
Access to all articles, new health classes, discounts in our store, and more!
Roentgenographic Manifestations of Osseous Changes in the Jaws
Presented at the 99th Annual Scientific Section of the American Dental Association, Section on Roentgenology, Dallas, Texas, November 10-13, 1958. Published in Oral Surgery, Oral Medicine, and Oral Pathology, Vol. 12, No. 4, pp. 442-458, April 1959.
* * *
Introduction
The roentgenographic reflections of osseous changes are the direct result of the degree of bone mineralization.1,2 The amount of mineralization (that is, the concentration of calcium salts) present in bone tissue at anyone moment is a function of the simultaneous interplay of factors which are contributing to bone formation and bone resorption. Consequently, consideration must first be given to the conditions which produce normal bone tissue.
Normal Bone Tissue
Under physiologic conditions, bone tissue is constantly being formed and destroyed. Hence, two mechanisms are operating in parallel (Fig. 1).
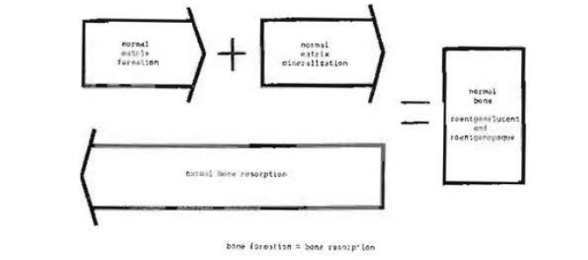
Fig. 1–Mechanism of physiologic bone formation and bone resorption.
Bone formation, also called osteogenesis, takes place in two phases. First, an organic matrix consisting of collagen and mucopolysaccharides is formed. Next, this organic stroma is modified by molecular rearrangement and mineralization. From a chemical standpoint, the mucopolysaccharides are conjugated with calcium salts arranged in the form of hexagonal crystals.3,4
Bone resorption, in the light of present information, is due to the action of highly differentiated cells, the so-called osteoclasts.5,6 Unlike bone formation which occurs in two stages, bone destruction is an all-or-none process during which there is removal of both the organic and inorganic components of bone tissue. Hence, such terms as demineralization and decalcification of bone are incorrect, since they imply the extraction of the calcium salts without removal of the organic matrix.
Throughout the life of bone tissues in the adult human being there are constant, simultaneous, and more or less equal bone formation and bone resorption. From a roentgenographic standpoint, the bone tissue (Fig. 2) is represented by a series of blacks to whites. There are areas of relative roentgenolucency (for example, cancellous bone and periodontal membrane) and other regions of relative roentgenopacity (for example, lamina dura and alveolar crest).
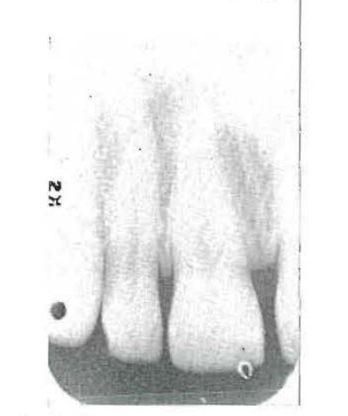
Fig. 2–Roentgenogram of normal bone.
Pathologic Bone Tissue
It becomes readily apparent, even from this simple explanation of normal bone tissue, that disturbances in the osseous mechanism can occur in either the formation or the destruction of bone (Fig. 3).
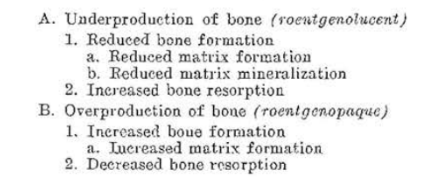
Fig. 3–Roentgenographic analysis of jaw pathosis.
All or part of a bone may show evidence of underproduction or overproduction. The former will appear as a roentgenolucent shadow; the latter will be roentgenopaque.
Roentgenolucency, in turn, may be the result of reduced bone formation or increased bone resorption. Finally, a reduction in the formation of bone may stem from impairment in one of two mechanisms. There is the possibility of reduced development of the osteoid matrix or a normal matrix may never become properly mineralized. Whatever the mechanism, the end result is a roentgenolucent shadow.
On the other hand, an overproduction of bone tissue may arise in one of two ways. First, there is a mechanism which leads to an increase in matrix which subsequently becomes mineralized. The other possibility is a decrease in bone resorption. Whatever the mechanism, the end result is a roentgenopaque shadow.
Roentgenolucent Shadows
Roentgenolucent shadows are always the result of (1) reduced bone formation due to a decrease in matrix development or lack of matrix mineralization or (2) increased bone resorption. These are the basic mechanisms. However, the observed roentgenographic picture will be the result of modifications of these basic processes. For example, the picture will vary in accordance with whether the pattern is generalized or localized in one of the jawbones, whether the lesion is clearly delimited or ill defined, whether the mandible or the maxilla is implicated, and whether or not local irritating factors are operative.7-10
Roentgenolucent lesions due to a defect in matrix formation: Reduced matrix formation, in the presence of normal mineralization of the matrix which is being formed and in the presence of normal bone resorption, will produce roentgenolucent shadows (Fig. 4). The roentgenographic appearance is referred to as osteoporosis. Osteoporosis is due to one of three things (Fig. 5): (1) a disturbance in the osteoblasts which form the osteoid matrix, (2) a matrix defect itself, and (3) idiopathic causes.
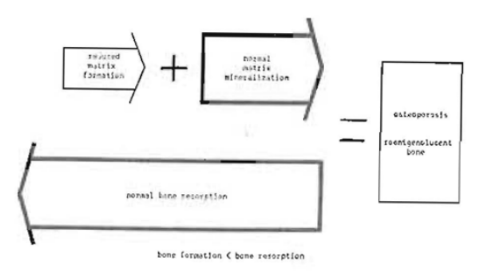
Fig. 4–Mechanism of osteoporosis.
Fig. 5–Causes for roentgenolucent shadows due to a defect in matrix formation (osteoporosis).
The normal stimuli to the osteoblasts are stresses and strains. Immobilization of a part of the skeleton for any reason (for example, plaster cast, intermaxillary jaw fixation, or neurologic or muscular disease) leads to decreased osteoblastic activity. Thus, with an inadequate osteoid matrix, total mineralization of that area is reduced. The end result is a roentgenolucent picture. The importance of disuse atrophy has been convincingly shown in a study of four healthy young men who were immobilized in bed by means of plaster casts for six weeks.11,12 During this interval, these subjects lost 9 to 24 grams of calcium, which is equivalent to 1 to 2 per cent of total body calcium.
Osteoporosis may be present in all of the skeleton, generalized in a particular bone, or occur only in a portion of a single bone. Osteoporosis of the entire mandible and/or maxilla without other bone involvement is rare except in isolated cases (e.g., intermaxillary jaw immobilization). However, osteoporosis of the jaws as part of a systemic skeletal problem is frequently encountered.
CASE 1:–Fig. 6 shows the markedly atrophic hands of a patient with scleroderma13,14 of approximately fourteen years’ duration. Fig. 7 demonstrates the marked osteoporosis of the phalanges and the carpal and metacarpal bones due, in part, to the disuse atrophy. Fig. 8 shows the rigid facial skin and points up the difficulty which the patient had opening and closing her mouth. Finally, Fig. 9 demonstrates the obvious roentgenolucent reflections of osteoporosis of the jaws. It is generally agreed that several factors operate to produce osteoporosis in such stress disorders. However, the pertinent point here is that the osteoporosis is the result of a disturbance in matrix formation and that disuse atrophy is one of the important causes.
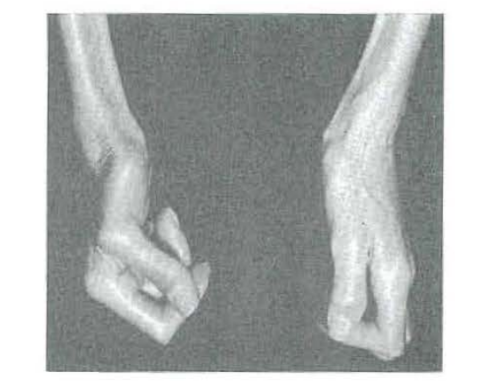
Fig. 6–Immobile hands of a patient with scleroderma.
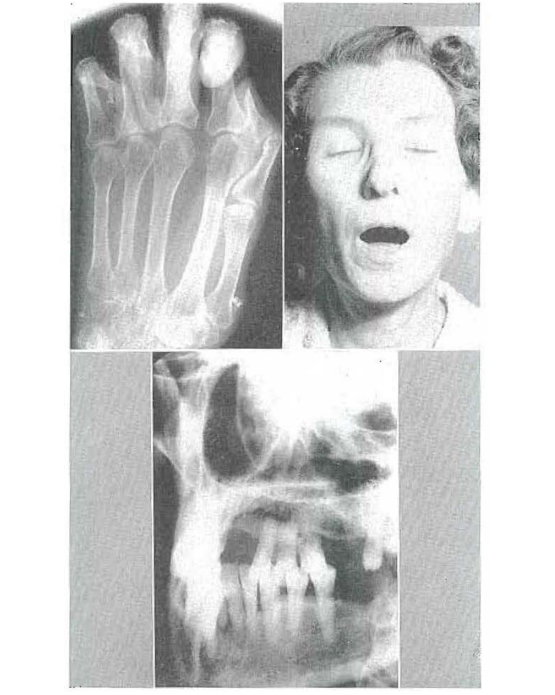
Fig. 7–Hand roentgenogram of a patient with scleroderma showing osteoporosis.
Fig. 8–Clinical picture of a patient with scleroderma showing difficulty in opening mouth.
Fig. 9–Roentgenogram of a patient with scleroderma showing osteoporosis.
CASE 2:–Osteoporosis due to a lack of physiologic stresses and strains may be confined to a portion of a single bone. Fig. 10 shows a periapical projection of an area of the left mandible where a tooth-borne prosthesis is worn with little if any stress exerted to the underlying bone. The trabeculae are widely spaced and the dominant feature is relative roentgenolucency. In contrast, Fig. 11 shows a periapical view of the opposite side of the arch, taken under the very same roentgenographic standards, where a free-end saddle prosthetic appliance is worn. Here there are very obvious stresses and strains to the subjacent bone. The roentgenogram discloses a much more dense trabecular pattern with greater mineralization leading to greater roentgenopacity.
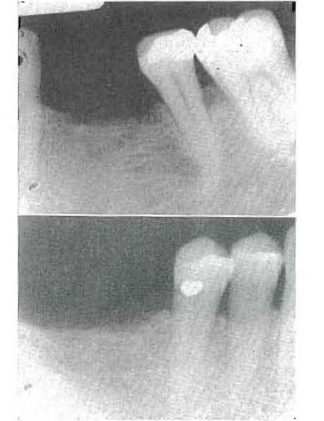
Fig. 10–Periapical roentgenogram of a patient who wears a partial denture. The denture is tooth borne on one side. The large trabecular spaces (indicating osteoporosis) are probably due to lack of stimulation of the subjacent bone (disuse atrophy).
Fig. 11–Periapical roentgenogram of a patient who wears a partial denture. The denture is tissue borne on one side. The small trabecular spaces should be compared with those in Fig. 10 from the same patient.
Time does not permit a detailed discussion of the many reasons for failure of the matrix to develop physiologically (Fig. 5). It is enough to say merely that a deficiency of any one or a combination of the ingredients necessary to make matrix will produce osteoporosis. Thus, a gonadal deficiency will cause osteoporosis. The changes which accompany the climacteric are often subtle and sometimes difficult to identify.15,16 However, when hypogonadism occurs abruptly or at a time other than in the autumnal years, the osteoporotic pattern is clearly evident.17,18 Other causes include malnutrition in the form of a deficiency of protein or ascorbic acid,19,20 thyrotoxicosis,21,22 congenital osteoblastic defects, as in osteogenesis imperfecta,23,24 and finally idiopathic osteoporosis.
Roentgenolucent lesions due to a defect in matrix mineralization: Osteomalacia is a disorder of bone tissue caused by failure of calcium salts to be conjugated with the mucopolysaccharides and properly and promptly deposited in the osteoid matrix (Fig. 3). This mechanism is graphically depicted in F ig. 12, which shows the normal osteoid matrix formation and normal bone resorption.
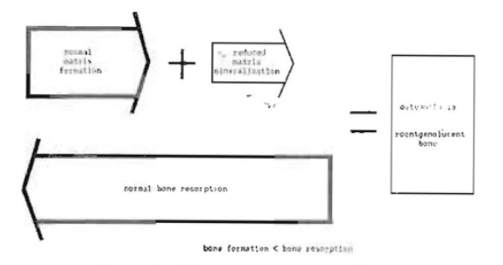
Fig. 12–Mechanism of osteomalacia.
The basic difficulty is one of mineralization. Osteomalacia may be due to one of four reasons (Fig. 13): (1) lack of intake or failure of utilization of vitamin D,25,26 (2) renal acidosis,27,28 (3) idiopathic loss of calcium in the urine, and (4) the transitional period of hyperparathyroidism after parathyroidectomy.

Fig. 13–Causes for roentgenolucent shadows due to a defect in matrix mineralization (osteomalacia).
CASE 3:–Fig. 14 shows the roentgenogram of the wrist of a 13-year-old boy with rickets. The characteristic cupping at the distal ends of the radius and ulna29 are compared with the lack of cupping in the wrist of a nonrachitic 13-year-old child. Fig. 15 depicts the relative roentgenolucency of the mandible due to a lack of physiologic mineralization in the presence of normal matrix formation.
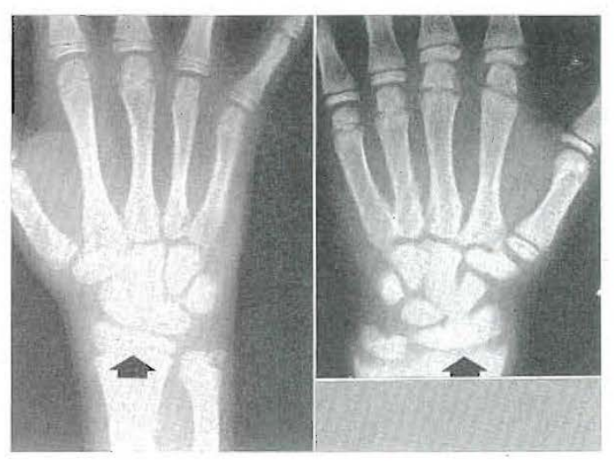
Fig. 14–Roentgenographic comparison of a normal wrist (left) and a rachitic wrist (right) in two 13-year-old boys.

Fig. 15–Periapical roentgenogram of a 13-year-old rachitic child showing osteomalacia.
Roentgenolucent lesions due to increased bone resorption: Roentgenolucent shadows may also be due to accelerated bone resorption in the presence of normal bone formation (Fig. 3). This mechanism is depicted graphically in Fig. 16. The classical, but uncommon, example is primary hyperparathyroidism, also called osteitis, fibrosa cystica generalisata, which is caused by a parathyroid adenoma or hyperplasia of parathyroid tissue.30,31 However, there are many other, more common disorders characterized by increased bone resorption. Some of these are systemic, while others are localized. Included in this group, for example, are multiple myeloma,32,33 metastases of malignant neoplasms,34,35 and even localized areas of infection36,37 encountered with periapical infection.
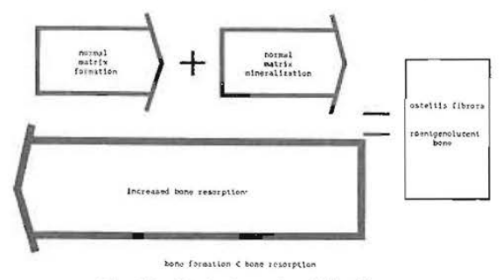
Fig. 16–Mechanism of osteitis fibrosa.
CASE 4:–A 38-year-old man had a “mole” removed from his back five years previously. Biopsy proved it to be a melanoma.38,39 When the patient was last seen, five years after removal of the lesion from the back, 132 metastatic lesions could be counted in the skin alone (Fig. 17). However, he was referred to the dental clinic because of tenderness and looseness of the lower anterior teeth. The roentgenolucent shadows apparent in the periapical (Fig. 18) and occlusal projections (Fig. 19) represent metastatic lesions. These roentgenolucent shadows are due to accelerated bone destruction in the presence of normal bone formation.
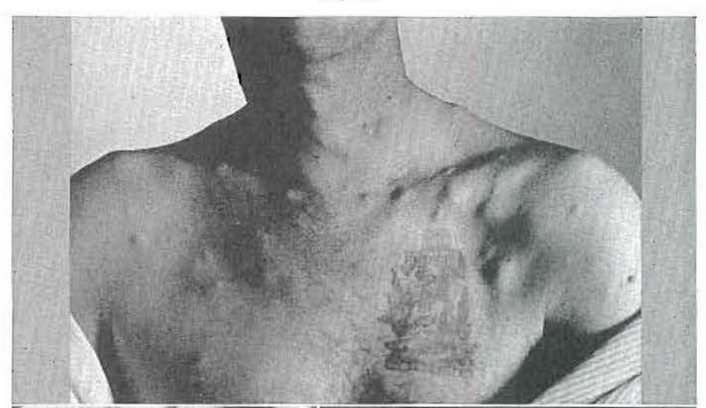
Fig. 17–Patient with melanoma and 132 palpable metastatic nodules.
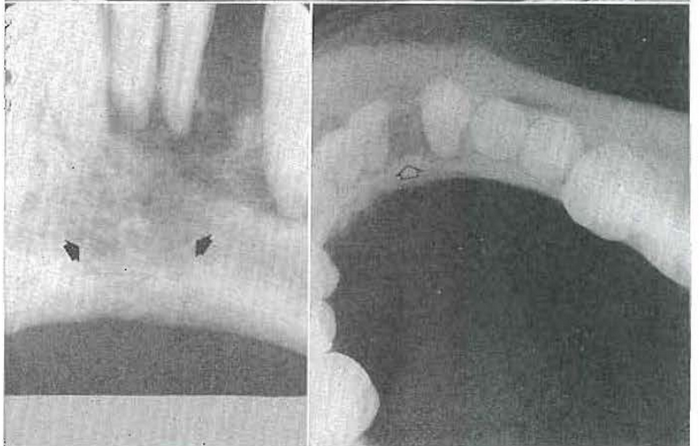
Fig. 18–Osteitis fibrosa secondary to melanoma metastasis causing loose teeth.
Fig. 19–Osteitis fibrosa secondary to melanoma metastatic causing loose teeth.
CASE 5:–Fig. 20 shows well-defined roentgenolucent shadows in the mandible. Fig. 21 simply underscores the fact that they are multiple. This type of roentgenolucent lesion can be due to a number of systemic and local causes. However, Fig. 22 shows a similar punched-out lesion in the skull, characteristic of multiple myeloma. Of importance to this discussion is the fact that such lesions are the result of invasion of tumorous tissue leading to increased bone resorption in the presence of normal bone formation.
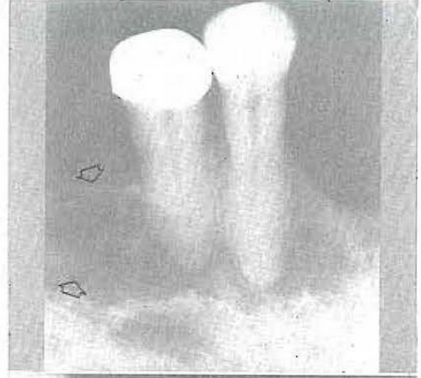
Fig. 20-Osteitis fibrosa secondary to multiple myeloma.
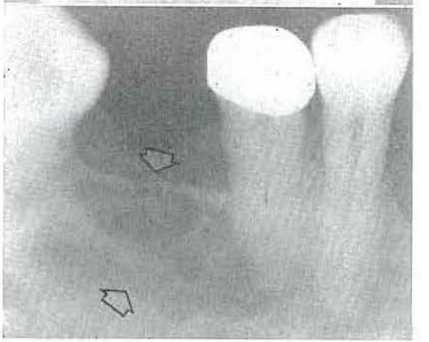
Fig. 21–Osteitis fibrosa secondary to multiple myeloma.
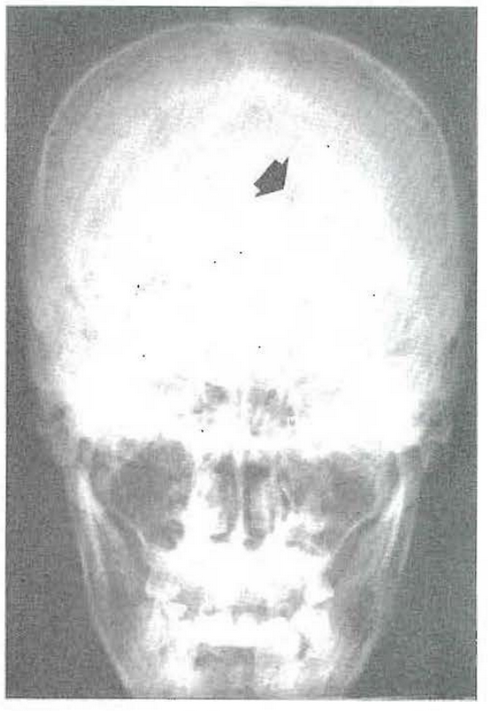
Fig. 22–Typical punched-out skull lesion suggestive of multiple myeloma.
All of the cases shown thus far have one common denominator. The roentgenolucent lesions are the result of (1) a decrease in the formation of osteoid matrix, (2) a reduction in the physiologic mineralization of normal matrix, or (3) increased bone resorption.
Roentgenopaque Shadows
Roentgenopaque lesions, like roentgenolucent ones, are the result of a disturbance in either bone formation or bone resorption. Whatever the mechanism, the roentgenographic picture is termed osteosclerosis.
Roentgenopaque lesions due to increased bone formation: Mice treated with estrogens show evidence of a generalized overproduction of osteoid matrix, probably the result of osteoblastic stimulation. The exuberant matrix is mineralized. The end result, not due to hypermineralization but rather to physiologic mineralization of overabundant matrix, is a generalized roentgenopaque skeleton.40 There is no human counterpart of such generalized roentgenopacity due to increased matrix formation. However, this very same mechanism can and does operate in man within a circumscribed segment of bone tissue. Thus, it is possible to observe in the human being an area of well-delimited roentgenopacity due to an overproduction of osteoid matrix (Fig. 23).
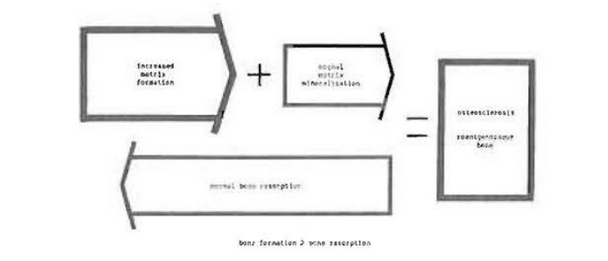
Fig. 23–Mechanism of osteosclerosis due to increased matrix formation.
CASE 6:– Fig. 24 shows a typical roentgenographic picture of an osteoma 41,42 of the mandible. This pattern of a benign bone-forming neoplasm is due to an overproduction of osteoid matrix and the normal mineralization of this osteoid frame.

Fig. 24–Osteoma demonstrating osteosclerosis.
Roentgenopaque lesions due to decreased bone resorption: Finally, roentgenopacity may be the result of decreased bone resorption in the presence of normal matrix formation and physiologic mineralization (Fig. 25). This is classically shown in osteopetrosis, also called Albers-Schönberg or marble bone disease.43,44 In this particular developmental disorder, osteoclastic activity is reduced although normal bone formation is present.
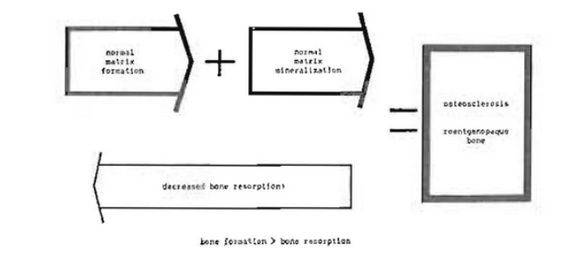
Fig. 25–Mechanism of osteosclerosis due to decreased bone resorption.
This same mechanism may operate locally. A classic example of stomatologic import is the separation of a bone fragment from the neighboring bone and blood supply. The roentgenopaque area is called a sequestrum, which is a section of necrotic, highly mineralized bone associated with chronic suppurative osteomyelitis.45,46
Roentgenolucent-Roentgenopaque Shadows
The story thus far described is simple–in fact, it is too simple. From this discussion, one might gather that osseous changes are simply the result of a disturbance which occurs in a single mechanism while the others continue in a physiologic fashion. Actually, the pathophysiologic sequence of events in osseous disease is more complex. It follows that the roentgenographic picture will also be more complicated.
In many instances, the pattern observed in the roentgenogram is characterized by some areas which are roentgenolucent and other regions which are relatively roentgenopaque. This type of roentgenographic pattern usually signifies a primary process of chronic bone destruction. It should be recalled that bone resorption per se is a stimulus to bone formation. Hence, it is not unusual to find roentgenolucent areas indicative of increased bone resorption and, close to these, other roentgenopaque areas representing compensatory osteoid matrix formation and mineralization. This mechanism is graphically portrayed in Fig. 26.
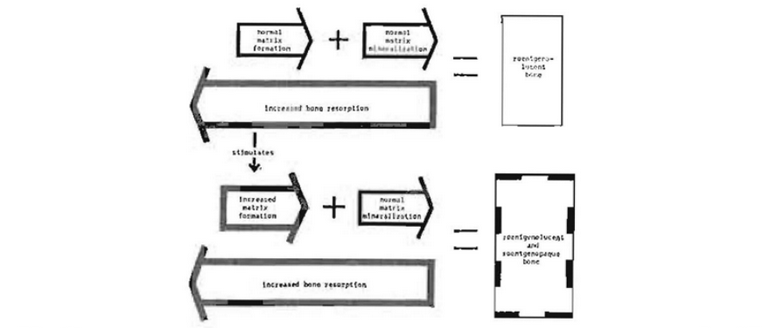
Fig. 26–Mechanism of roentgenolucent (osteitis fibrosa)–roentgenopaque (osteosclerosis) bone.
CASE 7:–Fig. 27 shows the characteristic roentgenographic lesions of Paget’s disease of bone.47,48 There are roentgenolucent areas intermingled with other roentgenopaque areas. Actually, increased bone resorption is the primary process. This accounts for the roentgenolucent shadows. However, the irritant is of low-grade intensity. This is a stimulus to increased osteoblastic action. The end result is compensatory osteoid matrix formation and mineralization, represented in the roentgenogram by the roentgenopaque areas.

Fig. 27–Paget’s disease of bone.
CASE 8:–The mechanism just described is a common one and occurs in many systemic disorders. This same sequence of events may be found in local disorders confined to a portion of a single bone. Usually, the basic process is a low-grade infection or mechanical trauma. This is the stimulus which sets off compensatory bone formation. Fig. 28 shows a typical example of intermingled roentgenolucent and roentgenopaque areas in a person with chronic suppurative osteomyelitis.
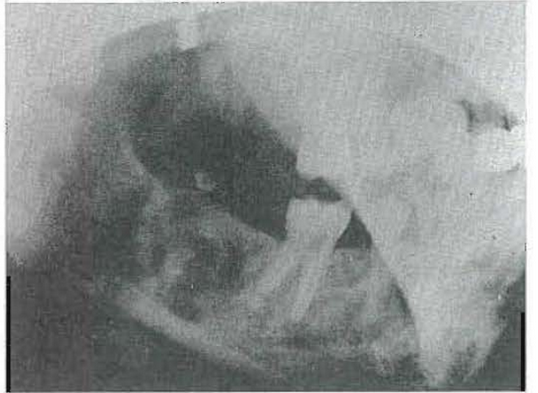
Fig. 28–Chronic osteomyelitis.
Summary
- Bone tissue, under physiologic conditions, is the result of an interplay of two mechanisms: (a) bone formation and (b) bone resorption.
- Bone formation actually occurs in two phases; (a) the formation of an osteoid matrix and (b) matrix mineralization.
- Bone resorption is an all-or-none phenomenon characterized by removal of both the organic and the inorganic components of bone.
- Pathologic bone tissue is the result of a disturbance in either bone formation or bone resorption.
- Roentgenolucent shadows are due to (a) decreased osteoid matrix formation, (b) decreased mineralization of the osteoid frame, or (3) increased bone resorption.
- Osteoporosis may be defined as a roentgenolucent shadow due to a decrease in osteoid matrix formation.
- Osteomalacia is defined as a roentgenolucent shadow, the result of an interference with physiologic mineralization.
- Osteitis fibrosa is defined as a roentgenolucent shadow caused by an increase in bone resorption.
- Roentgenopaque shadows, referred to as osteosclerosis, are caused by an increase in the formation of osteoid matrix or a decrease in bone resorption.
- Many disorders are characterized by a basic process of increased bone resorption with superimposed secondary and compensatory bone formation.
- Roentgenolucent, roentgenopaque, and roentgenolucent-roentgenopaque shadows may be part of generalized skeletal disease, confined to a single bone, or restricted to only a small portion of one bone.
References Cited:
- Weinmann, J. P.: “Variations in the Structure of Bone and Bones and Their Significance in Radiology,” Oral Surg., Oral Med. & Oral Path. 8: 988, 1955.
- Swenson, P. C., and Jeffery, R. B.: “Defective Skeletal Mineralization,” GP 7: 34, 1953.
- Brasseur, H., Dallemagne, M. I., and Melon, T.: “Chemical Nature of Salts From Bones and Teeth and of Tricalcium Phosphate Precipitates,” Nature (London) 157: 453, 1946.
- Dallemagne, M. I.: “The Physiology of Supporting Tissue,” Rev. Physiol, 12: 101, 1950.
- Weinmann, J. P.: “Bone Formation and Bone Resorption,” Oral Surg., Oral Med. & Oral Path. 8: 1074, 1955.
- McLean, F. C., and Urist, M. R.: Bone: An Introduction to the Physiology of Skeletal Tissue, Chicago, 1955, University of Chicago Press, p. 64.
- Cheraskin, E.: “The Arithmetic of Disease” (to be published).
- Cheraskin, E.: “Preventive Medical Case-Finding Opportunities and Responsibilities of the Dentist,” Clin. North America, p. 281, July, 1958.
- Cheraskin, E.: “Oral Manifestations of Systemic Diseases,” South Carolina M. A. 53: 241, 1957.
- Cheraskin, E.: “Oral Manifestations of Systemic Diseases,” Nat. M. A. 50: 241, 1958.
- Deitrick, J. E., Whedon, G. D., and Shorr, E.: “Effects of Immobilization Upon Various Metabolic and Physiologic Functions of Normal Men,” J. Med, 4: 3, 1948.
- Deitrick, J. E., Whedon, G. D., an d Shorr, E.: “The Effects of Bed Rest and Immobilization Upon Various Chemical and Physiological Functions of Normal Men: Their Modification by the Use of the Oscillating Bud,” Conference on Metabolic Aspects of Convalescence, Transactions of the Twelfth Meeting, Feb. 4-5, 1946, New York, Josiah Macy, Jr. Foundation, pp. 44-61.
- Looby, J. P., and Burket, L. W.: “Scleroderma of the Face With Involvement of the Alveolar Process,” J. Orthodontics & Oral Surg. 28: 493, 1942.
- Taylor, D. V.: “A Case of Atrophy of the Mandible Associated With Scleroderma,” D. J. 87: 216, 1949.
- Albright, F., Bloomberg, E., and Smith, P. H.: “Post-Menopausal Osteoporosis,” Am. Physicians 55: 298, 1940.
- Albright, F., Smith, P. H., and Richardson, A. M.: “Post-Menopausal Osteoporosis: Its Clinical Features,” A. M. A. 116: 2463, 1941.
- Albright, F., Smith, P. H., and Fraser, R W.: “A Syndrome Characterized by Primary Ovarian Insufficiency and Decreased Stature; Report of Eleven Cases With a Digression on Hormonal Controls of Axillary and Pubic Hair,” J. M. Sc. 204: 625, 1942.
- Fraser, R. W., and Smith, P. H.: “Simmond’s Disease or Panhypopituitarism (Anterior);j Its Clinical Diagnosis by the Combined Use of Two Objective Tests,” J. Med. 10: 297, 1941.
- Shwachman, H., and Gould, B. S.: “Blood and Tissue Phosphatase in Experimental Scurvy,” J. Dis. Child. 64: 949, 1942.
- Wolbach, S. B.: “The Pathologic Changes Resulting From Vitamin Deficiency,” A.M.A. 108: 7, 1937.
- Williams, R. H., and Morgan, H. J.: “Thyrotoxic Osteoporosis,” Clin. 2: 48, 1940.
- Kinsell, L. W.: Hertz, S., and Reifenstein, W. C., Jr.: “The Effect of Testosterone Compounds Upon the Nitrogen Balance and Creatine Excretion in Patients With Thyrotoxicosis,” Clin. Invest. 23: 880, 1944.
- Mittleman, J. S.: “Osteogenesis Imperfecta (Odontogenesis Imperfecta),” Oral Surg., Oral Med. & Oral Path. 3: 1562, 1950.
- Winter, G. R., and Maiocco, P. D.: “Osteogenesis Imperfecta and Odontogenesis Imperfecta,” Oral Surg., Oral Med. & Oral Path. 2: 782, 1949.
- Albright, F., and Stewart, J. D.: “Hypovitaminosis of All Fat-Soluble Vitamins Due to Steatorrhea; Report of a Case,” New England J. Med, 223: 239, 1940.
- Bauer, W., Marble, A., and Claflin, D.: “Studies on the Mode of Action of Irradiated Ergosterol. I. Its Effect on the Calcium, Phosphorus, and Nitrogen Metabolism of Normal Individuals,” Clin. Invest. 11: 1, 1932.
- Weinmann, J. P.: “Bone Changes in the Jaw Caused by Renal Hyperparathyroidism,” Periodont. 16: 94. 1945.
- Lighterman, T.: “Renal Osteodystrophy With Oral Manifestations,” Oral Surg. 10: 238, 1952.
- Snapper, I.: Medical Clinics on Bone Diseases, New York, 1949, Interscience Publishers, Inc., P. 134.
- Keating, F. R, Jr., and Cook, E. N.: “The Recognition of Primary Hyperparathyroidism; an Analysis of Twenty-four Cases,” A. M. A. 129: 994, 1945.
- Schneider, W.: “Hyperparathyroidism (Generalized Osteitis Fibrosa),” Oral Surg., Oral Med. & Oral Path. 6: 745, 1953.
- Bruce, K. W., and Royer, R. Q.: “Multiple Myeloma Occurring in the Jaws: a Study of Seventeen Cases,” Oral Surg., Oral Med. & Oral Path. 6: 729, 1953.
- Meloy, T. M., Gunter, J. H., and Sampson, D. A.: “Mandibular Lesion as First Evidence of Multiple Myeloma,” J. Orthodontics & Oral Surg. 31: 685, 1945.
- Salman, I., and Langel, I.: “Metastatic Tumors of the Oral Cavity,” Oral Surg., Oral Med. & Oral Path. 7: 1141, 1954.
- Aisenberg, M. S., and Inman, C. L.: “Tumors That Have Metastasized to the Jaws,” Oral Surg., Oral Med. & Oral Path. 9: 1210, 1956.
- Thoma, K. H.: Oral Pathology, ed. 4, St. Louis, 1954, The C. V. Mosby Company, p. 421.
- Shafer, W. G., Hine, M. K., and Levy, B. M.: A Textbook of Oral Pathology, Philadelphia, 1955, W. B. Saunders Company, p. 356.
- Bluestone, L. I.: “Malignant Melanoma Metastatic to Mandible,” Oral Surg., Oral Med. & Oral Path. 5:237, 1953.
- Baxter, H.: “A Review of Malignant Melanoma of the Mouth,” J. Surg. 51: 379, 1941.
- Gardner, W. U., and Pfeiffer, C. A.: “Influence of Estrogens and Androgens on the Skeletal System,” Rev. 23: 139, 1943.
- Smith, A. G., and Zavaleta, A.: “Osteoma, Ossifying Fibroma, and Fibrous Dysplasia of Face and Cranial Bones,” Path. 54: 507, 1952.
- Wilkinson, F. C., and Pollack, E.: “Benign Bone-Forming-Tumors of the Jaws,” D. J. 77: 341, 1944.
- Seigman, E. L., and Kilby, W. L.: “Osteopetrosis,” J. Roentgenol. 63: 865, 1950.
- Kneal, E., and Sante, L. R.: “Osteopetrosis (Marble Bones); Report of Case With Special Reference to Early Roentgenologic and Pathologic Findings,” J. Dis. Child. 81: 693, 1951.
- Thoma, K. H., Rowe, H. D., and Wenig, M.: “Osteomyelitis,” J. Orthodontics & Oral Surg. 31: 235, 1945.
- Wilensky, A. O.: Osteomyelitis; Its Pathogenesis, Symptomatology and Treatment, New York, 1934, The Macmillan Company, p. 380.
- Stafne, E. C., and Austin, L. T.: “A Study of Dental Roentgenograms in Cases of Paget’s Disease (Osteitis Deformans), Osteitis Fibrosa Cystica and Osteoma,” Am. Dent. A. 26: 1202, 1938.
- Albright, F., and Reifenstein, E. C., Jr.: The Parathyroid Glands and Metabolic Bone Disease, Baltimore, 1948, Williams & Wilkins Company, p. 284.