
Access to all articles, new health classes, discounts in our store, and more!
Orthodontics Periodontics: The Until Now Hidden Nutrient Connection
Publication and date unknown.
* * *
A careful check of the current conventional orthodontic and periodontic textbooks reveals four unanimously agreed upon orthodontic/periodontic connections. First, periodontal factors may contribute to orthodontic abnormalities; second, orthodontic aberrations may invite periodontal sequelae; third, the commonly employed treatment in orthodontics with banding techniques may generate periodontal symptoms and signs; fourth, by act if not always by printed word, these relationships are held to be mediated purely and simply through local physicochemical and microbial mechanisms. As far as we can determine, not one of the current orthodontic or periodontal standard textbooks has addressed the burning general question as to why seemingly similar orthodontic patients treated by the very same orthodontist with seemingly similar orthodontic techniques so often respond so differently. And finally, as far as we can ascertain, no one has attempted the solution to the specific question regarding the often observed clinical paradox following orthodontic banding, namely with the same treatment by the same practitioner, one child responds quickly and successfully, another less swiftly and not so successfully, while a third fails.
The purpose of this brief report is to assess a possible previously unmentioned nutrient connection by means of two separate studies conducted by us at our clinic. The first study is intended to measure the periodontal repercussions which follow orthodontic banding with and without multivitamin/trace mineral supplementation in presumably healthy children. The rationale for such nutritional support is based upon two observations. First, there is reasonable evidence that many youngsters in so-called civilized cultures eat badly.1,2 Second, there is nothing in the standard periodontic/orthodontic textbooks regarding studies of the eating habits of such dental patients. We have reported in the orthodontic literature that somewhere between 17 and 72% of presumably healthy children undergoing orthodontic therapy demonstrate suboptimal vitamin C levels.3,4 The second experiment we wish to describe attempts to cast light on the prediction of periodontal response to orthodontic banding through an appraisal of nonfasting blood glucose in a subset of the original sample of allegedly healthy children employed in the first experiment.
One hundred forty-two supposedly healthy children being readied for orthodontic therapy constitute the participants for the first experiments. Age, sex, oral health status, and other relevant particulars all have been detailed in earlier publications.5-8
In one-half of the children, the right side and in the other half the left side was orthodontically banded. Additionally, half of the group received a standard multivitamin/trace mineral supplement; the other half an indistinguishable placebo. The gingival state, clinical tooth mobility, and labial debris were graded by standard clinical techniques in the banded and nonbanded sides at the start and completion (thirty days later) of the experiment by the same examiner with no knowledge of the nature of the supplement.
The clinical effects of orthodontic banding versus no banding with multivitamin/trace mineral versus placebo supplementation upon gingival inflammation (Fig. 1), clinical tooth mobility (Fig. 2), and labial debris (Fig. 3) are summarized. Four points require special mention. First, in all parameters studied (gingival inflammation, +5.6%, clinical tooth mobility, +8.4%, and labial debris, +1.6%) there were no significant changes in the nonbanded placebo group. This, one would anticipate, if the measuring techniques are reasonably valid. Second, there was a statistically significant worsening in the subjects provided and placebo support. Specifically, the scores were 25 % deterioration in gingival inflammation, 14.3% in clinical tooth mobility, and 28% in labial debris. This observation is consistent with general clinical observation, namely that unfavorable periodontal reactions frequently parallel orthodontic banding. Third, there were no significant changes in the group with banding but provided with vitamin/mineral supplementation. Actually, the values were +1.5%, -5.3%, and -8.6% in gingival inflammation, clinical tooth mobility, and labial debris respectively. Fourth, with all parameters studied, there was a statistically significant improvement in the areas with no banding and with multivitamin/mineral support.
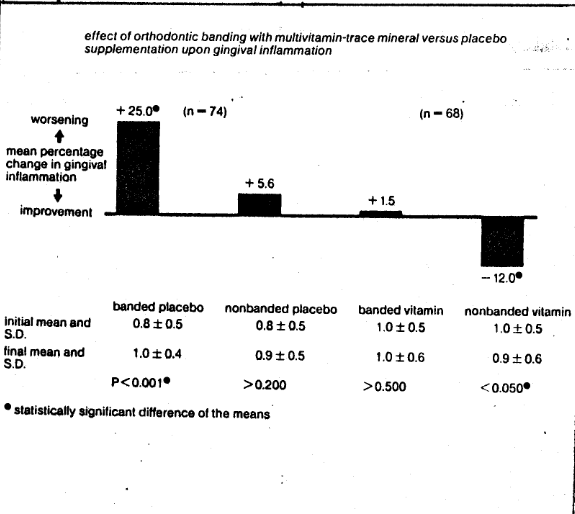
Fig. 1–The effect of orthodontic banding with multivitamin-trace mineral versus placebo supplementation upon gingival inflammation. There is a statistically significant (25%) worsening in the banded placebo group. There is a significant worsening (1.5%) in the banded multivitamin-trace mineral group.
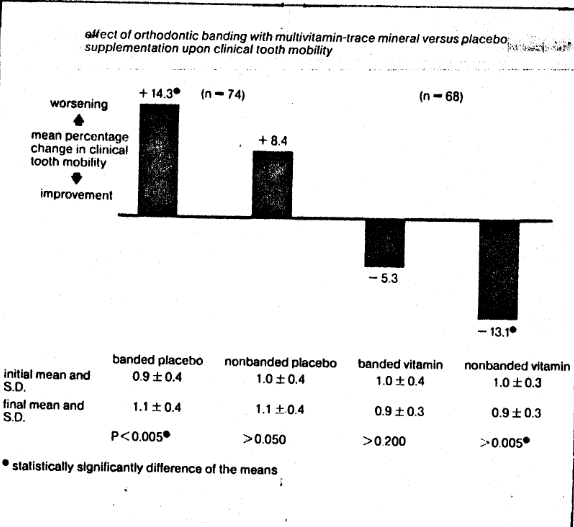
Fig. 2 The effect of orthodontic banding with multivitamin-trace mineral versus placebo supplementation upon clinical tooth mobility. There is a statistically significant worsening (14.3%) in the banded placebo group. There is an insignificant reduction (5.3%) in the group with banding and multivitamins and trace minerals.
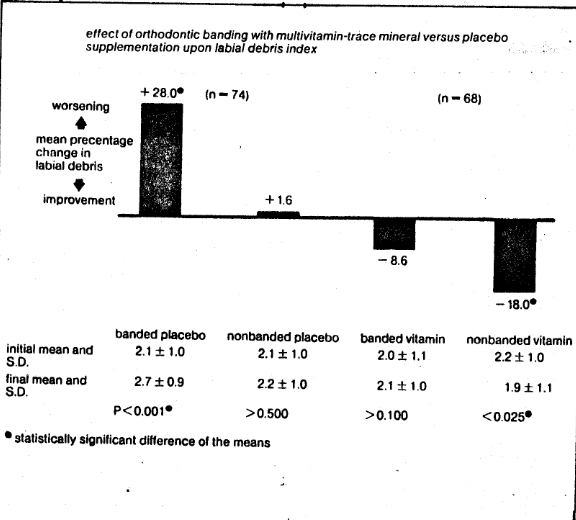
Fig. 3 The effect of orthodontic banding with multivitamin-trace mineral versus placebo supplementation upon labial debris. There is a statistically significant worsening (28%) in the banded placebo group. There is an insignificant improvement (8.6%) in the banded multivitamin/trace mineral group.
The obvious and relevant conclusion that must be drawn is that such nutritional support, by mechanisms still to be elucidated, vaccinates the periodontal structures against the environmental trauma attendant to orthodontic banding.
An examination of the raw data in the group with orthodontic banding and placebo support that, while on a mean basis, there was a statistically significant worsening of all parameters studied, all subjects did not behave the same. Many worsened, some remained unchanged, and some actually improved. The question now at hand is to ascertain whether it is possible to predict which children will respond favorably and which unfavorably to banding. This is the purpose of the second experiment.9
The gingival inflammation changes (Fig. 4), clinical tooth mobility (Fig. 5), and labial debris (Fig. 6) with placebo supplementation and banding in terms of nonfasting blood glucose (as one nutritional measure of homeostasis) were examined. Specifically, at the beginning and end of the 30-day experimental period nonfasting blood glucose was measured in all subjects (in the 27 in whom there was an increase in gingival inflammation versus the 42 in whom there was no increase in gingival inflammation) (Fig. 4). The reliability of the blood glucose measurements is clear from their consistent initial versus final values (93 ± 44 versus 90 ± 39 and 86 ± 7 versus 84 ± 9). Particularly exciting is the statistically significant difference of the variances in the group which worsened, as against the group which did not (44 versus 7 which is approximately sixfold). Hence, the evidence clearly suggests greater dysglycemia (a greater tendency to either hyper-or hypoglycemia) in those subjects responding unfavorably to orthodontic banding as judged by gingival inflammation (Fig. 4). The general pattern obtains for clinical tooth mobility (Fig. 5) and labial debris (Fig. 6).
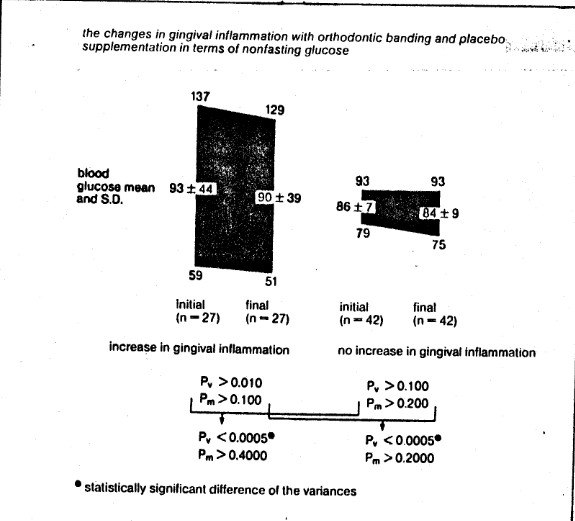
Fig. 4 The changes in gingival inflammation with orthodontic banding and placebo supplementation in terms of nonfasting blood glucose. Note that the initial and final values are very similar. Observe that there is a statistically significant variance difference between the group which worsened clinically versus the group which did not (93 ± 44 and 86 ± 7, a six-fold difference). The evidence suggests great dysglycemia (hyper- or hypoglycemia) in those subjects responding unfavorably to orthodontic banding as measured by gingival inflammation.
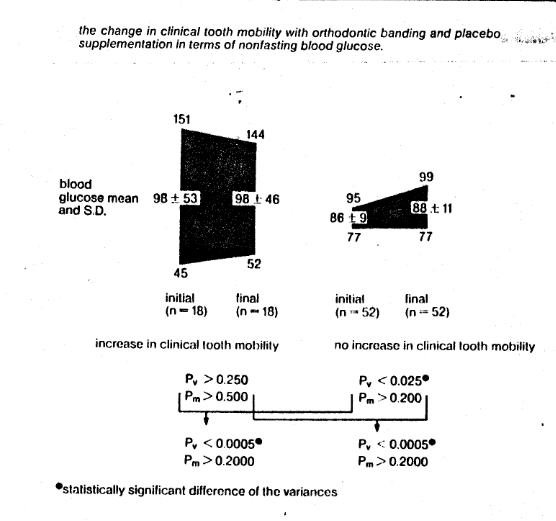
Fig. 5 The changes in clinical tooth mobility with orthodontic banding and placebo supplementation in terms of nonfasting blood glucose. Note that the initial and final values for each group are similar. Observe that there is a statistically significant variance difference between the group which worsened versus the group which did not (98 ± 53 versus 86 ± 9, a six-fold difference). The evidence suggests great dysglycemia in those subjects responding unfavorably to orthodontic banding as measured by clinical tooth mobility.
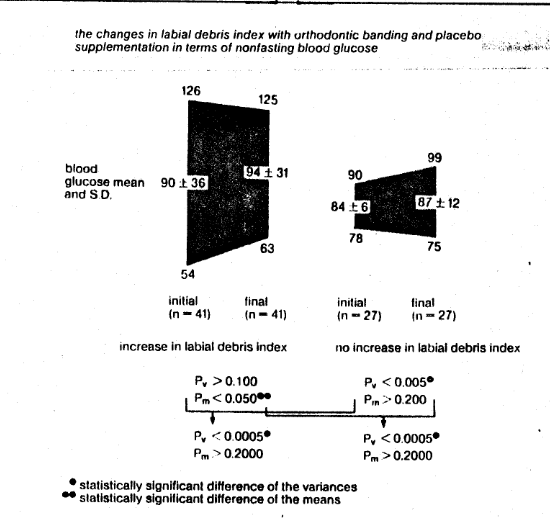
Fig. 6 The change in labial debris with orthodontic banding and placebo supplementation in terms of nonfasting blood glucose. Observe that there is a statistically significant variance difference between the group which worsened versus the group which did not (90 ± 36 versus 84 ± 6, a six-fold difference). The evidence suggests greater dysglycemia in those subjects responding unfavorably to orthodontic banding as measured by labial debris.
These data underscore the often mentioned but rarely investigated variability of therapeutic response, referred to as tissue tolerance, predisposition, constitution, resistance, and susceptibility, which can indeed be explained by nonfasting blood glucose. We have reason to believe that such predictability can be derived by other biochemical and physiologic instruments besides blood glucose. In any case, the subjects who demonstrated no decline from banding exhibited high (meaning good) tissue tolerance as judged by greater homeostasis (greater homogeneity of blood glucose). On the other hand, those who worsened with banding placement exhibited low (or poor) tissue tolerance and displayed greater variability in blood glucose scores. Thus, blood glucose is one mirror of homeostasis and may well be one avenue to quantitate and possibly predict the heretofore elusive factor referred to as tissue tolerance.
Parenthetic mention should be made that these studies were done with children. As interest burgeons in adult orthodontics, the problems become more grave since the coping systems progressively decline with the aging process. Hence, it would be reasonable to expect, if and when the appropriate studies are done, that diet and nutrition will play an even greater role in the management of adult orthodontics.
References Cited:
- “Agriculture Department Report: Poor diet trend in U. S. continues.” JAMA 203 (12): 49, 18 March 1968.
- US Department of Agriculture: “Food and nutrient intakes of individuals in 1 day in the United States, Spring 1977.” Nationwide Food Consumption Survey 1977-1978. Preliminary Report No. 2. Washington, D.C.; Science and Education Administration, 1980.
- Cheraskin, E., and Ringsdorf, W. M., Jr. “Biology of the orthodontic patient: I. Plasma ascorbic acid levels.” Angle Orthodont. 39 (2), 137-138,1969.
- Cheraskin, E, and Ringsdorf, W. M., Jr. “Biology of the orthodontic patient: II. Lingual vitamin C test scores.” Angle Orthodont. 39 (4), 324-325, October 1969.
- Dusterwinkle, S. A. “Tissue tolerance to orthodontic banding. A study of multivitamin supplementation.” Master’s Thesis. University of Alabama School of Dentistry, 1965. Birmingham, Alabama.
- Lane, W B. “Nutrition and oral response to orthodontic banding.” Master’sThesis. Birmingham, Alabama: University of Alabama School of Dentistry, 1968.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F H. “Gewebsverträglichkeit der kieferorthopadischen Bebanderung: Zwei Studien in Zusammenhang mit Multivitamin-Spurenmineral-bzw. Placebo-Verabreichung.” Informationen aus Orthodontie und Kieferorthopädie 2: 233-255, 1978.
- Cheraskin, E., Ringsdorf, W M., Jr., and Medford, F. H. “Tissue tolerance to orthodontic banding: Two studies in multivitamin/trace mineral versus placebo supplementation.” Int. J. Orthodont. 17 (4) 6-60, December 1979.
- Cheraskin, E., Ringsdorf, W. M., Jr., and Medford, F. H. “Gewebeverträglichkeit der kieferorthopädischen Bebänderung: Studie zum Kohlenhydratstoffwechsel.” In E. Hösl, et al. (ed.): Konzept & Perspektiven. Munchen, Verlag: Zahnärztlich-Medizinisches Schrifttum, 1980.
- Cheraskin, E, and Ringsdorf, W. M., Jr. “Tissue tolerance to orthodontic banding: A study in carbohydrate metabolism.” Angle Orthodontist 52 (2), 118-128, April 1982.
- Cheraskin, E, and Ringsdorf, W. M., Jr. “Predictive dentistry: A study in carbohydrate metabolism.” Med. Hypotheses (in press).