eight years ago!
A great step in the progress of the problem is the importance which nearly every article gives to the bacteriology of handling instruments used in dentistry, and the cleanliness and sterilization of these instruments. Best33 voices this sentiment. Miller in 1891,34 Hasseltine in 191635 and Kells36 believes that no sterile precautions need be used, maintaining that the medicament itself is sufficient to produce perfect results.
The most striking feature which is evidenced in reviewing the literature is the apparent lack of understanding concerning the meaning of the term “Sterilization.” There has been considerable confusion in the use of aseptic, antiseptic, disinfectant and germicide and bacteriacide. The general consensus of opinion of bacteriologists, as found in modern works such as Jordan,37 Dorlans’ Medical Dictionary,38 etc., places disinfectants, germicides and bacteriacides in the same category. An antiseptic is defined as being antagonistic to a septic state, or as being prohibitory to a septic condition, not necessarily producing sterilization but preventing further growth. To illustrate this point La Odontologia39 1913, shows an interesting comparison of the relative merits of antiseptics for use in the mouth, giving a table for the comparison of the amount of time required to produce antisepsis. From this one could not hope to produce sterilization in the oral cavity but a fairly respectable amount of antisepsis is possible. On the other hand “aseptic” is an ideal state in which no bacteria have ever occurred. For these reasons the only term synonymous with sterilization is “disinfectant.”
Dental literature is full of such expressions as “to thoroly cleanse” root canals, to make them “nearly sterile,” to “produce good results,” to “serve a good purpose,” to “have a good effect,” and so on. Polet in 191340 claims that the use of iodin, sealed in a canal, will disinfect any pulp debris that may remain in the canal and likewise in the apical region. Albrecht in 191341 advocates the use of resorcin-formalin in root canal treatment for the production of “normal” root canals, probably meaning sterile canals. In this connection, Hinman42 states definitely that, “in the treatment of septic canals, sterilization is accomplished first by washing out the canals with the hydrogen-peroxide bi-chloride of mercury solution. This is followed by the use of Schrier’s paste or the potassium sodium compound manufactured for this purpose. It has been found that if the canals are thoroly cleansed with this material that sterilization is nearly complete in every case.” Further on the author continues, “While I fully appreciate that there is no permanent antiseptic that we know of which may be introduced into the root canals, the iodin in the iodoform, which is set free in contact with moisture, does serve a good purpose in sterilization.”
In the search for a disinfectant, the use of silver nitrate has claimed the attention of many authors for a long period of time. Prinz43 gives a complete historical summary of the literature and practical details. Brooks44 calls attention to the value of this chemical in the treatment of erosion as early as 1854. Taft45 as early as 1859 expresses himself very favorably on the subject. Harlan in 1898,46 Truman in 189547 and Szabo in 1902,48 noticed remarkable properties in the use of silver nitrate in dentistry. Other recent endorsements on the subject come from Stebbins in 1891,49 Shanasy in 1898,50 Niles in 190051 and Bryan in 1903.52 Bethel in 189653 advocated the cataphoric method but the many disadvantages in its use prevented its general acceptance by the dental profession. Preiswerck in 190654 explains this phenomena in the following manner: “The favorable action of the argentic nitrate on the course of caries may be explained by the insoluble combinations which it forms with the organic tooth substance and thus withdrawing the nourishment from the bacteria. We may assume that the chemic process consists in the coagulation of the albumin and the formation of the albuminate of silver oxide. Miller in 190555 has proven that it is the precipitated black silver albuminate which acts principally as the resisting force, and not the silver chloride formed by the action of the silver nitrate upon the sodium chloride always found in animal tissues, which is responsible for the disinfecting powers of the silver combination. Hence, the significance of Black’s, in 190856 dogmatic postulate: “Expose the tooth structure treated with silver nitrate to the sunlight until it.turns black.” Whitslar in 189757 states that cataphoresis drives AgNO3 to the ends of the tubuli. Hartzell in 191258 mentions the prophylactic treatment of silver nitrate in which he says that this medicament can be rubbed into the gums and the roots of the teeth as a prophylaxis three or four times a year.
A step further in the efficiency of disinfectants has been accomplished by Dakin in 1917,60 when he advocated the use of chlorazene, and later Dichloramin-T,61 in surgical wounds. The two principles of an ideal disinfectant, namely, the killing of bacteria and the absence of injury to the cell of the living body, also applies to dentistry. Dakin,60,61 and his co-workers, are accomplishing this aim in surgery. Some practical applications of chlorazene and dichloramin-t to dentistry are stated in this paper.
It is a remarkable fact that the researches in this connection are practically a new field. A deeper insight into literature will reveal numerous references to the lack of such knowledge, and very few investigations, leading to solutions of the difficulty. Dahlgren in 191762 calls attention to the works of Boennecken of 191363 and Blessing in 191464 as a few of the genuine inquiries into this line of research.
Blessing’s64 studies consisted of the use of “Phobrol” (Cresol Preparation), thymol alcohol and aqua regia, which he places in the first rank; antiformin, Perugen and tricresol formalin in the second rank.
Boennecken63 placed thymol alcohol, chlorophenol, aqua regia and formalin in the first rank, and tricresol formalin, sodium hydrate, phenol, chloral hydrate, balsam of Peru, antiformin and eugenol in order of their efficiency.
As pointed out by Dahlgren,62 both of these authors place a high value upon thymol alcohol and aqua regia. Dahlgren62 has carried out these experiments still further. He has used fifteen of the most widely used preparations of the present day and in some cases has given two treatments where one did not suffice. In his experiment the teeth were placed in sterilized plaster of paris, infected medium placed in the canals of the teeth in this position, and two treatments were given where one did not produce a sufficient percentage of sterilization. As a result of these experiments, Dahlgren ranks formalin, tincture of iodin, chlorophenol, formocresol and iodin creosote in the first rank, without obtaining one hundred per cent efficiency in any case.
The author emphasizes the importance of further inquiry into the extent to which dentin can be disinfected and the role played by accessory canals, and also points out the necessity of sterilization in the elimination of infection.
To further test the efficiency of present day methods in the treatment of root canals, and to throw more light on the present vague results which follow the use of certain specified medicaments, the following experiments haye been conducted during the Spring and Summer of this year at the Research Institute of the National Dental Association.
Outline of the Problem and Our Approach to It.
In attacking this problem we have outlined it as follows:
We have recognized that the following structures and conditions exist as important factors:
First, the pulp canal to which the infection has access and thru which the infection can reach the dentin. Second, the dentin with its tubuli. Third, thru the foramen or foramina the infection can reach the cementum, which probably can also be infected from the dentin. Fourth, the periapical tissues which constitute not only pabulum but also a locked area which may contain an infected culture medium, which may reinfect cementum and dentin and pulp canal contents.
We have arranged our experiments in the following order:
- A study of the ability of the medicaments to sterilize dentin and cementum under the most ideal conditions, irrespective of compatibility with clinical conditions.
- The study of the ability of the medicaments to even retain the sterility of a medicated dressing when placed in an infected root canal without the influence of a periapical infection.
- The influence of a periapical infection upon these last named conditions.
- The ability of medicaments placed within the root canal to sterilize infected dentin and cementum while these tissues are surrounded by a periapical infection; including a study of the areas of these structures that are most readily sterilized.
- A study of the time factor.
- A study of Silver-Ammonium-Formalin and Dakin Solutions.
Experiment I.
Purpose. This experiment was undertaken as a rough draft on the efficiency of medicaments.
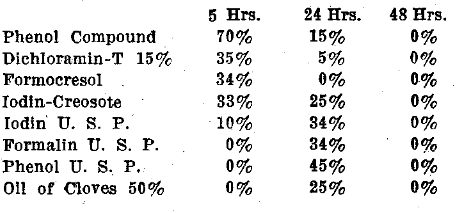
Materials. One hundred and ten different medicaments, including the various per cent-dilutions, were used. These are enumerated below:
Salicylic Acid, in aqueous and alcoholic solutions, and Na, Mg and Quinine Salicylates in aqueous and alcoholic solutions, 32 dilutions.
Three separate series of observations were made for this experiment, and each series included ten teeth for each medicament, making 1080 teeth for each of the three series or 3240 teeth for this one experiment.
It proved to be an exceedingly difficult matter to procure a sufficient number of freshly extracted straight rooted teeth, for which reason it became necessary to use for a part of the observations teeth that had been dried and saturated with moisture, and also for some of the observations we sterilized the teeth by boiling on successive days and freshly reinfecting them after saturating them with culture media. We did not run controls to determine whether results were different with freshly extracted infected teeth and teeth which had been reinfected after being dried. However, several sets of teeth are comparable and show practically the same uniformly negative results where the teeth were boiled and infected as where they were known to be freshly extracted infected roots.
A mixed culture of bacteria from the mouths of several persons, producing a heavy growth in one per cent dextrose bouillon broth after two days incubation at 37° C., was used for the first and third series and a pure culture of oral streptococcus isolated in the laboratory, was used for the second series.
Procedure. The teeth were prepared by cutting off the crowns with a circular saw and opening up the root canals with reamers thru the apex. The air was eliminated from the teeth by placing them under a bell jar attached to the exhaust pump in which condition they were emersed by changing the center of gravity of the bell jar, which dumped them into infected culture media and the atmospheric pressure was restored. They were then placed in the incubator at 37° C, for from four to five days. At the end of this time a medicament was pumped into sets of ten teeth each and the ten teeth were then submerged in the medicament for 24 hours. The acids received special treatment which will be explained in detail later.
The three parallel series have the following relationship to each other:
Series 1 was to determine in general the relative and actual efficiency of the various medicaments for sterilizing tooth structures which had been contaminated with mixed oral infections.
Series 2 was to determine the efficiency of those medicaments in sterilizing similar tooth structures when the infecting organism was a pure oral streptococcus and to check the technic.
Series 3 was made partly as a control for series 1 and partly to determine whether teeth that were infected in the mouth and freshly extracted would give the same results as reinfected teeth that had been allowed to dry. In this series all the teeth used in the first 71 medicaments or 710 teeth had been freshly extracted.
In the mixed culture no special bacteriological precautions for sterility were taken up to this point. However, after treatment for 24 hours all precautions were used and the teeth taken out of their medicaments and placed in series of tens upon sterile watch glasses. A number of these watch glasses were continuously boiled during the operation of transference and were used to hold the teeth during the next step, which consisted of pumping the canals with water previously sterilized and getting rid of as much of the medicament as possible. Each tooth was then picked up with a pair of forceps flamed before each operation and placed in sterile dextrose bouillion and incubated for 15 days. Results were recorded at the expiration of one, two, three, four, five, six, seven, eight, nine, eleven, thirteen and fifteen days. (See Chart 1).
Each acid was used by immersing the tooth in it in a watch glass and the medicament pumped in for five minutes instead of 24 hours, and then neutralized with a sterilized sodium bicarbonate solution until all chemical activity had ceased. Each tooth was then thoroly washed in sterile water so as not to afford any cause for decrease in growth, by modification of the medium and placed by means of sterile forceps in sterile dextrose broth and incubated for 15 days as mentioned above.
In the second trial, consisting of the pure culture of the streptococcus, the procedure was slightly modified. The teeth were sterilized intermediately for four days in the autoclave at a pressure of thirty pounds for one hour. They were then allowed to incubate for forty-eight hours to test for sterility, after which they were inoculated with the pure culture of streptococcus previously isolated and allowed to grow for four days. A smear proved the exclusive presence of the streptococcus. The teeth were placed in the infected culture medium under a reduced atmospheric pressure as previously described but in this case all the instruments used were sterilized to keep the culture pure.
Difficulty was experienced in sterilizing infected teeth even by repeated autoclaving, B. subtilis proving very persistent. After several trials we succeeded in producing an infection of the tooth structure with the single organism-streptococcus from the mouth.
In this series, the same method in general was used as in the previous series except that a smear was made of all tubes which showed growth, to check the infection. In this way it was possible to ascertain whether these tubes contained the culture from the original infection or whether the cloudiness was due to an accidental contamination thru error in the technic.
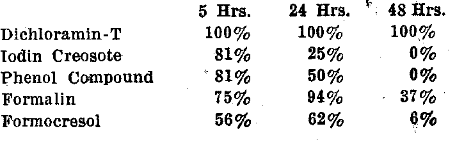
Results. Briefly stated, the results of these three series of determinations may be summarized as follows:
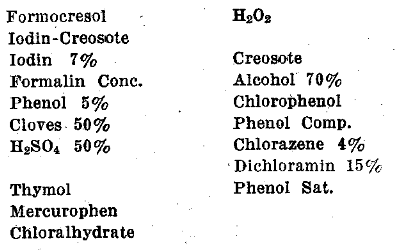
- Even under ideal conditions where the medicament bathes both the inner and outer surfaces of the infected tooth structure and even where the mass of the medicament is relatively large and without consideration for the compatibility to surrounding tissues, the dentine and cementum were not disinfected except with a few medicaments, namely, formalin in all strengths, iodin 5% and Chlorphenol.
The great majority of the results were negative and in direct contradiction to the general teachings and expectations in current dental practice. These results have determined the details for the next series of experiments. Before outlining these we give here in full detail the results of the three series.
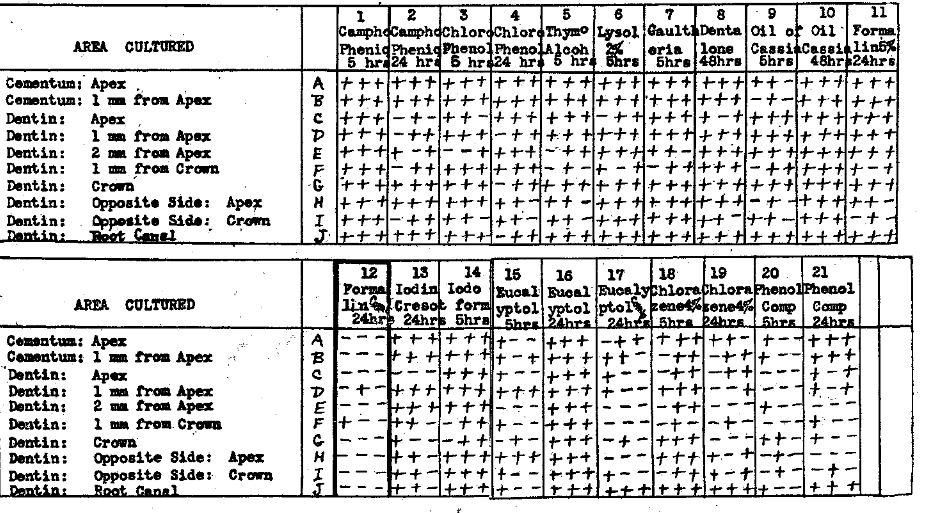
Chart No. 1 shows clearly the inhibiting effect of certain agents. Ten teeth being used, it will be noted that frequently it required three or more days before any growth appeared in even a few of the tubes, with other tubes showing growth as days went on. With Oil of Cassia the first growth appeared on the 8th day with pure strep. and with Thymol Alcohol on the 15th day. The pure culture of strep. indicated that it was not a contamination. Iodin and Creosote also showed a marked delay in the growth.
Experiment I, Chart 1–Determinations of the Ability of Medicaments to Sterilize Infected Dentin and Cementum when Emersed in them for Varying Periods of Time and the RCelation of the Incubation Time Factor to the Efficiency.
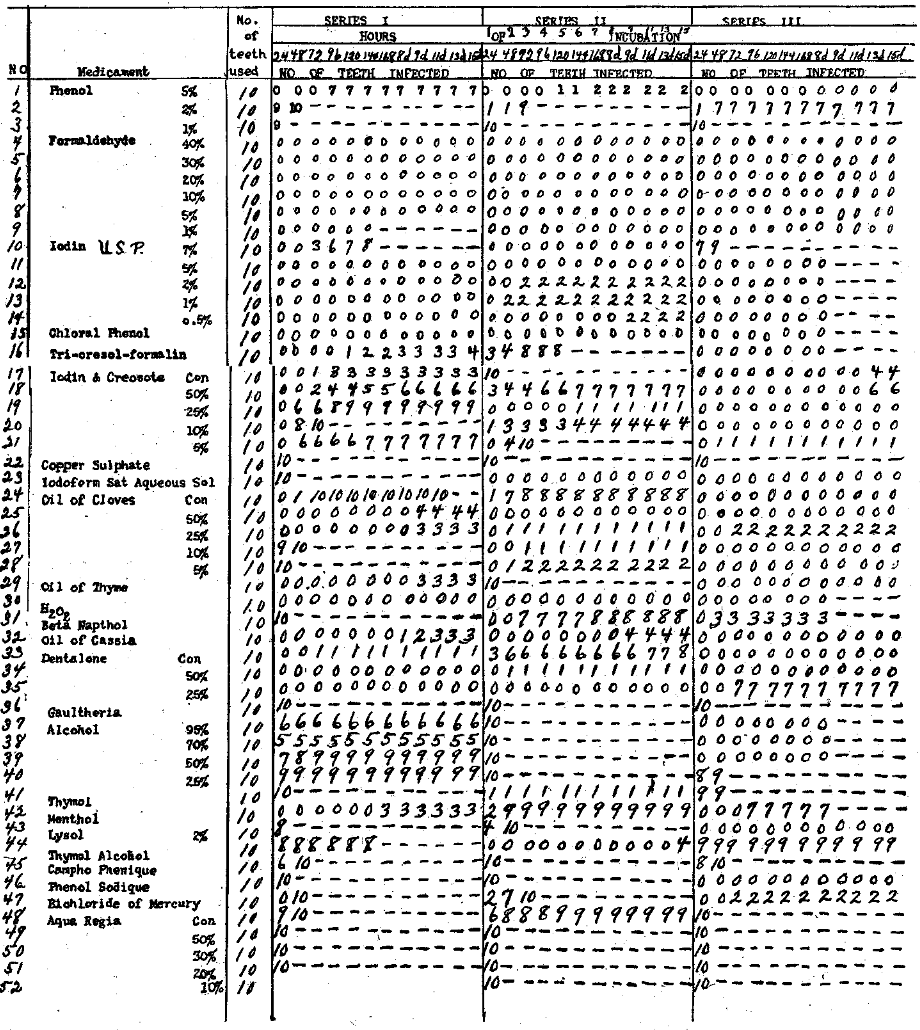
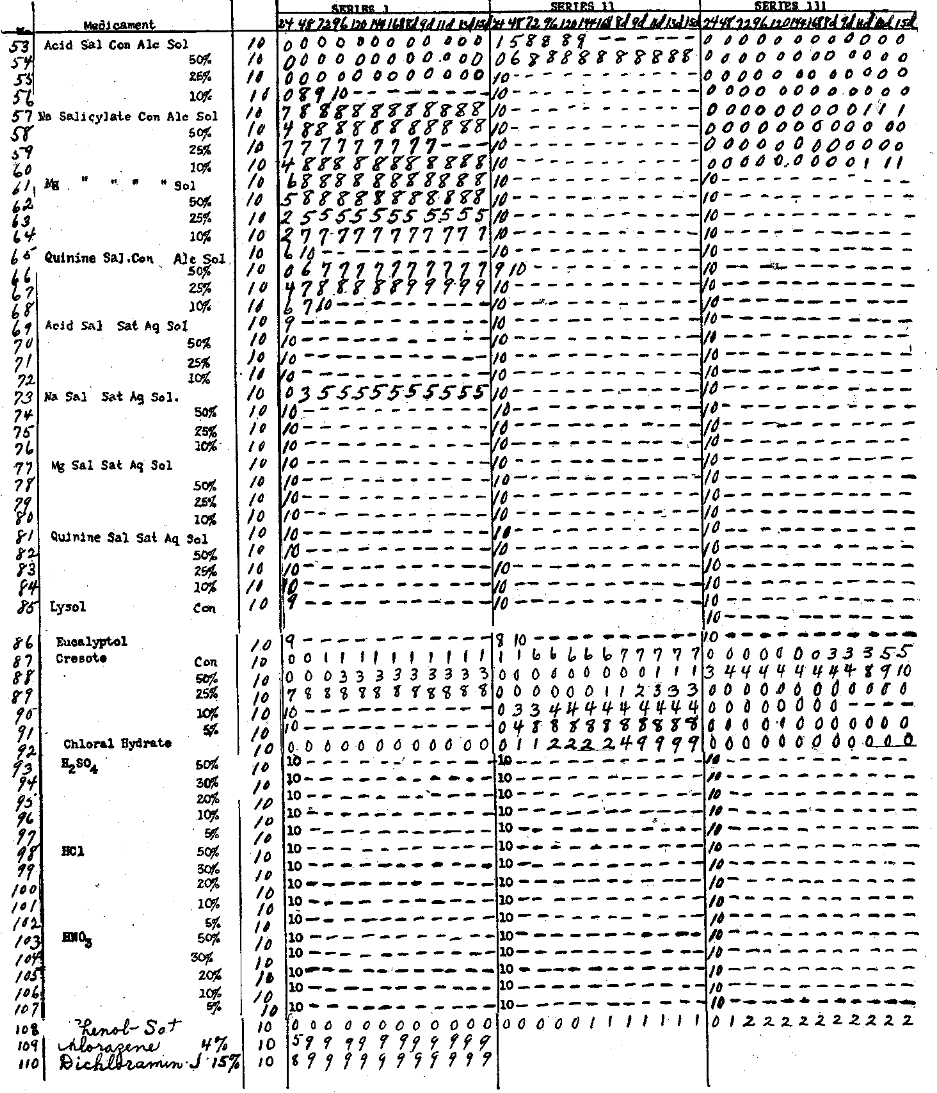
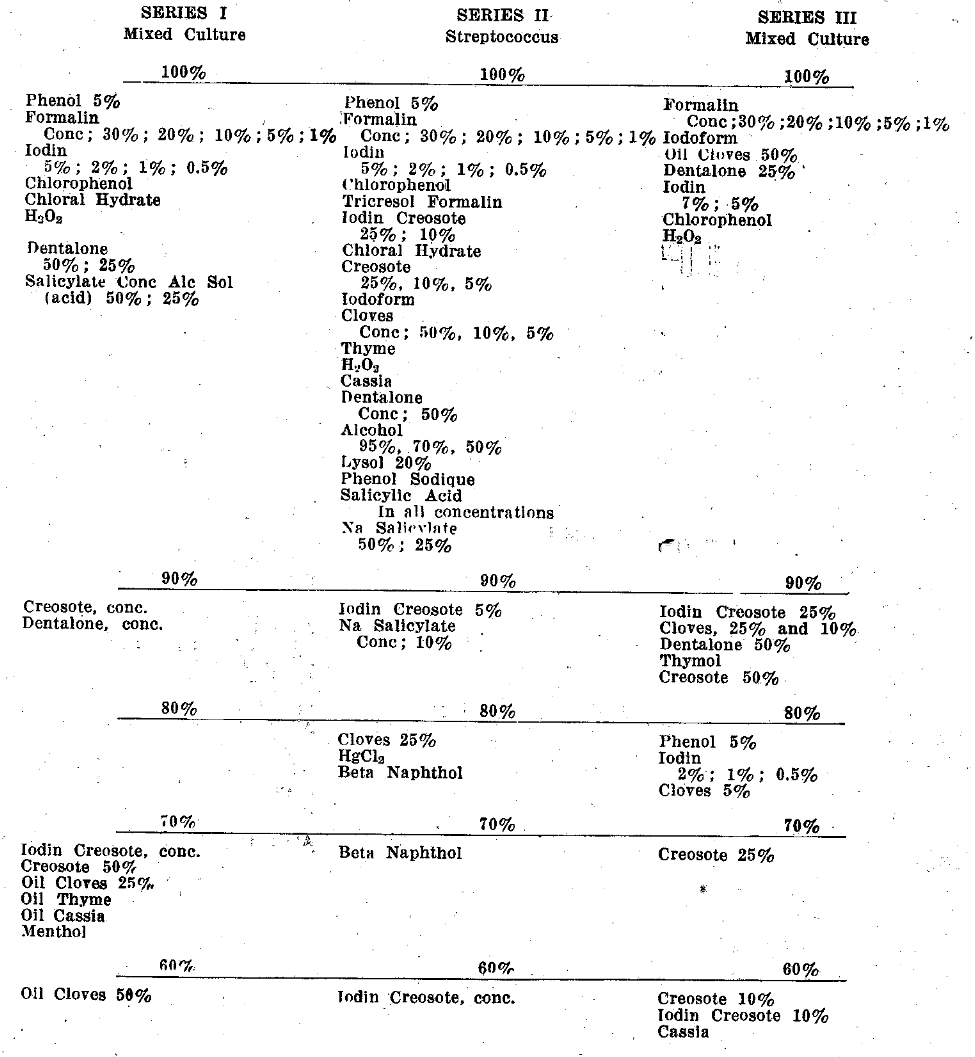
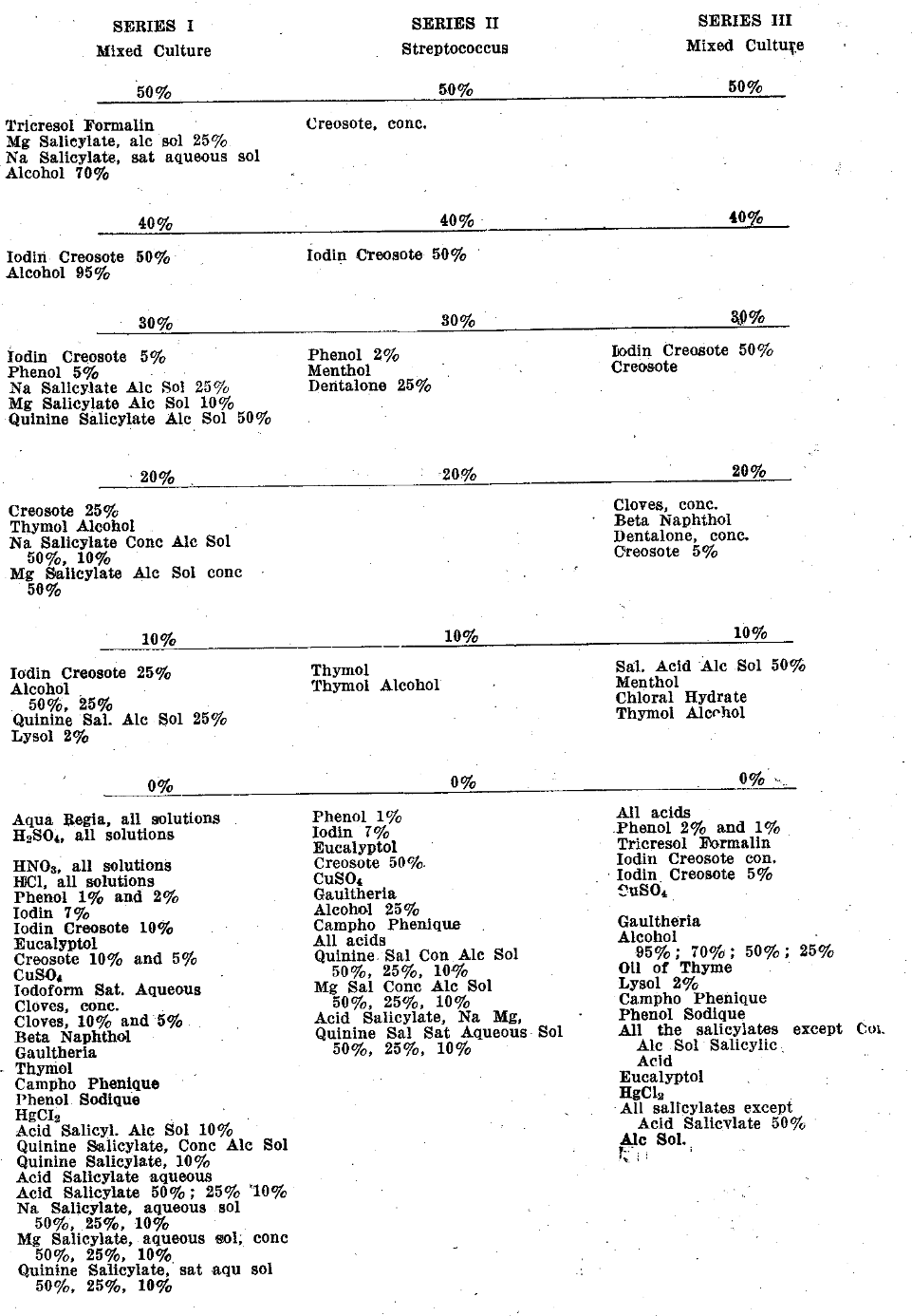
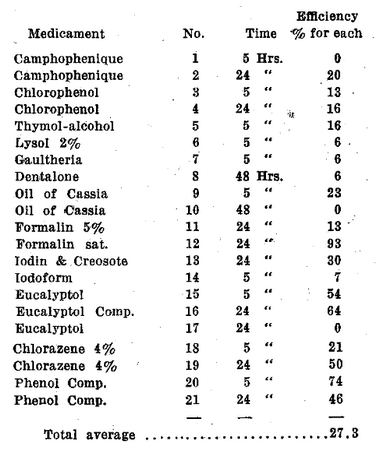
Chart No. II is an analysis of the information in Chart No. 1 with the efficiency expressed in terms of per cent. It shows very strikingly the low efficiency of the acids and the high efficiency of the formalins and a few others. This chart also shows graphically the relative efficiency of different concentrations.
Experiment No. I, Chart 2–Analysis of Chart No. I, Demonstrating the Efficiency of Medicaments for Sterilizing Infected Tooth Structures.
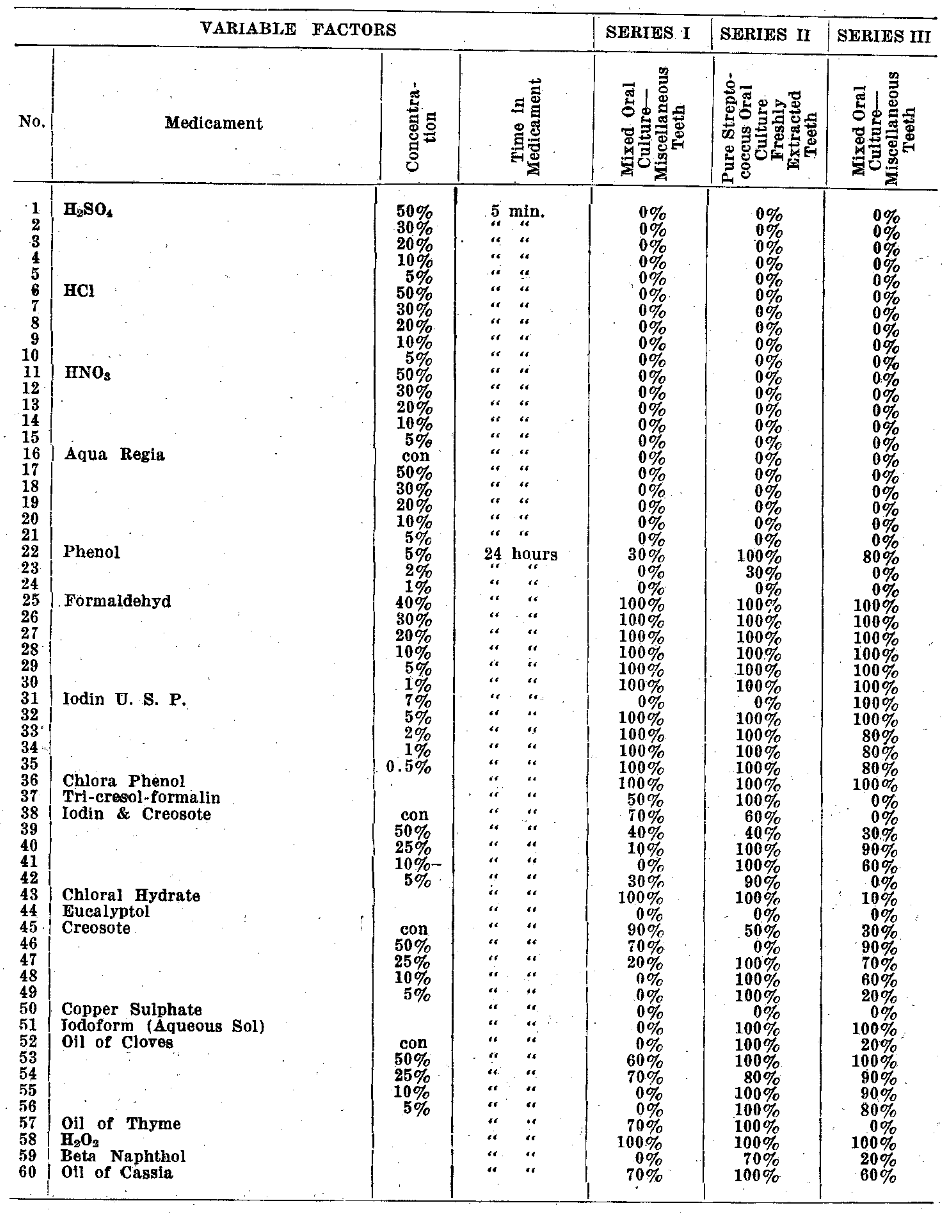
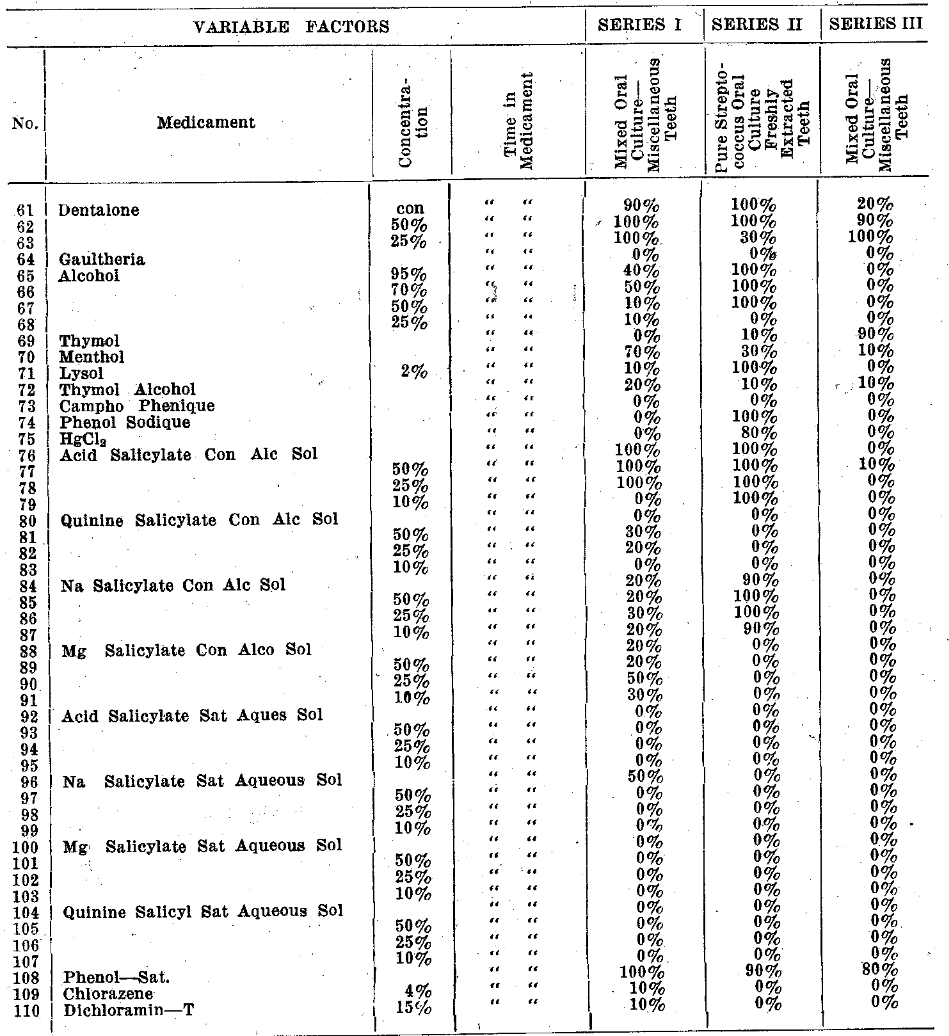
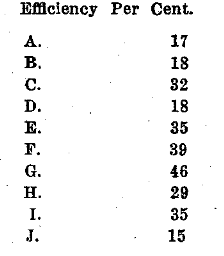
Chart No. III shows all the 100% drugs together and also the same for each range of 10 per cent. Note the greater efficiency for strep. The majority of these drugs appear, however, in the zero group.
Experiment I, Chart 3–Results in Order of Efficiency of Medicaments.
While the results obtained in experiment No. 1 are exceedingly important and suggest the measure of our failure to sterilize dentine and cementum the conditions are not identical or even similar to those in the mouth and hence the necessity for making a series of determinations which could be considered as comparable to practice. The divergence of the conditions prevailing in experiment No. 1 from the normal and the details for making a more nearly comparable experiment are suggested by a comparative study of the two sets of conditions as follows:
- In all these cases where the tooth was placed in the medicament of stated concentration for 24 hours and washed in sterile water and transferred to culture broth, the medicament came in contact with both the inner and outer surfaces of the tooth instead of only the inner surface.
- The ration of the volume of the medicament to the volume of a tooth is reversed from practice and such that there would be but slight reduction in the concentration of the active agent at any tooth surface.
- The total amount of the medicament that can be placed in the tooth is exceedingly small, but in the experiment it was very large.
- There was no adjoining fluid which could remove a part of the active sterilizing elements by diffusion which the periapical fluids do by their contact thru the foramina.
- There was no mass of infecting medium in such relation to the tooth structure as to promptly reinfect.it after a neutralizing or diffusing of the medicament which occurs from the infected periapical fluids.
- No consideration was necessary of the destruction or injurious action of the medicament on the adjacent or surrounding tissues. Most medicaments that will destroy bacterial cells will destroy tissue cells.
Summary of Experiment I.
It is very difficult to destroy bacteria growing in dentin and cementum.
Experiment II.
Determinations of the Ability of Medicaments to Maintain the Sterility of the Root-Dressing when Sealed in an Infected Root and Without the Perforated Root-Apex Being Immersed in an Infected Culture Medium.
Purpose: This experiment was conducted to show the results of the present day methods of root canal treatment in scientific terms, and to emphasize for the dental profession the efficiency of the various medicaments which it uses in every-day practice. In this paper there is no emphasis laid on the proper number of treatments, and how many would be needed in each case to show the optimum power of each medicament. It shows merely the inadequacy of the common practice of applying a treatment a certain length of time with the delusion that this may produce sterilization throughout all the tooth structures.
Procedure: A carefully selected number of medicaments which gave promising results in Experiment I was used. These are as follows:
Two hundred and sixteen freshly extracted teeth were procured and prepared for experimentation as in Experiment I. They were cultured in a mixed salivary infection for from four to six days, when they were ready for treatment. No pure cultures of bacteria were used and no attention was paid to species of bacteria. There was only one treatment given in each case. A series of five, twenty-four and forty-eight hour treatments, including four teeth for each period of time were run.
In endeavoring to make the conditions as nearly comparable as possible to the conditions as found in the mouth when no periapical infection exists, the following method was used:
The teeth were taken out of the broth infected by saliva and a J. & J. absorbent point, soaked in the medicament, was carefully inserted in the root canal down to the apex, under sterile precautions. The entire tooth was then placed into sterile tubes containing a small amount of moistened cotton, and then placed in the incubator for the length of time charted for that series. At the end of that time they were taken out of the test tubes and sterile forceps used to pick out the absorbent point. This was then cut into four pieces with sterile scissors which were carefully flamed between each cutting.
Each piece of cotton was then dropped into sterile tubes of dextrose broth and labeled “A, B, C, and D” respectively from the apical to the crown end of the absorbent point.
Results were recorded at the end of 72 hours. Chart 4 gives a complete record of all positive and negative cultures obtained.
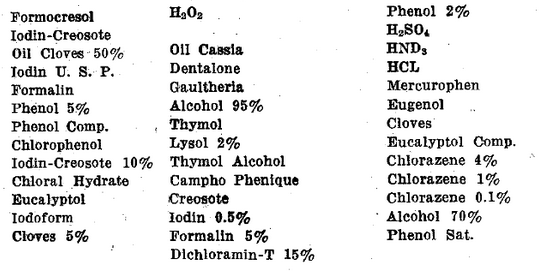
Results: Of the 18 medicaments used for this experiment, only six gave any negative results in cultures; the remainder were all positive cultures in every case for the complete series of hours run. There was only one medicament which produced 100% efficiency and that was Dichleramin-T of Dakin.
The medicaments approaching any degree of sterilization are as follows, in order of five, twenty-four and forty-eight hours efficiency:
Thymol, creosote and chlorophenol.showed antiseptic but not sterilizing properties.
Several experiments were conducted upon a rabbit’s ears to prove whether or not the medicament produces eschars. A subcutaneous inoculation was made with iodin-creosote, phenol compound, dichloramin-T and chlorazene 4% aqueous solution as used in the experiments.
Chlorazene and iodin-creosote produced no eschars, but dichloramin-T and phenol compound gave small eschars with a great amount of irritation in the case of dichloramin-T. Probably this was due to the 15% solution used in the dichloramin trial. One rabbit died instantly from the ear injection of Phenol compound. It is probable that it entered a vein which, however, could not be seen.
Conclusions: The most radical disinfectant was dichloramin-T. This medicament in a concentration of 15% as used in this experiment gave 100% efficiency in all treatments but also produced irritation of living tissue.
A further observation on the lowest percentage needed for root-canal sterilization and the amount of time for the production of this condition will be continued. This drug may, in dilute solutions of 1% or less, be both safe and efficient but it is one of the most painful and destructive agents we have tried in practical cases. The members of the profession are warned never to place the 15% or even a 5% solution of the Dichloramin-T in oil of Eucalyptol, its solvent, in any tooth or on tissues.
Experiment II, Chart 4–Determinations of the Ability of Medicaments to Maintain the Sterility of the Root Dressing When Sealed in an Infected Root Without Periapical Infection

Experiment III.
Determinations of the Ability of the Medicaments to Maintain the Sterility of the Root Dressing When Sealed in an Infected Root When the Perforated Root Apex IS IMMERSED in an Infected Culture Medium.
Purpose: This experiment was conducted to show the results of the present day methods of root canal treatment in scientific terms, and to emphasize for the dental profession the efficiency of the various medicaments which it uses in every day practice when the tooth root is surrounded by a periapical infection. There is also no emphasis laid on the proper number of treatments, or whether these disinfectants could be brought to produce sterility by a repeated number of applications.
Procedure: From the medicaments which gave the best results in Experiment I the following forty were carefully selected:
Six hundred freshly extracted teeth were procured and prepared for experimentation as in Experiment I. They were cultured in a mixed salivary infection for from four to six days, when they were ready for treatment. No pure cultures of bacteria were used and no attention was paid to species of bacteria. There was only one treatment given in each case. A series of five, twenty-four and forty-eight hour treatments, including five teeth for each period of time, were run.
The aim of the experiment was to make the conditions of culture as nearly comparable to the conditions of the mouth as possible. For this reason infected broth was used to culture the teeth after they had received treatment, because a broth containing living organisms surrounding an apex is like the abscessed condition of a peridental membrane in which the tooth in the mouth rests.
The following method was employed: The infected teeth were taken out of the broth and a J. & J. absorbent point, soaked in the medicament, was carefully inserted in the root canal of the tooth down to the apex. The crown was then paraffined to the gingival margin and the tooth placed into the test tube containing about 6 cc. of infected broth, placed in the incubator according to the length of time charted out for that series.
At the end of the allotted time, they were taken out of the infected broth, dipped into 70% alcohol to wash off the main mass of bacteria on the outside of the paraffin, and then placed on a sterile petri dish to dry the exterior. The paraffin was carefully lifted off by slightly melting the gingival margin of paraffin and lifting it with forceps without touching the absorbent point. A sterile forcep was used to pull out the absorbent point which was then cut into four pieces with sterile scissors which were carefully flamed between each cutting. Each piece of cotton was dropped into a sterile tube of dextrose broth and labelled “A. B, C, and D,” respectively, from the apical to the crown end of the absorbent point.
Results were recorded at the end of 72 hours. Chart 2 gives a complete record of all positive and negative cultures obtained.
Results: Of the 40 medicaments used for this experiment, only eight gave any negative results; the remainder were all positive in every trial for the complete series of hours run. With the infected medium used in which to incubate the treated teeth no 100% efficiency was obtained. The medicaments approaching any degree of sterilizing ability are as follows in order of five hour efficiency:
The best of the above results is Phenol Compound prepared according to Buckley’s Prescription, but even 70% is not a very high degree of efficiency attained. All of the medicaments showed zero efficiency in a 48 hour treatment, but varied in the per cent of efficiency in the five hour and the 24 hour treatments.
The medicaments not mentioned above all gave zero efficiency in all three of the series of hours, and prove their absolute worthlessness in one treatment for so short a period as five hours, not to say anything of the amount of growth which has taken place at the expiration of 48 hours.
A chart in this connection was made, which was plotted to contain the percentages of all of the cultures under the various areas of each of the series of hours. In referring to the chart, it will be seen that the highest percentage efficiency is in the areas “C” and “D.” These areas were the ones which did not come in contact with the infected medium and may be explained as not having had a long enough period of time in which the medicament would diffuse with the broth in contact. Aside from this explanation, the factor of accessory canals and tubuli containing bacteria which are not reached by medicament must be considered.
The grand total efficiency counts all negative areas in any one medicament irrespective of areas from which it is taken.
Experiment III, Chart 5–Determinations of the Ability of Medicaments to Maintain the Sterility of the Root Dressing When Sealed in an Infected Tooth Root When the Perforated Root Apex is Emersed in an Infected Culture Medium

This experiment might have been carried on further by replacing the piece of cotton with a new sterile piece and after 72 hours culturing the sections as the above was cultured. Experiments are now in progress which will show the exact amount of time required to obtain maximum efficiency by giving the medicament every opportunity for producing best results.
Eucalyptol, thymol and creosote show remarkable antiseptic qualities in delaying the growth of bacteria, which, on further incubation produced positive cultures.
Conclusions: Under the conditions specified above, the medicaments used in the previous experiment are not ideal disinfectants for the following reasons:
- They do not produce 100% efficiency.
- Formalin and its compounds Dichloramin-T and creosote in strengths used have been shown to produce tissue suppuration.
- Iodin compounds produce dark stains.
- The difference between antiseptics and disinfectants was shown in the results obtained from the use of Eucalyptol, thymol and creosote. The interpretation of this experiment is probably that the penetration of the disinfectant is not sufficient to reach the remote and minute recesses of the tubuli.
Having satisfied ourselves that this is a chief reason for non-sterilization of the tooth, it remains to find some disinfectant that will meet with these requirements and fulfill the desired efficiency. This is the subject of the remaining experiments, altho these are not yet completed and require more time.
Experiment IV.
Determinations of the Ability of Medicaments to Sterilize Infected Dentin and Cementum when Sealed in the Root Canal, and when the Perforated Apex is Surrounded by Infected Culture Medium, as per Condition in Experiment III.
Purpose: After the results obtained in the previous experiments, it was deemed advisable to determine to what extent the infected dentine and cementum of the teeth have been sterilized by root canal medication.
Procedure: A number of teeth, 63 selected, according to results obtained from the previous experiments were used. These were handled with sterile precautions in the following manner:
They were taken out of the vessels containing them and placed in 95% alcohol for a few minutes and then the surface allowed to dry on a sterile petri dish. All instruments used in handling them were flamed until hot, dipped in alcohol and this again burned off, before, and after operation. When dry the teeth were placed one by one between sterile paper and clipped longitudinally in half with heavy plate shears. Cultures were taken from the freshly cut surface with a fine pointed bur, sterilized by flaming before each use. The ten areas from which cultures were taken are as follows:
A. A small amount of the cementum from the apical end, external surface.
B. A small amount of the cementum about 1 m.m. from the upper apex, external surface.
C. The dentin from the inside of the split tooth at the apical end near the cementum.
D. The dentin from the inside of the split tooth about 1 m.m. from the apical cementum.
E. Dentin from the same area about 2 m.m. from apical cementum.
F. Dentin about 1 m.m. from the crown, from inside of split tooth.
G. Dentin from inside of split tooth at crown region.
H. Dentin from the opposite half of split tooth, inside area, apex.
I. Dentin from opposite half of split tooth, inside area, crown region.
J. Dentine scraped from entire surface of pulp canals.
Figure 6 shows a diagram of a tooth with these areas indicated.
Experiment IV. Fig. 6
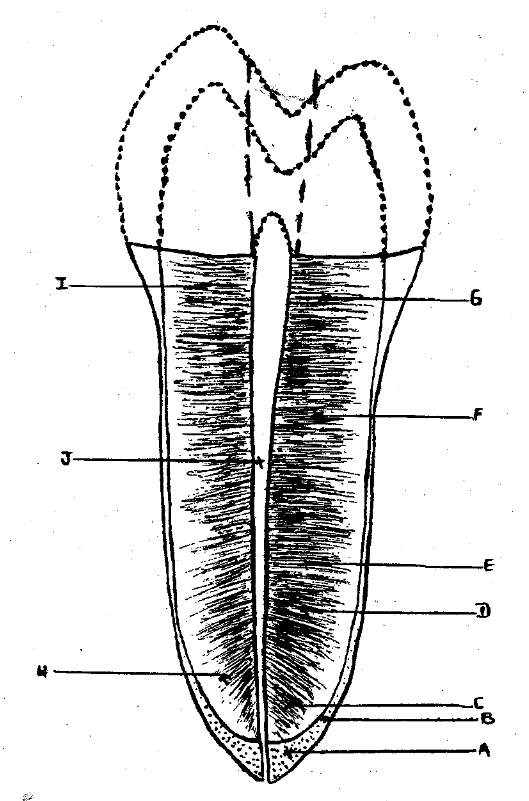
Diagram Showing Areas from Which Cultures of Dentin and Cementum Were Taken.
Results: Chart 7 illustrates the results obtained in each individual case. All positive signs indicate growth of bacteria, all negative signs show absence of growth, therefore efficiency. The areas cultured are lettered from A to J according to the region from which they were taken.
The accompanying diagram gives a more concise idea of these results which were obtained by taking the percentage of all the results obtained under each area respectively not considering the medicament from which each was taken. In no structure or area was the efficiency high.
Summary I.
The second summary, given below, shows the results obtained by percentage efficiency of each medicament not considering the areas from which each was cultured. Note the very low net efficiency.
Summary II.
With the exception of formalin which shows 93% sterility, all other teeth show a general infected condition of the tooth structure.
Conclusions:
- The low percentage of efficiency and the corresponding high percentage of general infection is a very definite proof of the general infection which is found in the teeth.
- That, with the above medicaments the sterilization of a root canal, does not necessarily sterilize the surrounding tooth structures.
- That the efficiency of a medicament to sterilize all tooth structures should be the criterion of a disinfectant. The criterion of a competent root canal medicament is its ability to sterilize all infected tooth structures.
Experiment V.
Determinations of the Ability of Double Salt of Ammonium Silver and Formalin to Sterilize Infected Dentin and Cementum when Applied in the Root Canal.
Purpose: The action of formalin as a test for silver has long been known in chemistry but dental application of this fact is probably of recent suggestion by Dr. Howe.59a There are frequent references to the toxicity of silver in the last decade. To correlate this past knowledge, test it and observe in experimental medicine whether it would be used as an efficient disinfectant in the treatment of root canals, has been attempted.
Materials: A number of freshly extracted infected teeth, which had been placed for a few days in saline solution, were used. The crowns were removed with a circular saw and canals opened, as in the previous experiments.
A 35% solution of silver nitrate, with the addition of NH4OH until the precipitate has just redissolved, and a 25% solution of formalin was used as a precipitating solution. The method of conveying these solutions to the tooth was by means of a capillary pipette with rubber bulb. Sterilized glass plates were used upon which the teeth lay. A blast of hot air was used for hastening the chemical reaction or precipitation of the silver. A sterile broach was also used to force the medicament to the end of the canal.
Procedure: The teeth were held with sterile forceps and one drop of the silver nitrate NH4OH solution inserted, and pumped into the canal. Next a drop of formalin was added and likewise pumped into the canal. Hot air was then applied to the canal. This was repeated from three to five times, during a period of about ten minutes. The teeth were then split open as in experiment 3, and under the same conditions as experiment 3 and cultures made from 8 internal areas of the tooth. These areas were as follows:
A. Dentin near apex.
B. Dentin 1 m.m. from apex.
C. Dentin 2 m.m. from apex.
D. Dentin 3 m.m. from apex.
E. Dentin from near crown end.
F. Dentin from opposite side near apex.
G. Dentin from gingival area opposite side.
H. Culture of root canal contents.
The control used on this experiment was taken from the first two sets of teeth in Experiment IV (See Exp. IV, Chart 6). In fact the whole experiment may be considered a control on experiment V.
Experiment IV. Chart 6
Determinations of the Ability of Medicaments to Sterilize Infected Dentin and Cementum When Sealed in the Root Canal and When the Perforated Apex is Surrounded by Infected Culture Media as Per Conditions in Chart V.
Results: Four trials were made on four different days. Trial No. 1 contained ten teeth or 80 cultures. These showed contamination in 25 cultures, making a total efficiency of 69%. Area H, canal contents, however, showed sterility in every case.
Trial No. 2 contained eleven teeth or 88 cultures. These showed contamination in twenty tubes, making a total efficiency of 78%. Area H showed sterility in every case except one.
No. 3 contained six teeth or 48 cultures. These showed contamination in eight tubes, making a total efficiency of 84%. Area H showed complete sterility.
Experiment V, Chart 7
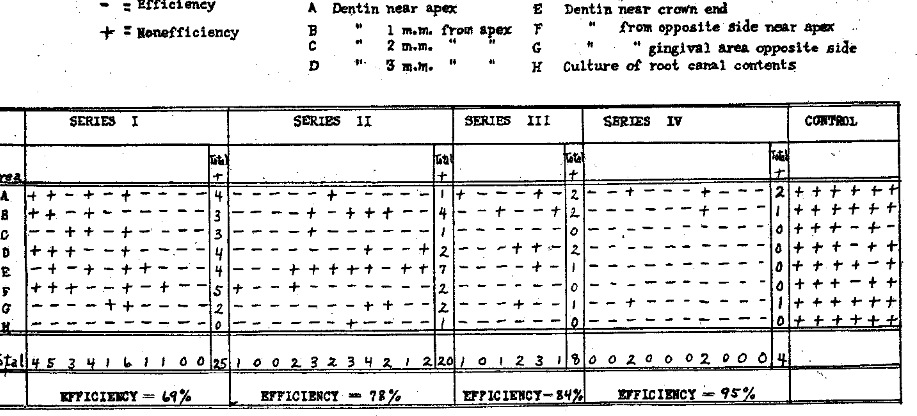
These three trials were deemed not sufficient evidence for the efficiency of this silver nitrate method. Another set of experiments, with technic slightly revised, was run. Under the exacting conditions used in No. 4, this series, the following results were obtained:
Ten teeth or 80 cultures were run. Two of these teeth showed contamination in four tubes each. However, these were probably contaminated, owing to a slip from the bur, as they were being ground. The efficiency was 95%.
Further determinations with various modifications of technic must be made of the silver method.
Conclusions: In comparing the results obtained from this method of treatment with the results from other methods obtained as in experiment 3, there is inclination to the belief that a perfected technic will produce sterilization of the tooth structures which are reached by the medicament in so short a period as ten minutes.
In comparing the four trials, the ascending percentages in efficiency leads to this conclusion. The sterility in the cultures obtained from the root canal proves the toxicity and bactericidal power of this treatment in the canal itself. The chemical action may be explained as follows:
The addition of the NH4OH to the AgNO3 forms a double silver salt as follows: AgNO3+NH4OH = AgOH+NH4NO3.
The further addition of the NH4OH gives the following formula: AgOHNH4OH = Ag(NH3)2 OH.
If formaldehyd is brought into this solution now, the silver is precipitated and deposited as free silver in the following: Ag(NH3)2 OH HCHO = free silver, formic acid and water. Chart 7 will give the details of this experiment.
The toxicity of both silver and of silver nitrate and formaldehyd has been proven on rabbits by making a subcutaneous inoculation.
The sterility obtained from the various cultures of the various areas of the tooth points, also, to sterility of the tubuli themselves. Inasmuch as a uniform treatment was used thruout all of these experiments, no difficulty seems to be encountered, perhaps thru the methods of infection.
Experiment VI.
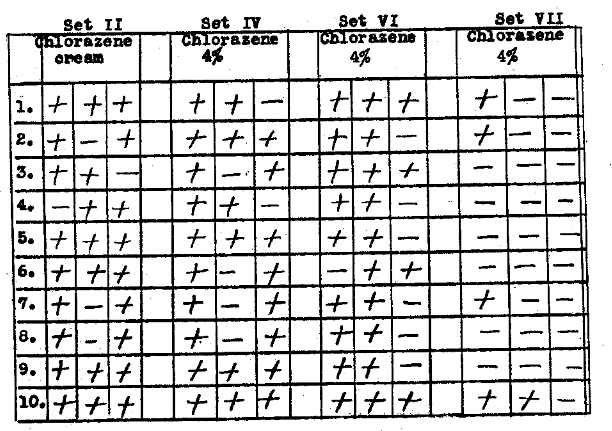
Determination of the Ability of Dakin’s Recent Chlorazene and Dichloramin-T Products to Sterilize Infected Dentin as Observed by Inserting Sterile Culture Medium.
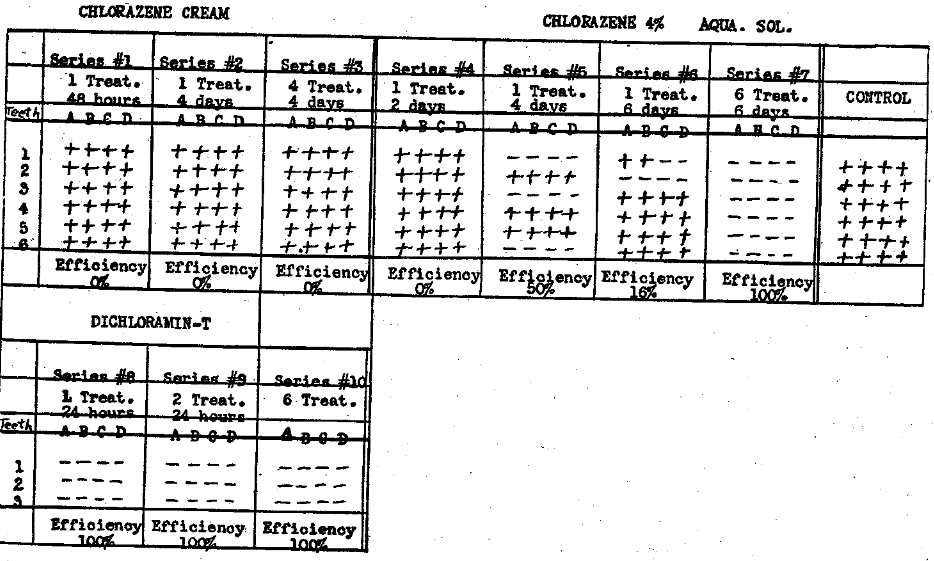
A separate experiment on Chlorazene and Dichloramin-T, consisting of a series of seven different methods for the production of disinfection, was performed. (Chlorazene is a sodium salt of toluene-parasulphochloramin. The systematic name for dichloramin-t is toluene-parasulphondichloramin. J.A.M., Vol. LXIX, No. 1)
Six teeth freshly extracted and cultured in a mixed salivary infection were used for each series of the chlorazene experiment and three teeth for each series of the Dichloramin-T experiment. The crowns had been cut off and the root canals opened thru the apex. Two kinds of Chlorazene preparations were used, chlorazene cream obtained directly from the Abbott Laboratories and a four per cent aqueous solution of chlorazene made in the Research Institute Laboratories, kept in a dark bottle in the ice chest thirteen days after preparation. The Dichloramin-T experiment is in the nature of a preliminary report, and because of the recent discovery of the drug there has not been time for a complete study, both of its properties and existing results in clinical practice. The Dichloramin-T consisted of a fifteen per cent solution in chlorinated eucalyptol, used on the same day that it was sent us from the Abbott Laboratories. Sterile wooden sticks, sterile capillary pipettes and occasionally a sterile smooth broach were used. All root canals were treated without the use of absorbent points. After treatment, sterile absorbent points were inserted for forty-eight hours, the teeth having been placed into sterile tubes containing moistened cotton and incubated. The ten sets consisted of seven series for chlorazene and three for dicliloramin-T.
Set I. One treatment of chlorazene cream was placed in the root canal and incubated for two days. This was then removed and an absorbent point saturated in dextrose broth, inserted. After two more days of incubation the cotton point was taken out, cut into four pieces, and cultured as in Experiments II and III.
Results: All cultures at end of twenty-four hours showed growth.
Set II. One four day treatment of chlorazene cream was given in the same procedure as in Set I.
Results: All cultures at end of twenty-four hours showed growth.
Set III. Four treatments of chlorazene cream on four successive days were given in the same manner as Experiment I.
Results: All cultures at end of twenty-four hours showed growth.
Set IV. One treatment of chlorazene four per cent, aqueous solution, for two days was given. The apical ends of one-half of the teeth were sealed with paraffin to contain the liquid in root canal and the other half unsealed and kept in a vertical position. Procedure same as in previous experiment.
Results: All cultures at end of twenty-four hours showed negative growth. There was no difference in the results with the sealed and the unsealed teeth.
Set V. One treatment of chlorazene four per cent, aqueous solution, was given over a period of four days in the same manner as in Set. IV.
Results: The test tubes showed fifty per cent growth and fifty per cent efficiency.
Set VI. One treatment of chlorazene four per cent, aqueous solution, for six days duration.
Results: The test tubes showed eighty-four per cent growth and sixteen per cent negative.
Set VII. Six treatments of chlorazene four per cent, aqueous solution, on six successive days.
Results: All the test tubes after four days’ incubation were negative.
Sets VIII, IX and X were made with Dichloramin-T 15% in Eucalyptol. Set VIII received one treatment for 24 hours. Set IX two treatments for 24 hours, and Set X six treatments for 24 hours.
Results are that three sets gave 100% efficiency. This drug, however, cannot be used in this strength as it is exceedingly painful and destructive. Further work must be done with it.
Conclusions:
- Chlorazene cream in all of the above tests gave no favorable results.
- Chlorazene cream was not efficient in a two days treatment, improved to fifty per cent in a four days treatment and again declined to sixteen per cent in a six days treatment, which shows the optimum power of, efficiency of one treatment.
- A number of six treatments of chlorazene four per cent, aqueous solution, on six successive days gave one hundred per cent efficiency.
Chart 8
It is not yet ascertained what the minimum number of treatments for efficiency is and how long the chlorazene remains sterile in the root canal.
Altho Chlorazene is advertised as being non-toxic, it was deemed advisable to test the authenticity of this statement. The toxicity and irritating effect on living tissue was tried by making a subcutaneous inoculation in a rabbit’s ear with a few drops of Chlorazene. Subsequent observation for several weeks showed no injury of suppuration of any description.
Three teeth from each of Sets II, IV, VI and VII were used for making cultures for the various structures as in Experiment IV.
Set VII shows a high percentage of negative cultures and we refrain from overemphasizing the results on account of not obtaining 100% efficiency. More cautious experiments will show the value of this result. The remaining sets coincide with their respective cultural results as stated before.
Experiment VI, Chart VIII
Controls.
The following checks on procedure were made:
- All media incubated 72 hours minimum after sterilization in the autoclave.
- Scissors after flaming gave negative results on four successive trials.
- Forceps cultured after flaming gave negative results on four successive trials.
- An interesting experiment was made to prove the sterility of the J. & J. absorbent points. A new box of these points were opened under sterile precautions, the cotton carefully removed with sterile forceps and the points picked out with flamed forceps and dropped into sterile dextrose broth and placed in the incubator for 24 hours. Five trials were made and each showed a luxuriant growth after incubation. We have been led to conclude that these guaranteed sterilized points should be sterilized by the operator, before subjected to such use as would require the presence of strictly sterilized material.
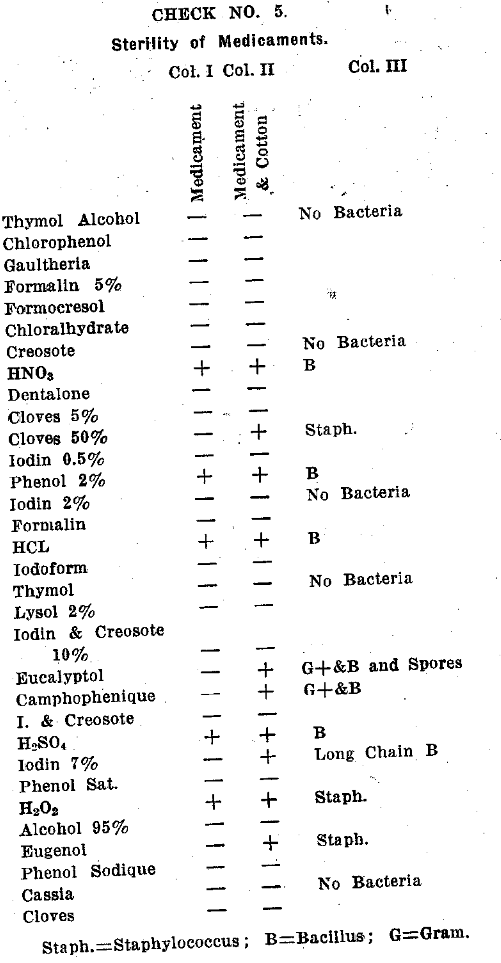
Where the medicament in use is a disinfectant, the sterility of the points would be accomplished by this agent, but where the medicament is not of such an efficiency, contamination from the absorbent points might result. - Sterility of Medicaments.
An interesting check on the sterility of medicaments per se was made by culturing the medicament alone, and by culturing the absorbent cotton dipped into the medicament.
A few drops of the medicament were removed with a sterile pipette which had previously been flamed, and placed in sterile culture broth. The results were negative in every case except nitric acid, sulphuric acid, hydrochloric acid, all fifty per cent, phenol two per cent, and hydrogen peroxide. These showed absolute lack of efficiency. Column I gives the results as indicated above.
Absorbent points placed in each of the above medicaments and cultured gave the following results as indicated in column II. The fact that Cloves, 50%, Eucalyptol, Campho-phenique, lodin 7%, Eugenol, were sterile per se, but when the cotton absorbent points were placed in the medicament, a positive growth ensued, shows lack of efficiency in the production of antisepsis, when a contaminated cotton point was placed in the medicament. Smears were made of medicaments showing growth and results indicated on column III.
According to these data, the above medicaments could have been omitted from the experiments on the evidence of their own lack of efficiency, while the negative production illustrated an important check on the remaining medicaments. These organisms, however, may not be disease producing. - All experiments were controlled in order to prove that the cultures were not killed by any other means, as for example, thru their own toxic products. For this reason a culture was made of teeth taken from the same infected media and placed into sterile dextrose broth for the same length of time as the experiment lasted. These cultures all grew out and smears showed the existence of bacteria.
The root canal dressing points used in the previous experiments were autoclaved.
Controls, Check No. 5.
General Summary and Conclusions.
- Infected dentin and cementum are not readily sterilized by medication, even when the amount of medicament is largely in excess of the mass of tooth structure.
- The medicament contained in a medicated root dressing very readily and rapidly loses its disinfecting power, for the dressing itself becomes infected in a few hours, even from the infected dentin and without being in contact with an infected solution.
- The medicament in the dressing dissipates more rapidly when one end of the dressing is in contact with an infected culture medium, such condition as obtains in a periapical infection.
- The efficiency of a root treatment is greater a few hours after it has been placed in the tooth than after several days, or even one day’s time.
- All areas of cementum and dentin are difficult to sterilize, as well as tend to reinfection, when the medicated root dressing is left more than a few hours.
- The medicaments that are most efficient, namely, silver nitrate and formalin, are very objectionable, the former by its discoloration and the latter by its destructing and irritating properties, except when used very dilute and for a short time and then quite efficiently.
- There is much encouragement in the use of Chlorazene and Dichloramin-T products. They are, however, exceedingly painful and destructive in over half of one per cent strength.
- We now understand why it has been that if a root treatment is left in the tooth for an extended period of time it becomes foul in odor. Also a verification of the observation previously reported by one of us, Price, to the effect that medicated root dressings will always show bacterial growth after they have been left in infected teeth for a few days.
- These determinations indicate to us that an exceedingly small per cent of the teeth that have been treated by members of the dental profession in the past have actually been sterilized.
- Nature is, and has always been, very tolerant, and much of the credit that has been taken by, and given to, the dental profession for the sterilization of infected roots has really been due to nature for her kindness in tolerating, at least without local irritation, a probably almost universal and permanent condition of infection, tho in lessened amount, when tooth structures have once been infected and have been subjected to treatment.
References Cited:
- Sewell, Henry. Items of Interest, 1885, page 1.
- Ingersoll, D. C. Dental Science.
- Garretson, J. E. A System of Oral Surgery, 1895, page 223.
- Williams, Leon. London Cosmos, 1892-1896.
- a. Kirk, E. C. The American Text Book of Operative Dentistry.
b. “Putrefaction.” - Grieves, C. J. “The Relation of the Vitality of the Periapical Cementum and the Adjacent Tissues.”
- a. Buckley, John. Dental Review, August, 1911, A. M. A. Journal, Vol. 63, No. 23.
b. Modern Dental Materia Medica, Pharmacology and Therapeutics.
c. Items of Interest, April 1910. - Rhein, M. L. Items of Interest, August 1909.
- Barrett. Oral Pathology & Practice.
- Gorgas, F. I. S. Dental Medicine.
- Truman, Jas. “Cataphoresis,” Cosmos, 1896, No. 38, page 758.
- Abbott. Dental Pathology and Practice.
- Ottolengui, R. Items of Interest, Sept. 1914.
- Thoma, K. H. “Oral Abscesses,” page 182.
- Herff, Otto von, “Principles of Combating Local Inflammations in the Mouth,” Muencheneor Medizin, Wochenschr, April 27, 1915, Cosmos 1915, page 1404.
- Brophy, Truman W. “Carbolic Acid and Creosote; Their Chemistry and Therapeutic Application to the Practice of Dentistry.” 1880.
- LeRoy, L. C. “Treatment of Pulpless Canals.” Items of Interest, Vol. 19, 1897.
- Burchard. Dental Pathology, Therapeutics and Pharmacology.
- Bodecker, F. W. “Iodoform in Dental Surgery.” Reprint from the Independent Practitioner of March & April, 1884, page 6.
- Rhein, M. L. “Cure of Acute and Chronic Alveolar Abscess.” Dental Items of Interest, Vol. 19, 1897, page 688.
- McCurdy, S. C. Oral Surgery, page 76.
- Frahm, Frederick W. “The Value of Formaldehyd in Septic Root Canals.” Pacific Dental Gazette, February, 1914.
- Black, G. V. Special Dental Pathology. Page 291-299.
- Dunning, Wm. B. “New Standards in Root Canal Fillings.” Dental Cosmos, Vol. 58, No. 6.
- Callahan, J. R. “Rosin Solution for Sealing of the Dental Tubuli,” Reprint from Journal of the Allied Dental Societies, March 1914.
- Marshall, John A. “The Neutralizing Power of Saliva in Its Relation to Dental Caries.“ American Journal Physiology, Vol. 36, No. 3, February 1915.
- Gies, William J. “Chemical Studies of the Relations of Oral Microorganisms to Dental Caries.“ Journal Allied Dental Soc’s, 1915, pp 137-140.
- Bunting and Rickert. Dental Caries.
- Daufresne, Maurice. “Cicatrization of Wounds. VII. The Use of Chloramine-t paste for the sterilization of wounds.“ Journal Experimental Medicine, Vol. 26, No. 1.
- Boyd, Bert. “The Present Status of the Root Canal Problem.“ Pacific Dental Gazette, Vol. 25, No. 1.
- Callahan, J. R. “Root Canals.“ Transactions of the National Dental Association, 1909, p. 158.
- Brownell. Practical Dentistry by Practical Dentists.
- Best, E. S. “The Responsibility of the Dentist In the Care of Pulpless Teeth.“ Items of Interest, 1914. Page 498.
- a. Miller, W. D. “Asepsis and Antisepsis in Practice.“ Dental Cosmos, 1893, page 1.
b. “Disinfection of Dental and Surgical Instruments.“ Dental Cosmos, 1891, page 514. - Hasseltine, H. E. “Sterilization of Dental Instruments.“ Dental Summary, 1916.
- Kells, C. E. “The Rationale of Immediate Root Canal Filling.“ Items of Interest, 1914, page 481.
- Jordan. General Bacteriology.
- Dorlan. Medical Dictionary.
- La Odontologia, Madrid, Spain, September 1913. “Antiseptic Solutions for use in the Mouth.“
- Polet, M. “The Iodin Treatment of Root Canals.“ Le Laboratoire, Paris, September 1913.
- Albrecht. “Resorcin-Formalin in Root Canal Treatment.“ Deutsche Monatsschrift für Zahnheilkunde, Berlin, 1913.
- Hinman, Thomas P. “Therapeutic Treatment of Pulp Diseases.“ The Journal of the National Dental Association, Vol. 4, No. 1.
- Prinz, Herman. Dental Materia Medica and Therapeutics.
- Brooks. American Journal of Dental Sciences, Vol, III.
- Taft. Operative Dentistry, 1859. Page 214.
- Harlan. Dental Cosmos, 1898, page 287.
- Truman. Dental Cosmos, 1895, page 1.
- Szabo. Osterrechish–Ungarische Vierteljahrsschrift für Zahnheilkunde, 1902.
- Stebbins. International Dental Journ. 1891, No. 10.
- Shanasy. Dental Cosmos, 1898, page 876.
- Niles. La Odontología, 1900, No. 8.
- Bryan. Dental Review, 1903, No. 7.
- Bethel. Ohio Dental Journal, 1896, No. 9.
- Preiswerck. Atlas and Text Book of Dentistry, 1906, page 219.
- Miller. Dental Cosmos, 1905, page 193.
- Black. Operative Dentistry, 1908, Vol. I.
- Whitslar, W. H. “AGNO3 and Cataphoresis.“ Items of Interest, Vol. 19, 1897.
- Hartzell, Thomas B. “The Post-Operative Treatment of Pyorrhea.“ Trans. National Dental Assoc’n, 1912, page 261.
- a. Howe, P. R. Preliminary Report before the Pennsylvania State Society at Philadelphia, June, 1917.
b. Research Reports of the National Dental Association, October, 1917. - a. Dakin, H. D., Cohen, Daufresne and Kenyon. Proc. Royal Soc. Biol Science, Series B., Vol. 89, No. 13614, page 234. “Antiseptic Action of Substances of the Chloramine Group.“
b. Carrel and Hartmann. “Cicatrization of Wounds, VIII. Sterilization of Wounds with Chloramine-T.“ Journal Experimental Medicine, Vol. 26, No. 1.
c. Vincent, A. “Cicatrization of Wounds. Bacteriological Asepsis of a Wound.“ Jour. Experimental Medicine, Vol. 26, No. 1. - Dakin, H. D. “A Report of the Use of Dichloramin-T (Toluene-Parasulphondichioramin) in Treatment of Infected Wounds.“ Jour. American Medical Association, Vol. LXIX, No, 1, page 27.
- Dahlgren, B. E. “Study of Efficiency of Disinfectants and of Ionization in Root Canals of Infected Teeth.“ The Journal of the National Dental Association, Vol. IV, No. 3.
- Boennecken, H. “Untersuchungen über einige neueren bei der Wurzelbehandlung verwandte Antiseptika.“ Österr. Zeitschr. f. Stomal., 1913, Vol. 3, No. 51.
- Blessing, G. “Untersuchungen uber den antibacteriellen Wert einige bie der Therapie der Pulpagangrän gebräuchlichen Mittel.“ Deutsche Monats. f. Zahnheilk, 1914, page 763.
- Barnes, Henry. “Treatment of Root Canals.“ AgNO3 cataphoresis.“ Items of Interest, Vol. 19, 1897, page 915.
- Bodecker. Anatomy and Pathology of the Teeth.
- Burchard and Inglis. Dental Pathology and Therapeutics.
- Catching, B. H. Compendium of Practical Dentistry, 1896.
- Dahlgren, B. E. “The Root Canal Problem, Asepsis and Sterilization.“ The Journal of the National Dental Association, Vol. IV, No. 1.
- Evans. Cosmos, 1893.
- Harlan, A. W. “Review of the Question of the Treatment of Putrescence as Related to Pulps and Pulpless Teeth.“ Transactions of the N. D. A., 1904-1905.
- Lambert, Robert. “The Comparative Resistance of Bacteria and Human Tissue Cells to Certain Common Antiseptics.“ Journ. Exp. Med., 1916, Vol. XXIV, No. 6, page 683.
- MaWhinney. Oral Pathology.
- Miller. Microorganisms of the Human Mouth.
- Mitchell. Dental Chemistry.
- Moffitt. “The Treatment of and Filling of Root Canals.“ Transactions of the National Dental Association, 1912.
- Nieholl. “Toxicity of Ions.“ Journal Biol. Chem. 1909 (5) page 453.
- Pickerill. Stomatology in General Practice.
- Reclus. “The Antiseptic Properties of Tincture of Iodin.” La Odontología, Argentina, Buenos Aires, June, 1913.