
Access to all articles, new health classes, discounts in our store, and more!
Principles Which Govern Reflex Action in Disease
Published in Transactions of the American Therapeutic Society, Vols. XXVIII and XXIX, 1927-1928.
* * *
An understanding of the principles of the reflex is essential to the understanding of disease, yet no effort commensurate with its importance is made to understand the subject. Certain reflexes arising and ending in the voluntary structures are described in all text books, but the visceral reflexes receive very little discussion except in the writings of physiologists.
Disease expresses itself in symptoms. Symptoms are disturbances of normal physiology. A disease can rarely be suspected by the one affected until it begins to produce changes in physiologic action, such as discomfort, pain, or a disturbance in function of some organ, as the eye, heart, lungs, stomach, intestines, liver or kidney.
In order to understand the part played by the reflex in disease it is necessary to understand to what processes activity in the body is due. Activity of cells is automatic. In the viscera it exists independently of nerves and hormones, and takes place normally as long as their protein and lipoid masses are bathed in the physiologic salt containing body fluids.
The hormones or chemical messengers are not for the purpose of causing action but of altering the action established by certain cells. They are more selective than the electrolytes found in normal body fluids. Apparently, calcium on the one hand and sodium and potassium on the other bear a share in the activity of all cells of the body. They antagonize each other and when rightly balanced keep cellular activity within the bounds of physiological equilibrium. The hormones on the other hand, through selective action, affect certain activities to the exclusion of others. They, however, form the chemical system for correlating activity in different parts of the body, and are thus a part of the mechanism which is provided for serving the more complex organisms.
Function of the Nervous System
The nervous system, however, is the chief correlating and integrating system of the body, and causes a very complex organism made of many parts to function as a unit. From the central nervous system fibers go out to every muscle and gland cell in the body. The neurons going to the body cells are of two kinds; one for picking up stimuli and carrying them centralward, the other for translating stimuli into action. Every afferent neuron which carries stimuli centralward ends in the posterior root ganglion of the cord and the part which corresponds to it in the brain. From here the stimulus is carried further into the central nervous system by what are termed connector or intercalated neurons. Through these connector fibers every afferent neuron is able to join with every efferent neuron of the body. Thus is established a mechanism which is able to bring every part of the body into a close and harmonious relationship during conditions of physiologic activity; and, thus is established, furthermore, a mechanism which is able to produce disharmony through reflex effects in any and every part of the body during conditions of pathologic activity.
While the body cells can function without nerves, yet their action is under the influence and control of nerves. There is a difference in the nerves supplying different structures. Thus we have the voluntary nerves supplying the skeletal structures and the involuntary or vegetative nerves supplying the visceral structures. The latter supply all smooth muscles and secreting cells, and in supplying the blood vessels go to every part of the body. The vegetative system is shown in Figure 1.
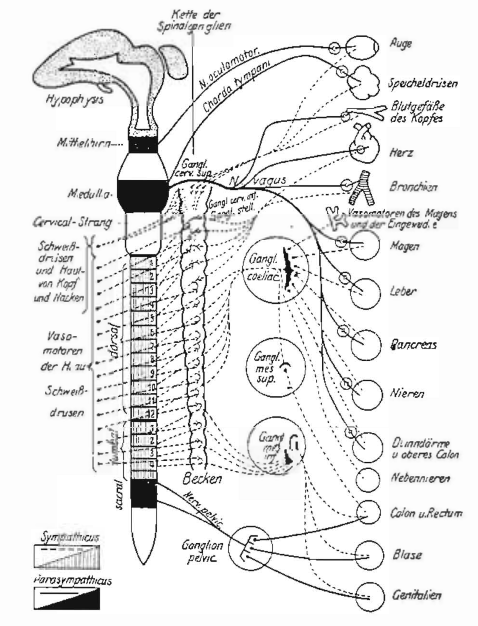
Fig. 1. Schematic illustration of the distribution of the two components of the vegetative nervous system, showing its division into sympathetic and parasympathetic and their branches to the various organs.
The thoracolumbar portion of the cord, which gives origin to the sympathetic nervous system, is represented by lines. The portions of the midbrain and medulla, and sacral segments of the cord, which give origin to the parasympathetic system, are represented in black. The peripheral nerves belonging to the parasympathetics, are shown as solid black lines, while those belonging to the sympathetic system are shown as broken lines. This chart shows the double innervation of the structures of the head, heart, and the entire enteral system, and likewise indicates the single innervation for the blood vessels, pilomotor muscles and sweat glands of the body. (Symptoms of Visceral Disease)
There is a free and intimate communication between the various neurons of the voluntary system with each other, and the various neurons of the vegative system with each other, and the various neurons of the voluntary system with the various neurons of the vegetative system, which binds together visceral and skeletal structures in such a way that action under either physiologic or pathologic conditions in one organ or structure of the body may influence other organs or structures through reflex action.
Whenever disease exists in the body it alters function in few or many structures. It may produce its effects in several different ways. It may be an infection producing bacterial toxins. It may exert a destructive action on certain tissues and cause toxins to be liberated from them. It may interfere with the action of some important organ so that it fails to do its work and allows a retention of poisonous products to circulate in the body fluids. It may exert an injurious effect locally because of its assuming an inflammatory nature. Lastly, it may disturb function in other viscera reflexly.
We must attempt to find out in what way function is disturbed as a result of the above mentioned harmful influences. We assume that toxins which circulate generally produce harmful effects on the cells throughout the body. This affects to a varying degree the automaticity of the cells themselves and further affects them in the aggregate as found in definite structures and organs. Thus we assume that higher centers in the central nervous system, the nerves themselves, as well as glands, muscles and other peripheral structures, come in for injury from toxins.
Through their effects on ganglia in the central nervous system toxins produce harmful stimuli which are sent peripheralward, where they produce dysfunction. This is evident in cases of general toxemia where the equilibrium of the entire vegetative system is disturbed. The chief peripheral effect, however, is that of an oversympathetic stimulation. The reflex is most evident in disease caused by definite organic inflammation. In such instances the inflammatory process causes stimulation of the sensory neurons whose receptors are found in the tissues affected by the pathologic process, beyond the degree of stimulation which is usual for that organ or tissue in health. These excessive stimuli cause impulses to be carried centralward and to be transmitted to efferent neurons which translate them into action, often excessive, in other structures.
This excessive action is represented as symptoms of disease. It may be a pain, or a muscle contracture, or disturbed secretion in some gland. The reflex activity may affect only one organ or it may extend widely according to laws which we shall discuss later.
There are several groups of reflex symptoms possible in the presence of disease, such as: (1) from one part of the voluntary system to another part of the same system, as is met in inflammation of a joint; (2) from the voluntary system to the vegetative system, the principle of which is utilized when heat or blisters are applied to the surface of the skin in order to influence internal organs; (3) from the vegetative system to the voluntary system, as is illustrated by the muscle spasm in skeletal muscle in the presence of visceral inflammation; and (4) from the vegetative system to the vegetative system, as is witnessed so often in visceral inflammation and is especially well known in the so-called functional symptoms which affect one part of the gastrointestinal canal when another part or a neighboring organ is the seat of inflammation.
Types of Reflexes Met Clinically
Reflexes commonly met in clinical practice are: (1) the motor reflex in case of visceral disease, such as the spasm of the muscles of the abdomen in appendicitis, gall-bladder disease, and ulcer of the stomach; of the muscles of the shoulder girdle and diaphragm in tuberculosis of the lung; of the intercostals in pleurisy; and of the lumbar muscles when the kidney is inflamed as in tuberculosis of that organ; (2) the sensory reflex or pain which is referred to the surface of the body when important viscera such as the appendix, gall-bladder, stomach, pancreas, urinary bladder, kidney, ureter, heart, lungs and pleura are inflamed (this is not a true relex, physiologically, but may be so classed clinically); (3) the tropic reflex which shows as a degeneration of tissue when nerves have long been irritated by excessive stimuli, such as is best illustrated by the atrophy which takes place in the muscles and skin and subcutaneous tissue innervated by those cervical nerves which express reflexly the stimuli arising in the lung in chronic pulmonary tuberculosis; and (4) the motor and secretory reflexes which are usually spoken of as functional symptoms for which the stimuli arise in one organ and are expressed in another, such as the motor and secretory changes in the gastrointestinal canal caused by inflammation of the appendix, gall-bladder, stomach (ulcer), lungs, heart, kidney and genitourinary organs, or the asthma resulting from nasal irritation and the cardiospasm and pylorospasm which result from various visceral irritations.
Nature of Reflexes
Reflexes may be comparatively simple or very complex. While a reflex requires only three components: a sensory receptor to pick up the stimulus, a motor effector to translate the stimulus into energy, and a synapse, where the stimulus is transferred from receptor to effector, yet such a simple arrangement is probably never found. There are usually several and more often many neurons interposed between the receiving and affecting nerve. Therefore reflexes are, as a rule, quite complex.
The complexity of reflex action is provided for by the multiplicity of connector neurons in the central nervous system as previously mentioned, which connect the incoming nerve bearing the stimulus with all motor nerves of the body. This widespread connection is seen in strychnia poisoning where the resistance at the synapses is broken down and universal contraction of muscles may be reflexly affected from irritating any afferent neuron.
While widespread efferent paths are open to all stimuli, yet most reflexes arising in definite tissues and organs are expressed in certain other definite areas, according to a well established law and when a departure from this regular course takes place, it too, follows definite laws which will be discussed later.
Segmental nature of reflexes. In order to understand visceral reflexes we must acquaint ourselves with the embryologic development of the body, for here alone can we acquire a comprehension of the segmental relationships which are fundamental to understanding the reason why action in a given tissue or organ, or a definite skeletal area, is expressed as a result of impulses arising in other definite tissues or organs. It is quite easy to understand the segmental relationships of such organs as the heart and stomach in prevertebrate life where underlying viscera and overlying skeletal structures are innervated by nerves from a corresponding cord segment, as may be inferred from Figure 2, in which each segment is complete in itself; but to understand the relationships of the viscera in the thorax and abdomen through the cranial nerves to the somatic structures of the head is not so obvious; yet it follows the same segmental law of body development.
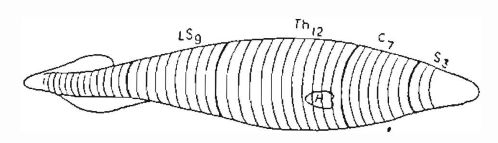
Fig.2. Diagrammatic representation of a primitive vertebrate animal–the amphioxus, divided for convenience into three segments for the head, seven for the neck, twelve for the thorax, nine for the lumbosacral region, and an indefinite number for the coccygeal region.
For clearness of comparison the heart (H) is represented as occupying the same position as in man, so that an adequate stimulus from the heart would cause pain in the distribution of the four upper thoracic nerves covering and protecting the heart. (Ross and Mackenzie.)
In vertebrates segmentation for striated and unstriated muscle, as the relationship is shown through spinal and sympathetic neurons, is evident throughout the entire length of the body. The lateral ganglia send connector fibers segmentally to the smooth dermal muscles just as the anterior roots supply the striated muscles of the body. Furthermore, connector fibers pass peripherally to visceral musculature through definite ganglia, thus connecting them segmentally with the somatic segments. The segmental relationship in man may be seen best in the embryo as illustrated in Figure 3.
The segmental relationship between the somatic and endodermal musculature in the vertebrates, as the relationship is shown through the cranial and parasympathetic neurons, however, is just as regular. The endodermal musculature was derived from the appendicular unstriated musculature of the invertebrate which was closely related segmentally to the head and face muscles. Thus in evolution, vagus innervation, which was related to definite somatic head and face segments in the invertebrate was carried as far as the colon as it developed into the digestive tube of the vertebrate.
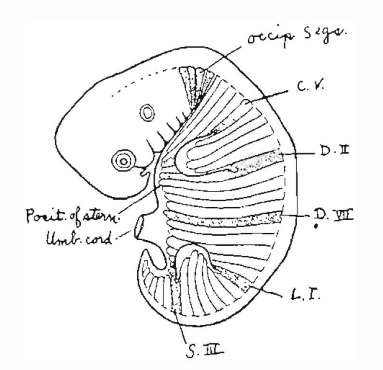
Fig. 3. Diagram of a human embryo, fifth week, showing the arrangement and extension of the mesoblastic segments.
The first and last of each segment entering into the formation of the limbs is stippled (C.V. and D.II, and L.I. and S.III). The position is indicated in which the sternum is formed. (A. M. Patterson.)
So we must understand the striated skeletal musculature, the smooth dermal musculature and the visceral musculature, all as being related segmentally in such a manner that the relationships in the more primitive organisms are preserved in the vertebrate.
Reflexes are primarily segmental because the neuron connections of tissues belonging to the same segment are most closely connected. From a clinical standpoint this is extremely important for it points the way for interpreting reactions which accompany disease.
One can interpret the origin and expression of reflexes only as one understands the manner in which the body has developed from more simple segmental organisms; and can understand them only by possessing a knowledge of the physiologic laws which govern reflex action.
The Laws of Reflexes
The law of the minimal stimulus. Sensory end organs in tissues are being subjected to stimulation more or less constantly; but they withstand a certain strength of stimulus before they pick it up and carry it centralward. All stimuli which are insufficient to affect the sensory receptor are called subminimal. The one which is just sufficient to affect it is called the minimal stimulus. Subminimal stimuli, if repeated in sufficiently rapid succession, are raised to minimal or even above, and cause impulses to be carried to the higher centers.
Each tissue or organ develops sense organs capable of picking up the particular type of sensory stimuli to which that tissue or organ is subjected. The somatic receptors are thus able to pick up and translate into their proper sensory manifestations such forces as heat, cold, light, sound, pinching, cutting and pressure, because the skin naturally comes in contact with all such forces and must develop the sensory end organs for them as a matter of defense. The internal viscera, on the other hand, do not meet conditions which require the development of many types of sensory receptors. The viscera normally never come in contact with such forces as heat, cold, light, sound, pinching and cutting, consequently have no sensory apparatus to pick up this type of stimulus. In order to carry impulses centralward the particular receptor found in an organ must be excited by the particular stimulus which it is designed to convey and the stimulus must be at least minimal in strength. The term adequate stimulus is used to designate that the stimulus is of a quality to excite action. A stimulus can not produce reflex action unless it be both adequate and at least minimal.
Sherrington’s law of segmental proximity. Sherrington enunciated a law which governs the production of spinal reflexes as follows:
“Broadly speaking the degree of reflex spinal intimacy between afferent and efferent spinal roots varies directly as their segmental proximity.”
And then, by way of making the law more explicit he says:
“Taken generally, for each afferent root there exists in immediate proximity to its own place of entrance in the cord (e.g. in its own segment) a reflex motor path of as low a threshold and of as high potency as any open to it anywhere.”
I have suggested that in order to make this law complete it should be understood that this relationship of afferent and efferent neurons in the cord preserves developmental relationships; then, it will apply to all viscera, including the lung which otherwise would be an exception, since its skeletal reflexes take place through cervical nerves (the union being completed by intercalated neurons), although the afferent impulses enter the cord through the upper five or six thoracic segments.
The somatic segmental nerves in which reflexes from the principal organs are expressed, according to Sherrington’s law, may be inferred from Figure 4, in which their sympathetic innervation is shown.
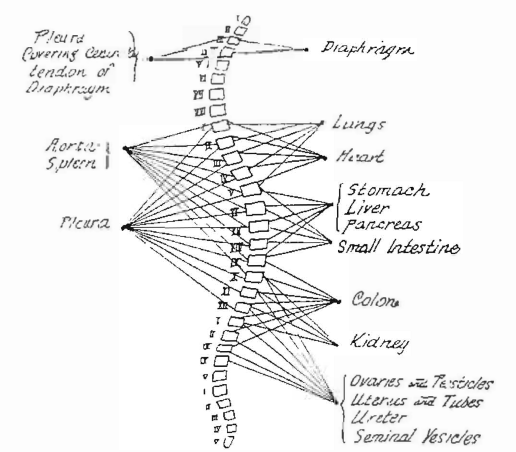
Fig. 4. The connector neurons for the important Thoracic Abdominal, and Pelvic Viscera
In the figure the connecting neurons are those which belong to the thoracolumbar outflow; except those going to the diaphragm, which are spinal nerves (phrenics). The motor cells for the viscera are found in the various collateral ganglia.
The figure shows that the innervation of the various viscera may be divided into groups. The heart and lungs are innervated from practically the same segments, the upper Ist to VIth thoracic. The stomach, liver, and pancreas from the same segments, Vth to IXth thoracic. The colon, kidney, and pelvic viscera from practically the same segments, IXth and Xth thoracic to IIIrd and IVth lumbar.
In spite of this grouping in innervation, each organ is brought in reflex connection with efferent neurons, both sensory and motor, which are more or less definite, in such a way that the motor and sensory reflexes do not overlap as much as might be indicated. (Symptoms of Visceral Disease)
Law governing the spread of reflexes. When a stimulus is sufficient to discharge reflex activity over certain efferent neurons it produces as much activity in the skeletal muscle fibers innervated by those particular neurons as though the stimulus were many times stronger, according to the “all or none’” law of activity. That is, when a muscle fiber contracts it produces a maximal contraction. A stronger stimulus can not make its contraction stronger but can express itself only by causing activity in more muscle fibers.
The corollary to this muscular action is that a minimal stimulus affects a minimal number of efferent nerve fibers, while a maximal stimulus spreads to many, thus widening the extent of the reflex.
Visceral Pain
Visceral pain in a physiologic sense is not a reflex but from the clinical standpoint we may be allowed to discuss it as such.
Most confusing to students is the fact that sharp visceral pain is not in the organs affected; but such is true, as may be readily seen in the pain in the arm caused by angina, and pain in the epigastric region in ulcer oi the stomach, whether the stomach has a high position as in individuals of sthenic build or is found at the pelvic brim, as in individuals of hyposthenic build, as pointed out years ago by Mackenzie.
There is a feeling of pressure or distention, and one of contraction, in such viscera as the stomach and intestines that may be noted and found directly in the organ according to Head. But a true sharp pain can not be expressed by the sensory receptors of viscera which have never come in contact with or developed a sensory organ for detecting such sensations.
Head has announced the following law governing visceral, or referred pain:
“When a painful stimulus is applied to a part of low sensibility in close central connection with a part of much greater sensibility, the pain produced is felt in the part of higher sensibility rather than in the part of lower sensibility, to which the stimulus was actually applied.”
It should further be noted that the projection of referred pain follows the same laws of the segmentation of the body as is followed by the visceromotor reflex.
In harmony with the preceding discussion, it can be seen that the visceral nerves must be very active in conditions of disease. They are disturbed by all toxemias, and they are irritated whenever a tissue or organ is inflamed. If the stimulation is sufficient, it is followed by action in some or many other tissues and organs. Such action is abnormal although it follows the usual nerve paths. It is recognized as a part of the symptom-complex of the particular disease in question.
The best preparation for appreciating visceral reflexes is an understanding of the vegetative nerves, and the laws which govern reflex action. There are certain reflex disturbances in organs which can be produced by stimuli coming from many sources. Instances are cardiospasm and pylorospasm, which may be caused by stimuli from many organs such as the lung, gall-bladder, appendix, stomach and intestines, urinary bladder, kidney or generative organs. The stimuli from the different organs here mentioned will enter the cord at all levels from the first dorsal to the upper two or three thoracic segments, but no matter where they enter, before mediation with motor neurons occurs, the impulses will be carried to that part of the cord, thoracic segments 5 to 10, from which the nerves supplying the pyloric and cardiac sphincters arise.
The fact that stimuli arising in so many organs can cause disturbed function in a single organ, and stimuli from a single organ can cause reflexes in so many organs, is very confusing in itself, but there are always other symptoms, very often other reflexes, which will help to indicate the organ which is diseased. Every important organ has through its afferent sympathetic nerves and their connection in the cord with spinal nerves particular areas for expressing reflexes in the skeletal structures, which are fairly definite, because they follow the laws of segmental relationship.
In my book on Symptoms of Visceral Disease I enunciated the following law as governing the subject of visceral reflexes expressed in skeletal structures:1
“Every important internal viscus is so connected in the central nervous system that it is able to produce reflexes through afferent sympathetic and efferent spinal nerves with definite skeletal structures; and if acutely inflamed, should show motor reflexes and altered sensation (pain), and if chronically inflamed, trophic changes. Therefore, spasm of muscles, altered cutaneous sensation, and degeneration of muscles, subcutaneous tissue and skin in areas having definite limited segmental innervation become important diagnostic phenomena.”
While the laws herein discussed as governing reflexes hold in most instances, yet reflexes sometimes fail to follow such laws. Fortunately, we have learned some of the important reasons for such failure. We find causes at every physiologic level of the individual. The first cause may be in the cell itself. The electrolytes in the cell may not be present in proper proportion. It has been shown in the experimental heart, for example, that if calcium is in excess in the cell, stimulation of the sympathetic nerves may cause inhibition instead of acceleration.
Again the relative acidity of the tissues makes a difference in nerve reaction and might make uncertainty in reflex action.
Different hormones produce selective action on certain body cells and when greatly in excess or markedly deficient might throw these cells into disharmony which in turn might be reflected in any reflex action which was to be expressed in these tissues.
The nerves themselves become hypersensitive at times, their threshold of response becomes lowered and action takes place as a result of what under ordinary conditions would be subminimal stimulation. This is often met in clinical practice. We see it particularly in the toxemias of various kinds and in nerves which have been subject to prolonged stimulation, as occurs in such chronic conditions as pleurisy, pulmonary tuberculosis, pelvic troubles and chronic kidney inflammation. The neurons connected with these organs become so easily affected, that is, their threshold of response becomes so lowered, that pain or discomfort is shown whenever any marked physiologic adaptation is required of the patient. Under conditions of tiring, worry, changes in weather, or other disease, the neurons connected with the particular, injured organ, respond with pain or discomfort, while sensory neurons from other structures react normally, so that as far as they are concerned the individual is entirely unaware of the extra load.
Last but not least, reflexes are altered by emotions. Through such harmful emotions as fear, anger, worry, disappointment, discontent, and unhappiness nerve reaction becomes altered, and this manifests itself in changes in the reflexes which are brought about by disease. In the presence of such emotions, reflex action is often exaggerated. We see this in the various disturbances of function in internal viscera and the exaggeration of referred pain.
If man were a machine instead of a thinking, emotional, physiologic and pathologic human being, our problems would be more like test-tube reactions, more certain but less interesting. It is the quest for the hidden, the concealed, the desire to understand the vagaries in man’s reactions that make the study of medicine so interesting and so worth while. With a knowledge of the vegetative nervous system, an understanding of the physiologic action of the body cell, an acquaintanceship with the laws of the reflexes, and the factors which act to prevent reflex activity from following these laws, we have at our hand the key to the solution of many of our diagnostic and therapeutic problems.
Discussion
Secretary Mallory: Mr. Chairman, I should like to discuss Dr. Pottenger’s paper. First, I wish to express my appreciation of it. He certainly gives us an illustration of the rare faculty of a man who can condense his ideas and words. He has given us in this very brief paper the gist of the whole text on the subject.
This impresses me as being very important and appropriate to present before the Therapeutic Society, because it gives us a rational point of approach to the real philosophy of therapeutics.
In the first place this undoubtedly is a method of interpreting the origin and mechanism of symptoms and thereby comes to a just conception of the real nature of the disease process with which we wish to deal.
The second point is that that very understanding leads us to what I consider the philosophy of therapeutics, the understanding of the vicious process and brings about a physiological reversal of the process very much as the chemists bring about a reversal of certain chemical processes.
The immediate inference from Dr. Pottenger’s paper was largely interpretative and diagnostic, but I should mention one or two points in which I think it is also of definite therapeutic value.
In the matter of symptoms referable to the abdomen, to the stomach, and the whole digestIve tract, it has been my experience repeatedly to have to survey and examine patients with persistent and continual digestive disturbance, and on the most thorough survey that a whole team can give them, nothing will be found, but these were patients who for the past five or eight or ten years had carried diagnosis of pulmonary tuberculosis minimal, or pulmonary tuberculosis active, chronic tuberculosis, pulmonary tuberculosis arrested. The present examination by the internist would perhaps give them dry pleurisy or the diagnosis of pylorospasm or colonospasm, and I am glad to hear Dr. Pottenger mention that because I had felt a little hesitation in making such a diagnosis and attributing it to such a cause, and I certainly agree with him on that.
There is one other important application of this that I believe should be appreciated a little more widely. Post-operatively we see in patients who have had abdominal operations, some very acute and alarming situations develop, and the question arises whether they really have a post-operative obstruction or not. Sometimes that stormy period goes over successfully. Sometimes it does not, and I have seen two autopsies upon patients who died with all the symptoms and signs of intestinal obstruction who at the examination showed no intestinal obstruction but collapse and no fault with the operation, no leakage, no infection, but diseased gallbladder or stone in the kidney.
That may sound a little bit remote, but not long ago I saw a report in literature of this type. A woman who had had a pelvic operation, not on the digestive tract, shortly afterwards, in a few days, developed an illness with evidence and signs of obstruction. A consultation was held, the internes, the surgeons and others, and it was finally decided after all the ordinary measures of producing a movement of the bowels had failed, that intestinal obstruction was present and operation was imperative, but as the patient had also developed bronchial pneumonia, it was decided to perform the operation under spinal anesthesia. Within a few minutes after the anesthetic had been injected there was a copious movement of the bowels and the patient made complete recovery without any operation for intestinal obstruction. I have seen two or three who were considered for opening the abdomen that were relieved by the use of a drug that the pharmacologists say causes inhibition of action of the vagus thus reducing activity in the involuntary muscles of the tract, namely, belladonna. I won’t report the cases in detail, but they had the same finding that occur in intestinal obstruction, except that under intensive belladonna treatment the symptoms subsided and the fecal vomiting was no longer present, and the patients made good recovery.
So I feel that what Dr. Pottenger has presented to us is a thorough aid in diagnosing and leads up to a form of therapeutics that is thoroughly rational.
I enjoyed his paper very much, and I certainly hope aside from its publication in Transactions, I will have reprints from it. I am sure that many members of our profession are not utilizing the information that Dr. Pottenger has given us and that he has stated in his book. They are all leery of interpretations and actions based upon the sympathetic nerve system. They are afraid of that as they are of the endocrine system and probably with some reason, but there is still some well established information upon which we can base safe action, and I believe he has given it to us.
Chairman MacCready: Is there any further discussion? Dr. Pottenger, have you anything to add?
Dr. Pottenger: I wish to thank Dr. Mallory for his remarks. They are pertinent. Of course, our attitude toward things of this kind comes from a wrong frame of mind. Our medical mind has been dominated for fifty or seventy-five years bv the structural idea in Medicine. As physicians, on the other hand, we are constantly dealing with functional disturbance, but thinking in terms of structural change.
We have all seen physicians search for some important structural disease and not finding it consider that the functional disturbance was not worthy of attention. Functional disturbance is always worthy of consideration. The patient is just as sick with functional disturbances, so far as his feelings are concerned, as he is with some definite organic lesion. We have had too much of an idea that organic lesions must be removed, and that functional lesions will remove themselves.
A very interesting approach to Medicine is to consider disease according to its relationship to the vegetative nervous system. A very large group of individuals have a very delicate equilibrium maintained between the sympathetic and the parasympathetic systems. If the sympathetic nerves are predominant, we have one group of symptoms; if the parasympathetics are predominant, we have another. These two types of individuals react differently toward disease, and they react very differently from the individual who has a more stable balance. Take the individual of whom Dr. Mallory spoke. He would be very apt to show disturbances of a hypermotility in the gastrointestinal tract, due to his vagotonia. We must remember the vegetative nervous system is a system which carries impulses for reflexes from all the internal viscera. I very often see disturbances in the gastrointestinal tract which are produced by impulses arising in the lung. We all know how other disturbances in the gastrointestinal tract are produced by disease of the gall-bladder. Dr. Toland of Los Angeles recently described several cases of intestinal obstruction which were purely functional, resulting from disease of the gall-bladder. The reflex from the gall-bladder produced a block which, so far as symptomatology was concerned, was identical with an organic obstruction. I have seen pylorospasm produced by pulmonary tuberculosis many times.
If one only understands the nerves that supply an organ, and their connections in the central nervous system. then he knows where to look for reflex action; although he must always bear in mind that reflexes may be mediated higher or lower in the cord than the level at which the impulse enters, according to the law that I mentioned in my paper.
I often wonder that individuals are able to overcome the injury which results from an abdominal operation as easily as they do. Some will have a complete relaxation of the ileum; others will not. This is effected through reflex stimuli. Since different individuals have different nerve balance, so they react differently to disease, injury and emotional stresses. Physiologic equilibrium is distributed by many unrecognized factors. It is a strange thing to me that the profession has not recognized this fact to a greater degree. This condition may be illustrated by pain. This is very commonly experienced by people who have had inflammation in some important organ; for example: pleurisy, or pulmonary tuberculosis, or inflammation in the pelvic organs. Under many kinds of emotional or physical stress these pains may recur. I see them in my patients when they become worried, discontented, unhappy, tired from overdoing; also with changes in weather, and at the period time in women. We have long known that patients suffering from chronic rheumatism or neuritis show pain in weather changes, but it is also true that others do the same thing. Changes in weather require a great deal of compensation on the part of man in order to maintain a physiologic equilibrium. Patients with a poor nervous balance fail to compensate as they should; consequently they suffer from sleeplessness, increased nervousness, digestive disturbances, as well as pain, during weather changes.
We must learn to look at Medicine from a physiologic as well as structural basis. Part of the fault lies with our teachers of physiology. There has been entirely too much frog physiology, and not enough of human application. Physiology has been too far from clinical medicine, and the clinician has been too far from adequate physiology. Physiologists have the biggest opportunity in the world today, if they would only grasp it. Clinical Medicine is just beginning to recognize the importance of its physiologic basis, but neither clinicians nor physiologists seem to grasp it fully. But ere long there will undoubtedly be raised a group of psychologists who do recognize this fact and who will be able to teach physiologic change in Medicine the same as the pathologists have been able to teach structural change.
For the basis of physiologic Medicine we must study both inherited and environmental factors. We must know the cell, its development, its chemistry and physics, the internal secretions, and the vegetative nervous system.
The vegetative nervous system is a very complex system, and at the same time the truths which are necessary to be known for the understanding of critical Medicine are comparatively simple.
It is necessary to know that it is made up of two components, the sympathetic and parasympathetic, and that when any structure or organ is supplied by both, one produces action and the other inhibition of action. It is further necessary to know that different fibers course in each system and carry impulses which join in the central nervous system with other neurons to form reflexes, in both skeletal and visceral structures, according to laws which I have discussed in my paper. The nervous system must be understood as a correlating and integrating system which makes the body act as a whole instead of as so many units. Then with the knowledge of the innervation of the important organs, one has the basic acts for understanding much that takes place in the body during disease.
References Cited:
- Pottenger, F. M.: Symptoms of Visceral Disease. C.V. Mosby Co., St. Louis, 3d Edition, 1925.