
Access to all articles, new health classes, discounts in our store, and more!
The Eating Habits of Smokers and Non Smokers
Published in Journal of the International Academy of Preventive Medicine, Vol. II, No. 2, Second Quarter 1975.
* * *
Doctor Cheraskin has been trained both in medicine and dentistry and is now Professor and Chairman of the Department of Oral Medicine at the University of Alabama in Birmingham School of Dentistry in Birmingham, Alabama. He is the author of numerous publications and books, the latest being a lay book entitled Psychodietetics designed to relate food and behavior.
Introduction
A logical but often misleading hypothesis involves the assumption that if B follows A, then A is necessarily the cause and B is the effect. By this logic, one correctly concludes that the patellar tap is the cause and the subsequent knee jerk is the effect. By this same hypothesis, one incorrectly concludes that an aspirin deficiency is the cause of headache since a headache is frequently relieved after the administration of aspirin.
This report is intended to analyze the same hypothesis with regard to daily tobacco consumption. Are the salutary effects which follow the elimination of tobacco the direct result of the tobacco? For example, is tobacco the cause (A) and improvement in cardiovascular fitness the effect (B)? Or, does tobacco act as a cause (A) and so serve to effect a change in some other variable (C) which, in turn, determines (B)? Or, is the effect (B) really the result of tobacco consumption (A) and another variable (C)?
Materials and Methods
Approximately 700 members of the health professions shared in a multiphasic health examination extended over a period of about seven years. Every subject completed the Oral Health Index Questionnaire (OHI).1 Question #44 asks: “Have you smoked more than one-half pack of cigarettes each day?” Additionally, the subjects completed, at each annual examination, a dietary survey. The dietary record consisted of the answers to a food frequency questionnaire, which was submitted to a computer center and provided a readout showing the daily intake of the major foodstuffs and the common vitamins and minerals.2
By means of this information, it was possible to analyze the diet in terms of an assessment of tobacco consumption habits.
Results
Figure One shows the mean daily intake of vitamin C as obtained from the food frequency dietary record versus the daily tobacco consumption as derived from the Question #44 on the Oral Health Index Questionnaire (OHI). Subjects who reported the lesser tobacco consumption (0-10 cigarettes per day) consumed, on the average, 333 milligrams of vitamin C. In contrast, subjects who reported a greater consumption (11+ cigarettes per day) consumed 267 milligrams of vitamin C per day. More importantly, the difference of 20 per cent was statistically significant (t = 3.888, P<0.001). Thus, it would appear that the relative nonsmoker tends to consume more vitamin C than do the individuals with the greater tobacco intake.
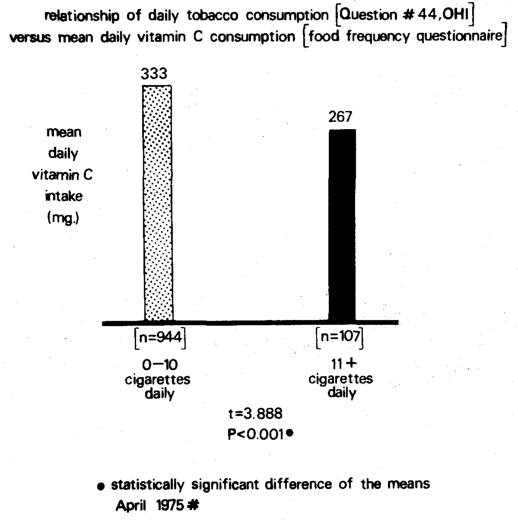
Figure One. The relationship of daily cigarette consumption (on the abscissa) versus daily vitamin consumption (on the ordinate). Those consuming the fewer cigarettes clearly show the higher vitamin C intake.
Table One summarizes the relationship between daily tobacco consumption and the daily intake of all nutrients (according to the food frequency questionnaire). Table One also lists the nutrient-tobacco relationships in decreasing order of statistical significance as judged by the t values and the probabilities. The dietary intake of several nutrients was substantially different in smokers compared with nonsmokers (lines 1-12). The relatively heavier smoker group showed a lower intake of vitamin C, potassium, vitamin B12, pantothenic acid, percentage polyunsaturated to saturated fat, vitamin B6, total protein, vitamin B2, valine, and vitamin E. On the other hand the heavier smokers displayed a larger intake of refined carbohydrate foodstuffs (line 12).
Table One. The relationship of daily cigarette consumption versus dietary habits.
A sizable number of nutrients are consumed in lower quantities in the relatively heavier smoker. Even where there are no statistically significant differences, the trends are the same. With regularity, sugar and other measures of refined carbohydrate-intake are higher in the smoker.
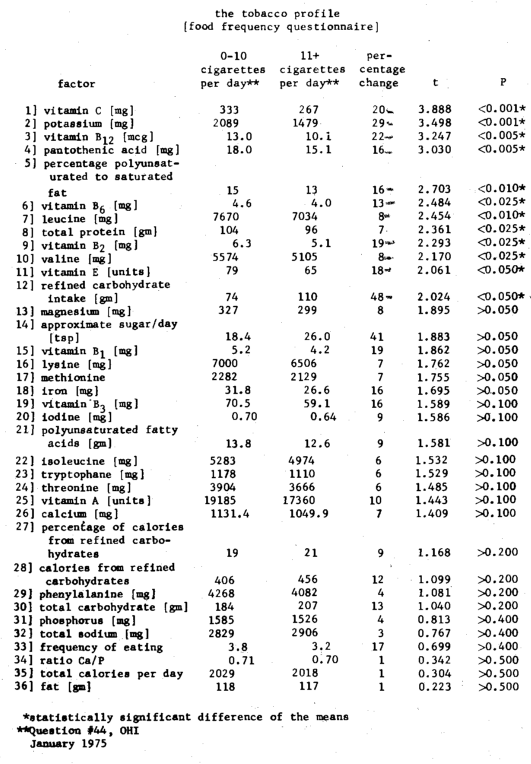
The pattern prevailed even in cases in which the differences were not statistically significant. Thus, although not significant by the usual statistical criteria, the magnesium, vitamin B1, lysine, methionine, iron, vitamin B3, iodine, polyunsaturated fatty acids, isoleucine, tryptophane, threonine, vitamin A, calcium, phenylalanine, and phosphorus were lower in the relatively greater smoking group. Conversely, though not meeting the rules for statistical significance, the approximate sugar per day in teaspoonsful, the percentage of calories derived from refined carbohydrates, calories from refined carbohydrates, and total sodium were higher in the heavier smoker group.
Discussion
Man may be viewed like a sphere (Figure Two).3 The peripheral layer represents the clinical pattern of signs. Beneath this lamella are the prodromal symptoms. Stripping away this area brings into focus the performance layer which suffers before the advent of symptoms and signs. Subjacent is the biochemical pattern which reflects problems before they erupt more peripherally. In order, moving toward the center, are the hormonal and then the enzyme layers. Finally, at the core is the real problem. The core factors are mistakes in living and include such things as diet and nutrition, drugs, physical activity, and light. For purposes of this discussion, tobacco will be utilized to show that tobacco intake modifies all of the peripheral lamellae.
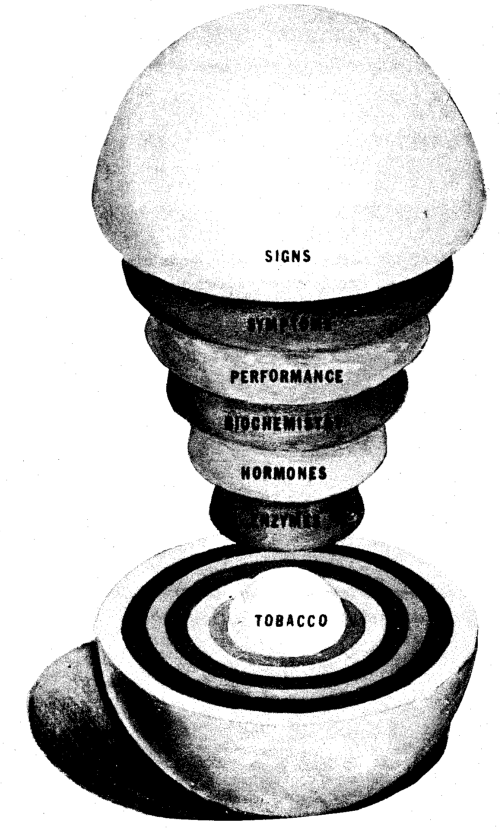
Figure Two. The sequence of events leading to clinical evidence of disease (signs) by utilizing tobacco as one of the core problems.
However, it must be remembered that smokers tend to eat differently than nonsmokers. Hence, changes in the peripheral areas may be the result of the (1) smoking habit, or (2) the diet which is different in the smoker, or (3) both.
For example, Figure Three outlines the relationship between cigarette intake (the core in Figure Two) and the mean number of oral symptoms and signs designated the Presorex (in the most peripheral layer in Figure Two). In the 950 subjects consuming 0-10 cigarettes per day, the mean number of oral symptoms and signs is 7.8; in the group of 112 with 11+ cigarettes daily the oral symptoms and signs average is 14.4. Thus, under these conditions, the heavier smokers display almost double the oral disease score.
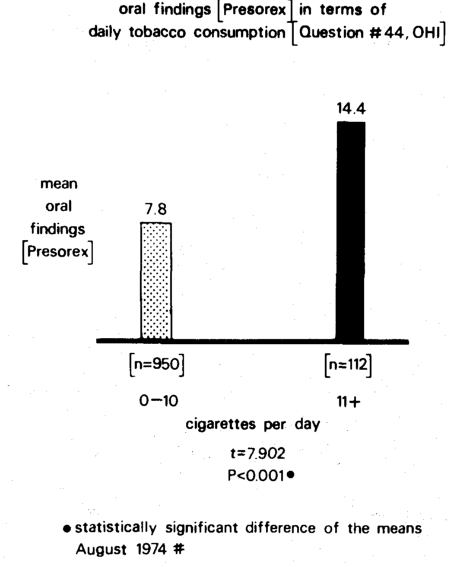
Figure Three. The relationship of daily cigarette consumption (on the horizontal axis) versus mean number of oral symptoms and signs, Presorex (on the vertical axis). The heavier smokers report almost twice as many oral findings.
Since the possibility prevails that the tobacco may not be the only variable, Figure Four pictorially portrays the relationship of tobacco and vitamin C in terms of oral symptoms and signs. The fewest oral findings (7.2 per person) are noted in the group with the lower cigarette intake (0-10 cigarettes daily) and the larger vitamin C intake (>300 mgm. per day). The greatest number of oral findings (15.4 per individual) is associated with the group characterized by the greater cigarette intake (11+ cigarettes per day) and the lower vitamin C intake (<200 mgm.). The other two possibilities occupy intermediate positions in terms of present oral findings.
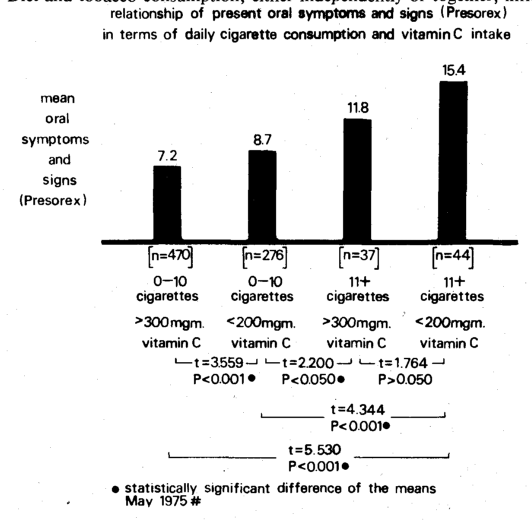
Figure Four. The relationship of current oral symptoms and signs, designated as Presorex (on the ordinate), versus daily tobacco consumption and vitamin C intake (on the abscissa). The group characterized by the lesser tobacco and higher vitamin C intake parallels the least number of oral findings; the group with the greater tobacco intake and lesser vitamin C shows the greatest number of oral symptoms and signs. The other two groups in terms of tobacco and vitamin C occupy intermediate positions.
There seems to be no question but that smokers and nonsmokers eat differently. What is not so clear is why this should be. There is some clinical evidence in the literature to suggest that nonsmokers are more health conscious and, therefore, are more careful of their eating habits.4 There is also some reported material to indicate that tobacco consumption is, in many instances, an attempt to correct a metabolic defect, frequently hypoglycemia.5 When the metabolic imbalance does not exist, then there is no need for tobacco and no need for food consumption intended to correct the low blood sugar syndrome.
One point which appears unquestioned is that there is a relationship between tobacco consumption (as judged by cigarettes) and health and disease (as judged by oral symptoms and signs) utilizing the sphere as the experimental model (Figure Two). It is also clear that the relationship between tobacco intake and oral health and disease becomes more sharply delineated when viewed, additionally, in terms of eating habits, in this instance vitamin C.
Summary
Dietary intake and daily tobacco consumption were assessed in approximately 700 members of the health professions. It was found that, although the diets of both smokers and nonsmokers contained about the same number of calories, there was a great difference in the proportions of nutrients involved in these calories. On a mean basis, for the smoker group, the intake of almost every vitamin, mineral, and amino acid studied was less than for the nonsmoker group and many of the differences were statistically significant. Since many of these nutrients are classified as resistance agents because they decrease the likelihood of disease, the dietary pattern adopted by nonsmokers should be encouraged. The smokers consume more refined carbohydrates than do the nonsmokers; the difference is highly significant statistically. Since refined carbohydrates are classified as susceptibility agents because they enhance the possibility of disease, the dietary pattern adopted by these smokers is to be avoided.
Diet and tobacco consumption, either independently or together, influence health. A poor nutrient intake and smoking are susceptibility factors which diminish health, whereas a good nutrient intake and nonsmoking are resistance factors which promote health.
References Cited:
- Cheraskin, E., Ringsdorf, W.M., Jr., and Clark, J.W., Oral Health Index Questionnaire and Manual, University of Alabama in Birmingham, University Station, Birmingham, Alabama 35294.
- Dietronics, Division of Hanson Research Corporation, Form F-1, Standard Frequency Questionnaire, Post Office Box 35, Northridge, California 91324.
- Cheraskin, E., Ringsdorf, W.M., Jr., Hicks, B.S., and Romano, D.M., “The prevention of oral disease,” J. Internat. Acad. Prev. Med. 2:22-52, 1975.
- Cheraskin, E. and Ringsdorf, W.M., Jr., Predictive medicine: A study in strategy, Mountain View, California, Pacific Press Publishing Association, 1973.
- Cheraskin, E., Ringsdorf, W.M., Jr., and Brecher, A., Psychodietetics: Food as the Key to Emotional Health, New York, New York, Stein and Day Publishers, 1974.