
Access to all articles, new health classes, discounts in our store, and more!
The Intradermal Ascorbic Acid Test, Part II. A Review of Human Studies
Published in Journal of Dental Medicine, Vol. 13, No. 1, pp. 19-40, January 1958.
* * *
Introduction
In an earlier report,1 an attempt was made to review the literature on the use of the intradermal ascorbic acid test as revealed in animal studies. This paper will concern itself with an analysis of the literature dealing with human subjects.
Human Studies
Rotter,2,3 having already established in his animal studies that the 2,6 dichlorophenolindophenol (DCPIP) decolorization was a chemical reduction phenomenon, decided to verify this by injecting the dye into detached portions of human mucosa (perineal and vaginal). He found that the DCPIP reagent disappeared in a time comparable to that in the living organism. The next study which he undertook was that of determining the connection between the velocity of reduction and body ascorbic acid. He placed six persons on a scorbutic regime for ten days. The urine level of ascorbic acid and the dye disappearance time were performed daily. The dye was injected into an area of the forearm free from hairs and veins. He observed that the urine level of vitamin C gradually declined while the intradermal time increased slowly. After ten days, oral and intravenous ascorbic acid was given to these subjects. The urinary ascorbic acid level increased and tended to become constant while the decolorization time decreased. He felt that the most astonishing finding was an 80 to 90 percent reduction in intradermal time two minutes after an intravenous injection of 600 mgm. of ascorbic acid. These findings, he believed, established the fact that the cutaneous reaction was the direct result of the ascorbic acid in the body. He recommended a N/400 concentration and 2 mm. wheal of DCPIP as a result of his experience with different concentrations and wheal sizes. Using this technique, he maintained that a disappearance time of 5 minutes or less spoke for saturation; 5 to 10 minutes should be considered normal; over 10 minutes indicated hypovitaminosis C. Rotter submitted that this procedure was better suited than urine or blood determinations for large population studies.
Portnoy and Wilkinson
Portnoy and Wilkinson,4 in an experiment on 103 patients, employed Rotter’s method of dye injection into the forearm. They used a N/400 concentration, injected .01 cc. to raise a 2 mm. wheal. To minimize technical errors, four wheals were raised in every instance and the average decolorization time established. From the entire group of 103 subjects, 35 were selected and then these were divided into two categories (21 unsaturated and 14 partially saturated) on the basis of plasma concentration. The unsaturated group (plasma levels of .27 to .52 mgm. percent) showed decolorization times of 3 to 29 minutes (mean 16.9). The partially saturated individuals (plasma levels of .72 to 1.3 mgm. percent) had times of 3 to 13 minutes (mean 7.5). Seventeen patients, taken from the unsaturated category, were then saturated (final plasma levels of 1.32 to 2 mgm. percent). The time range diminished to 0.5 to 6 minutes (mean 2.3). In every instance there was a decrease in intradermal time after saturation. On the basis of a dietetic history, the remaining 68 subjects were categorized as saturated (18 persons), normal (37 persons), and unsaturated (13 persons). The mean intradermal times for these three categories were found to be 3.4, 8.8, and 16.1 minutes, respectively. This, it should be recalled, was consistent with the observations made on the original 35 subjects. The authors recognized the fact that there are individual variations. However, they concluded that the intradermal decolorization time is a useful and rapid indicator of the ascorbic acid status of the tissues. Consistent with Rotter’s standard, these authors contended that an intradermal time of 5 minutes or less is indicative of tissue saturation; times over 10 minutes speak for deficiency.
Portnoy and Wilkinson,5 in an enlarged. study of 107 patients, investigated six different methods of vitamin C determination. These subjects were divided into the following groups: (1) two control categories of 51 patients, (2) one group with peptic ulcer (25 patients), and (3) peptic ulcer patients with hematemesis (31 subjects). It became clear that all measures of ascorbic acid status correlated with each other in an overall appraisal. In other words, those individuals with a presumably normal ascorbic acid body level showed higher plasma and urine levels and shorter intradermal decolorization times. Their evaluation of the intradermal time has already been considered.4 The results of this phase of their study may be summarized in six statements. First, the daily excretion of ascorbic acid proved to be greatest in the two control groups. Specifically, in staff personnel the average vitamin excretion amounted to 29 mgm. per 24 hours; in the other control group consisting of random ward patients, the mean daily urinary excretion was 17 mgm. In contrast, only 7 mgm. per day was excreted by the ulcer patients. Secondly, these investigators determined the saturation of their patients on the basis of a urine saturation test. According to the test, when the daily urinary excretion level reached 50 percent of an oral dose of 500 to 1000 mgm. of ascorbic acid, the subject was regarded as being saturated. On the basis of such a standard, Portnoy and Wilkinson found that the control groups required less supplementation with ascorbic acid to reach the 50 percent “spill-over” period than the experimental groups. Actually, this end point in the control groups was reached after a total of 500 to 2300 mgm. of the vitamin were administered. In contrast, 2100 to 8000 mgm. were required before one could demonstrate the 50 percent excretion in the experimental group. Thirdly, it was observed that the fasting plasma ascorbic acid levels in the control groups ranged from .60 to 1.85 mgm. percent whereas the peptic ulcer categories varied from .14 to .59 mgm. percent. Fourthly, observations were made using a 1000 mgm. intravenous load dose. It was noted that a maximal plasma level was reached 15 to 20 minutes after the intravenous dose. The 24-hour urinary vitamin excretion after a 1000 mgm. intravenous injection totalled 660 to 985 mgm. in the normal groups and 72 to 458 mgm. in the experimental subjects. Parenthetically, the statement can be made that about 80 percent of the total urinary excretion occurred in the first five post-injection hours. Fifthly, following a single oral dose of 1000 mgm. of ascorbic acid to a normal subject, the plasma level returned to its original value in 5 to 6 hours. In contradistinction, the return among the experimental subjects was found to occur in less time. Sixthly, Portnoy and Wilkinson observed that the decolorization time agreed quite well with the other laboratory tests though they preferred to regard the skin test time as only a rough estimate of saturation. The authors concluded with the statement that the evidence suggests that ulcer patients suffer with a severe ascorbic acid deficiency probably due in part to the ulcer diet which is customarily quite low in its ascorbic acid content.
Poncher and Stubenrauch
Poncher and Stubenrauch6 performed intradermal times and plasma levels on 41 persons. Rotter’s technique was employed. The subjects were arranged into three categories according to the plasma level of ascorbic acid. Group 1 (6 persons) varied in plasma concentration from .15 to .45 mgm. percent and were regarded as the scorbutic group. Group 2 (9 persons) showed a range from .5 to .7 and were considered subnormal. The normal group (26 persons) varied from .8 to 1.8 mgm. percent. No correlation was found between the dye decolorization time and ascorbic acid tissue saturation as evidenced by the plasma level. In the scorbutic group, the decolorization times were 4 to 8 minutes (average 5.8), in the suboptimal group 6.8 to 12 minutes (mean 9.4), and in the normal group 3.5 to 13.1 minutes (average 7.6). The authors stressed the fallacy of drawing conclusions from one test on one individual. Although they found no value with the procedure, Poncher and Stubenrauch reported that the decolorization times were constant for each individual.
Jetter
Jetter7 found no correlation between the fasting ascorbic acid level of whole blood and the intradermal time in 50 female tuberculous patients. It is of interest that Jetter differed from his predecessors in that he used a N/500 DCPIP solution, .01 cc., and a 2 to 3 mm. wheal. Three wheals were raised on the forearm at the time the blood was drawn and the average of the three was reported. The intradermal times ranged from 2 to 10 minutes. The plasma values varied from .40 to 1.39 mgm. percent. Assuming 1.1 mgm. percent whole blood ascorbic acid as the minimal normal level, he divided his subjects into two groups: (1) 43 hypovitaminotic, and (2) 7 normal patients. The deficient patients evidenced skin times from 2 to 9 minutes (average 4.7) and the normal group decolorized the dye in 2 to 10 minutes (average 6.3). This investigator felt that vitamin C plays little or no role in the tissue decolorization of DCPIP.
Codvelle et al.
Codvelle et al.,8 injecting intradermally .016 cc. of a N/200 (80 mgm. dye in 100 grams of diluent) DCPIP solution into the forearm of human subjects, found decolorization times between 5 and 22 minutes in 9 persons of the same age (20-23 years) and diet. In a second group of 5 normal patients given 100 mgm. of ascorbic acid daily for 15 days, the final disappearance times lay between 8 and 10 minutes. No initial times were given. A third group of 5 patients, who had received 500 mgm. of ascorbic acid for 6 days, ranged in time from 3 to 5 minutes. Again no initial values were given. Even though their method represented an extensive modification of Rotter’s original technique, they designated the three groups as deficient, normal, and saturated respectively on the basis of Rotter’s times. The authors then took groups comparable in age and with identical diets and performed urinary excretion tests of saturation at various levels of daily ascorbic acid intake. In the cases receiving a 100 mgm. supplement (9 persons) and in other groups receiving 150 or 200 mgm. (? persons), there was no abrupt increase in urinary excretion over a period of 30 days. A sudden increase of urinary excretion of the vitamin was held to indicate body saturation. Five persons receiving daily dosages of 250 mgm. showed a rapid rise in urinary excretion in from 4 to 7 days. Six subjects receiving 500 mgm. displayed the first massive excretion in 3 to 5 days. Assuming that this sudden rise of urinary ascorbic acid excretion denotes saturation, the group-nutrition of vitamin C would seem to be well related to the group-intradermal test time. Both the intradermal times and the urinary excretion would appear to speak for unsaturation in the non-supplemented and the 100 mgm. supplemented groups, whereas the 500 mgm. groups would appear to be saturated from either aspect. The authors were primarily interested in establishing an optimal daily ascorbic acid intake. They felt, on the basis of these and other findings, that 100 mgm. per day is needed.
Gambigliani-Zoccoli and Lombardo
Gambigliani-Zoccoli and Lombardo9 utilized the technique of Rotter in evaluating the intradermal test. The recorded decolorization time was an average of four wheals produced simultaneously on the forearm. In an unspecified number of healthy human subjects, 500 mgm. of ascorbic acid were introduced intravenously. The investigators observed that the time range, before the injection of the vitamin, was 4 to 13 minutes. One hour later, the disappearance time decreased to as little as 2 to 3 minutes. The times returned to the normal range after 15-24 hours except in a few cases which required 48 hours to regain the original score.
Oliveira Lima
Oliveira Lima10 employed Rotter’s technique in estimating the value of the decolorization test. Twenty-four children (age 3-12 years) were separated into two groups (12 in each category), saturated and unsaturated. The saturated subjects excreted in the urine 40 percent of a 300 mgm. intravenous dose of vitamin C in three hours. The unsaturated group eliminated only 10 percent of the same dose in the same time. Prior to vitamin C injection the times ranged from 4 to 13 minutes (average 8) in the unsaturated group and from 6 to 11 minutes (average 9.7) in the saturated category. A scatter diagram revealed no relationship between the intradermal time and the urinary excretion pattern. The decolorization times were plotted against both absolute elimination values and percentage (of test dose) excretion within three hours. Oliveira Lima asserted that the test had no value. He suggested that the other reducing agents in the skin supervene and render the test, as offered, valueless.
Poulsen and Lieck
Poulsen and Lieck11 determined skin test times and ascorbic acid levels in 70 subjects. They used a N/300 (approximate) solution of DCPIP and a .01 cc. injection. They found times of 6 and 13 minutes in the same person when two wheals were raised simultaneously. This prompted them to standardize the injection at .01 cc. with a syringe modified to accomplish such exactitude. Then a double determination was done in 64 cases. None of the subjects showed differences in score greater than 2 minutes. The 70 experimental subjects, on whom plasma ascorbic acid levels and skin test times were performed, varied from 6 to 20 minutes in intradermal time and from 0 to .8 mgm. percent plasma level. The skin times were performed with the patients lying down and arms alongside the body. It was observed from a scatter diagram that decolorization times were not associated with plasma levels. For example, a decolorization time of 9 minutes corresponded to a plasma range of .08 to .8 mgm. percent. In another study, four subjects were supplemented with ascorbic acid for 11 to 42 days. The plasma ascorbic acid level rose from 0-.12 to .1-.8 mgm. percent. The skin times decreased from 8.5-15 to 8-12.5 minutes. The authors neglected to state how much ascorbic acid was administered, although they indicated that it was given orally. A load dose determination was done in one case. The fasting scores were .8 mgm. percent and 9 minutes. Two and three hours after the oral administration of 600 mgm. of vitamin C, the plasma levels were 1.15 and 1.6 mgm. percent respectively. On the other hand, the intradermal time decreased only slightly in 2½ hours–from 9 to 7 minutes. It is well to note that this patient had been taking supplementary vitamin C for 26 days before the load test. The authors pointed out that they failed to corroborate the finding of Rotter of an 80-90 percent reduction in time after a tolerance dose of ascorbic acid. To illustrate further the many variables which modify the skin test, Poulsen and Lieck injected both arms of one subject simultaneously and then had the patient raise one arm and lower the other. The higher arm decolorized the dye in 24 minutes; the other accomplished a decolorization in 16.5 minutes. Another patient was similarly injected and both arms were kept at the same level. However, one was immersed in a water bath at 40° C. The intradermal time in the immersed limb was 14 minutes; the non-immersed arm, 18 minutes. An intradermal dye injection in the patellar skin of this same patient decolorized in 19 minutes. The authors concluded, from these observations, that the skin test time has no clinical value.
Wright and MacLenathen
Wright and MacLenathen12 studied the intradermal time from two aspects: (1) the correlation of diet and blood level, and (2) relationship of site of injection to disappearance time. Of 11 patients with adequate diets and normal blood levels, only three had decolorization times of 10 minutes or less. According to Rotter,2,3 individuals with adequate blood levels should have shown disappearance times between 5 and 10 minutes. Of 11 patients with poor dietary habits and subnormal blood levels, 4 showed intradermal times less than 10 minutes. Of the latter group of 11, the remaining 7 subjects displayed disappearance times ranging from 11 to 33 minutes. The authors did not state which blood level was considered normal nor did they list the observed plasma levels. It should be emphasized that the research of these men is at variance with Rotter2,3 even though the same dye, in the same concentration, was used. Wright and MacLenathen also compared decolorization times at different sites of injection. In some of the subjects utilized in the preceding experiment and in a group of individuals with vascular disease there was a difference in the test times when two wheals were simultaneously raised within a few centimeters of each other. For example, in one instance the disagreement between the decolorization times of concurrent dye injections amounted to ten minutes. Parenthetically, the authors pointed out that intense pain occurs at the site of injection and that there remains a hard, erythematous nodule for 4 to 5 weeks.
Banerjee and Guha
Banerjee and Guha13 studied 9 human beings using Rotter’s original technique. Each subject was given an oral dose of 700 mgm. ascorbic acid. Intradermal times and 24-hour urine ascorbic acid excretion values were performed before and after administration of the load dose. Eight of the 9 subjects showed a decrease in test time and all displayed increased urinary excretion. In these 8 cases, an average reduction of 35 percent of the original skin time resulted. It is interesting to note from their chart that the longer original times showed the greatest average percentage reduction.
Suzuki
Suzuki,14 using Rotter’s method of intradermal injection2,3 compared blood serum values with the decolorization times. He employed eight groups of a mixture of healthy persons and individuals afflicted with skin diseases. He did not, however, reveal the number of persons in each group. The groups were divided into increasing levels of vitamin C in the blood serum. He found a direct relationship between the two scores–the intradermal times became lower just as the serum level increased. He noted in seven cases of lichenifying and pigmenting skin diseases that the dye disappeared in a shorter time when it was injected into an area of the skin involved by the disease. Times were longer when the dye was injected into an uninvolved skin site. In eight patients with urticarial wheals he injected the dye into unaffected areas, into the halo area between the wheal and the surrounding skin, and directly into the wheal itself. Proceeding from the normal to the involved area in this manner, a progressive decrease in test time occurred. He felt that these observations could be explained on the basis of a local increase in “reducing substance” due to acute or chronic inflammation.
Goldsmith, Gowe and Ogaard
Goldsmith, Gowe and Ogaard15 made 100 observations on 45 persons. These individuals were classed into three groups: (1) unsaturated, (2) saturated, and (3) normal. The classification was based on the level of ascorbic acid in the plasma. Using .01 cc. of a N/400 solution of DCPIP, they claimed no correlation between the plasma ascorbic acid level and the intradermal time. They, therefore, concluded that the intradermal test cannot replace blood determinations as a measure of vitamin C status. They found that factors other than the ascorbic acid level could modify the decolorization time. This observation was derived from studies in which they instituted changes in circulation and room temperature. The authors further felt that other reducing agents might interfere with the disappearance time of DCPIP. An analysis of data from 9 persons who had received more than 5 injections was made. Once again, the authors found no correlation between the test time and plasma level. For example, in one subject given 25 intradermal injections, within 75 minutes, there was a time range from 4.5 to 11.6 minutes. On the other hand, they observed that the intravenous administration of 1000 mgm. of ascorbic acid caused a plasma level rise from .15-1.4 to 6-8 mgm. percent. During this same interval the intradermal time was halved. They failed to indicate the number of cases analyzed and the time interval between injection of the load dose and the final measurements.
Slavich and Torrini
Slavich and Torrini16 performed Rotter’s test on 50 individuals. They employed 36 human beings in a loading study. The group contained normal and sick persons. The intradermal time of each person was taken, and then varying amounts of ascorbic acid (200-250-500 mgm.) were given intravenously. Fifteen to 20 minutes later, the skin test time was repeated. The subjects fell into three groups on the basis of original times: (1) 14 revealed skin times below 10 minutes (range 3.5-10 minutes), (2) 9 had times between 10 and 14 minutes (range 11-13 minutes), and (3) 13 exhibited decolorization times above 14 minutes (range 14-35 minutes). In group 1, 4 persons were apparently in normal health and 10 were diseased. Group 2 was composed of 4 normal and 5 sick patients; in group 3 all were ill. It is interesting to note that the decolorization times found after ascorbic acid administration were lower in every case than the preinjection scores. And further, the average percentage reduction in time was greatest in the groups which originally showed the longest disappearance times. Specifically, group 1 revealed an average reduction in skin test time of 42 percent, group 2 an average of 46 percent, and group 3 (with the longest original times) presented an average of 50 percent reduction. The authors felt that the other reducing agents present in the skin did not lessen the clinical value of the intradermal test. They believed that the time obtained reflects body saturation since the integument acts as a storehouse for the vitamin. The other reducing agents (as glutathione and cysteine) seem to remain constant within any individual even though the ascorbic acid may fluctuate. Slavich and Torrini, however, did agree that each individual should be viewed singly. These authors implied that load testing with calculation of percentage reduction of time may be an indication of body ascorbic acid status.
Baraldi
Baraldi17 employed Rotter’s method in performing the intradermal test on 84 mentally-ill patients, ranging from 15 to 85 years of age. He obtained times between 5 and 8 minutes in 80 of the 84 patients. Two subjects revealed times below 3 minutes and two above 13 minutes. The author noted that these times were well within the physiologic limits set by Rotter, except for the two cases above 13 minutes. According to the author, the skin test time did not distinguish between the new admissions to the institution (22 persons) and those who had been there some time. The new admissions were alcoholics and other malnourished persons. The old patients had, Baraldi submitted, enjoyed a nourishing diet. For this reason, the investigator contested the specificity of the intradermal test.
Beck and Krieger
Beck and Krieger18 utilized Rotter’s method in evaluating the skin time in human beings. In preliminary studies they found that variations in both blood supply to the tissue and in light intensity had no appreciable effect on the disappearance time. They performed the decolorization time before and after cutting off blood circulation in the arm (pressure cuff), before and after intensive rubbing of the skin and before and after cardiazol injection (which decreases peripheral blood circulation). Under these circumstances the time-scores differed in value by only 1 to 2 minutes. Upon injecting the dye different depths into the skin on the same person simultaneously, they observed differences in time of over 50 percent. This led them to fabricate an apparatus whereby a constant depth of puncture could be achieved. The intradermal time was then determined in 62 presumably healthy persons. They ranged from 5 to 16 minutes with an average value of 10 minutes. Three persons who were experimentally saturated with vitamin C (urine level verification) showed diminished times (4 to 5 minutes). In 16 subjects from the first study a load-dose experiment was done. The subjects were given 300 mgm. of ascorbic acid per day, per os, until the urine concentration of the vitamin reached a particular level. They indicated that this level in the urine was normally attained after 5 days–i.e., after a total dose of 1500 mgm. The amount of ascorbic acid required to reach the desired urine concentration was then compared with the initial disappearance time. There was a close relationship–persons with longer original times required greater amounts before urine saturation was attained. It is interesting to note from their graph that the usual amount of vitamin C necessary to saturate the tissues (1500 mgm.) is related to an initial disappearance time of 12 minutes. In a larger study of 92 patients, Beck and Krieger distinguished two groups: (a) 52 persons who had illnesses known to be unaccompanied by ascorbic acid deficiency, and (b) 40 subjects who had diseases characterized by ascorbic acid deficiency. The average disappearance time was found to be 10.5 and 18.5 minutes respectively. The tendency for group b to exhibit prolonged times was clear. In addition the authors performed skin times on 8 mothers and their newborns soon after delivery. The greatest difference in time between mother and child was 3 minutes. Beck and Krieger felt the Rotter test was valuable as a rough clinical estimate of tissue ascorbic acid.
Rapaport and Miller
Rapaport and Miller19 performed plasma ascorbic acid levels and intradermal times on 100 children selected at random from the hospital wards. Using a N/400 solution of DCPIP, they raised 1 mm. wheals on the extensor surface of the thigh about 6 inches above the knee. These children were arranged into three groups according to their plasma ascorbic acid levels: (1) low-level below .5 mgm. percent (26 children), (2) subnormal-leve l.5 to .7 mgm. percent (21 children), and (3) normal-level above .7 mgm. percent (53 children). Group 1 (low) varied in intradermal time from 2.5 to 30 minutes (average 6.8 minutes). Group 2 (subnormal) showed an intradermal time range from 2 to 20 minutes (average 5.5 minutes). Group 3 (normal) varied from 2 to 20 minutes (average 5.4 minutes). Only in the normal range did they observe that the intradermal time allowed a fair estimation of the plasma level. In the other two groups, no predictive correlation was possible. For this reason, Rapaport and Miller deemed the disappearance test valueless for clinical purposes.
Bakhsh et al.
Bakhsh et al.,20 using Rotter’s technique, performed plasma ascorbic acid levels and intradermal disappearance times in students. One hundred and forty determinations were done. Twenty cases (14.3 percent) fell below .8 mgm. percent in plasma value; 81 cases (57 percent) lay between .8 and 1.5 mgm. percent; 39 cases (27.9 percent) yielded plasma levels in excess of 1.5 mgm. percent. The times varied from 1 to 25 minutes and the plasma values from .3 to 2.0 mgm. percent. The mean standard deviations for the students were: Plasma level 1.19 ± .3 mgm. percent; skin time 8.2 ± 4.2 minutes. The authors established statistically that the two values were not independent of each other. However, they were distributed over such a wide area as to preclude any mutual predictivity. For example, a blood level of .8 mgm. percent corresponded to times from 7 to 19 minutes. In a second study the authors described the results of 200 determinations done on in-patients. The average plasma value was .88 ± .20 mgm. percent while the average intradermal time was 9.1 ± 3.6 minutes. Sixty cases (30 percent) had plasma levels below .8 mgm. percent; 138 cases (69 percent) revealed levels between .8 and 1.5 mgm. percent; only 2 cases (1 percent) had values above 1.5 mgm. percent. The times varied from 3 to 24 minutes and the plasma values from .4 to 1.6 mgm. percent. The two variables were found to be in a relation which could have arisen by chance. The coefficient of correlation for the student data was -.6522 and for the in-patients -.6111. Of 61 “pyorrhea cases,” no low plasma levels were noted. Bakhsh et al. concluded that the intradermal time cannot replace the plasma level for estimating vitamin C status of the tissues. Additionally they noted that the intradermal time for any one individual did not vary significantly.
Banerjee and Guha
Banerjee and Guha21 sought a minimal decolorization time in human subjects. Six healthy adult students were subjected to the skin test (Rotter technique) and then given an oral dose of 700 mgm. of ascorbic acid. On the following four days the intradermal time and three-hour urinary ascorbic acid excretion were measured. The initial time range of the students was 1 to 2.5 minutes (average 2 minutes). On the fifth day a minimum skin time of 90 seconds was found in every case but one, whose score was 85 seconds. According to the urinary saturation test, all students were saturated on the third day. It should be mentioned that this urinary saturation test claims body saturation where the urinary disposal of ascorbic acid reaches a peak. Banerjee and Guha felt, on the basis of these studies, that the skin test is a more valuable indication of body saturation with ascorbic acid than the urinary excretion method. This they based on the fact that the renal threshold may vary and that the diuretic action of vitamin C may promote its own excretion in large amounts before the body has time to assimilate it.
Glatt
Glatt22 determined the plasma ascorbic acid values and intracutaneous decolorization times on 30 ill and convalescent infants ranging in age from 3 weeks to 5 months. Rotter’s technique was used except that the thigh was the injection site. In 20 of the infants, he found plasma levels from .36 to 1.44 mgm. percent (which he regarded as normal) and intradermal test times ranged from 9 to 46 minutes. The remaining 10 cases were given small (amount not specified) ascorbic acid supplements in the diet. He found no significant differences in skin test times in this group compared with the other 20 subjects, although the plasma levels were higher.
Rossini and Ferrari
Rossini and Ferrari23 employed Rotter’s technique in evaluating the intradermal test. Fortyseven pulmonary tuberculosis patients were studied from the standpoint of urinary saturation, capillary fragility, and intradermal time. They called attention to the fact that tubercular patients are recognized as deficient in vitamin C by all authorities. They stated that the deficiency status of the 47 patients was confirmed by the urinary saturation test and by the capillary fragility index. The urine saturation test consisted in determining the amount of ascorbic acid excreted within three hours after a 300 mgm. dose (route?) of ascorbic acid. A 40 percent excretion was accepted as normal; a 10 percent or less elimination was considered to be evidence of a deficiency state. They then proceeded to perform an intradermal time tolerance study. The decolorization time was determined for each patient. This was followed by an intravenous injection of 300-500 mgm. of ascorbic acid. One hour later, the test-time was again performed. The average disappearance time of four wheals raised simultaneously was taken as the true score. Initially the time-score range was 9-14 minutes. The postinjection values were from 6 to 9 minutes. The authors found that, within this group, the hemoptysis patients presented postinjection times longer than those who did not bleed. They concluded that a single skin test time is not informative.
Uzan
Uzan24 stated that he had been able to confirm the parallelism between the dye decolorization time and the body ascorbic acid status. Although no description of method nor results was given, he avowed that the correspondence between the skin time and the urine saturation test was experimentally verified by him. He also agreed with Rotter that local changes in vascular flow (dilatation, constriction) or changes in temperature did not appreciably alter the decolorization time. He felt that the action of other reducing agents in the skin was relatively weak. Uzan suggested that the skin test is an invaluable tool when other more complex methods are not available.
Uzan and Bronstein
In an abstract of an article by Uzan and Bronstein,25 based on Rotter’s technique, it was pointed out that times of 10 minutes or more denote deficiency; disappearance times of 2-3 minutes indicate health relative to vitamin C.
Uzan and Bronstein,26 in another publication, simply confirmed their earlier observations.25
Reddy and Sastry
Reddy and Sastry,27 in pilot studies on themselves, found that the decolorization time decreased from 10 minutes to 3 minutes 10 seconds, and from 6 minutes 40 seconds to 3 minutes 20 seconds respectively, after 5 and 7 days on a supplement of 70 mgm. ascorbic acid per stone weight (14 lbs.). They also noted that the intradermal time continued to diminish even after saturation was reached (on the basis of urinary excretion). These researchers used the Rotter method already described. In a series of medical students and young elementary school children, classified into three groups according to frequency of citrus fruit consumption, they found that those with the highest intake exhibited the lowest intradermal times, the scores being less than 10 minutes. Out of the 65 apparently healthy medical students, 48 (74 percent) had decolorization times between 5 and 9 minutes. Reddy and Sastry, consequently, agreed with Rotter that a 5 to 10 minute disappearance time signifies a satisfactory state of ascorbic acid nutrition.
Reddy and Sastry28 performed the intradermal test on 69 ophthalmic patients, employing a N/400 solution and 2 mm. wheal. At the same time, they collected information on the dietetic habits of the subjects. These authors were not evaluating the intradermal test–they were utilizing it as a measure of vitamin C status of ophthalmic cases. They concluded that patients with inflammatory eye diseases (retinitis, corneal ulcer, trachoma, optic neuritis) are more frequently associated with a vitamin C deficiency than those with cataracts alone.
Dollé
Dollé29 measured the intradermal times (Rotter’s method) of four healthy persons using as the variable dye solutions of different ages. In other words, it was possible to determine the disappearance time employing a freshly prepared solution and one which had been allowed to stand for one day. Under these conditions, he found variations of 3-4 minutes in decolorization times in each person. Dollé believed that this is due to a strong light sensitivity of the dye. It then follows that the post-preparation time of the test solution must be standardized. Dollé then performed intradermal times on each of 82 obstetric and gynecologic patients. No specific times are listed. However, the group with unusual surgical blood loss revealed the greatest number of subjects with prolonged disappearance times (values above 10 minutes). The converse was true in the normal group. The author then related these skin times to the clinical history of each patient regarding possible indications of a vitamin C deficiency (Rumpel-Leede phenomenon, gingival bleeding, general malaise). In about one-half of the subjects, there was a significant parallelism between the intradermal time and the clinical observation. Twenty-eight patients with prolonged times were given an unspecified amount of vitamin C per os. After one day, 6 showed normal times; after 6 days 14 revealed normal scores. Six other patients who had had initial decolorization times of 20 minutes decolorized the dye in 14 minutes at the end of the 6 day period. Six control persons not receiving the supplement showed consistently the same times throughout this study. Forty-three surgical patients were tested intradermally before and after an operation. The 6 patients with only minor surgical treatment showed no differences in pre- and postsurgical time. Of 37 who underwent extensive surgery (laparotomy), 16 showed increased postoperative skin times. Six others could not be evaluated since they had been injected intravenously with Ce-Ferro (an iron-ascorbic acid compound). In the remaining 15, no change was noted. Dollé concluded that the prolonged dye disappearance time is due to blood loss during the operation, lack of absorption and poor appetite following surgery. The author felt that his results qualify the skin test as a rough index of ascorbic acid nutrition.
Slobody
Slobody30 performed intradermal tests using varying wheal sizes and dye concentrations. He determined early that the 4 mm. wheal yielded the most constant test time when intradermal injections were performed simultaneously on the same forearm. Employing the 4 mm. wheal, he then introduced dye concentrations from N/1500 to N/300 intracutaneously in 167 patients. It became clear that the greater the concentration of DCPIP, the more reliable the test results would be. Not only would longer times lend themselves to easier interpretation, but the effects of other reducing substances present would be minimized. He subsequently employed a 4 mm. wheal (about .05 cc.) and a N/300 dye solution. (A N/300 DCPIP solution is prepared by dissolving 24 mgm. sodium 2,6-dichlorobenzenoneinindophenol in 35 cc. of distilled water heated to 95° C. This solution, when cooled, is then diluted to 50 cc. with distilled water in a volumetric flash.) He performed 285 skin test times in 167 hospital patients in duplicate on the same and opposite forearms. At the same time, a blood vitamin C determination was done. The blood levels varied from 0 to 1.97 mgm. percent. The decolorization times ranged from 3.5 to 25.6 minutes. Fifty-nine blood levels were below .3 mgm. percent. In this group, 5 subjects exhibited times between 9.5 and 13.2 minutes; the remaining 54 showed times above 14 minutes. The mean skin test time for this category was 16.7 minutes. Since a correlation existed in only about 50 percent of the total number of patients, the author questioned the validity of plasma level as a determinant of nutritional status. The statement was made that the continuous fluctuating plasma ascorbic acid level reflected only recent dietary intake. In some patients, for example, who had taken vitamin C the previous day, high plasma levels were manifest while the intradermal time remained elevated. Forty-five cases were given 200 mgm. ascorbic acid intravenously following plasma and intradermal determinations. Thirty minutes postinjection the same measurements were repeated. In 44 of the 45 cases, the skin test time diminished and the plasma level of ascorbic acid increased. In addition, 10 children (aged 3 to 11 years) were placed on diets free of fruits and fruit juices. Plasma scores and intradermal times were determined weekly. The blood vitamin C level decreased with simultaneous increase in disappearance time. After 9 weeks, the skin test time exceeded 14 minutes. Biomicroscopic gingival examinations revealed changes attributable to hypovitaminosis C as described by Kruse.31 Two of the children were subsequently given ascorbic acid and the skin test times returned to normal. The DCPIP time in one typical child, on this regime for 9 weeks, increased from 7.5 to 16.5 minutes. Within this same period, the blood level of ascorbic acid declined from 1.33 to .20 mgm. percent. Slobody suggested, on the basis of his recommended technique, with N/300, 4 mm. wheal and .05 cc., that a disappearance time above 14 minutes be regarded as evidence of pronounced unsaturation; 9 to 13 minutes as mild unsaturation; less than 9 minutes as proof of a satisfactory vitamin C status. He further suggested that the intradermal decolorization time might well be developed into a saturation index. This would be, he believed, a welcome and simple tool. It is of interest that some of his subjects reported a burning sensation during injection. Two of the 10 children developed nodules at the injection site which persisted for two weeks.
Banerjee
Banerjee32 found statistically insignificant variations in decolorization time in 6 individuals when the dye solution was injected into the same part of the arm oa successive days, into adjacent sites on the same day, and simultaneously in opposite arms. Six subjects were given 200 mgm. of ascorbic acid daily for 3 weeks. The intradermal times diminished gradually from 5-12.5 minutes to 2.7-5.0 minutes. On the basis of his previous study,13 in which he established that 90 seconds indicates saturation, he concluded that 200 mgm. ascorbic acid per day is not sufficient to produce saturation. He indicated in this report that the skin test time varied with the season and with the availability of fresh citrus fruits and vegetables. It was Banerjee’s opinion that the decolorization time is a fair index of group vitamin C status but only a rough estimate of the individual’s ascorbic acid tissue level.
Gounelle and Vallette
Gounelle and Vallette,33 using a N/400 dye concentration and 2 mm. wheals, studied the whole blood ascorbic acid levels and skin test times in 88 human beings. The subjects included 38 controls, 41 apyretic and 9 pyretic tuberculous individuals. The whole blood ascorbic acid levels and disappearance times in the control group ranged from 0 to 17 mgm. percent and 2 to 12 minutes respectively. in the apyretic tuberculous group the scores were 0 to 13 mgm. percent and 2.5 to 13 minutes. The pyretic group exhibited values of 2.5 to 14 mgm. percent and 3 to 6 minutes. The investigators contended that there is no correlation between blood and skin test results and that the blood determinations remain the best index of latent hypovitaminosis C.
Moena and Nolff
Moena and Nolff34 employed the method of Slobody.30 They modified the method by utilizing an 8.5 percent solution of sodium chloride as the dye solvent in place of distilled water. This substitution was found to reduce the burning pain associated with the injection. In the majority of cases, an indurated postinjection nodule persisted for 3 to 4 days. An interesting observation was that a characteristic red, pruritic papule appeared 10 days following the skin test and persisted 6 to 8 days. They felt this was an anaphylactic phenomenon. They performed the skin test in 1,150 persons. Of these, 845 were considered to be healthy individuals. The group was analyzed as a whole and in the light of such factors as age, sex, type of work. The authors evidently accepted the contention of Slobody30 that disappearance times above 14 minutes indicate a subnormal ascorbic acid status. The findings in the 845 healthy persons disclosed 77 percent with skin time below 10 minutes, 21 percent between 17-20 minutes, and 2 percent 21-25 minutes. The authors concluded that, with advancing age, the intradermal time lengthened. No sex differences could be observed. They next undertook a study of 305 pathologic cases. It appeared to these investigators, from a study of intradermal time in patients with different disorders, that certain conditions (e.g. osteomyelitis and pregnancy) were not associated with an ascorbic acid deficiency. In contrast, in other pathologic states (e.g. typhoid fever, deficiency states, narcosis, chronic gastritis) 100 percent of the subjects showed significantly prolonged intradermal times. Thus, of the total 305 pathologic cases, 40 percent exhibited times below 14 minutes whereas 57 percent of the so-called healthy persons showed the same disappearance values. The authors then selected 162 patients on the basis of factors presumed to be associated with vitamin C deficiency. The evidence, from intradermal testing, disclosed that 60 to 90 percent of such individuals displayed decolorization times greater than 14 minutes. Another study was performed with 28 patients. They were given vitamin C orally or intravenously to observe the effect upon the skin time. No information as to dosage or time intervals was given. Specific figures were available in some cases but not in others. Fourteen persons who had original times over 14 minutes, declined to a level below 14 minutes after load dosing. Seven persons who were originally above 14 minutes, exhibited a 16 percent mean decrease (from an average of 19.7 minutes to 16.4 minutes). This group did not, then, fall below 14 minutes after the tolerance dose. Two persons who had received 500 mgm. of ascorbic acid for 2 and 3 days respectively, showed no change from the original score of 16 minutes. Five persons who were originally below 14 minutes declined in time an average of 19.5 percent (from a mean of 11.2 minutes to 9 minutes). All the patients except two showed a decrease in time. Another study was done to observe the changes in plasma ascorbic acid following a load dose. Oral administration elicited a rise in ascorbic acid blood level in one hour; the intramuscular route caused an increase in 30 minutes; the intravenous injection prompted an immediate climb. The ascorbic acid levels began to decline after about 4 hours in the case of intramuscular and oral routes, whereas the intravenous route was associated with an intense level for 2 hours, after which there was a decline. The authors measured the plasma ascorbic acid level twice in the same day on 16 patients following oral vitamin C. They stated that each individual exhibited the same pattern on both occasions. On the basis of plasma ascorbic acid determinations of 10 presumably healthy individuals, they established a plasma level of .8 mgm. percent or more as an index of health. Using this plasma norm and 14 or less minutes as a normal intradermal time, they studied 39 subjects. Twenty of the patients, with intradermal times above 14 minutes, showed plasma levels less than .8 mgm. percent and 11 subjects, with intradermal times greater than 14 minutes, displayed plasma levels above .8 mgm. percent. In contrast, only 1 of the 8 persons with an intradermal time below 14 minutes showed a plasma level below .8 mgm. percent. Moena and Nolff then determined 24 hour urinary concentrations of ascorbic acid. They found a great periodic variation in the amount excreted during the day. They cautioned that single determinations are not sufficient to fix a diagnosis of vitamin C deficiency. The researchers concluded that treatment with vitamin C should be evaluated on a three-fold basis: (1) enhanced urinary ascorbic acid excretion, (2) 3-day normal fasting plasma level, and (3) normal skin time. Of these, the authors seemed to prefer the skin test.
Bicknell and Prescott
Bicknell and Prescott,35 having reviewed the literature, considered the intradermal test of no clinical value. They believed that too many variables exist to allow any specific knowledge of vitamin C status from the skin test time (other reducing agents, changes in temperature, circulation and oxygen supply).
Zanotti
Zanotti36 employed Rotter’s method to determine intradermal times in 50 frostbitten soldiers. All decolorization times were in excess of 10 minutes: 10 subjects ranged between 10 and 15 minutes; 25 yielded times between 15 and 25 minutes; 15 revealed skin times in excess of 25 minutes. The author felt that subnutritional states and frostbite are somehow related. For this reason Zanotti suggested that the test might measure only skin saturation which was not a true barometer of total body status. He gave large doses to the soldiers and found that the intradermal times diminished. He was then inclined to postulate that, perhaps, the Rotter skin time could be utilized in ascertaining complete saturation after prolonged ascorbic acid therapy.
Viñas-Espin
Viñas-Espin,37 using a concentration of 40 mgm.1100 cc. of DCPIP (approximately N/300) and an intradermal injection of .025 cc., found a clear decrease of decolorization time following the administration of 300 mgm. of ascorbic acid. Precisely how the ascorbic acid was given and the number and health of the patients was not mentioned. In addition, he determined the concentration and the absolute amount of ascorbic acid in the urine of patients who were given ascorbic acid and thiamin for 4 to 13 days. According to his observations, the first effect of vitamin C administration is a lowering of urinary ascorbic acid and phosphate. On the basis of this observation, Viñas-Espin postulated that ascorbic acid plays a role in phosphorylation. He found that thiamin hydrochloride, given after ascorbic acid had been taken regularly, further improved the cellular reductive power. Expressed more simply, the irreducible intradermal time following ascorbic acid intake can be further reduced with thiamin hydrochloride. Additionally, when thiamin was administered together with ascorbic acid, there was an increase in the urinary excretion of vitamin C. From these observations the author then theorized a relationship between the oxidative metabolism of tissue ascorbic acid and the phosphorylation process.
Summary
The following tables are submitted as a historical outline of the intradermal ascorbic acid test in human subjects. All reports available to the compilators were based on the use of 2,6 dichlorophenolindophenol. From Table 1 it is evident that: (1) of those who report the quantity of dye injected, all investigators except four utilized a .01 cc. injection as proposed by Rotter, (2) a DCPIP concentration of N/400 was employed in all studies except six, (3) when wheal size was specified, it was, with three exceptions, 2 mm., and (4) the forearm was the most popular injection site.
Table 1
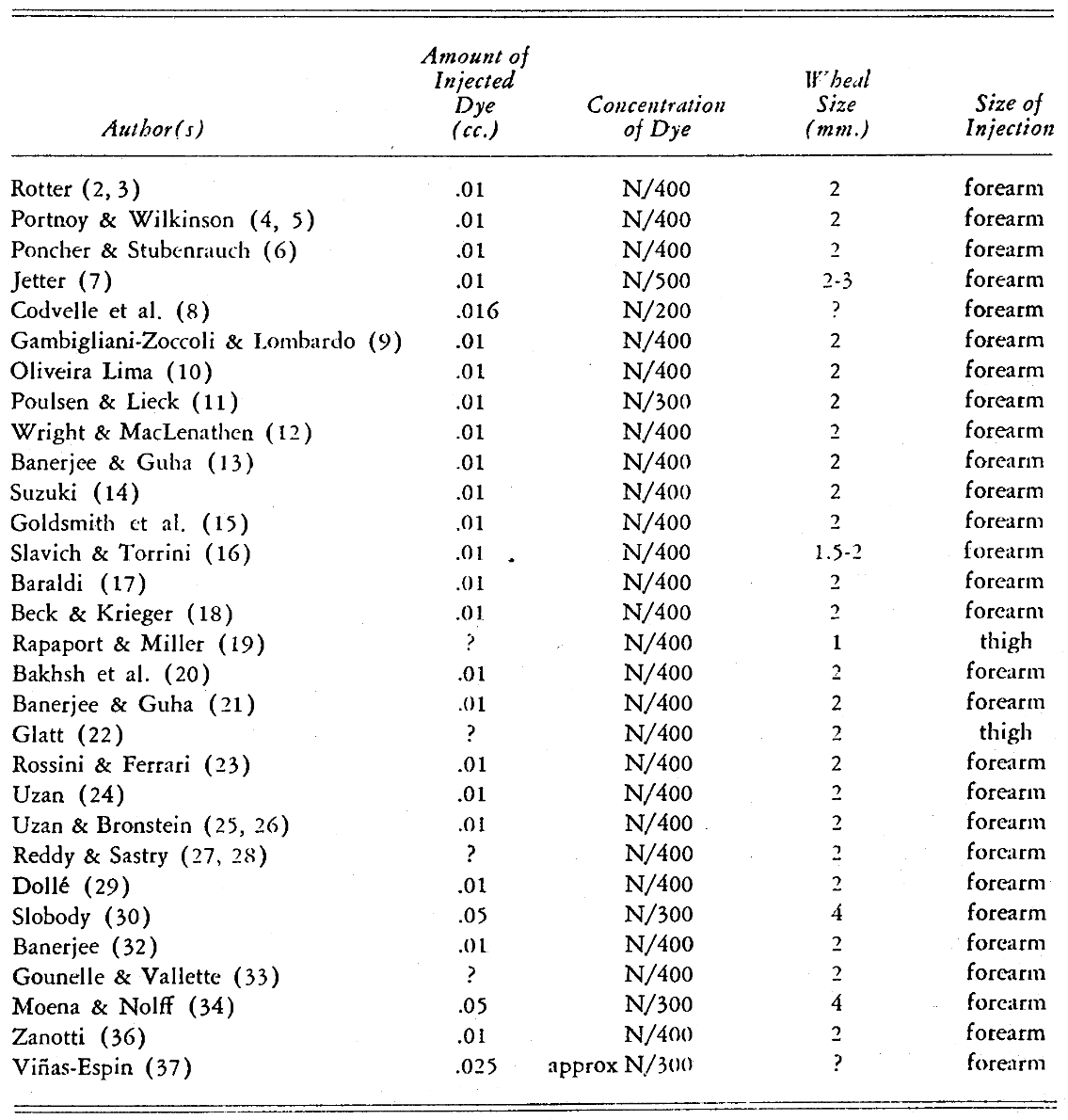
Table 2 summarizes the number and health of the subjects and the length of the investigation.
Table 2
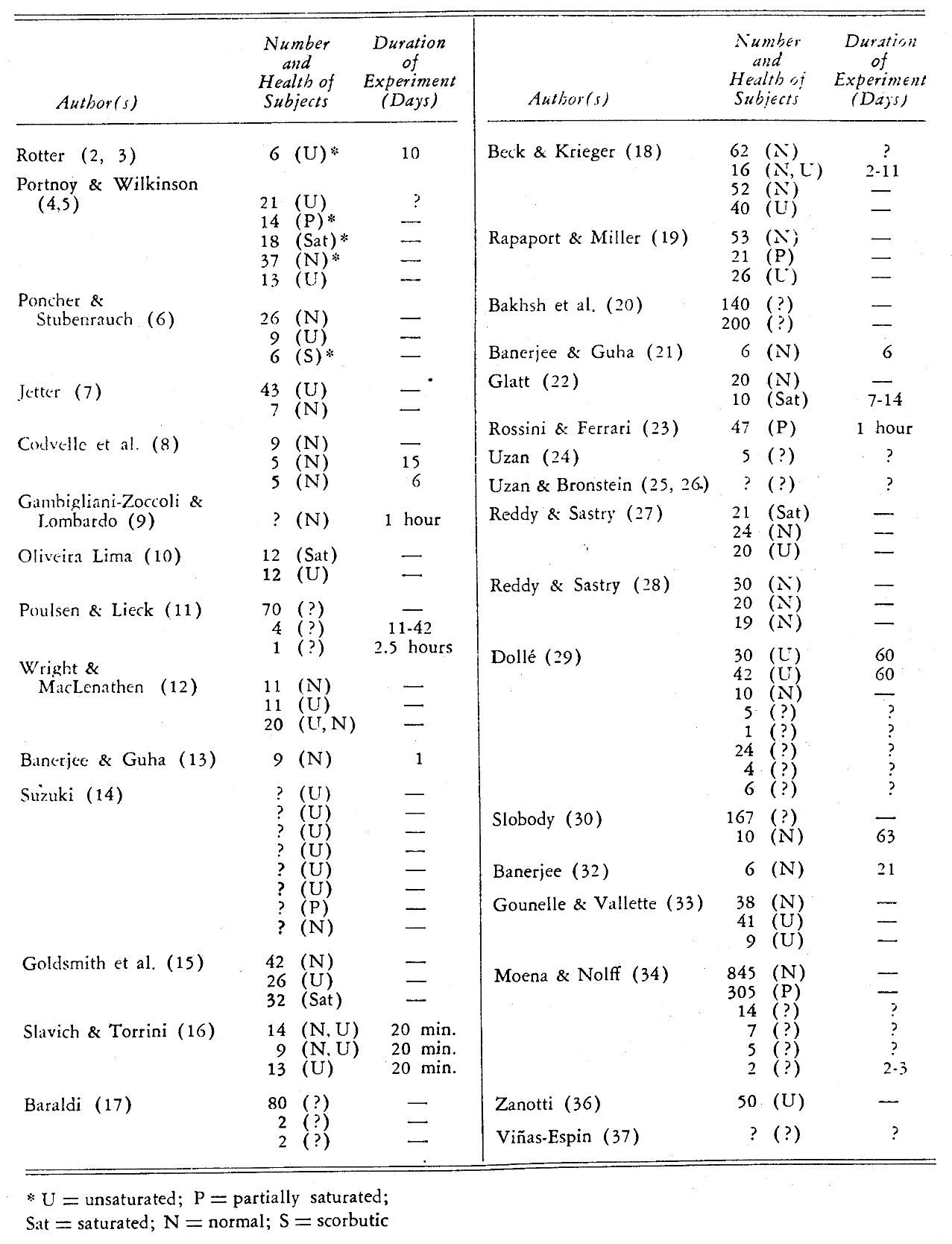
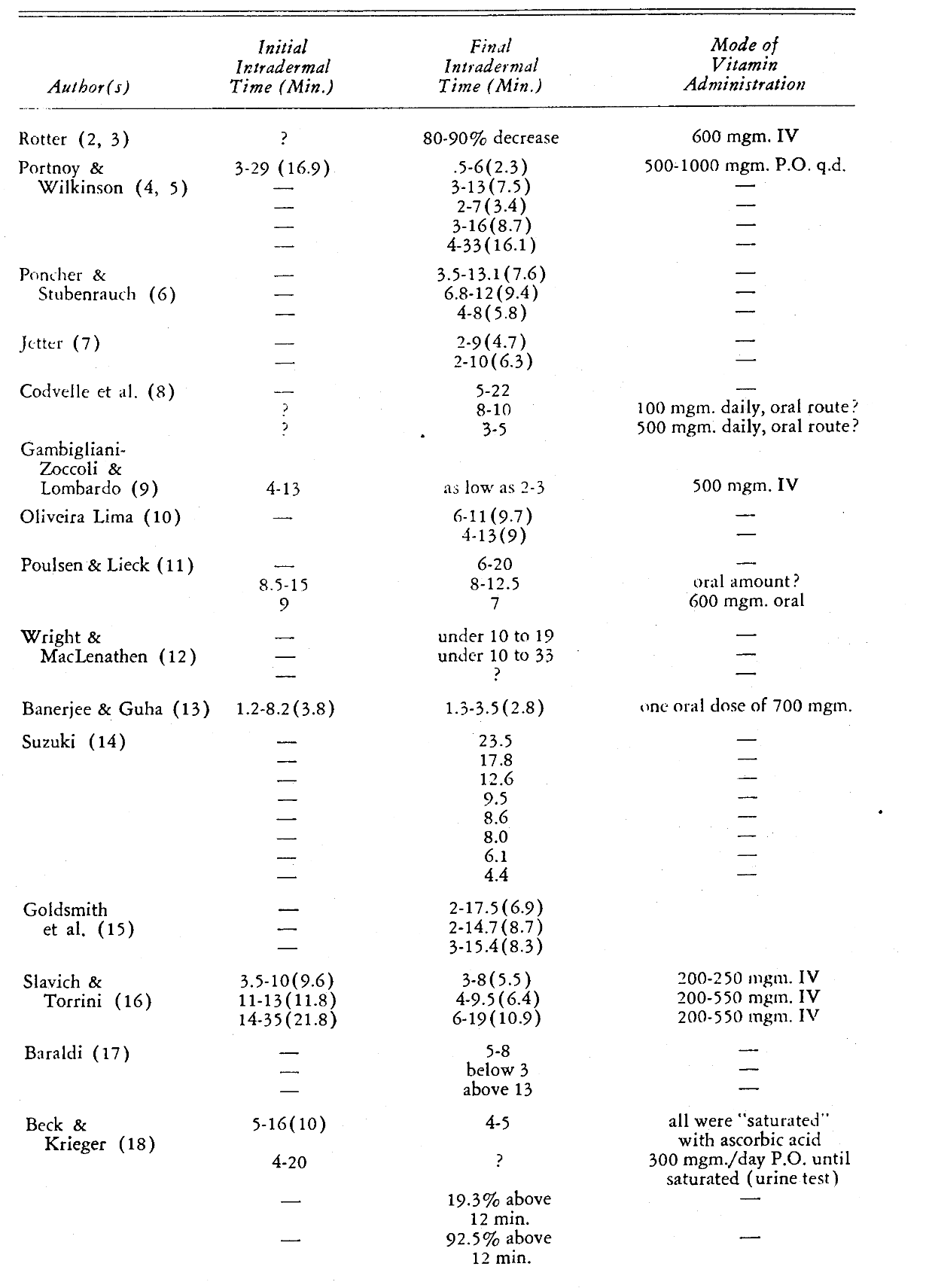
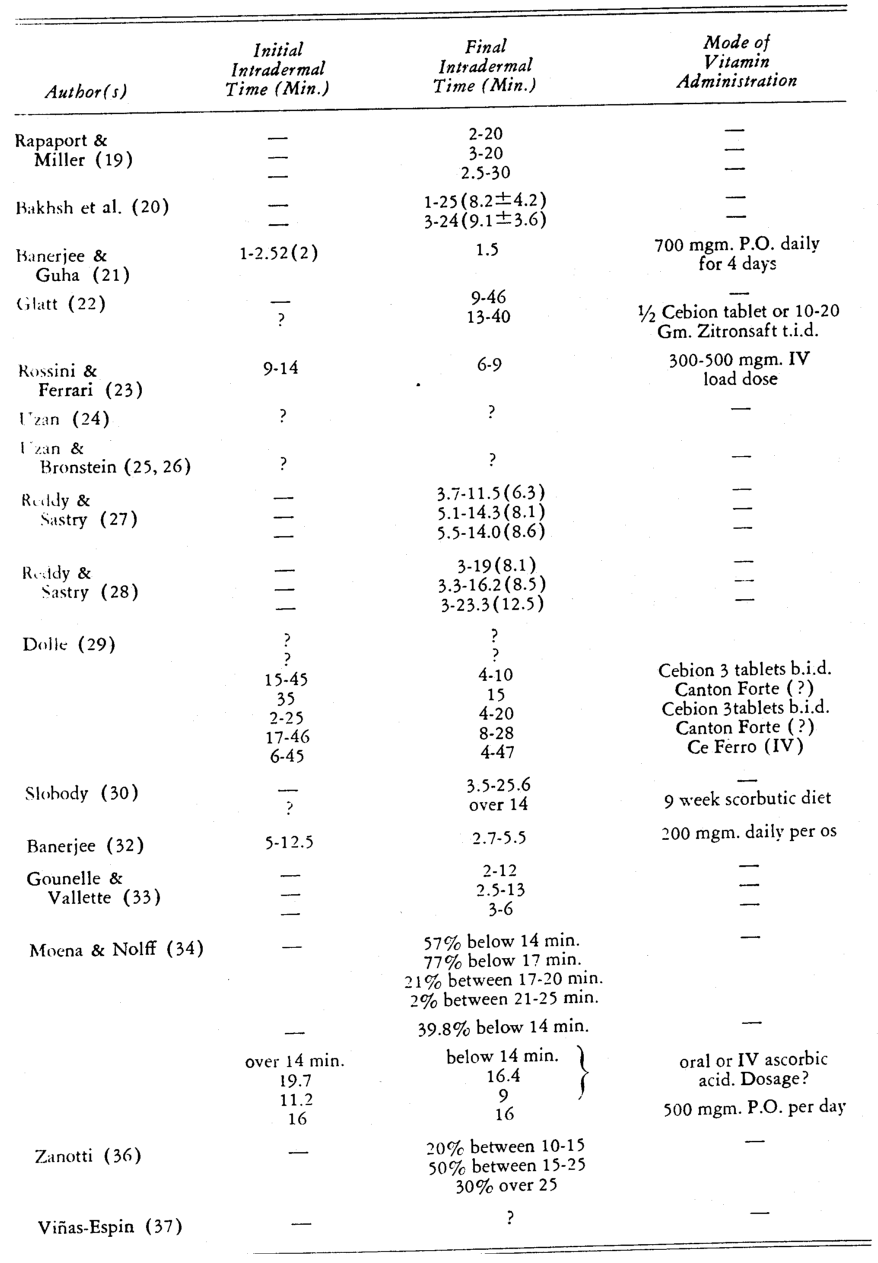
Table 3 outlines the essential experimental data relative to the intradermal test. Examination of the tabulation reveals:(1) in only 11 out of 31 investigations are there scores reported both at the start and finish of the investigation, (2) groups of subjects deficient in ascorbic acid generally require a longer therapeutic interval to reduce the DCPIP disappearance time, (3) group administration of ascorbic acid is followed by a diminution in decolorization time and the decline is related to the amount of vitamin given, the route of administration, and the time interval between dosage and final intradermal testing.
Table 3
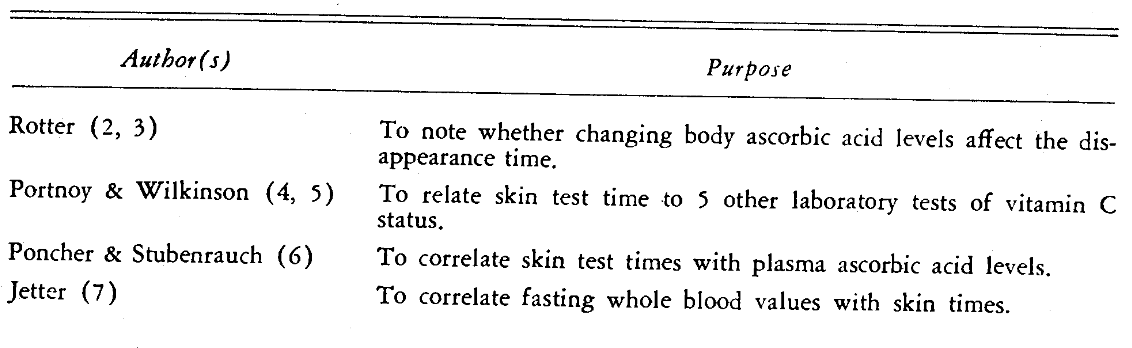
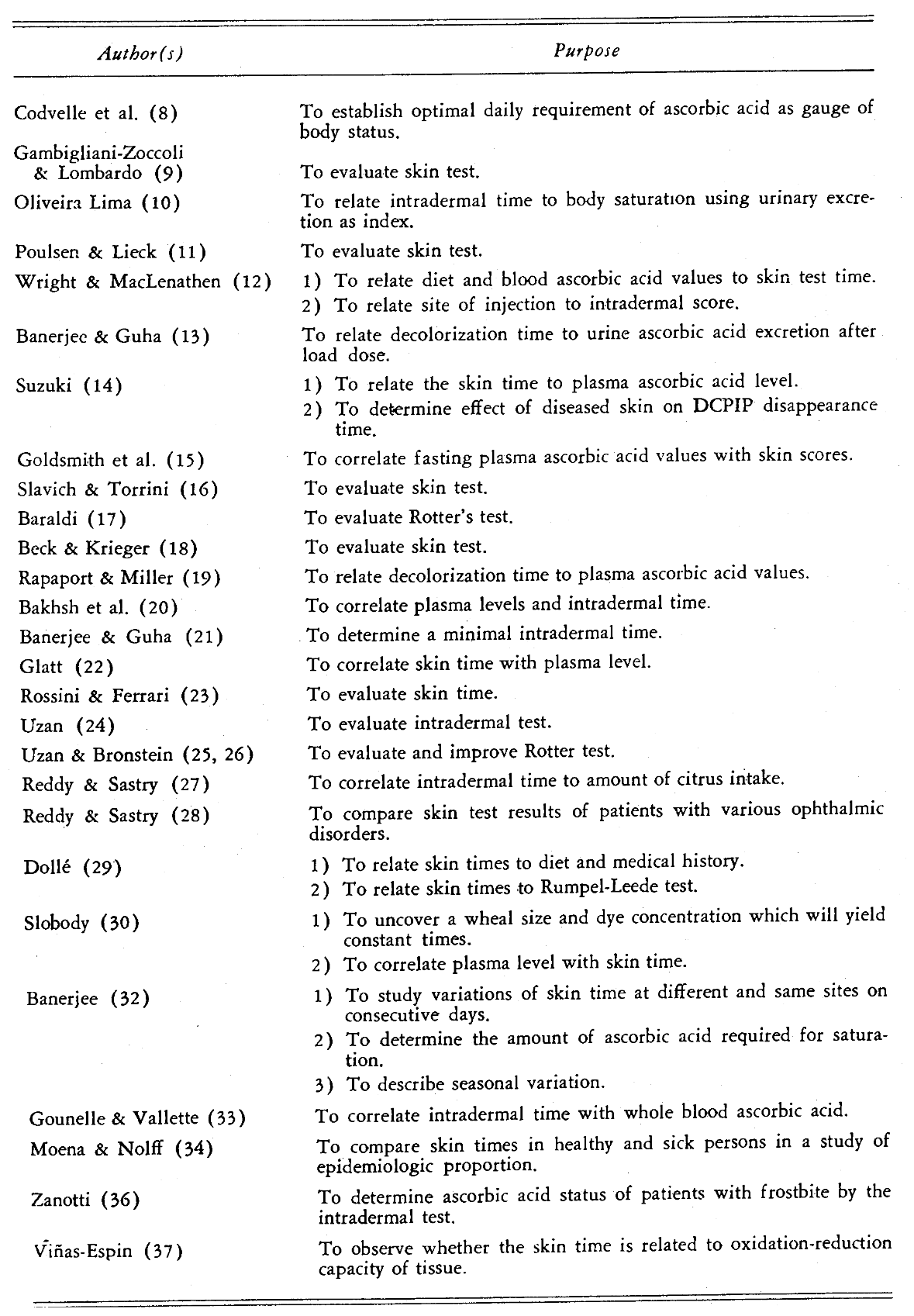
The essential aim of each report is briefly stated in Table 4. The purpose may be summed up in a few statements: (1) to ascertain whether the decolorization time varies with decrease and increase of body ascorbic acid, (2) to establish whether a significant relationship exists between the intradermal score and other measures of vitamin C status–particularly the fasting plasma ascorbic acid concentration, (3) to evolve an irreducible skin test value indicative of absolute saturation, (4) to determine local variables affecting the final decolorization score, (5) to establish empirically a dye concentration and wheal size which provide repetitive decolorization times, (6) to relate cutaneous decolorization scores to age, (7) to contrast the skin test values of healthy and ill subjects, and (8) to disclose whether the Rotter test measures oxidation-reduction capacity of the tissues.
Table 4
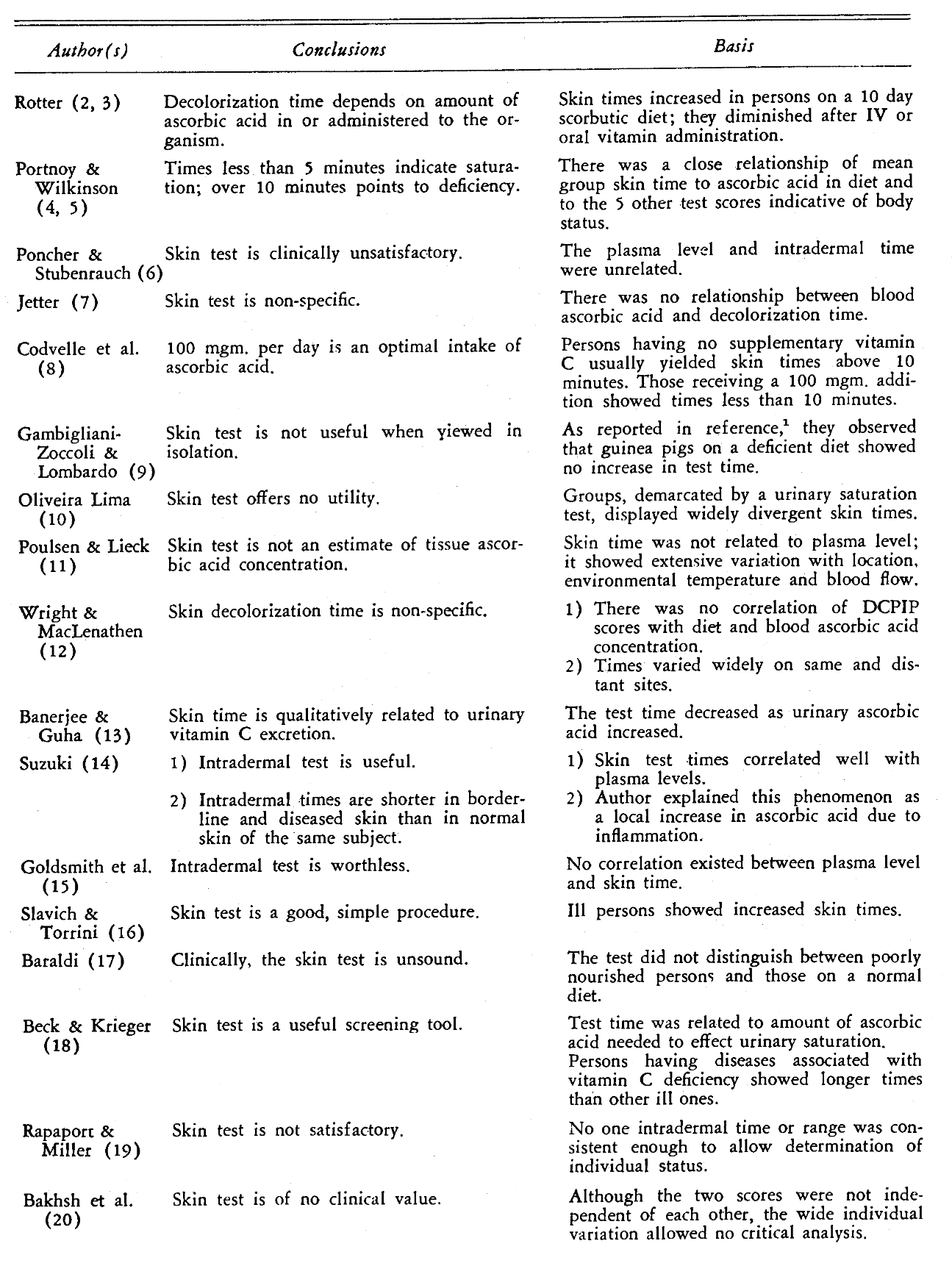
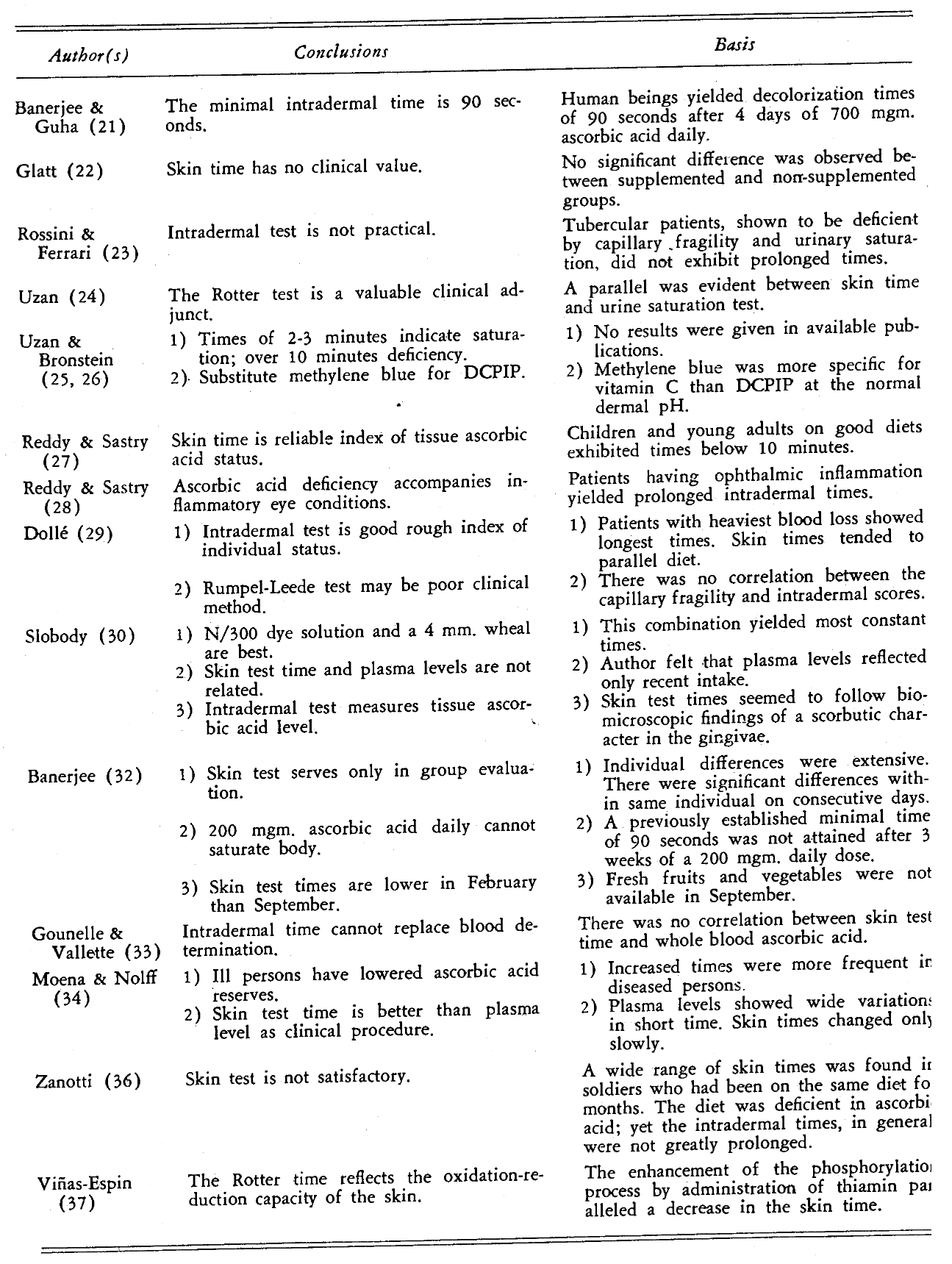
The evidence from Table 5 is that: (1) the decolorization time does vary inversely with changes in total body ascorbic acid, (2) there is no experimental unanimity concerning the presence or absence of a relationship between Rotter’s time and plasma ascorbic acid content, (3) ninety seconds is an irreducible DCPIP disappearance time, (4) changes in age and concentration of solution, vascular flow, site of injection, wheal size, light intensity, and depth of puncture do significantly alter the decolorization time, (5) a dye concentration of N/300 and a wheal size of 4 mm. yields the most reproducible results, (6) skin test time appears to increase with age and/or disease, (7) the cutaneous vanishing time varies with changes in oxidation potential of the tissues.
Table 5
A subsequent publication38 will concern itself with an analysis of a group of our own patients.
References Cited:
- Cheraskin, E., Dunbar, J. B. and Flynn, F. H. “The intradermal ascorbic acid test. Part I. A review of animal studies.” Jour. Dent. Med. 12:174-184, Oct. 1957.
- Rotter, H. “Determination of vitamin C in the living organism.” Nature 139: #3521, 717, April 24, 1937.
- Rotter, H. “Bestimmung des Vitamin C in lebenden Organismus.” Wiener Klin. Wchnschr. 51: #7, 205- 206, February 18, 1938.
- Portnoy, B. and Wilkinson, J. F. “Intradermal test for vitamin C deficiency.” Brit. Med. Jour. 1: #4023, 328-329, February 12, 1938.
- Portnoy, B. and Wilkinson, J. F. “Vitamin C deficiency in peptic ulcer and haematemesis.” Brit. Med. Jour. 1: #4027, 554-560, March 12, 1938.
- Poncher, H. G. and Stubenrauch, C. H. “Intradermal dye test for vitamin C deficiency.” J. A. M. A. 3: #4, 302-304, July 23, 1938.
- Jetter, W. W. “Correlation between blood ascorbic acid and the dichlorophenolindophenol intradermal test.” Proc. Soc. Exper. Biol. and Med. 39: #1, 168- 171, October 1938.
- Codvelle, E., Simonnet, H. and Mornard, J. “Recherches sur la carence en acide ascorbique.” Presse Med. 46: #95, 1745-1748, November 26, 1938.
- Gambigliani-Zoccoli, A. and Lombardo, V. “L’intradermoreazione di Rotter quale indice del grado di saturazione dell’organismo in vitamina C.” Riforma Medica 54: #39, 1489-1490, October 1938; Accademia di Med. di Torino Gior. 101: #3, 428-433, July-September 1938.
- Oliveira Lima, A. “Sobre o valor do ‘test’ intradérmico com o dichlorophenol para o reconhecimento de estados sub-escorbuticos.” Brasil-Medico 53: #5, 178-180, January 1939.
- Poulsen, E. and Lieck, H. “Undersolgelser over H. Rotter’s intracutanprove paa mennesker til paavisning of vitamin C.” Ungeskrift for Laeger 101: #7, 206-208, February 16, 1939.
- Wright, l. S. and MacLenathen, E. “The intradermal test for vitamin C determination.” Jour. Lab. and Clin. Med. 24: #8, 806-807, May 1939.
- Banerjee, S. and Guha, B. C. “The intradermal test as an index of vitamin C nutrition. Part 11.” Indian Med. Gaz. 75: #8, 468-471, August 1940.
- Suzuki, S. “Vitamin C and skin diseases. Report 11. Intradermal test with 2,6 dichlorophenolindophenol.” The Jour. of Oriental Med. 30: #6, 267-269, June 1939.
- Goldsmith, G. A., Gowe, D. F. and Ogaard, A. T. “Determination of vitamin C nutrition by means of a skin test. A critical evaluation.” Proc. Soc. Exper. Biol. and Med. 41: #2, 370-374, June 1939.
- Slavich, E. and Torrini, A. “Prova di Rotter e suoi rapporti con il contenuto cutaneo di vitamina C.” Gior. Di Clin. Med. 20: #9, 831-841, June 30, 1939.
- Baraldi, M. “La vitamina C determinata col metodo di Rotter nell’organismo dei malati di mente.” Revista Sperimentali di Freniatria 63:368-373, June 30, 1939.
- Beck, H. and Krieger, F. H. “Was leistet Eine Intrakutanprobe mit Indophenol zur Prüfung des Vitamin C Haushaltes?” Deut. Med. Wchnschr. 65: #34, 1336-1340, August 1939.
- Rapaport, H. G. and Miller, S. H. “The determination of vitamin C in children by intradermal injections.” Jour. Pediat. 15: #4, 503-507, October 1939.
- Bakhsh, M. l., Kochlar, B. D. and Malik, A. W. “The evaluation of the intradermal dye test for vitamin C in health and disease.” Indian Jour. Med. Res. 27: #3, 695-703,,January 1940.
- Banerjee, S. and Guha, B. C. “The intradermal test as an index of vitamin C nutrition. Part IV. The relation between the intradermal test time and the ascorbic acid content of the liver of guinea pigs.” Ann. Biochem. and Exper. Med. 2: #2, 121-124, March 1942.
- Glatt, J. “Die Beurteilung der Vitamin C. Sättigung der Gewebe durch die Intrakutanreaction von Rotter bei Kranken und rekonvaleszenten Säuglingen.” Dent. Med. Wchnschr. 66: #47, 1304-1305, November 1940.
- Rossini, G. and Ferrari, B. “Sul valore della intradermoreazione di Rotter nella tuberculosi pulmonare.” Boll. Soc. Med. Chir. Pavia 54: #6, 1277-1285, November-December 1940.
- Uzan, M. “L’appréciation de l’hypovitaminose C, parle test de Rotter.” Medecin chez Lui 1 5: #14, 13-14, July 1938.
- Uzan, M. and Bronstein, l. “Epreuve de Rotter et ascorbotherapie.” Abstracted in: Zeitschrift f. Vitaminforschung 9: 379-380, 1939.
- Uzan, M. and Bronsteín, l. “Contribution nouvelle à l’étude de L’épreuve de Rotter.” Médecin chez Lui 16: #9, 16-21, May 1939.
- Reddy, D. V. S. and Sastry, P. B. “Intradermal test as an index of vitamin C nutrition of the body observations at Vizagapatam.” Indian Med. Gaz. 76: #8, 476-480, August 1941.
- Reddy, D. V. S. and Sastry, P. B. “Intradermal test for vitamin C nutrition of the body in ophthalmic patients.” Jour. Indian Med. Assn. 10: #11, 440-443, August 1941.
- Dollé, W. “Uber Vitamin-C-Schnellbestimmung mit dem intradermalen Testverfahren nach Rotter.” Zentralbl. f. Gynäk. 65: #8, 1414-1418, August 2, 1941.
- Slobody, L. B. “An intradermal test for vitamin C subnutrition. Preliminary report.” Jour. Lab. and Clin. Med. 29: #5, 464-472, May 1944.
- Kruse, H. D. “The gingival manifestations of avitaminosis C, with especial consideration of the detection of early. changes by biomicroscopy.” Milbank Mem. Fund Quarterly 20: #3, 290-323, July 1942.
- Banerjee, S. “A study of the intradermal test of Rotter for vitamin C status.” Indian Med. Gaz. 79: #9, 420-423, September 1944.
- Gounelle, H. and Vallette, A. “Test de Rotter et teneur en vitamine C.” Comp. Rend. d. Sean. de la Soc. de Biol. 138: #19-20, 740-742, October 1944.
- Moena, A. and Nolff, E. “Test intradérmico para la determinación de la saturación tisular en vitamina C.” Anales Médicos de Conception 2: #3 & 4, June December 1945.
- Bicknell, F. and Prescott, F. The vitamins in medicine. Ed. 2., 1946. New York, Grune and Stratton. pp. 542-543.
- Zanotti, M. “Risultati della intradermoreazione di Rotter nei militari colpiti da congelamento.” Gior. Med. Mil. 94: #6, 442-453, November-December 1947.
- Viñas-Espín, J. “Le test de Rotter dans la détermination de l’avitaminose C-B1 chez l’homme.” Bull. Soc. Chim. Biol. 33: #9, 1168-1173, Summer 1951.
- Cheraskin, E., Dunbar, J. B. and Flynn, F. H. “The intradermal ascorbic acid test. Part III. A study of 100 patients.” (To be published).