
Access to all articles, new health classes, discounts in our store, and more!
Reported Psychologic Symptoms and Signs Before and After Dietary Counsel
Published in ACA Journal of Chiropractic, Vol. 13, No. 6, July 1976.
* * *
The following article was presented to the chiropractic profession by Dr. Cheraskin through the ACA Council on Nutrition. The council was instrumental in obtaining this original monograph by Drs. Cheraskin and Ringsdorf, Jr.
The evidence presented in this report suggests that the course of emotional disease can be altered. The data offered here indicate that a stopping, slowing, or reversal in psychologic state can be effected during the incubation period of chronic emotional disease. Finally, the changes made, in part, can be possible by relatively simple dietary means.
Introduction
One of the characteristics of the aging process is the progressive increase in symptoms and signs. Initially, and this is most prevalent in the younger years, the clinical findings are seemingly unrelated (Figure 1). For example, there is a symptom in one organ system and a sign in another area. With time, the findings become more numerous and more localized in one or another site. Finally, the symptoms and signs crystallize, according to textbook description, so that a diagnosis of a specific syndrome (e.g., arthritis, cancer, heart disease, schizophrenia) is possible.
Clearly, the optimal point to interrupt the pattern is early during the amorphous period. However, the evidence at this stage is subtle, and the changes can only be minimal.
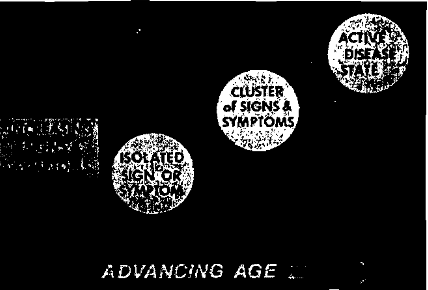
Figure 1. The clinical sequence of events in chronic disease. At first, there are few and diverse symptoms and signs (circle on the left). With time, the findings become numerous and localize in a system or organ (middle circle). Finally, the clinical evidence fits the textbook picture of a particular disease or syndrome (circle on the right).
Evidence was presented earlier1-3 that the course of disease can be altered early. First, the data offered indicated that a stopping, slowing, or reversal in the overall general symptoms and signs as well as in the gastrointestinal and cardiovascular areas can be effected during the incubation period of chronic disease. Second, the point was made that the changes may, in part, be ascribed to relatively simple dietary means.
This report examines essentially the same population exclusively in terms of psychologic symptoms and signs. Specifically, an attempt will be made to resolve the following three questions:
- What is the pattern of reported psychologic findings in presumably healthy subjects?
- Can the pattern be influenced by dietary counsel?
- Of what significance is this observation?
Method of Investigation
Eight-hundred nineteen dentists and their wives participated in this program. These individuals are currently sharing in a multiple testing program in Florida under the auspices of the Southern Academy of Clinical Nutrition, in Los Angeles under the direction of the Southern California Academy of Nutritional Research, in Columbus under the sponsorship of the Northeast Academy of Clinical Nutrition, and in the San Francisco area under the responsibility of the Northern California Academy of Nutritional Research.
At the initial visit, each subject completed the Cornell Medical Index Health Questionnaire (CMI).4 This is a self-administered form consisting of 195 questions to be answered “yes” or “no.” The questions are so structured that a positive answer suggests pathology. Sections M to R represent the psychologic questionnaire. Hence, by simply summing the number of affirmative responses in these sections, one can derive a crude estimate of psychologic state. Table 1 summarizes the data for the 819 individuals at the first visit.
Table 1–Analysis of Psychologic Scores (M-R section of CMI) at First Annual Visit for the Entire Sample
| M-R scores | first visit |
| 0
1-5 6-10 11-15 >15 total mean S. D. minimum maximum range |
250
340 133 51 45 819 4.2 5.6 0 41 41 |
Three points deserve particular mention. First, the average score for the entire group is 4.2. Second, the group values range from zero to 41 symptoms and signs. Lastly, data are available to indicate that psychologic complaints are clearly very common in this population. This is particularly noteworthy since there is evidence to indicate that, generally, health-conscious persons are more apt to participate in health-evaluation projects of this type.5,6
At the initial visit, each subject completed two dietary records. One consisted of recording all foods consumed for a seven-day period.7 A second form, called the Dietronics Dietary Analysis,8 is a simple questionnaire designed to determine the dietary habits based upon food frequency.9,10
The dietary forms are submitted to a computer center, and a printout is derived setting out the daily intake of the major foodstuffs and the vitamins and minerals.
The group reconvenes almost annually. At each reexamination, the Cornell Medical Index Health Questionnaire and the two dietary fonns are restudied.
Results
Question One: According to the designers of the Cornell Medical Index Health Questionnaire, three or more positive responses represent significant pathology. On this basis, and in answer to the first question, there seems to be a considerable amount of psychologic pathosis in this relatively young, socioeconomically privileged group of health practitioners and their wives.
Question Two: Following the collection of the initial data, discussions were conducted with the group to show the individual psychologic scores. Generally speaking, the groups consumed large amounts of refined carbohydrate foods, marginally low protein intake, and suboptimal amounts of vita. mins and minerals according to the Recommended Dietary Allowances set by the Food and Nutrition Board of the National Research Council in 1974.11 The lectures included methods for correcting the diet to provide for adequate protein, vitamins, minerals, and essential fats. They were published for health professionals under the title, “The Optimal Diet,” in the book, Diet and Disease (1968).12 The lectures were recently (1974) published for both laymen and health professionals under the same title in Psychodietetics: Food as the Key to Emotional Health.13
At subsequent visits, it was possible to compare the changes in the psychologic responses with the changes in the dietary habits. Table 2 summarizes the psychologic scores in the same 265 subjects at the initial visit and one year later.
Table 2–Paired Analysis of Psychologic Scores (M-R section of CMI)
| M-R scores | first visit | second visit |
| 0
1-5 6-10 11-15 > 15 total mean S.D. t P minimum maximum range |
63
122 47 1.5 18 265 4.8 6.0 7.910 <0.001* 0 38 38 |
102
118 36 6 3 265 2.8 4.3 7.910 <0.001° 0 36 36 |
* statistically significant difference of the means
The mean number of psychologic complaints decreased from 4.8 to 2.8, and this difference is highly statistically significant (t = 7.910, P<0.001). The range decreases slightly from 0 to 38 at the first visit to 0 to 36 at the second visit. A like analysis was done (Table 3) extending from the initial visit to two subsequent annual visits in 102 subjects.
Table 3–Paired Analysis of Psychologic Scores (M-R section of CMI)
| M-R scores | first visit | second visit | third visit | |||
| 0
1-5 6-10 11-15 >15 total mean S.D. |
25
55 10 5 7 102 3.9 4.8 |
33
53 14 2 0 102 2.5 2.9 |
40
47 12 3 0 102 2.3 2.9 |
|||
| t
P |
4.288
<0.001* |
1.124
>0.200 |
||||
| minimum
maximum range |
0
18 18 |
0
13 13 |
0
12 12 |
|||
*statistically significant difference of the means
The mean psychologic score decreased from 3.9 to 2.5 during the first year, and this decrement is highly significant (t = 4.288, P<0.001). However, the decline between the second and third visit is small on a mean basis (2.5 to 2.3) and not statistically significant (t = 1.124, P > 0.200). Hence, in answer to the second question, psychologic state apparently can be significantly altered by simple dietary instructions with the maximal change, under these conditions, occurring during the first year.
Discussion
Question Three: Earlier mention was made that, with advancing age, there is an increase in psychologic symptoms and signs. This is generally regarded as the natural course of events (Figure 2). What is usually not emphasized is that the variance also increases with age. Thus, there are some older subjects with fewer psychologic findings than some younger people. This suggests that, while it may be normal (average) to display more psychologic findings with time, it may not be physiologic (healthy).

Figure 2, The relationship of age (on the x-axis) and reported psychologic findings (on the y-axis). On the average, with time, the mean scores rise. However, there is considerable variation (gray area) as shown by the fact that some older subjects have fewer findings than some younger people.
The additional point is that the line depicting the natural sequence of events (Figure 3) can be altered. In some, the clinical course can be slowed, in others probably stopped, and, in some, possibly reversed.
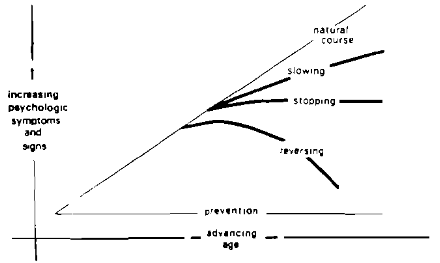
Figure 3. Present day curative medicine attempts to alter the natural course of disease by slowing, stopping, or reversing the psychologic symptoms and signs. In a sense, this is secondary prevention (prevention of recurrence). Primary prevention (prevention of occurrence) means to subtend an angle of zero.
References Cited:
- Cheraskin, E, and Ringsdorf, W. M Jr., “Reported Gastrointestinal Symptoms and Signs Before and After Dietary Counsel,” J. Med. Assn. State Alabama, 41(1): 21-26, July 1971.
- Cheraskin, E. and Ringsdorf, W. M., Jr. “Clinical Findings Before and After Dietary Counsel,” Geriatrics, 27(1): 121-126, January 1972.
- Cheraskin, E. and Ringsdorf, W. M., Jr., “Reported Cardiovascular Symptoms and Signs Before and After Dietary Counsel,” Alabama J. Med. Sci., 9(2): 174-179, April 1972.
- Brodman, I., Erdman, A. J. Jr. and Wolff, H. E Cornell Medical Index Health Questionnaire; Manual, New York, Cornell University Medical College, 1949.
- Editorial. “ADA Health Screening Program for Dentists,” J. A. D. A., 79(2): 235, August 1969.
- Cheraskin, E. and Ringsdorf, W. M., Jr., Predictive Medicine: A Study in Strategy, Mountain View, CA, Pacific Press Publishing Association, 1973.
- Dicalator System, P. O. Box 3217, Olympic Station, Beverly Hills, CA 94710.
- Dietronics Dietary Analysis, Hanson Research Corporation, P. O. Box 35, Northridge, CA 91324.
- Abramson, J. H., Slome, C, and Kosovsky, C, “Food Frequency Interview as an Epidemiological Tool,” Amer. J. Pub. Health, 53(7) 1093-1101,1963.
- Marr, J, W., Heady, J. A., and Morris, J. N., “Towards a Method for Large Individual Diet Surveys,” London, Third International Congress of Dietetics, 1961.
- Food and Nutrition Board, National Research Council, Recommended Dietary Allowances, 8th ed., Washington, D. C., National Academy of Sciences, 1974.
- Cheraskin, E., Ringsdorf, W. M., Jr. and Clark, J. W., Diet and Disease, Emmaus, PA, Rodale Press, Inc., 1968.
- Cheraskin, E. and Ringsdorf, W. M., Jr., Psychodietetics: Food as the Key to Emotional Health, New York, Stein and Day Publishers, 1974.