
Access to all articles, new health classes, discounts in our store, and more!
The Dental Aspect of the Relation of Endamoeba to Pyorrhhoea Alveolaris
Published in Surgery, Gynecology and Obstetrics, January 1916, pp. 37-43.
* * *
It gives me great pleasure to bring to this Clinical Congress of Surgeons greetings from the National Dental Association and from its department of research, The Research Institute of the National Dental Association. I wish particularly to express, in behalf of both of those organizations, their deep appreciation for the assistance given in the organizing of the latter by your presiding officer and president, Dr. Charles Mayo, and by Dr. George W. Crile, who is also on this platform, both of whom are officers in the Institute, and others of your members who are in the audience. Our dental profession desires to work in the closest possible coöperation with you on all these common and related problems.
I find on my arrival here that my subject has been changed from “Cinematographic Film Studies, Showing the Movements of Mouth Organisms, Including Endamoebæ,” as previously announced, to “The Dental Aspect of the Relation of Endamoebæ to Pyorrhoea Alveolaris,” owing to the inability of your officers to provide for a motion picture machine to be used in this room, due to a conflicting city ordinance. I assure you that they have done all in their power to accomplish it. For your sakes I regret this, since, by means of the motion picture studies of the infecting organisms of mouth lesions, we can learn much that cannot be presented in any other way. Many of the organisms of the mouth will not grow on artificial media and are readily recognized and studied by their living characteristics, including, in some instances, a changing motility. We would also have been able to show you both a normal end-artery and capillary circulation, and the same while changing, due to the introduction, intravenously, of a small quantity of pathogenic microorganisms which produced a mechanical embolic endartery block with attending cessation of the capillary circulation surrounding it. This cannot be seen in slides, since the moving red blood-corpuscles are very distinctly seen as individuals in their rapid migrations through the capillaries and small blood-vessels.
In discussing the subject assigned, we have to review what will probably prove to be one of the greatest disappointments that will have come to the dental and medical professions and humanity for some time. There are many seemingly very strong arguments in support of the end amoebic etiology of pyorrhoea, but there are probably twice as many seemingly as conclusive arguments against it. Owing to the briefness of the time available, I will only be able to summarize them both. A most remarkable and perhaps significant situation exists, in that while splendid authorities are found supporting each side, nearly all of those of distinction favoring the amoebic theory are bacteriologists and pathologists whose extended experience and training has been largely or entirely in other fields than the mouth, while of the experienced dental pathologists and bacteriologists, of which there are a great number, there are scarcely any who do not find after investigation that their judgment is against the deduction. For example, we have in this country an organization known as the American Academy of Periodontology, which is made up exclusively of specialists who are doing practically nothing else but studying and treating this disease, and at their meeting held just a month ago in Detroit it developed that all had been observing very critically, and but few, if any, cases of pyorrhoea alveolaris could be reported as cured or controlled after having been treated with emetin when those cases were judged by the standards that long experience has thought to be adequate, and by which exacting standards probably every person present could include as controlled if not cured many cases treated by other known efficient means. Experienced dental pathologists, however, greatly dislike to use that word “cured” and rarely do so. The use of the word is a bad sign. We have many skilled specialists who have been studying this disease intensively and almost exclusively for ten, twenty, and thirty years, and its special pathology is so well understood by them that the hastily made deductions of those without that experience reveal to them, in paragraph after paragraph, ample reason to account for the difference in conclusions. In view of the fact that a very great harm can be done by the expounding of a mistaken deduction, it is always a tragedy when the best established data is not used as a check. Many well established principles of dental pathology have been entirely overlooked in the theoretical explanation of the etiology of pyorrhoea alveolaris to provide for the role of amoeba. It is particularly to be regretted that boards of health have accepted as established a matter of so far reaching importance on so little evidence.
Probably the strongest argument in favor of the endamoebic etiology of pyorrhoea has been found in the fact that endamoebæ are generally found in pyorrhoea pockets, when there is a profuse flow of pus and, since emetine is almost a specific for the so-called amoebic dysentery, emetin should cure pyorrhoea. The clinical evidence gave some support to this deduction since the administration of emetin in many cases reduces the total quantity of pus flow and the relative number of endamoebæ. This seems like a plausible deduction, particularly so if we measure pyorrhoea disease and its cure by the presence or non-presence of pus and especially in the absence of evidence to show that the beneficial effect of emetin is accounted for by its action on other organisms, directly or indirectly, or that endamoeba are not pathogenic. It is probable that at this point there has been the greatest difference in the viewpoint of the dental and medical students of the condition. The trained dental pathologist looks upon the presence of the pus or the reduction of its flow as quite incidental to the establishment of a cured condition. Our specialists have known for years of different methods for producing this change in the symptoms.
In addition to the special studies that have been made by the Research Department of the National Dental Association to establish the role of amoeba and emetin, this department has also worked in coöperation with selected men in practically every state in the Union, and some from other countries. These men have furnished smears under uniform direction and have provided data. This information establishes that amoebic infection was very universal at the time these slides were made; namely, in February and March of this year; that the use of emetin locally and by injection in many cases temporarily modified the pus flow. A few claim considerable improvement but from the standpoint of pathological repair, the conditions are not what we could recognize as a cure. A few made very extravagant claims after an exceedingly short use of the drug. While the name pyorrhoea alveolaris assumes the presence of macroscopic pus, many of the worst cases of pyorrhoea alveolaris have no visible pus, though they do show it microscopically. Our studies, extending over more than one year of quite critical observation, indicate strongly that the demonstrable presence of endamæbæ is not a constant factor in Cleveland for certain typical cases. The number of this organism present in a given case, varies, through a wide range, at different periods. In general these organisms are much more prevalent in warm weather than in cold. Certain typical cases without much pus present were studied during November, December, and January, a year ago, and, although large numbers of slides were made, the organisms were not often found, nor were they in many mouths without pyorrhotic lesions. At certain periods in January and February, and with an increasing frequency toward spring, the endamoebæ appeared in these mouths, and with the approach of warm weather were constantly present; and also in a large percentage of patients who were free from pyorrhotic lesions. Some of these patients had emetin administered and, notwithstanding this fact, showed these protozoa in large numbers after the treatment, though they could not be demonstrated by the same or any used methods before the treatment. This was not because of the emetin but in spite of it. During this autumn the same condition of varying presence of the organisms in the same mouths has been found on certain days. At certain times practically all patients, whether suffering from pyorrhoea or not, may have the organism and a week later it may be absent in a majority of these mouths. It is very significant that the severity of the pyorrhotic lesion does not show any appreciable change in these same mouths, whether the organisms are present in abundance or so scarce that they are not found. We have kept a rather careful record of this condition and checked it against the mean temperature. At A and B in January (Fig. 4) the organisms were found in the motile state in pyorrhotic lesions in which they could not be demonstrated on any other days during that month in those mouths. These patients were not examined every day but two or three times a week. It will be noted that just prior to their appearance on January 4 and 5, there was a sudden rise in temperature from 20° to 50° F. and a less extreme change preceded their presence at B on January 19 and 20. In each, February 1 to 3, 8 to 10, and 21 to 24 they were again found in abundance in these same mouths but disappeared in the interims. During March and April the mean temperature was quite constantly on the rise and they were found in these same mouths on every occasion examined. During April, May, and June they were found in almost every mouth of the small children, even those without traces of pyorrhotic lesions, as well as in adults without this disease, almost as universally as in mouths with pyorrhoea. During this late autumn they have disappeared again from these same mouths so that very few people without pyorrhoea have the organisms demonstrable, and in many of those with severe cases of pyorrhoea they frequently cannot be demonstrated. If endamoebæ are the etiological cause of pyorrhoea, why does not the severity of the attack vary with their presence? It should be stated in this connection that careful observations have been made on all these cases to ascertain if the mouth flora varied at the same time the endamœbæ did, and it could not be seen that there was any variation in their numbers or variety.
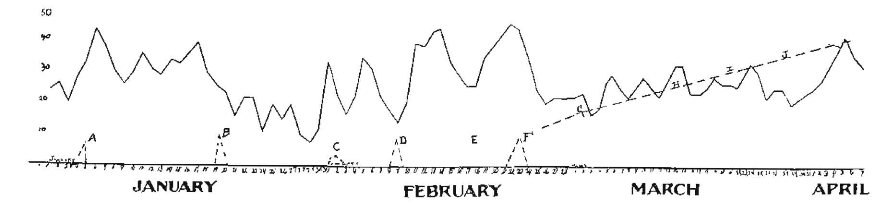
Fig. 4.
It seems to be certainly demonstrable that emetin has a definite beneficial effect on certain cases of pyorrhoea, expressing itself not only in the lessening of the number of endamoebæ and total pus flow but also in the tone of the gingival tissues surrounding the pockets. There is, however, an additional improvement in these cases, which has not, so far as we know, been reported except by ourselves; namely, a lessening of the relative number of microorganisms in the pockets. This is not true of all cases and in those in which it does exist the effect is seen whether the emetin is injected directly into the pyorrhoea pockets, subcutaneously or intravenously. It is not probable that this is due to a germicidal action of the emetin, for the dilution is too great when injected elsewhere in the body. Its action is strongly suggested, however, by an immediate change in the phagocytes found in the contents of the pyorrhoea pocket, for these undoubtedly form one of nature’s chief defenses against the majority of the mouth microorganisms. We are not certain what the mechanism is, though it seems to be an increase in the stickiness or adhesive property of the surface of the phagocytes, for in these cases after the use of emetin they, the phagocytes, will be found to contain much larger numbers of microorganisms. We have this beautifully illustrated in motion pictures where the contents of the pyorrhoea pocket have been prepared with the same technique before and after treatment and the change both in the number of microorganisms and phagocytosis is very marked. This, however, becomes a strong argument against the endamoebic etiology of pyorrhoea, since it has never been suggested that they are destroyed by a process of phagocytosis, and does account for the beneficial effect of emetin without assigning the result to its amoebicidal action. We believe that on this basis we will find that we are greatly indebted to Drs. Barrett and Smith for the suggestion of this drug, not so much because of its own beneficial effect and usefulness, as because of the confidence it should give us all to search further and find other specifics that will, in a similar or comparable manner, greatly benefit these cases. Indeed, there is strong evidence that such an agent will be found, if one has not already been found, in succinimid of mercury, for the introduction of which we are indebted to Drs. Wright and White. They claim practically 100 per cent “cures.” We have been making studies with this drug and, while we have not had the successes claimed by the gentlemen suggesting it, we believe it to be superior to emetin in a majority of cases. We find, however, that the criticisms that we have made in the beginning of this address, relative to the standards by which pyorrhoea is declared to be “cured,” are applicable here, for the chief change in the lesion is the quantity of pus. Greater care must be taken in using the doing because of the susceptibility of many patients and consequent danger of mercury poisoning, which shows itself probably more quickly in the structures with which we are dealing than in any other tissues of the body. Has it occurred to you why this is so? Is it not true that it is the practice of every man in this room to look at his patients’ gums when he suspects mercury or lead, etc., poisoning? Why do you do so? It is because of the abnormal susceptibility of these tissues to systemic irritation. The alveolus is, by its nature, being an end-organ, a transient tissue. It does not exist in either babyhood or old age, and, like the hair, the system tends to dispense with it at the approach of very early signs of decadence.
Another argument against the amoebic etiology of pyorrhoea is found in the clinical picture which is familiar perhaps quite exclusively to those who are devoting themselves to an intensive study and clinical treatment of pyorrhoea alveolaris. It is variously spoken of as a bacteriæmia or toxæmia following the procedure of instrumentation for mechanically removing the deposits from about the necks of teeth and within pyorrhoea pockets. It not infrequently occurs that the reaction upon the patient will be so great that there will not only be great local soreness of all the teeth as a result of the procedure but a rise of temperature often accompanied with considerable prostration. This occasionally will put the patient in bed and will last for a day or two. It is not demonstrated what the mechanism of this reaction is. There is strong evidence, however, that the temporary disturbance of nature’s defense in the soft tissues permits of the entrance into the circulation and lymph stream of motile organisms. The endamoeba that is considered responsible for this lesion is designated as the endamoeba gingivalis, Gros, by Drs. Barrett and Smith, or endamaeba buccalis by Drs. Bass and Johns, probably the same organism. Had we been able to use the motion pictures you would have seen readily that this organism has a very slight power or tendency to project itself across the field. It throws out lobose pseudopods first in one direction and then in another, usually with the tendency to a rhythmic flow of the pseudopodic wave in consecutively circular order (see Fig. 1).
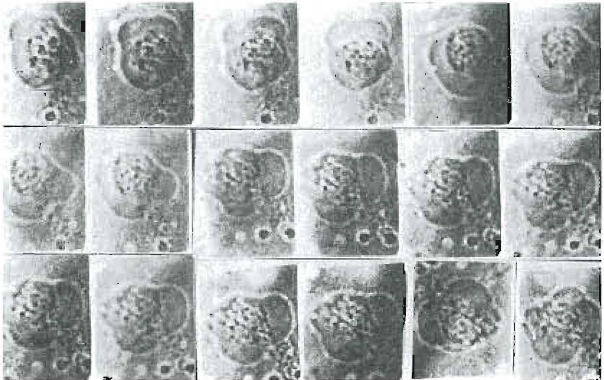
Fig. 1.
Unlike the kartilusi variety (Fig. 2), which is the species of endamæba found in many cases of pyorrhoea, it seldom migrates longitudinally. This latter species migrates quite rapidly and continuously in the same direction and could be conceived of as entering more freely into the tissues surrounding the pockets. An argument for the amoebic etiology has been that while other organisms may be the active cause, the endamoeba buccalis, by its migration over the granulations, drags the infecting bacteria on to and into the tissues and thus effectually plants them. If we could see the various organisms in the pyorrhoea pocket in the motion pictures, we would see that many of them can swim circles around the amoebæ like butterflies playing around a turtle, and except for the non-motile varieties there seems little occasion to provide such a slow means of transportation.
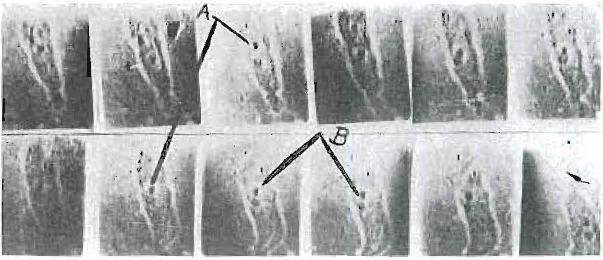
Fig. 2.
If we were to provide a rapid carrier for the microörganisms, we would find it in the ciliated protozoan shown in Fig. 3. This is only found in a small per cent of the pyorrhoea pockets but it has migration speed probably one hundred times greater than even the kartilusi variety. It is about the size of a leukocyte, is a ciliated protozoan and tends to keep under the debris. The relative motility of these two species of endamoeba and this ciliated protozoan can be seen in the illustrations. In the first two the motion pictures were taken at the rate of sixteen per second and only every seventh picture is shown here so that the change between one picture and the next, in Figs. 1 and 2, are at about one-half second intervals reading from left to right and from top downward. Figure 2 shows clearly the successive sequence of pseudopodic action. The relative size as compared with an erythrocyte is shown by the dark objects just above the endamoeba buccalis. In Fig. 2 of the kartulisi the organism is seen to migrate about one-half its own length in a little over six seconds. Of course, these are pictures of living organisms, not of stained specimens. In Fig. 3 the motion picture camera was run at the rate of twenty pictures per second and none were cut out so that the twelve pictures shown represent about one-half a second instead of six seconds as in Fig. 2. It will be observed that this ciliated protozoan has moved practically across the field in this half second.
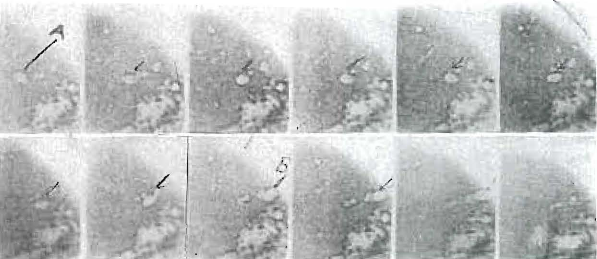
Fig. 3.
The progressive pathological stages of pyorrhotic lesions indicate very definitely that one of the most, if not the most, important factors is inherent in the tissue itself. There is not time to discuss this at length but we will call your attention to one of these factors; namely, that these lesions progress continually toward the apex of the root and but slightly laterally. It is difficult to account for this phenomenon as a purely infective process. Again this progressive destruction can be started at will in practically any mouth by the placing of almost any possible irritant against the gingival tissue in such a position as to either displace it or hold bacterial masses in contact with it. If it were a simple infective process, why does not the placing of such an irritant, as suppose an impinging bridge making pressure on the alveolar side at a point distant from either of the supporting teeth, produce a typical lesion. It will produce an irritation of the mucous membrane from which there may even be a systemic invasion, but there is not the progressive destruction of the alveolar bone, as develops when this irritant is placed in the same relation to the pericemental tissue. An important factor is, therefore, to be found in the structures immediately surrounding the roots of the teeth. This limitation will, of course, apply to all organisms that may be related to the lesion, unless they can be shown to have a specific liking for some element in the pericemental tissue. Black and other histologists have reported at length on the existence in the pericemental membrane of chains, strings and clusters of epithelial cells which run parallel with the long axis of the root and are possibly related to the formative enamel organ. Black considers them normal to the location because they are always present in both man and the higher animals.
We are strongly of the opinion that when the true etiology of pyorrhoea is understood, it will be found that some of the microorganisms of the mouth which do not grow on artificial media and which, consequently, are, as yet, slightly understood, will be found to play a much more important role than do endamoebæ. In fact, we believe we have found one which we can readily recognize with the motion pictures, which refuses to grow in any artificial media that we have found that does not contain blood, preferably the blood from the patient from whom it was obtained, and is killed by blood of other patients and of certain animals. The presence of the irritating substance, whether a deposit of tartar, an ill-fitting crown or filling, a mass of food or a mass of bacterial detritus, will be sufficient to call out from the tissue the elements of the blood stream necessary for developing their special and acquired appetite. The removal of the irritant immediately robs them of the intermediate means for providing this special food. There is indication that the progress of this disease toward the tooth apex is related to these chains or threads of epithelial cells which exist in the pericemental tissue. After they, with their symbionts, have destroyed the pericemental tissue opening up the minute alveoli or bone-cells of the alveolar bone, the latter become ideal fields for streptococcal infections, which are planted directly from the mouth. In these protected areas of varied oxygen tension, the various strains of streptococci are developed, which select out with great regularity certain tissues of the body which they reach through the blood stream, and which they infect by embolic processes. We see no more reason based on the evidence already submitted for claiming that endamoeba are the chief etiological factors in pyorrhoea than for blaming it upon any one of several other mouth microörganisms which, like the endamoeba buccalis, will not grow on any artificial media that we yet know of, and which organisms are as constantly present in the pyorrhoea pockets as are this protozoan. It is our belief that not until we know very much of these but little understood organisms will we have solved the problem as to what the real etiology of pyorrhoea alveolaris is.
In the meantime it seems to be our duty to withhold judgment and recognize that it has not been demonstrated that any one organism is the chief etiological factor in pyorrhoea alveolaris. The evidence in favor of assigning it to endamoeba gingivitis or buccalis is, we believe, entirely circumstantial. More definite evidence must be established before we can say that it is, or that it is not, the cause. Typical lesions can be artificially produced without its presence. If this should be accomplished with this organism as the chief agent, it will quite quickly establish it as an important factor. Drs. Barrett and Smith are of the opinion that the evidence does not justify the differentiations between the various varieties of endamoeba, including the hystolitica. The most certain phase of this pyorrhoea problem seems to be that more exhaustive research is imperatively demanded in the interests of humanity, who are paying and will continue to pay such a terrible price so long as our two professions remain in ignorance as to the true facts underlying its etiology, cure, and prevention.
References:
- Hartzell and Henrici. J. Nat. Dental Ass., ii, 2; Report Minn. Div. Nat. Dental Research Commission, ibid., p. 4.
- Price and Bensing. J. Nat. Dental Ass., ii, 2.
- Wright and White. Dental Cosmos, lvii, 779; Wright, ibid, 1003.
- Bass and Johns. Dental Cosmos, lvii, 102, 460, 1299.
- Barrett and Smith. Dental Cosmos, Ivii, 101, 1201; J. of Parasitol., i, No. 4, 159.