
Access to all articles, new health classes, discounts in our store, and more!
The Arithmetic of Disease
Presented before the 15th Annual Meeting of The American Institute of Dental Medicine, Palm Springs, CA, October 1958. Published in Journal of Dental Medicine, Vol. 14, No. 2, pp. 71-82, April 1959.
* * *
Introduction
All carefully studied natural phenomena follow mathematical laws and can be represented in equation form. This is well demonstrated by the equation for a circle or sphere and this is just as apparent from the formula for renal clearance. Strangely enough, this concept has never really been attempted with oral diseases though allusions to it appear in the literature.1,2,3 An attempt will be made within these few pages to develop a concept of oral disease which can be put into formula fashion.
Characteristics of the Disease Process
There are a host of properties of disease which could be listed. However, there are two inescapable features about the disease process which are peculiarly pertinent to this discussion. They are: (1) that a pathologic process is the end product of more than one operating factor, and (2) that health and disease seldom, if ever, become clinically evident in pure blacks and whites. In other words, sickness and health are relative states. To pursue this color analogy, health and disease present themselves to the clinician in a series of shades of gray. Because of the paramount importance of these two features of disease, they will now be considered.
Disease A Product of Multiple Factors
The evidence for this statement is abundant from many different sources: (1) animal studies, (2) the layman’s observations, (3) the experiences of the medical practitioner, and (4) the observations in the average dental office.
Animal Studies: The literature is replete with examples which underscore the point that disease is the end result of more than one factor. Two examples will be cited. First, the evidence is clear that a guinea pig can readily be made scorbutic.4 Under these conditions, rather classic gross and microscopic changes take place. One of the rather standard observations is the extravasation of blood into the joint spaces. It is generally agreed that such hemarthrosis is due solely to the scorbutic state. But, interestingly enough, if one extremity of a scorbutic guinea pig is immobilized in a plaster cast or by bandaging, the findings are quite different.5 In this case, the mobile limbs do indeed show the typical hemarthrosis. But bleeding into the immobilized leg cannot be demonstrated. Conversely, if a lead weight is attached to one joint or if one limb is exercised more than the others, the observations are once again quite different. In this case, the weighted or exercised limb shows more hemarthrosis than the non-weighted extremity. These extraoral experiments point up one very important item. It seems clear that hemarthrosis or no hemarthrosis is dependent upon two operating factors (Fig. 1): (1) an ascorbic acid deficiency, and (2) the presence or absence of local trauma in the form of a weight, excessive exercise, or plaster cast immobilization.
(Figure 1)
The second bit of evidence deals with the oral cavity. It has been shown that there are rather well-defined periodontal alterations associated with ascorbic acid deficiency in the guinea pig.6 It has also been clearly indicated that the so-called “scorbutic” changes are much greater in the presence of local chemical irritation of the gingival crevice with silver nitrate.7 Once again, it seems very evident that more than one factor seems to be a requisite to the development of pathosis.
The Layman’s Observations: The point that more than one factor operates in the causation of disease is not confined to animal studies. This concept is well-known to the man in the street. For it is a common experience for two persons, simultaneously drenched in a rain storm, subsequently to fare very differently. One of the individuals may contract a very severe upper respiratory infection, perhaps pneumonia, and may possibly even die. The other person remains unscathed. This kind of very crude observation (Fig. 2) suggests that the very same trauma, chilling, yields quite different results because of differences in people. The layman calls this difference by many names–notably resistance. Thus it is that the man on the street says, “he caught a cold because his resistance was low.” Here again, we learn that disease is not the result of but one operating factor.
(Figure 2)
The Experience in Medical Practice: The point that more than one factor operates in the causation of disease is also plentifully evident in everyday medical practice (Fig 3). For example, a seemingly healthy soul (at least free of any symptoms and signs of disease) steps out into the bright sun. Shortly thereafter, he notes a dermatitis on the dorsa of his hands. The examining physician quickly recognizes that the character and distribution of the lesions can mean but one disease–pellagra. No one will question that the patient was just as pellagrous the day before he stepped out into the sun. This story underlines the point that a suitable systemic substrate, niacin deficiency can be present unnoticed until some type of local trauma, the sun rays, does something to yield an end-result which neither alone could have produced.
(Figure 3)
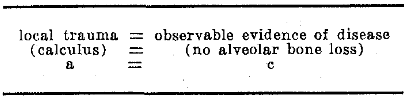
The Experience in Dental Practice: Examples of the interaction of local trauma and an appropriate systemic substrate are not confined to animal studies, observations by the layman, nor are they restricted to medical practice. There is very good reason to believe that these very same interrelationships are as much, if not more so, present in the oral cavity. For example, it is an everyday occurrence in the dental office to observe a patient with abundant amounts of calculus. The average dentist, by act if not by word, points out to the patient that the calculus is causing the bone loss. In other words, the practitioner might admit that what he is saying is (Fig. 4) that the local trauma, in this case the calculus, is causing the observable evidence of disease, in this instance the alveolar bone loss. In other words, a = b. Yet the very next patient might well present himself in the dental office with as much or more calculus than the preceding individual and yet with no observable alveolar bone loss. Then the following equation (Fig. 5) should be acceptable–namely, that local trauma, in the form of calculus, equals no alveolar bone loss. In other words, a = c.
(Figure 4)
(Figure 5)
If (Fig. 6) local trauma (calculus) equals observable evidence of disease, (alveolar bone loss), then a = b. If local trauma (calculus) equals no alveolar bone loss, then a = c. It then follows that b = c. This is obviously absurd since alveolar bone loss cannot equal no alveolar bone loss. It becomes clear, then, that the calculus, and this is but one example, cannot be considered to be the single cause of the disturbed bone picture. Illustrations of this same type are plentiful in everyday dental practice.8
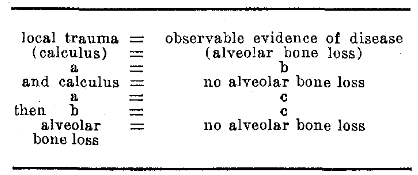
(Figure 6)
It would appear from these few, simple examples that the observable pattern of disease fits into a formula which may be expressed as follows (Fig. 7): that a suitable systemic substrate in combination with an appropriate exciting factor will yield observable evidence of disease as recognized clinically by way of symptoms and signs. It would follow, for stomatologic purposes (Fig. 8), that an appropriate systemic substrate acting in concert with suitable exciting oral factor would net observable oral evidence of disease i.e., oral symptoms and signs.
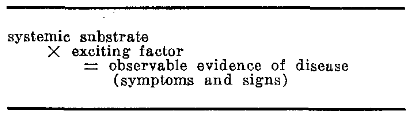
(Figure 7)
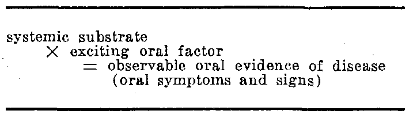
(Figure 8)
All of the data thus far indicate an attempt to underscore the fact that a pathologic process is the result of more than one causative agent. The question which may still persist is why clinical (observable) proof of disease should equal the product rather than the sum of a suitable systemic substrate and an appropriate exciting factor as shown on the left side of the equation. The answer may be found by studying the examples already cited.
It should be recalled that the pellagrin was asymptomatic and free of signs until he walked out into the blazing sunlight. In other words, as long as there was no exciting agent of threshold strength, in this instance no cutaneous trauma, this variable in the equation was zero (Fig. 9). Thus, regardless of the systemic imbalance, the hyponiacinosis alone does not produce clinical proof of disease. The right side of the equation is zero.
(Figure 9)
It would appear logical, then that the converse might also be true. In other words, had the patient not had aniacinosis, if this factor were now zero, then regardless of the actinic exposure, the product would again be zero (Fig. 10). There would not be the typical pellagrous dermatosis so characteristic of this nutritional deficiency state.
(Figure 10)
In the final analysis, it is rare, if not impossible, to eliminate (reduce to zero) either of the variables on the left side of the equation. This is so because disease states are not clinically observable in simple black and whites but rather in an infinite number of shades of gray–in other words, in degrees.
Degrees of Disease
There is no argument that an individual can be seemingly very healthy or undeniably sick. These are the blacks and whites of disease. However, too little attention is directed to the fact that there are degrees of sickness and well-being. In all probability, white (perfect health) is never attainable. Black, at the other pole, represents the ultimate in disease. Between these two limits is an infinite number of shades of gray–a limitless graduation of health to sickness.
This concept of degrees is not without clinical support. The clinician is constantly confronted by the patient who is clinically well today and clinically ill ten years hence. Surely the patient with diabetes mellitus, rheumatoid arthritis, ascorbic acid deficiency, to pick but a few examples, does not develop his disease overnight. But more relevant to this discussion is the individual at age 20 who has no alveolar bone loss, who continues to be well for the next 30 years, but yet, at age 50, does show severe alveolar bone degeneration. Obviously, this picture did not develop in a week, or month, or year. During the 30-year interval between white (age 20) and black (age 50), the patient cannot have been in perfect health. The question now is, “How does this new information fit into the formula?”
For illustrative purposes only, let us assign numbers to the two variables on the left side of the formula (Fig. 11). Let us simply say that there are graduations from 0 to 10. Zero, for the first variable in this scheme, indicates a perfectly healthy systemic substrate. Zero, for the second variable, signifies the complete absence of any exciting factors. Translated into a mythical situation, we are confronted with a subject who has absolutely no systemic disorder. Also, in this hypothetical case, the patient is free of calculus, there are no overhanging restorations, the occlusion is perfect. The end result is apparent–there are no observable symptoms nor signs in this perfect mouth.
(Figure 11)
On the other hand, we shall assign the value 10 to each of the two factors on the left side of the equation (Fig. 12). For example, a factor of 10 means that the patient is suffering with diabetes mellitus in its classical form with polyuria, polyphagia, polydipsia, and weight loss. A value of 10 for the second variable signifies abundant calculus, a host of ill-fitting restorations, and marked occlusal imbalance. The value on the right of the equation is high, representing the presence of many and marked symptoms and signs of disease. Thus, in the diabetic patient who meets these specifications, there are polyphagia, polyuria, polydipsia, and weight loss. In addition, there are marked gingivitis, extensive alveolar bone loss, possibly a history of slow post extraction healing, and perhaps gingival bleeding. The clinical evidence is clear–the patient is indeed systemically ill and there are plenty of oral symptoms and signs to prove it.
(Figure 12)
The two extremes, the 0 x 0 = 0 and the 10 x 10 = 100, the whites and the blacks, are simple to comprehend. But there are many other possible combinations (Fig. 13). Equation A represents a severe diabetic patient with only minimal local (oral) irritating problems. We note on the right side of the equation the value 10. This means that there are some few observable symptoms and/ or signs of disease. Translated into clinical terms, the 10 on the right side of equation A may represent minimal alveolar bone loss, slight gingival recession, or minimal marginal gingivitis in a severe diabetic patient with minimal oral trauma. Equation B shows the same end result, a value of 10. In this case, we are faced with a mild diabetic subject with marked local irritation.
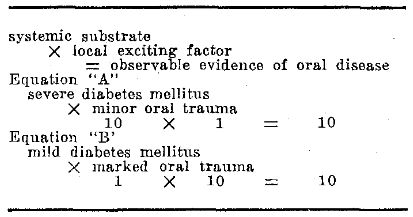
(Figure 13)
The latter combinations thus are potentially demonstrable. However, even more often the clinician is faced with a mild to moderate diabetic patient with mild to moderate local oral trauma (Fig. 14). In clinical parlance, the examiner is confronted with a patient with minimal alveolar bone loss or very subtle gingivitis and/or recession who appears, for all practical purposes, to be perfectly well.
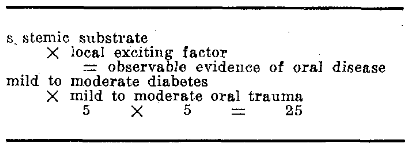
(Figure 14)
We have now established a formula for health and disease. The question which now arises is, “How does the oral cavity fit into this equation?” In order to answer this vital question, one must analyze the structure and function of the mouth.
The Oral Cavity
The mouth is a most unusual area of the body. This is so because: (1) it is, in many respects, exactly like other regions and, at the same time, (2) it is unlike any other part of the body. This is true both from a structural and functional standpoint.
The Structure of the Oral Cavity
Generally speaking, the mouth is very much like other mucosally-bounded cavities. It is lined by an epithelium much like that of the vagina, anus, and the nose. Beneath the mucosa are various types of connective tissue histologically similar to their homologues in other parts of the body. Thus, with such structural similarities, it is understandable why changes in the oral tissues parallel alteration in like tissues elsewhere in both health and disease. Herein lies the explanation for the simultaneous cyclic epithelial changes in the oral and vaginal mucosae during physiologic menstruation and the climacteric.9 This is the basis for the similarity of the cutaneous and mucosal lesions in such disorders as intestinal polyposis10 and Addison’s disease.11
At the same time, there are cells and tissues in the mouth which are truly unique in that they have no counterpart elsewhere. The teeth and the associated periodontal structures are the most glaring examples. The presence of the odontogenic apparatus makes the oral cavity special in two different ways: (1) problems arise in the mouth, notably caries and periodontal disease, not encountered anywhere else in the human body, and (2) the oral symptoms and signs of systemic disease states are modified by the presence of the very special cytoarchitecture of the teeth and the periodontium. Thus, simply by way of example, the oral findings of plumbism12 and lichen planus13 are far different from the evidences of these same diseases in the leg, or abdomen, or chest.
The discussion of the anatomy of the mouth can be simply summarized. First, the oral tissues are like their counterparts elsewhere. In other words, epithelium is still epithelium and fibrous tissue basically remains fibrous tissue. Consequently, a so-called collagen14 or bone disease15 implicates the collagenous or osseous elements wherever they may be. And so, understandably, systemic diseases do have their oral reflections. But, secondly, the oral tissues are in some anatomic respects quite unique. Hence, problems arise in the mouth which are not encountered elsewhere. Thus it is that the filiform papillae of the tongue atrophy in various nutritional disorders.16 So it is that the teeth become subclinically more mobile during the pregnancy state.17
The Function of the Oral Cavity
Not only is the mouth structurally like and unlike similar cavities, but it is also functionally like and unlike other mucosal zones. The similarities require little elaboration. What are more important are the differences–the unusual functional demands placed upon the oral tissues.
The mouth, it should be recalled, is expected to participate in a host of vital functions, notably speech and mastication. Within the very same breath, literally, the oral mucosa is required to tolerate high (boiling coffee) and low (freezing ice cream) temperatures. No other tissue of the body is asked to withstand such repeated insult. It is of parenthetic interest when one conducts a similar experiment upon the supposedly tougher skin, that an erythema results. Yet the mouth is expected, and does indeed, handle such microtraumata exceedingly well. The oral tissues, it must be emphasized, can only weather such persistent local irritation as long as the systemic substrate is in good health. This last point bears directly on the present discussion of a formula for disease.
We have already observed that the product of a systemic substrate and a suitable exciting oral factor yields observable oral evidence of disease. Now one can add that, under so-called physiologic conditions, oral irritation is high. Thus, in the formula one can say that local trauma is customarily assigned a value of 3, or 4, or 5 or more. It then becomes clear that the higher the value on the left side of the equation, the greater will be the product of the two variables on that side.
The Formula of Disease
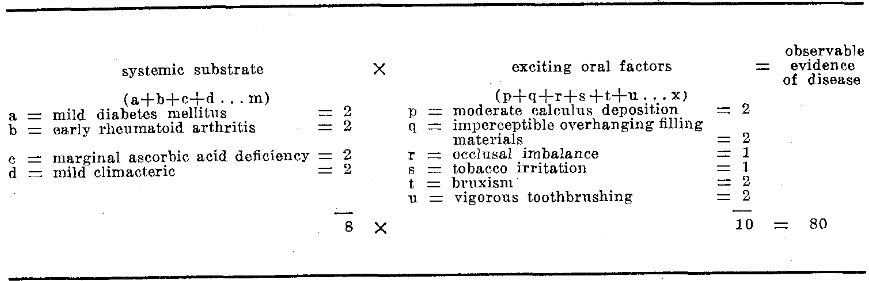
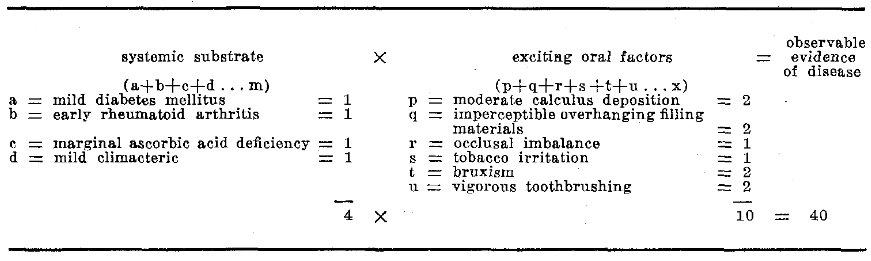
The equation which has just been developed suffers from one very great fault, its over-simplification. It implies that there are but two variables (systemic substrate and exciting factor). It suggests, to pursue the example, that a patient must be diabetic and must, in addition, have calculus. Actually, each of these factors in the equation may indeed be a host of variables (Fig. 15). Is it not conceivable that a patient, in the climacteric, may be a very mild diabetic suffering with early rheumatoid arthritis complicated by a marginal ascorbic acid deficiency? Is it not further possible that there may be a slight collection of calculus, imperceptible overhanging restoration(s), and minimal occlusal imbalance in an individual who smokes just a little bit too much, who grinds his teeth while asleep, and who brushes his teeth a bit too enthusiastically? Thus, in the formula (Fig. 15), a might well represent mild diabetes mellitus valued at two, b early rheumatoid arthritis, c marginal ascorbic acid deficiency, and d mild climacteric, with possibly other pathologic problems up to m. At the same time, p signifies minimal calculus deposition, q imperceptible overhanging filling materials, r occlusal imbalance, s tobacco irritation, t bruxism, u vigorous toothbrushing, and other local irritating factors up to x. It would appear that, actually, this is usually the state of affairs. In other words, the individual at 20 with alveolar bone loss is probably suffering with some of these disorders in their mildest forms. Hence, he remains presumably well, though at age 50 he does indeed display severe alveolar bone degeneration. Perhaps, here is the explanation for so-called idiopathic periodontal disease.
(Figure 15)
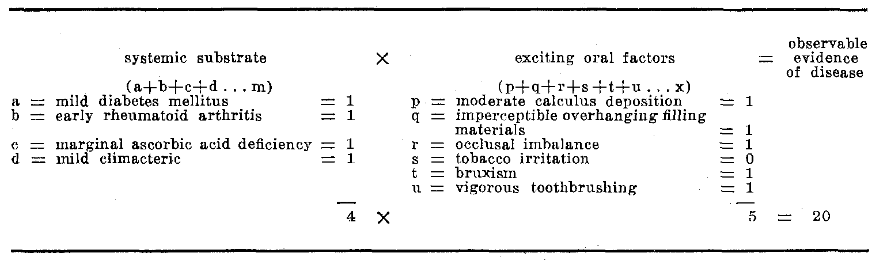
This equation also allows the opportunity to consider what the practitioner actually does when he treats and cures a particular problem. Assuming this equation to be correct, it then follows that the dentist is dedicated to reducing the numbers in both variables on the left side of the equation (Fig. 16). For example, in this particular patient, it is possible to correct the diet and better control the diabetic state, administer the adrenocortical hormones, supply ascorbic acid supplementation, and possibly even estrogen therapy. If one could do just this so that each of the assigned numbers were reduced from 2 to 1 then the sum of the far column would be 4 instead of 8. Thus, even without any oral therapy, the product would be 40 instead of 80. Accordingly, the oral symptoms and signs would decrease considerably. In other words, the oral cavity would be improved. If one could then add oral therapy the situation would become even more favorable (Fig. 17). For example, calculus could be eliminated. One must question whether it could be eliminated entirely to reduce this factor to zero. But even if the twos in the second column could be reduced to ones and tobacco eliminated, the sum of these operating factors would be reduced from 10 to 5. This means that 4 x 5 = 20. Once again, the number on the right diminishes and the mouth shows even fewer symptoms and signs. The point being made is that this equation underscores the purpose of therapy–namely to reduce all of these values to as close to zero as possible.
(Figure 16)
(Figure 17)
Thus far, the discussion has been largely philosophic in that a concept of disease, certainly not a new one, has been analyzed. An attempt has been made to make this concept more “real” with mathematic overtones. But the final test would be to list and discuss the 200 or so systemic disorders and to consider the interplay of systemic with all of the known local oral irritating problems. Obviously, this is impossible because: (1) of time limitations, and, more important, (2) much information is still lacking about these systemic diseases and even more data are needed regarding the interaction of systemic and local factors. It is, however, possible to show, by example, how the formula applies to a specific clinical problem.
Case Report
This particular case is included for several reasons: (1) it is a common problem in the average dental office, (2) the solution, at first glance, is simple, and (3) the story provides the rare opportunity to observe, almost in vitro, the interplay of local and systemic factors by modifying these two variables independently.
A 15-year-old female was first observed in the dental clinic with a very simple and easily demonstrable complaint–gingival bleeding from the embrasure between the left maxillary premolar and the first molar precipitated by toothbrushing. This is the kind of observation which can be confirmed or negated simply by having the patient brush her teeth in the presence of the examiner. Oral examination proved negative (Fig. 18) except for an ill-fitting MOD amalgam restoration in the first molar with a moderate overhanging margin. Once again, the problem appears to be quite simple (Fig. 19). The local mechanism trauma due to the combination of toothbrushing and the ill-fitting restoration appears to be causing the observable gingival bleeding. The usual procedure in the average dental office is to recommend replacement of the MOD restoration. Implied in this type of thinking is that the local trauma is the cause of the gingival bleeding.

(Figure 18)
(Figure 19)
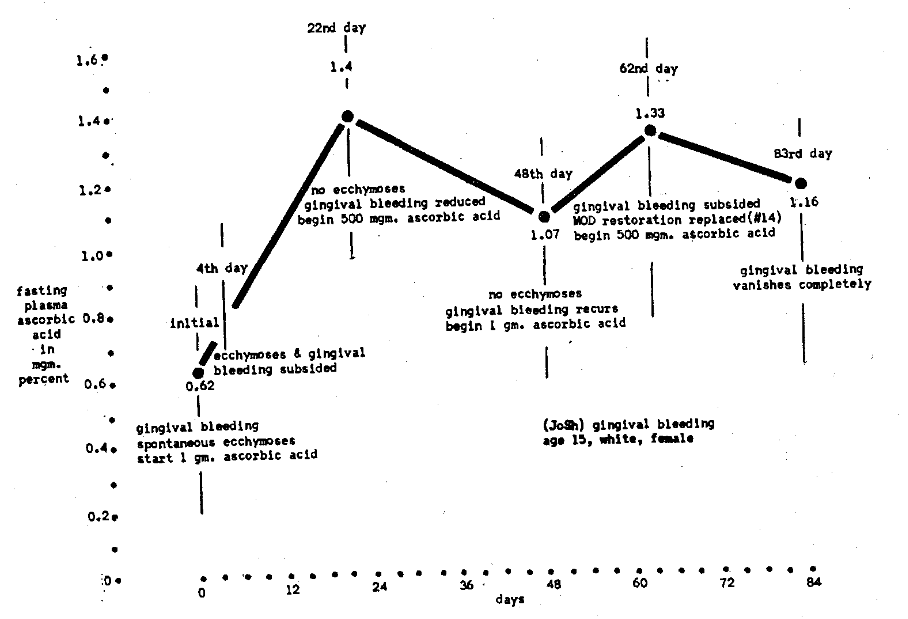
The only other findings of importance were seemingly spontaneous ecchymoses of the skin–incidentally, a very common observation particularly in the female and a very poor history of citrus intake–also a very common finding in about 30 to 40 percent of the population.18 The initial fasting plasma ascorbic acid level proved to be a marginal .62 mgm. percent (Fig. 20).
(Figure 20)
The patient was started on a daily regime of 1 gram of ascorbic acid by mouth in divided doses (250 mgm. four times a day). When seen four days later, she reported that both the ecchymoses and the gingival bleeding had subsided. It is important to point out that the toothbrushing habit was unchanged and the ill-fitting restoration still present. All that had been done was to decrease capillary fragility. However, the ascorbic acid regime was continued. On the 22nd day, there were no ecchymoses and reduced, but not absent, gingival bleeding. The fasting plasma ascorbic acid level was then 1.4 mgm. percent (roughly more than twice that on admission). Because of the interesting clinical course, the ascorbic acid dosage was halved–the patient told to take 500 mgm. ascorbic acid daily. When observed about three weeks later, on the 48th day, the gingival bleeding but not the ecchymoses had reappeared while the plasma ascorbic acid level had declined to 1.07 mgm. percent. The 1 gram per day ascorbic acid regime was instituted. Two weeks later, on the 62nd day, the plasma level had risen to 1.33 mgm. percent. Most interestingly, the gingival bleeding had once again subsided. This time the dosage was again halved at the same time that the ill-fitting restoration was replaced with a more acceptable one. The fasting plasma ascorbic acid level at the next visit, three weeks later on the 83rd day, was 1.16 mgm percent. The patient reported that the gingival bleeding had now vanished completely.
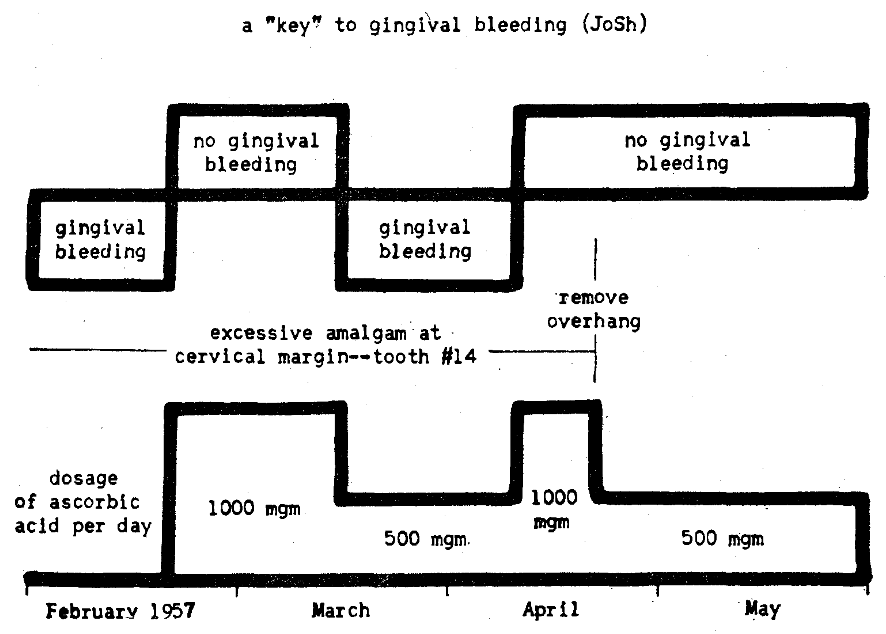
This case emphasizes very well the delicate interplay of systemic and local factors (Fig. 21). One can pictorially describe the relationship much like a “key” fitting a lock. Here is a child obviously suffering with a mild ascorbic acid deficiency as evidenced by the spontaneous cutaneous ecchymoses even if one wishes to explain away the gingival bleeding on purely local factors. However, the same increased capillary fragility and permeability which produced ecchymoses might well have contributed to the gingival bleeding with toothbrushing. This seems a likely explanation since decreasing capillary fragility (without local treatment) by means of ascorbic acid caused the disappearance of the ecchymoses and a reduction in gingival bleeding. This can be applied to the formula (Fig. 22). The mild to moderate vitamin C deficiency (arbitrarily assigned a value of 5) in combination with mild to moderate local trauma (also assigned the number 5) produced moderate gingival bleeding as indicated by the 25 in the right side of the equation. When the ascorbic acid status was improved (Fig. 23) by reducing the value, let us say from 5 to 1, the product yielded reduced gingival bleeding. However, when both the hypovitaminosis and the overhanging restoration were corrected (Fig. 24), the bleeding disappeared, at least macroscopically.
(Figure 21)
(Figure 22)
(Figure 23)
(Figure 24)
Summary
- An attempt has been made to show, in simple arithmetic fashion, that the observable oral evidence of disease is the product of more than one operating factor.
- Since oral trauma, even under physiologic conditions, is quite high, the product of it and even a marginal systemic imbalance may be critical enough to net oral symptoms and/or signs.
References Cited:
- Glickman, I. Clinical periodontology. 1958. Ed. 2, Philadelphia, W. B. Saunders Company. p. 477.
- Goldman, H. M. Periodontia. Third edition. 1953. St. Louis, The C. V. Mosby Company. p. 251.
- Bernier, J. L. The management of oral disease. 1955. St. Louis, The C. V. Mosby Company. p. 220.
- Mannering, G. J. “Vitamin requirements of the guinea pig.” Vitamins and Hormones 7: 201-221, 1949.
- Follis, R. H., Jr. “Effect of mechanical force on the skeletal lesions in acute scurvy in guinea pigs.” Path. 34: #4, 579-582, April 1943.
- Glickman, I. “Acute vitamin C Deficiency and periodontal disease. I. The periodontal tissues of the guinea pig in acute vitamin C deficiency.” Dent. Res. 27:# 1, 9-23, February 1948.
- Glickman, I. “Acute vitamin C deficiency and periodontal disease. II. The effect of acute vitamin C deficiency upon the response of the periodontal tissues of the guinea pig to artificially induced inflammation.” Dent. Res. 27: # 2, 201-210, April 1948.
- Cheraskin, E. “Preventive medical case-finding opportunities and responsibilities of the dentist.” Clinics of North America, 283- 296, July 1958.
- Papic, M. and Glickman, I. “Keratinizaton of the human gingiva in the menstrual cycle and menopause.” Oral Surg., Oral Med, and Oral Path. 3: #4, 504-516, April 1950.
- Jeghers, H., McKusick, F. A. and Katz, K. H. “Generalized intestinal polyposis and melanin spots of the oral mucosa, lips, and digits: a syndrome of diagnostic significance.” New England Jour. Med. 241: #25, 993-1005, December 22, 1949; 241: # 26, 1031-1036, December 29, 1949.
- Oard, H. C. Kaletsky, T. and Gettinger, R. “Addison’s disease with particular reference to oral chromatophores and the role of vitamin deficiency.” Clin. Oral Path. 3: # 1& 2, 16-37, March-June 1939.
- Schour, I. and Sarnat, B. G. “Oral manifestations of occupational origin.” A.M.A. 120: #15, 1197-1207, December 12, 1942.
- Darling, A. I. and Crabb, H. S. M. “Lichen planus.” Oral Surg., Oral Med. and Oral Path. 7: #12, 1276-1289, December 1954.
- Stafne, E. C. and Austin, L. T. “A characteristic dental finding in acrosclerosis and diffuse scleroderma.” Jour. Orthodont. and Oral Surg. (Oral Surg. Sect.) 30: #1, 25- 29, January 1944.
- Weinmann, J. P. “Bone changes in the jaws caused by renal hyperparathyroidism.” Periodontal. 16: #3, 94-98, disc. 98-104, July 1945.
- Bakwin, H., Reardon, H. S., Winn, J. S., Tenbrink, M. S., Stern, M. L. and Engel, M. G. “Relation of lesions of the tongue in children to niacin deficiency.” Jour. Dis. Child. 74: #6, 657-668, December 1947.
- Muhlemann, H. R. “Periodontometry: a method for measuring tooth mobility.” Oral Surg., Oral Med. and Oral Path. 4: #10, 1220-1233, October 1951.
- Cheraskin, E., Dunbar, J. B. and Flynn, F. H. “The intradermal ascorbic acid test. Part III. A study of forty-two dental students.” Dent. Med. 13: 135-155, July 1958.