
Access to all articles, new health classes, discounts in our store, and more!
The Cause of the Various Clinical Manifestations in Pulmonary Tuberculosis
Presented to the American College of Physicians, at the Annual Clinical Session, New Orleans, March 6, 1928. Published in the Annals of Internal Medicine, Vol. II, No. 1, July 1928, pp. 1-20.
* * *
Adult tuberculosis is a chronic disease whose clinical picture usually is made up of alternating periods of quiescence and activity. The symptoms vary according to the type and the particular state of the disease at the time of consideration. There are certain symptoms which belong almost exclusively to periods of activity, others to periods of quiescence, and still others to periods of both quiescence and activity. The disappearance of the common symptoms does not indicate that healing has been accomplished, or even that the disease is quiescent.
Most symptoms of ill health are due to altered physiologic reaction, a disturbance in the reflex arc according to Mackenzie; consequently the symptom complex of any disease will vary in different patients as their individual physiologic equilibriums vary, and, in the same patient at different times, according to the particular physiologic balance or imbalance which he happens to exhibit at the time. Difference in symptomatology is also affected by differences in virulence and in the numbers of bacilli which cause different infections.
Since the character of the disease in chronic tuberculosis depends upon the specific tissue reaction, the immunity mechanism, developed by the patient, and since this in turn depends upon certain variables on the part of both the patient and the infecting microorganisms as just mentioned, the disease picture must necessarily present many different types of reaction; and variability must be the rule.
Primary Infection Versus Reinoculation
When an infection takes place as a result of bacilli making a place for themselves in the tissues of a host, the course which it takes and the nature and severity of the symptoms which it presents will differ according to whether or not it is the first time that such implantation has occurred.
If it is the first inoculation, no immediate symptoms will appear. Symptoms do not appear until the incubation period has ended with the bacilli definitely implanted in the tissues, and the host’s immunizing mechanism called into play. This period varies from a few days to a few weeks according to the numbers and virulence of infecting bacilli and the general physiologic state of the patient. On the other hand, if it is a reinoculation, symptoms may appear almost immediately. Usually within from six to forty-eight hours after the bacilli have found lodgment in the tissues a marked reaction on the part of the host, accompanied by symptoms, takes place.
This difference in the manner in which an individual reacts to primary inoculation and reinoculation is due to the difference in defense under the two circumstances. In the former, it is the host’s virgin reaction to bacilli and is practically void of inflammatory characteristics. In the latter, on the other hand, it is a specific immunizing response, a heightened reaction, brought about by the hypersensitivity of the body cells to tubercle bacilli and bacillary products which has been brought about by previous infection. This is primarily inflammatory and exudative in character.
There are certain exceptions to these reactions which must be looked upon as the usual reaction of the tissues to tubercle bacilli, that must be borne in mind. Bartel recovered living bacilli from the lymphatic glands of a guinea pig months after inoculation which had not produced tubercle. Opie1 has shown that when latent apical lesions are present pulmonary tissue which shows no evidence of disease contains recoverable viable tubercle bacilli. Why bacilli should at times fail to be opposed by the usual tissue reactions is not clear.
Allergy
The change in response on the part of the body cells toward a reinoculation of bacilli has come to be known as “allergy.” Allergy is established by the primary inoculation and may be increased by repeated subsequent inoculations, provided the numbers and virulence of the bacilli engaged in the infection are not too great for the individual’s resisting power. It is greatest after the host has had several successive mild inoculations or after he has successfully withstood a severe infection. It is not only depressed by very severe infections but sometimes lowered almost to the vanishing point. It is lowered by various stresses, and particularly unfavorably influenced by such diseases as influenza, measles and scarlet fever; likewise by pregnancy. During the conditions mentioned the power of the skin to react to tuberculin lessens and sometimes disappears completely.
The severity of symptoms produced by a certain reinoculation dose of bacilli will vary according to the degree of allergy present. The more marked the allergy the greater the reaction. A strong allergic reaction indicates a stable physiologic balance on the part of the host and a defensive mechanism which should be competent to combat ordinary invasions.
The effect of the allergic reaction is manifested in several ways. First, a reaction comes on very quickly in bodies in which allergy has been established slowly in primary inoculation; second, it takes more bacilli to produce infection after allergy has been established than before; third, if a marked allergic reaction is present it is often able to prevent implantations trom taking place, or, failing this, to cause them to become abortive in character; fourth, the passage of bacilli through the tissues is retarded or prevented by the allergic reaction, hence the danger of spread of infection is lessened; and, fifth, the inflammatory reaction, unless too severe, promotes healing by stimulating the reticulum in the tissues which are the seat of tubercle infection so that it increases in amount and forms fibrous tissue. Even the severe allergic response with its exudative reaction, which is at times followed by caseation and necrosis, can not be looked upon as wholly harmful. The exudate resolves like that of a pneumonia, though taking weeks and months instead of days; and the reticulum in the walls of the air cells and in the small blood vessels increases in amount, growing inward into the air cells and replacing inflammatory products, even caseous material. And when caseation and necrosis have taken place bacilli are often cast off in numbers such as would be dangerous to the life of the host if he had not gotten rid of them. Even the exudative reaction, serious as it sometimes is, serves as a barrier to prevent the escape of bacilli into new tissues with a consequent reinoculation.
The allergic reaction is such an intimate part of clinical tuberculosis that we can not think of them apart. While allergy is primarily defensive, its manifestations at times become so injurious that its protective nature is for the time being almost completely overshadowed. Nevertheless, if one will examine advanced tuberculous lesions carefully, in which the exudative characteristics preponderate, he will note that there are two processes which go hand in hand, the one destructive, the other conservative; and, that, while caseation and destruction may predominate in the center of tuberculous masses, the formation of fibrous tissue is going on in the periphery, and even predominates in some areas.
The character of the lesion is determined, not by the presence of an exclusively destructive or an exclusively proliferative process, but by the predominance of one or the other.
While the allergic reaction is inflammatory in character, the degree of inflammation differs greatly under different circumstances. It may be so slight that it consists only of a mild hyperemia, or it may be so severe that the affected tissues are the seat of a severe serous, fibrinous, and cellular exudate as described so well by Krause.2
In order to understand the various manifestations of allergy as they are met in the course of clinical tuberculosis, it is necessary to know that allergy is a property possessed by the body cells generally, that it is possessed most strongly by the cells which make up the tubercle, and that the allergic reaction, either local, focal or general, may be called out by the presence of the tubercle bacillus itself–either living or dead–or by certain products which are produced by or from bacilli.
Exudative and Proliferative, Not Different Types of Tuberculosis but Different Degrees of Allergic Reaction
From the discussion of allergy it is plain to be seen that Aschoff’s exudative tuberculosis is not a distinct type but only the pathological manifest ratio of a severe allergic reaction in which an extensive exudation of serum, fibrin and cells takes place in the tissues. Neither is the proliferative a distinct type. It is likewise a manifestation of allergy, but of a mild degree in which only hyperemia, or hyperemia with an exudation of small amounts of serum and cells takes place. Allergy is responsible for any degree of reaction from the mildest hyperemia followed by proliferation of fixed cells to the severest exudation of serum, fibrin and cells, with resultant necrosis of tissue. The reaction is in all probability commensurate with the ability of the tissues of the host to respond to the demands made upon it by the invading bacilli. The greater the demands, unless they be so great that they overcome the patients’ immunity mechanism, the greater the allergic response and the more serious the pathologic changes. Yet if we know this is primarily a picture of defense rather than destruction, even though the latter may follow, we have a different and more hopeful attitude toward these more severe phases of active tuberculosis. They are not serious unless they overcome the ability of the cells to react further in protection of the host. Exudations are acted upon by digestive enzymes and the products carried off as they are in pneumonia, and proliferation of the reticulum in the tubercles takes place producing scar. Even in serious exudative reactions, fibrosis is taking place in the periphery of the lesions and extending centralward where it may even replace necrotic tissue.
Allergic Reaction Differs at Point of Reinoculation and in Other Foci in Body
The fact that there is a difference in the allergic reaction which takes place in the focus of disease where many bacilli are producing massive doses of antigen, and in other foci which are distant from the seat of active antigen production because they are stimulated only by small doses, must be accountable for the difference in severity which is noted in the allergic reaction seen in clinical tuberculosis in different areas and at different times.
This affords the basis for two different ways in which the allergic reaction may manifest itself in the course of tuberculosis. In all cases of reinoculation the bacilli settle in tissues which are hypersensitive or allergic and which react immediately, feebly or markedly as the case may be, in an attempt to prevent implantation from taking place. In instances where the immunizing mechanism is competent permanent infection may be prevented, and even where complete protection fails the bacilli may be hemmed in and held to a localized infection.
The presence of living bacilli in any considerable numbers, whether followed by successful implantation or not, calls out a local allergic inflammatory reaction which persists over a greater or lesser period of time, producing a definite syndrome of active disease. It does more than this, however. Certain bacillary substances escape from the foci of disease and gain access to the blood-stream, scattering throughout the body. Wherever they come in contact with unhealed foci they may call forth an allergic response, slight or severe in character, depending on conditions present, which, while similar to that at the seat of reinoculation, yet differs in certain very important features.
In the first place it is called forth by bacillary substances which have been so diluted in the blood-stream that the focal reaction called forth by them is slight compared to that at the seat of the reinoculation where the allergic producing substances are found in large quantities. As a result the reaction in the centers of the areas of reinoculation are apt to be much more severe than those produced secondarily in unhealed lesions found elsewhere in the body. This is a very important fact to be considered in judging of the seriousness of a given allergic inflammatory reaction.
In the first place, there are two processes which go on as a regular thing in tubercle at the same time–necrosis in the center and fibrosis at the periphery–both of which seem to be influenced by bacillary products, although fibrosis is found regularly and necrosis at times as a part of the tissue reaction to minute foreign bodies. The fact that particulate matter of any kind may be associated with necrosis of the central portion of the reacting tissue mass surrounding it indicates that toxins are not necessary to its production, but does not prove that they are not a factor in the necrosis of tuberculosis; on the other hand, the argument seems to point strongly to the toxins, as being the cause of the rapid necrosis in primary tubercle. Fibrosis is favored by the stimulation which affects the periphery of the tubercle. The local reticulum increases in quantity and even spreads inward into the caseous masses at times replacing the necrotic elements.
We can now understand in part the continuous interplay which takes place between bacilli and body cells during the course of clinical tuberculosis and can see that the most potent factors in determining the character of the disease following any infection are the numbers and virulence of the bacilli which cause it.
Symptoms Of Pulmonary Tuberculosis
The symptomatology in any case of pulmonary tuberculosis will depend primarily upon the number of organisms engaged in the process and upon the state of resistance of the patient at the time. The greater the numbers of bacilli in any given instance the more extensive the infection and the more severe the symptoms. When the disease is markedly active there are usually present some toxic symptoms, some of a reflex nature, and one or more of the local symptoms as shown in Table I. The cause of the symptoms is the allergic inflammatory reaction and its effect in: (1) discharging toxins into the circulation, probably both bacillary and from broken down pulmonary tissue; (2) stimulating the afferent sympathetic and vagus nerves in the lung and starting impulses centralward which end in reflex action; and, (3) causing local irritation of the tissues at the seat of the lesion.
Table I – Etiological Classification of Symptoms of Pulmonary Tuberculosis
|
Group I: Symptoms due to toxemia and other causes acting generally |
Group II:
Symptoms due to reflex cause |
Group III: Symptoms due to the tuberculosis process per se |
| *Malaise
*Lack of endurance *Loss of strength *Nerve instability *Digestive disturbances (hypomotility and hyposecretion) *Metabolic disturbances resulting in loss of weight *Increased pulse rate *Night sweats *Temperature *Blood changes |
*Hoarseness
*Tickling in larynx *Cough *Digestive disturbances (hyper motility and hypersecretion) which may result in loss of weight *Circulatory disturbances *Chest and shoulder pains *Flushing of face *Spasm of muscles of shoulder girdle *Diminished motion of affected side
|
*Frequent and protracted colds (tuberculous bronchitis)
*Spitting of blood *Pleurisy (tuberculosis of pleura) *Sputum
|
We may best be able to illustrate the relationship between the reinoculations which take place in clinical pulmonary tuberculosis and the allergic reaction called forth by them, and its influence in the production of symptoms, by analyzing a few chosen cases representing different phases of clinical activity.
Early Clinical Tuberculosis
Early clinical tuberculosis in the adult usually begins in one of three ways, pathologically: either as a reactivation of an old focus, or as a metastatic extension from a previous focus, or as a new infection from without. Sometimes reactivation in previously existing foci comes on quite suddenly as for example following acute respiratory disease such as influenza, pneumonia or bronchitis; but it also may come on slowly after severe stresses of a physical, nervous or emotional nature.
The plate shown in Fig. I is illustrative of early clinical activity in which metastases took place from a previous focus. The patient, Miss E. K., was examined June 17, 1927. One month preceding examination patient had what she thought was a cold followed by fatigue, loss of weight (5 or 6 lbs.) and general feeling of low vigor. Symptoms disappeared in a few days and she regained, but on June 16 spat up one or two drams of bright blood. Physical examination revealed an active lesion at right apex, where there was roughened breathing with few râles.
This reaction probably meant the breaking down of the fibrous wall which confined viable bacilli; the escape of bacilli to new tissue; the establishment of new foci, and an allergic reaction which resulted in recognizable symptoms and signs on physical examination, and which showed as an exudative reaction in the x-ray film.
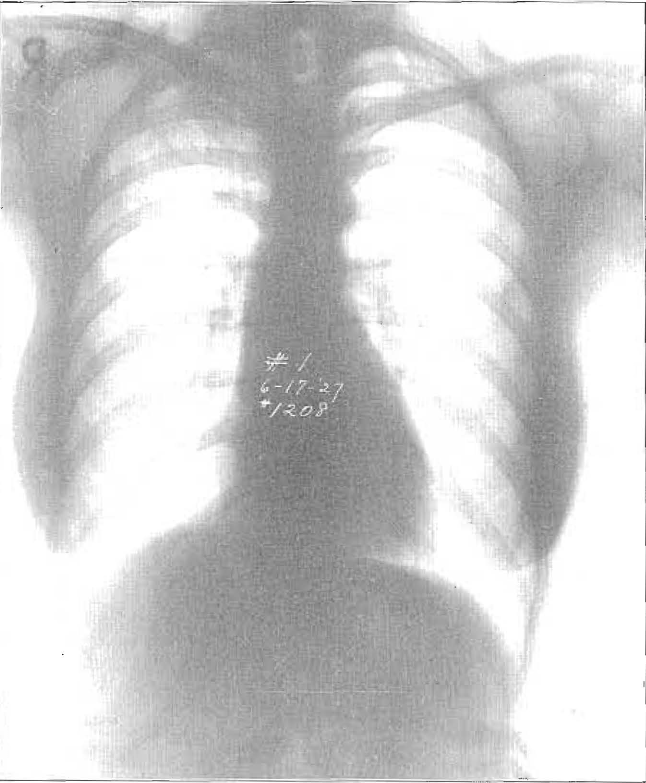
Fig. 1. Illustrating an early clinical activity in which metastasis took place from a previous focus. The allergic reaction which took place at the time of the metastasis one month before has disappeared.
This patient had been examined by me two years previously, at which time there was evidence of an old lesion at the right apex, with no activity.
The temperature curve of this patient remained normal, after she was put at rest, during the entire course of her disease. No subsequent reinoculation sufficiently large to produce symptoms took place after the early metastases and the hemoptysis of June 16. The infiltration in the lung gradually disappeared; the signs on physical examination decreased and the exudative process in the film gave way to fibrosis. This case illustrates the dependence of symptoms on the allergic reaction produced by reinoculation and shows how, when that has disappeared, the early symptoms may soon pass away and leave the patient in a state of false security. Had this patient not heeded this early warning but kept on working, the chances are at least even that the infection would have progressed.
Advanced Clinical Tuberculosis
Tuberculosis advances by forming metastases. No patient ever dies of his original infection unless it be such as a miliary spread or a meningeal invasion. It is only when repeated reinoculations, caused by many bacilli, have taken place, and the destructive reactions have predominated over the proliferative that death ensues.
Sometimes repeated reinoculations will take place before a real destructive disease is established. Even widespread exudative lesions are not inconsistent with healing.
Mrs. E. J. illustrates this fact. She entered the sanatorium Nov. 23, 1925, with the following history. Poor health for two years. Main symptom, indigestion. In June of 1925 severe “cold” followed by fatigue, loss of voice, loss of strength and weight (7 lbs.), cough and expectoration. In August, left-sided pleurisy and flushing of the face each evening. Had previously had several periods of elevation of temperature. At time of entering sanatorium, temperature was between 99 and 100°, but under rest came to normal within first month and remained so for the most part until healing was completed. The signs of activity gradually disappeared. The toxic symptoms disappeared first: the reflex symptoms remained longer, some until healing was complete.
The plate in Fig. 2 shows a widespread exudative lesion with little loss of tissue. The plate in Fig. 3. taken two years later, shows how such a lesion, when not followed by repeated large reinoculations, may go on to absorption of the exudate and healing. The healing in this case was brought about in part by resolution, the exudate revolving the same as in pneumonia, only taking months instead of weeks for the accomplishment; in part by the formation of fibrous tissue, and in part by calcification, as is seen in both apices.
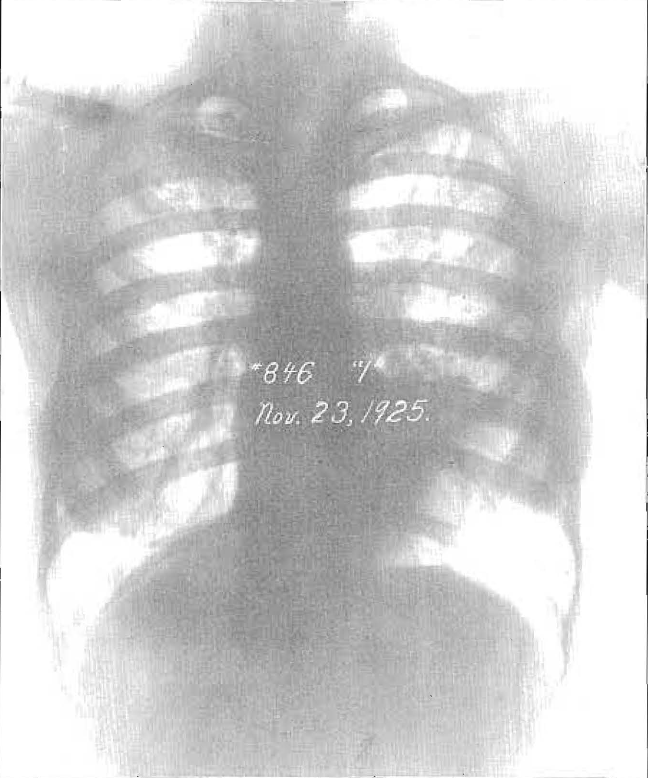
Fig. 2. Widespread allergic so-called exudative type of Aschoff, with Iittle loss of tissue.
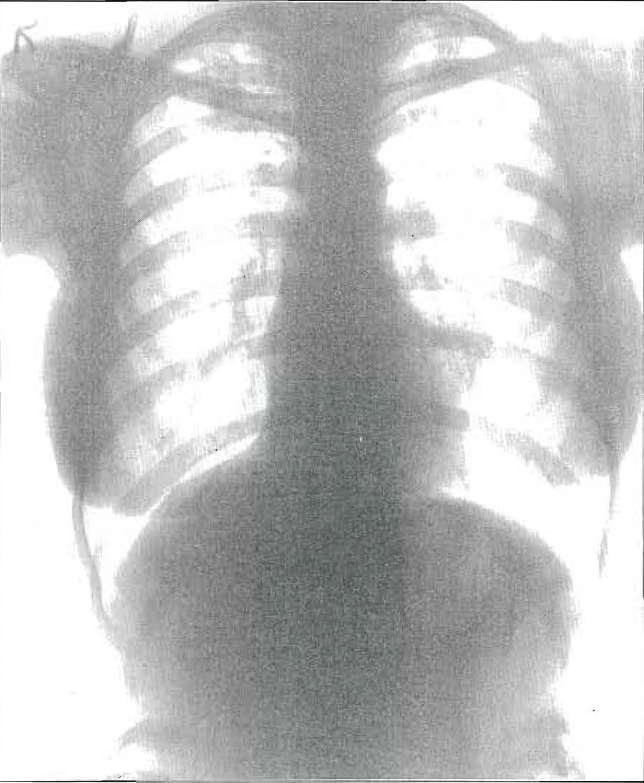
Fig. 3. Same chest as shown in Fig. 2, taken two years later. The exudation has disappeared, healing having taken place largely by resolution.
Sometimes a process becomes very acute from the beginning. This is illustrated by the following history. Mr. G. L. B. was examined on Jan. 5, 1924, at which time he was recovering from influenza. Chest showed slight evidence of old tuberculous process at both apices, without activity. X-ray revealed a calcified node on a level with the first rib, posteriorly; also few calcified nodes in hilum; no active tuberculosis, as shown in Fig. 4.
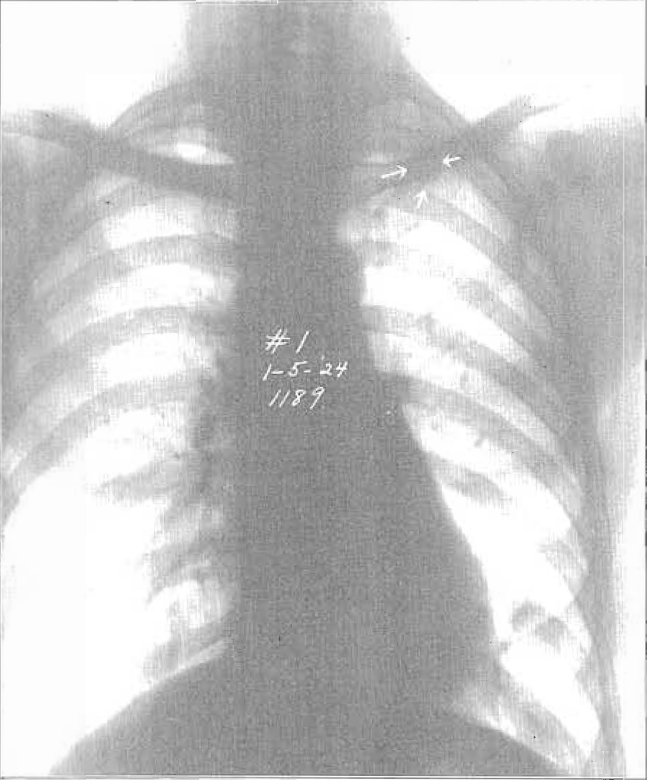
Fig. 4. Plate of a chest showing calcified nodule in the upper portion of the left lung.
Patient again presented for examination Nov. 8, 1927, giving a history of feeling ill during preceding few weeks, with languor, rise of temperature to 103°, loss of weight, severe cough, and free expectoration (20 cc in 24 hours, with 25 bacilli per field).
Physical examination showed cavity at left apex and considerable infiltration throughout the upper lobe, with numerous moist râles. The X-ray plate, Fig. 5, shows that the calcified node seen in Fig. 4 had been replaced by a cavity, and that a marked spreading had taken place throughout the entire upper lobe. Such a rapid spread, taking place before a competent immunity has been established furnishes the condition for a rapidly fatal tuberculosis.
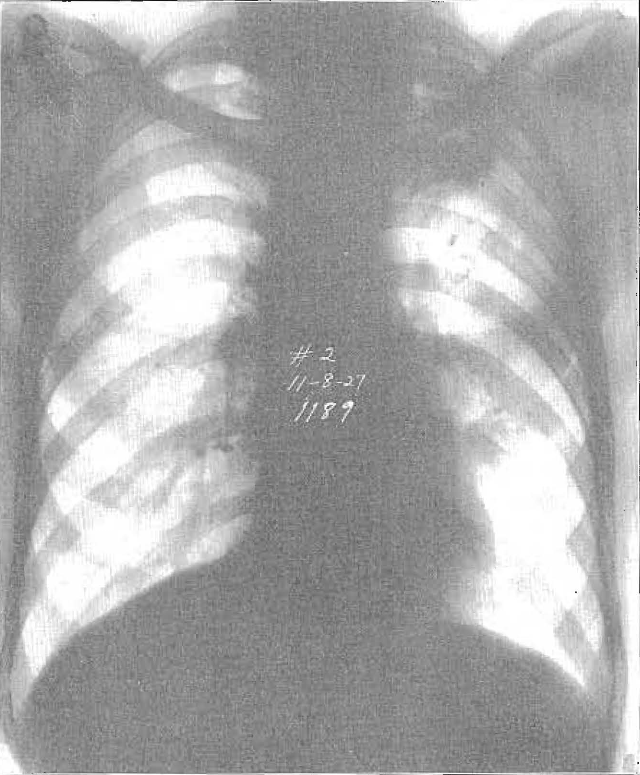
Fig. 5. Same chest four years later. Reactivation in area surrounding the calcified node, with cavity formation and general spread to neighboring tissue.
Ater the disease is once well established its course may be either progressive or regressive. Which the course shall be, is determined by the frequency with which bacilli escape from existing foci, their numbers and virulence and the degree of competence of the immunizing mechanism at the time the spread takes place. Competency in this connection is only a relative term. What would be competent for the withstanding of one reinoculation would not be for another.
We assume that in case of advanced progressive tuberculosis there is always an unprotected front from which bacilli sally forth more or less constantly. The more extensive the areas of activity the greater the opportunity for them to escape in large numbers. When they escape they call out an allergic reaction which, if severe, is not only inflammatory but exudative in type. This acts as a barrier to their further escape and so proves to be one of the chief methods of defense against a more extensive bacillary invasion. So while exudative lesions are correctly interpreted as being signs of activity, they are also very important barriers of defense for the organism against further bacillary spread.
Miss D. S. had been suffering from chronic tuberculosis for a period of several months. Had had repeated periods of high temperature (101 and 102°) for two or three weeks at a time. then dropping down to nearly normal at which time she would recover much lost ground. On Feb. 9, a moderate reinoculation took place, and on the 15th, before the effects of this one had disappeared, a second very severe reinoculation occurred, as shown in the chart, Fig. 6. As a result of these reinoculations a severe allergic reaction of the exudative type took place. Auscultation showed many râles throughout the entire right and part of the left lung. The patient’s temperature ranged from 102 to 104° for one week and then remained in the neighborhood of 102° for a month. The patient was severely toxic; appetite failed; lost weight; cough was severe; sputum increased from 40 cc in 24 hours Feb. 1. to 140 cc in 24 hours, Mar. 14.
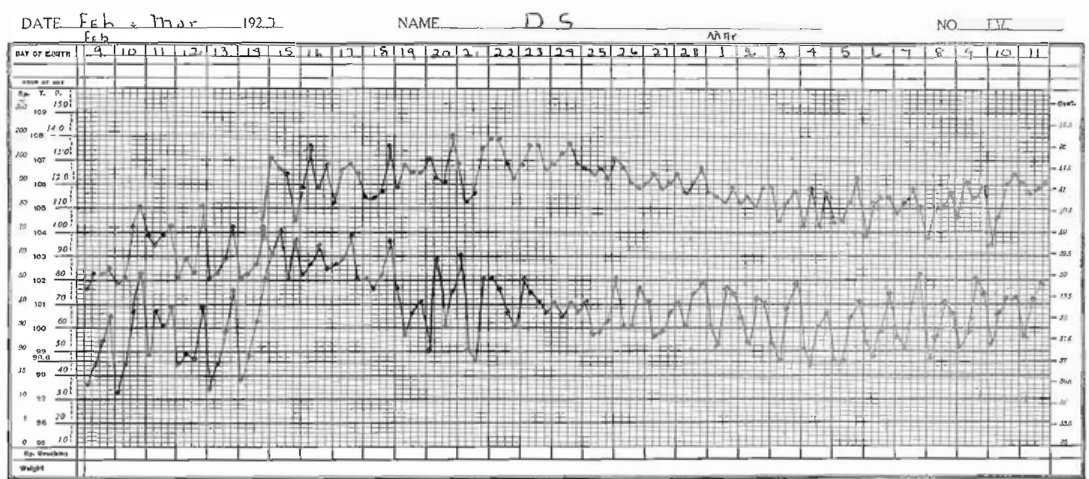
Fig. 6. Chart showing the effect of severe allergic reaction upon the temperature and pulse. A reinoculation on February 9 was followed by a second on the 15th, before the effect of the previous one had disappeared.
Patient was considered dangerously ill, but began to improve. Temperature gradually lowered, appetite improved, weight increased, and cough and sputum lessened, all of which indicated that her immunity had greatly increased as a result of the reinoculations and that the allergic reaction was passing off. This was followed by other similar reinoculations over a period of nearly a year, when finally immunity was so well established and the bacilli were so well incarcerated that the disease reached a stage of inactivity. The temperature dropped to normal, all symptoms of toxemia disappeared, the patient gained ten pounds in weight and assumed a state of general well being.
At times patients have one or two severe reinoculations with very marked allergic reactions, which result in sufficient stimulation of their immunity mechanism to cause the disease to go on to complete healing. This is in line with what we have seen in the use of tuberculin. Now and then we have seen healing of early lesions follow a severe tuberculin reaction. von Hippel3 reports several cases of tuberculosis of the eye which went on to healing after severe inflammatory reactions following injections of tuberculin.
The following case shows how the course of an active gradually spreading pulmonary tuberculosis was brought to a standstill by one severe reaction following a large reinoculation. The course of the disease was turned from one steadily advancing to one gradually receding.
Miss E. S., 18 years of age, examined September 1, 1927. History: Father, mother and one sister died of tuberculosis. Patient three years old when father died, and eight when mother died. Intimate association but not continuous. Measles, whooping cough, bronchitis during fifth year. During past ten years occasional twinges of left-sided pleurisy. September 1926, strength and endurance declined. Fatigue, poor appetite, loss of weight (8 lbs), rise of temperature to 99 and 100°. January 1927, severe left-sided pleurisy for one week. August 1927, severe pleurisy with slight cough. Had gained in weight from January until August, but lost five pounds during August.
Examined by me on Sept. 1, 1927. Symptoms: fatigue, loss of strength and endurance, decreased appetite, loss of weight, temperature 100°, severe cough, slight expectoration, 8 cc of sputum in 24 hours, with 10 bacilli per field.
Physical examination. Left lung: Extensive tuberculosis through upper lobe; much scarring, but also much activity. Pleurisy at the base. Right lung: Same condition but less extensive.
Under rest patient’s temperature came to normal in about one week. Remained so for about a month. On October 18 a reinoculation took place, causing a severe allergic reaction. The temperature was 100.5°; on the 22d, 103°, and on the 23d, 104.7°. It gradually declined, reaching normal November 17. Patient was severely ill. Much aching, extreme pleural pain over left side, lack of appetite, insomnia and rapid loss of weight. Marked increase of cough and expectoration, reaching 30 cc in 24 hours on October 22, and a much greater amount, although not recorded, a few days later, The clinical chart showing the effects of this severe reinoculation is shown in Fig.7.
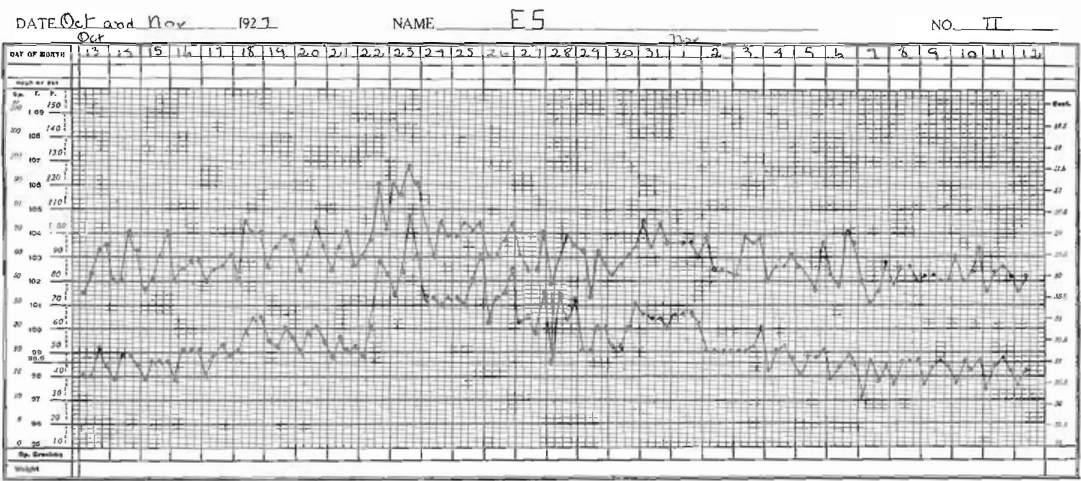
Fig. 7. Clinical chart showing the effects of a very severe reinoculation upon the temperature and pulse, followed by normal temperature. This one severe reaction raised the patient’s immunity and hastened recovery, and was followed by healing of an extensive infiltration throughout the left lung and in the upper portion of the right.
Physical examination at this time showed marked increase in moisture throughout the left upper lobe, indicative of a severe allergic reaction, exudative in character, with a lesser reaction in the right upper lobe. Following this, patient’s temperature came to normal and remained so until present time (Feb. 10, 1928). Has gained 18½ lbs. in weight; appetite excellent; cough practically nil; sputum 10 cc in 3 days, with 3 bacilli per field.
Physical examination in February reveals very marked reduction in physical signs in both lungs; right side entirely free from râles. As a result of the severe reinoculations that took place on October 18 and 22, the patient developed sufficient immunity, and sufficient allergic reaction took place throughout the areas of infection to cause a marked increase in fibrosis in and about the tubercles with a very definite stimulation to healing. It is possible that this one severe reinoculation may be ample to not only bring the disease to a state of quiescence but to carry it on to healing.
The escape of a few bacilli probably rarely causes new implantation unless the immune forces of the host are greatly depressed. On the other hand, if we may draw conclusions from experimental studies, these small reinoculations serve two very important purposes, that of stimulating the specific immunity reactions and raising them to a higher level, and that of calling forth slight allergic reactions in the periphery of tubercle and hastening fibrosis and healing.
Fig. 7 is a temperature chart representing a small reinoculation, yet one of sufficient magnitude to call forth definite symptoms. The symptoms were similar to those produced by a tuberculin reaction, viz.: malaise, aching, loss of appetite and weight, constipation, increased cough and expectoration. The picture was that of an allergic reaction of moderate degree. It is rational to assuture that the focus from which the bacilli which called forth this reaction escaped might readily have shed others, yet rarely in this particular type of the disease do we find one reaction superimposed immediately on a previous one. They are usually weeks–sometimes months–apart. Probably a few bacilli escape more or less continuously in many or most cases of this kind, yet not in sufficient quantities to call out continuous toxic reaction. Reflex action, however, is usually present in some organs.
At times we see a moderate reaction from reinoculation which fails to pass off short of two or three weeks, as shown in Fig. 8. Such temperatures are accompanied by slight toxic symptoms and could well be due to repeated reinoculations, insufficient to produce decided reaction of themselves, yet sufficient to prevent the passing off of the allergic reaction caused by the first reinoculation. It seems to me more probable, however, that they are due to the continuous absorption of toxins, the product of destroyed pulmonary tissue, in small amounts.
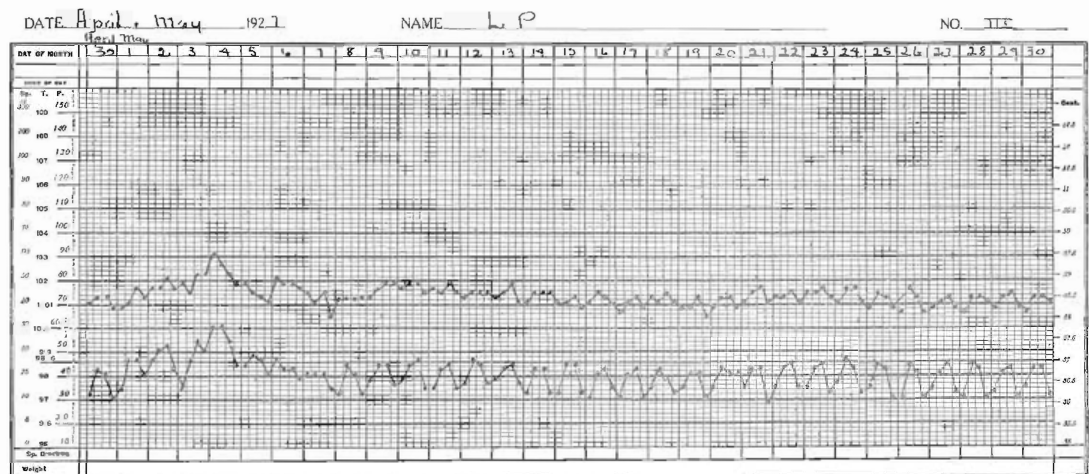
Fig. 8. Chart showing a normal temperature curve broken by a slight elevation of a few days’ duration, accompanied by increased cough and expectoration, malaise, headache, loss of appetite. Reinoculation caused by moderate numbers in bacilli.
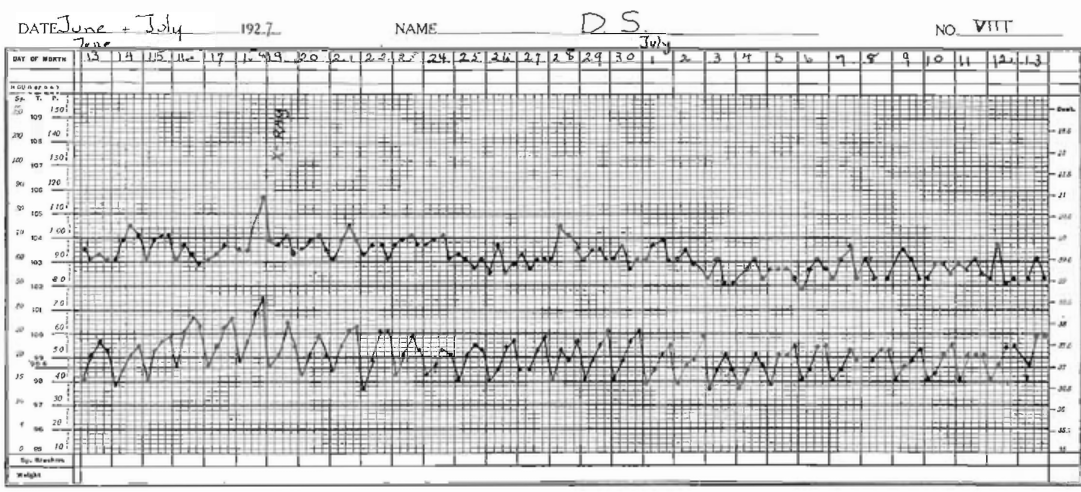
Fig. 9. Chart showing slight but continuous rise of temperature, which had followed several severe reinoculations, Temperature due to the absorption of toxins caused by destruction of both pulmonary tissue and tubercle bacilli.
Large reinoculations at times cause a more or less abrupt rise of temperature, although as a rule the maximum temperature is not attained until several days after the reaction has begun. Such reactions are accompanied by severe symptoms and more or less prostration of the patient. The lung, which before may have been only the seat of a mild process, at once takes upon itself a severe exudative inflammatory reaction. Such symptoms are prolonged often for weeks and even for months. Reinoculations continue to take place; bacilli are destroyed, tuberculoprotein enters the circulation, which, together with the products of the exudative reaction and the broken down pulmonary tissue, keep up a prolonged and often very injurious toxic action on the patient. If the patient withstands such a process, it is by developing a high grade of immunity and an unusual ability to withstand the effects of the toxins.
References Cited:
- Opie, Eugene L.: “Pathology of the Tuberculosis of Childhood: its Bearing on Clinical Work.” British Medical Journal, No. 3493, Dec. 17, 1927, pp. 1130-1135.
- Krause, Allen K.: “Anatomical structure of the tubercle from histogenesis to cavity.” Am. Rev. Tuberc., Vol. 15, 137-168, 1927.
- v. Hippel, A.: “Über die Nutzen des Tuberkulins bei der Tuberkulose des Auges.” A. F. O. Gr. 1905, Bd. 59, S. 1.