
Access to all articles, new health classes, discounts in our store, and more!
Predictive Medicine XI. Prognostic Levels
Published in Journal of The American Geriatrics Society, Vol. 19, No. 12, 1971.
* * *
ABSTRACT: With a lamelleted sphere as a model, an analysis of the periphery of the human subject (symptoms and signs) is useful in providing a measure of the extent of disease. However, in itself, it has little utility in a predictive medicine program. In present multiple-testing methods, correlation of the biochemical state with the symptoms and signs is the basis for making a diagnosis of classical disease. However, the predictive potential is limited. A predictive medicine program, to fulfill its true purpose, must view the total sphere in all its layers.
“Physicians think they do a lot for a patient when they give his disease a name.” – Immanuel Kant
Ten previous reports in this series1 have dealt with the relationships of clinical symptoms and signs, electrocardiographic signs, the biochemical state, enzymes, diet, physical activity, and genetics. The question arises as to how these diverse factors fit into a predictive scheme.
In conventional medicine, the usual procedure includes a comparative analysis of a particular classical syndrome and its biochemical components. For example, in a multiple-testing program, considerable attention is directed to blood glucose levels in relation to diabetes mellitus.
Predictive medicine, concerned as it is with the anticipation of disease, has given rise to a unique experimental model. This is another feature which sets predictive medicine apart from conventional medicine.
Anatomy of Man in a Predictive Medicine System
Man may be viewed as a multilamellated sphere.2-4 Any way one turns a ball, it looks the same. In a sense, any way one inspects man from the outside, he is the same. True, viewed from a certain angle, one may see a limp characteristic of a cerebrovascular accident; viewed from a different angle, one may see pimples. But these and all other peripheral stigmata have a common denominator; each is an index of the syndrome of sickness (Fig. 1).
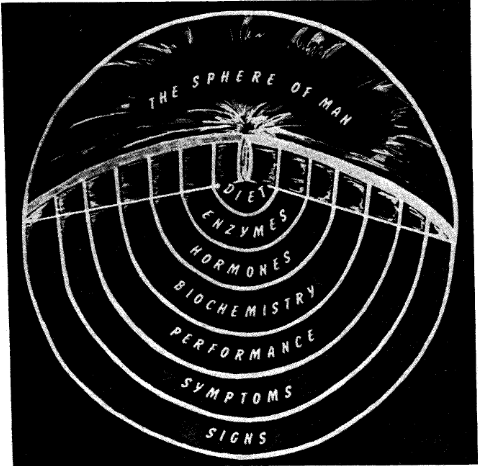
Fig. 1. Man may be likened to a lamellated sphere. The periphery is easily inspected. Layers can be removed which progressively expose the core.
A lamellated sphere permits the layers to be removed. In so doing, one eventually approaches the core. In man, layers may also be stripped away until the central problems are brought into focus (Fig. 1).
Signs. The outer, most peripheral, ring is readily inspected in both sphere and man. At this level, one can make three observations. First, one can identify evidence of the ravages of classical disease e.g., the pathognomonic gait associated with a cerebrovascular accident, the skin eruption typical of impetigo, or a carious tooth. This type of information fits into the category of “specific disease states” (see Figure 1 in article IV of this series; Reference 1).
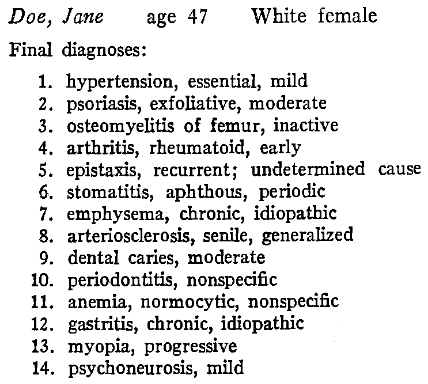
The end-product of such an analysis is demonstrated in Table 1. The patient had hypertension, the cause of which was unknown. There was emphysema, the etiology of which was not clear. The anemia could not be causally identified. This kind of diagnosis is simply an accounting of the damage, largely derived from a peripheral inspection of the human subject.
Table 1
Second, information derived at the peripheral level provides an estimate of the quality and quantity of symptoms and signs referable to a particular system (e.g., gastrointestinal) or site (e.g., eye) even though the findings do not fit the textbook description of a particular syndrome. This type of information fits into a category of “cluster of symptoms and signs in organ systems and/or anatomic sites” (Reference 1, article IV).
Lastly, one can simply establish the numbers and kinds of symptoms and signs without any regard for how or where they fit into systems or sites, i.e., sum the number of findings. This type of information fits into the category of “isolated symptoms and signs” (Reference 1, article IV).
Regardless of the information desired at this peripheral level, the data can be readily derived by physical examination and history-taking.
Symptoms. If one strips off the outer layer (Fig. 1), the zone of symptoms comes into focus. However, the line delineating where the outer layer ends and the next most peripheral one begins can be quite arbitrary. Symptoms are not as readily discernible as signs, and can be derived only through interrogation by means of a classical interview or questionnaire (e.g., the reporting of headaches, pain, or burning sensations in the mouth). The important point for predictive purposes is that symptoms generally precede signs of disease. Hence, evidence obtained in this zone may be regarded as prognostic of disease signs.
Performance. Stripping off the second layer reveals the world of performance (Fig. 1). Impairment of performance generally heralds disease symptoms and signs. Such information can be elicited from questionnaires dealing with physical, organ, and system performance. Physical activity is often used in the evaluation of organ and system performance (e.g., the treadmill in assessment of the cardiovascular system). The important point is that changes in performance precede the symptoms and signs of disease. Hence, this zone can be used effectively in a predictive medicine program.
Biochemical state. Removal of the performance layer brings into view the biochemical pattern. Illustrations would include blood sugar and serum fat determinations. This lamella is predictive for the three peripheral zones since biochemical imbalance antedates disturbances in performance and the advent of symptoms and signs. For instance, chemical diabetes mellitus characterized by disturbances in blood glucose concentration precedes the clinical diabetes mellitus by months and even years.
Hormonal balance. Removal of the biochemical layer brings into view the deeper hormonal area. Here are the measures of the endocrine state (e.g., serum protein-bound iodine level). Aberrations in the hormonal state precede changes in biochemical homeostasis; for example, the hypothyroid patient often is hypercholesterolemic. Hence, hormonal imbalances become predictive for the more peripheral layers because they produce metabolic disturbances.
Enzymes. Nearly at the center of the core is the enzyme pattern. Many of the 2,000 known enzymes can be measured. For example, determination of the serum glutamic oxalacetic transaminase (SGOT) level is often used as a predictive tool in impending cardiovascular disease. Since enzymes are essential for metabolism, enzymatic imbalance can be predictive of changes in every peripheral layer.
The core problems. The core, in Figure 1, is represented by diet. Since dietary nutrients are the building blocks from which enzymes are made, all the peripheral layers reflect dietary inadequacies or excesses. Physical fitness can also be regarded as a core problem (Reference 1, article X), and genetics must always be considered.
A Practical Application
There are countless illustrations to show the relative predictiveness of each layer of the sphere, since the layers are all interrelated. One such observation4 links physical fitness as the core problem with the more peripheral estimates of signs and symptoms (sick call).
The Officers Candidate School (OCS) at Fort Benning, Georgia, gives an intensive twenty-four week training program. At the start of the course, each student is graded in a number of intelligence and physical tests. One of the tests is the time required to run one mile. During the twenty-four week training period, a record is kept of a number of military and medical notes indicating the number of times each student reports for sick call. Figure 2 shows the relationship between the time required to run one mile and the frequency of sick call for 392 soldiers deemed healthy enough to be trained for officer status. The men who ran the mile fastest at the start of the program were the men who subsequently reported least for sick call. Conversely, those who were slowest in running the mile were those characterized by the highest number of sick calls. Thus, those who showed the best performance, as judged by the mile run, had the least number of peripheral problems (Fig. 3), and those with the poorest performance records had the most symptoms and signs (Fig. 4).
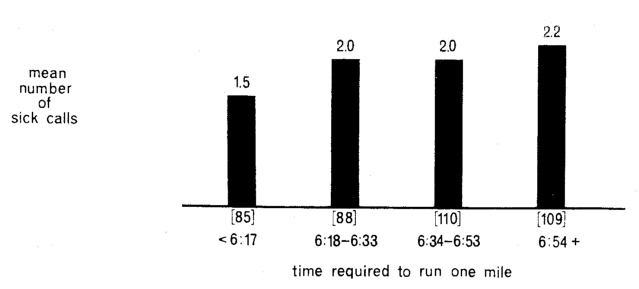
Fig. 2. Relationship between the time required to run one mile at the start of a 24-week training period and the subsequent frequency of sick calls. This indicates the predictive worth of one measure of performance (running a mile) with regard to the more peripheral manifestations of disease.
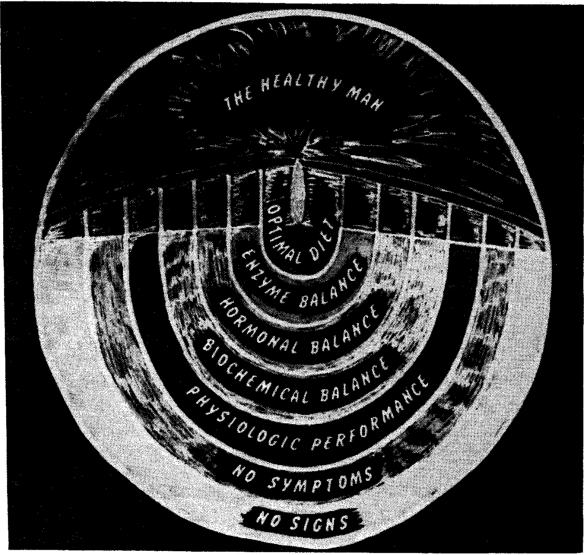
Fig. 3. In healthy man, all levels are in balance.
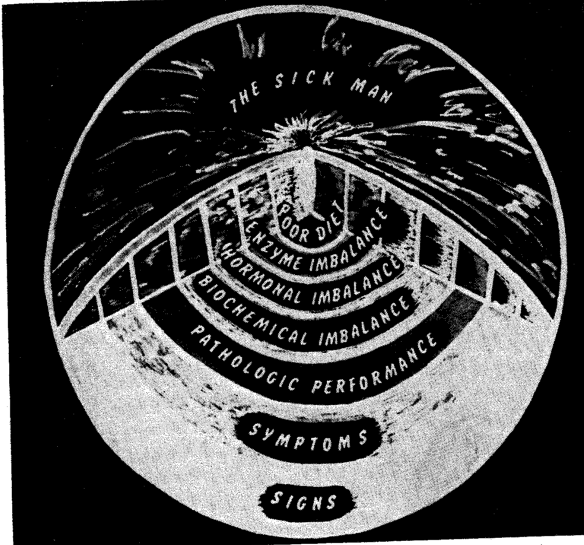
Fig. 4. In the wake of a core problem (inadequate diet or exercise), there are eventual disturbances in the levels of enzymes, hormones, the biochemical state, performance, and finally symptoms and signs.
References Cited:
- Cheraskin, E., and Ringsdorf, W. M., Jr.: “Predictive medicine. I. Definitions,” Alabama J. Med. Sc. 7: 444, 1970; “II. Experimental models,” J. Am. Geriatrics Soc. 19: 448, 1971; “III. An ecologic approach,” Ibid. 19: 505, 1971; “IV. The gradation concept,” Ibid. 19: 511, 1971; “V. Linear versus curvilinear functions,” Ibid. 19: 721, 1971; “VI. Physiologic versus normal values,” Ibid. 19: 729, 1971; “VII. The specificity of tests,” Ibid. 19: 802, 1971; “VIII. Familial versus genetic factors,” Ibid. 19: 887, 1971; “IX. Diet,” Ibid. 19: 962, 1971; “X. Physical activity,” Ibid. 19: 969, 1971.
- Cheraskin, E., and Ringsdorf, W. M., Jr.: “The health of the dentist and his wife. (a) A predictive medicine program,” J. South. California Dent. A. 37: 271, 1969; “(b) Present findings in a predictive health program,” Ibid. 37: 413, 1969.
- Cheraskin, E.: “Concepts in predictive medicine,” Lab. News 11: 23, 1970.
- Unpublished data, Department of Oral Medicine, University of Alabama Medical Center, Birmingham, Alabama.