
Access to all articles, new health classes, discounts in our store, and more!
New Light on Modern Physical Degeneration From Field Studies Among Primitive Races
Read before the Second Session Ohio State Medical Association, 91st Annual Meeting, Dayton, Ohio, April 28-29, 1937. Published in The Ohio State Medical Journal, Vol. 33, No. 9, September 1937.
* * *
Modern scientific research is based on the principle of comparing two or more groups where the least number of variables is involved. Animals react differently from each other and very often differently from man. Through the ages Nature has been carrying on experiments in her gigantic biological laboratory in which one of the experimental animals used has been man. She has done this through a very wide range of climatic and geologic conditions. She has demonstrated that if man will learn her laws as applied to that environment in the matter of the selection of his foods, he can not only build magnificent physical bodies but maintain them largely free from disease.
Since progress has often been so exceedingly unsatisfactory by using our modern laboratory procedures, I have undertaken to study Nature’s results in her great laboratory by going to the remnants of primitive racial stocks who have succeeded in meeting Nature’s demands and have noted the changes in that environment which occur when they lose that high efficiency and high excellence as a direct effect of making contact with our modern civilization and adopting certain of its methods of living. Particular attention has been given to the role of the adoption of the foods of our modern civilization as a displacement of the native foods used by these various primitive groups.
The splendid advancement that has been made in surgery, bacteriology and hygiene has produced very little change in the incidence of several of the degenerative diseases. Alexis Carrel, in his recent work, “Man, the Unknown,”’ states that:
“’Medicine is far from having decreased human sufferings as much as it endeavors to make us believe. Indeed, the number of deaths from infectious diseases has greatly diminished. But we still must die, and we die in a much larger proportion from degenerative diseases.”
After reviewing the reduction in the epidemic infectious diseases he continues as follows:
“All diseases of bacterial origin have decreased in a striking manner. Nevertheless, in spite of the triumphs of medical science, the problem of disease is far from solved.
“’Modern man is delicate. Eleven hundred thousand persons have to attend to the medical needs of 120,000,000 other persons. Every year, among this population of the United States, there are about 100,000,000 illnesses, serious or slight. In the hospitals, 700,000 beds are occupied every day of the year…Medical care, under all its forms, costs about $3,500,000,000 yearly…The organism seems to have become more susceptible to degenerative diseases.”
The limited space does not permit of a review of the unproductive researches of the writer and others in the effort to find a clue to the etiology of oral degenerative processes by a search for the controlling factor in the affected tissues, nor did these investigations explain why various individuals responded so differently to the influence of focal infections which they were carrying, such as dental infections. On the presumption that dental caries and degeneration of supporting tissues of the teeth were primarily related to the absence of something rather than the presence of something, I have been carrying forward through several years studies among these primitive racial stocks in order to ascertain what the factors were in the environment which changed when immune groups lost their immunity and came to behave like the people of our modern civilization.
Since dental caries is generally accepted to be the most universal disease in the world, particularly among our modern civilizations and since its activity immediately becomes a yardstick for measuring the severity of the forces at work, this has been used as one of the important criteria for interpreting the data. That tooth decay is a modern affection in the history of mankind has been claimed by many physical anthropologists. This is illustrated by Dryer1 who in discussing dental caries in prehistoric South Africans stated as follows:
“In not one of a very large collection of teeth from skulls obtained in the Matjes River Shelter (Holocene) was there the slightest sign of dental caries. The indication from this area therefore bears out the experience of European anthropologists that caries is a comparatively modern disease and that no skull showing this condition can be regarded as ancient.”
While much valuable information can readily be obtained from a study of skeletal material, it is not always possible to make even an approximate estimate of many of the conditions in the environment, particularly of the nutrition. It has accordingly, been very important to locate and reach for study, remnants of primitive racial stocks whose isolation has been sufficiently complete to provide protection and among whom a very high immunity to dental caries still persisted.
Another of the important problems of special study in this series has been a search for evidence that would throw light upon the cause of facial and dental arch deformities with associated irregular teeth. This is an affection which while some primitive races have suffered from it, as evidenced by their skulls, many other primitive stocks have been practically free from it.
I have proceeded on the assumption that, if racial groups can be found with high immunity to dental caries and freedom from dental arch deformities while under a relatively fixed environment of long standing, that where members of their groups have lost this high perfection with a change of that environment, an adequate study of that environment will lead directly to the causative factors.
These studies have included groups in isolated high valleys in the Alps in Switzerland,2, 3 where I found the incidence of dental caries to be only 4.6 per cent of the teeth studied. This is in striking contrast with the modernized group at St. Moritz at a comparable altitude, where I found the incidence of dental caries to be 29.8 per cent of the teeth studied.4
In the Outer Hebrides5 off the west coast of Scotland, I found the people in the isolated districts in the Isle of Lewis and Harris to have only 1.2 per cent of the teeth attacked by dental caries; whereas in the modernized sections the incidence was 30 per cent of the teeth examined.
Among the Eskimos6 in isolated districts in Alaska, I found that only two teeth out of 2,138 teeth, or 0.09 per cent had been attacked by tooth decay. At the port of Bethel, however, where a government station has been established and where the individuals secure modern foods which are shipped in, the incidence of dental caries among the local Eskimos was 13 per cent, constituting a 144-fold increase.
For the Indians in the far north inside the Rocky Mountain range in northern Canada, I found that in a study of 2,464 teeth in four groups of Indians there were only four teeth that had ever been attacked by dental caries, or 0.16 per cent. At the point of contact with modern civilization, however, 21.5 per cent of the teeth examined had dental caries. At the coast where the contact had existed for some time, six towns were found in which the average percentage of dental caries among the Indians, living largely on the imported foods, was forty of each hundred teeth examined. 7,8,9
In the archipelagos of the Southern Pacific, for the Melanesians who were still isolated, the incidence of dental caries was 0.38 per cent of the teeth studied. For those individuals living on trade foods of modern civilization at the ports, 29.0 per cent of the teeth studied had been attacked by dental caries.10 For the isolated Polynesians, 0.32 per cent of the teeth had been attacked by dental caries, and for those obtaining the imported foods of modern civilization at the ports, 21.9 per cent of the teeth had been attacked by dental caries.11 In the primitive Indians of Florida, from an examination of the skulls in three museums, I found practically 100 per cent immunity to dental caries.12 These skulls had been taken from the mounds in southern Florida and belonged to the pre-Columbian period. For the Indians living in the Cypress swamps and still endeavoring to live on the native foods, I found four teeth in each hundred teeth examined to have dental caries. In the modernized Indians of Florida, using the trade foods of modern civilization, 40 teeth out of each 100 had been attacked by tooth decay. In my studies in 1935 of 27 tribes in eastern and central Africa, five were found in which the individuals examined had no teeth with dental caries. For 13 groups of the 27, only 26 teeth out of 9,564 teeth examined, or 0.2 per cent had been attacked by tooth decay. Eight other groups partially modernized revealed that of 16,514 teeth examined, 1,122 teeth or 6.8 per cent were involved with dental caries.13,14
In 1936 I found the level of immunity to dental caries among the Bush natives of Australia to range from 0 for those with complete isolation to 4.3 teeth per 100 examined for those who had some slight contact with modern civilization. Those having intimate contact with modern civilization, being fed largely by government agencies, had up to 70.9 per cent of the teeth attacked by dental caries. For the Maori of New Zealand the range was from 1.7 for individuals using very largely the native foods, including sea foods, to 55.3 teeth per 100 teeth examined for the groups of natives fed in a public institution.
Samples of foods of all of these groups were gathered and brought to my laboratories for chemical analysis. Partial reports on these have been made in the references.
If we assume that dental caries is an expression of the level of immunity of that individual at the time that active caries is in process, we have still to consider, when comparing one individual with another, the possibility that one has a higher capacity for adaptation to that environment than the other. We will accordingly, be concerned to know what forces may have been at work to modify the efficiency of various individuals of the group–for example, one member of the family as compared with others living in relatively similar environmental conditions.
This leads us directly to a study of the forces at work during the formative period which may have controlled the general physical efficiency of that individual. In thinking of man as a biologic unit, we are concerned to know whether various individuals will react the same in various environments, that is, with the same divergencies from normal with the same variations in environment. We are concerned when making a study of causative factors to reduce the variables to as few factors as possible.
We have in general, the observation that the several racial stocks studied herewith changed from a high immunity to dental caries to a low immunity level, when changing their native adequate nutritions to the imported foods of modern civiliziation.15 On a chemical basis, by an analysis of these various efficient nutritional programs, I have shown them to be relatively comparable in that they have supplied a high level of body building and repairing materials which provide the energy factors required from day to day. I have shown in detail that the displacing foods of modern civilizations have been relatively higher in energy factors in proportion to the body building and repairing factors than the effective primitive dietaries. For example, I have shown that for the Eskimos of the far north the following reductions occurred: calcium, 81.1 per cent; phosphorous, 80 per cent; iron, 30 per cent; magnesium, 86.6 per cent; copper, 46.6 per cent; iodine, 97.8 per cent. For the Indians of the far north the figures for the reductions are comparable to those for the Eskimos.
In the eight different primitive racial stocks studied in very different geographic locations and therefore physical environments, there has been a change in the level of immunity ranging from 0 to 4.6 per cent for the isolated groups, to 13 to 40 per cent of the teeth of the modernized groups. In a study of the changes in facial form at the point of contact with this change in nutrition, there have developed in the next generation, irregularities in certain physical features of the body. It is important in relation to our problem that these changes have been very similar in all the various racial groups studied and similar to our modern deformities. Among the frequent typical changes in facial pattern and dental arch form is the dropping back of the upper lateral incisors and the narrowing of the upper arch. This may or may not be associated with a similar change in the lower arch.
In Figure 1 will be seen typical illustrations taken from several of the different racial stocks referred to above. This figure, however, represents only one type of deformity frequently met with in all the various groups. These characteristic types of facial and dental arch deformities have included (1) a lack of development forward of the middle third of the face; (2) a lack of development of the lower third of the face; (3) a lack of development of both zones with narrowing and crowding of the teeth; (4) a narrowing and lengthening of the face.
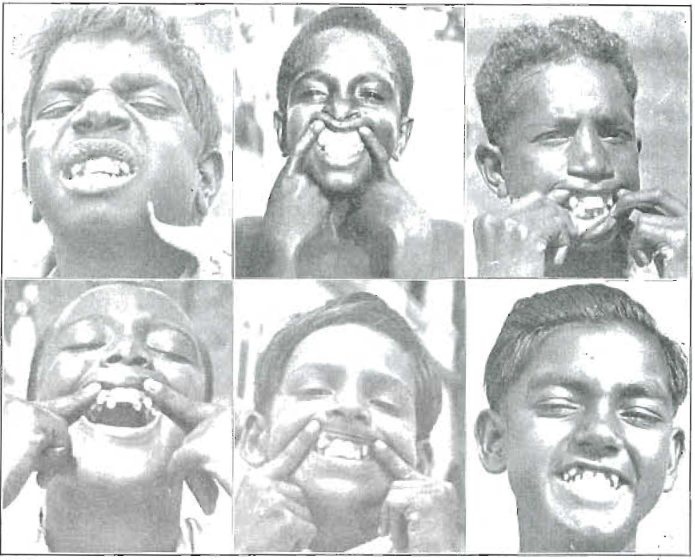
Figure 1. These six boys are first or second generation after the adoption by the parents of modern foods. Note the same type of facial and dental arch deformity. Above, left to right –Australian Aborigine; Malay; Melanesian, Fiji; Below, left to right–Central African; East Indian at Mombasa; East Indian at Suva, Fiji.
My data have indicated that when the nutrition is adequate to meet the body’s needs in all stages of its development, various individuals of the same racial stock reproduce the facial type or pattern so perfectly that they look like members of the same family, though actually unrelated. This condition is shown in Figure 2 which illustrates four Melanesian boys living on different islands who look like brothers but who have no family relationship. Each, however, has completed the reproduction of the racial pattern. Note the strong family resemblance. This is also shown in Figure 3 which presents four Polynesian girls, also from different islands who have a very strong family resemblance though they are not related, except that each has reproduced the racial type. In contrast with these, two first generation boys and a first generation girl after the adoption of the imported foods are shown in Figure 4. It is important to compare this girl’s features with those in Figure 3. She never can be beautiful like they are because of a gross disturbance in the formation of her face. One of the structural defects of this is readily seen in the teeth in the view to the right. The boys in the upper part of Figure 4 both show very marked disturbance in facial development.
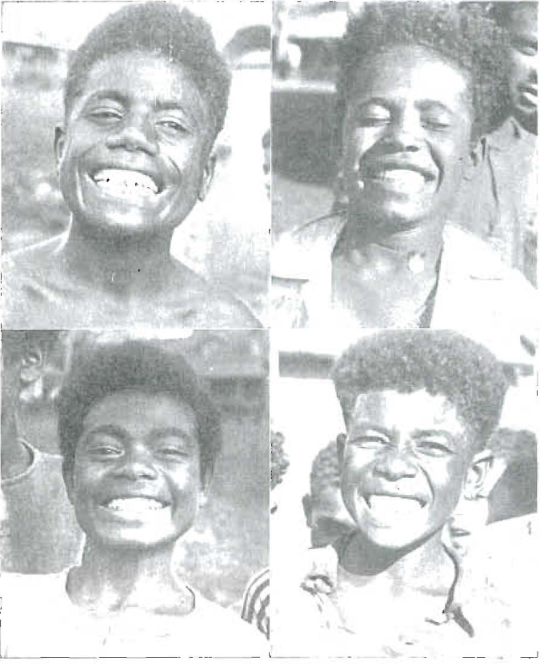
Figure 2. Melanesians–Note the family resemblance though not related.
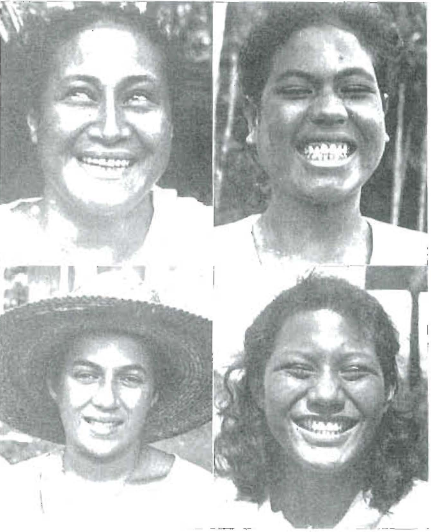
Figure 3. Polynesians–Note the family resemblance though not related.
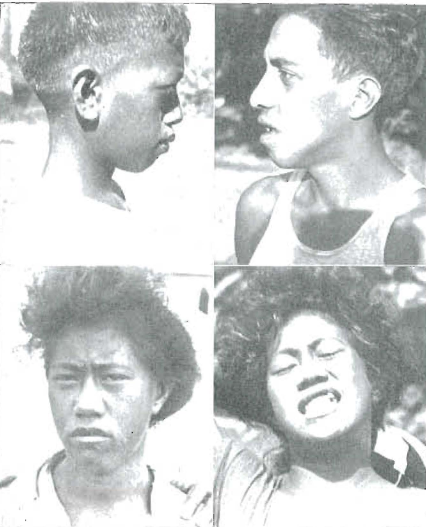
Figure 4. Irregularities of the dental arches with facial deformity developed in even the first generation on deficient diet.
A very striking and evidently significant type of information has come out of these studies among a large variety of primitive racial stocks. When members of these groups have adopted the imported foods of modern civilization, including white flour, sugar, polished rice, canned goods, or chiefly the first two, as a displacement for their native foods many individuals in the next generation have developed facial pattern changes with so marked a divergence from the tribal pattern that they must be classified as deformity patterns, and in each group we have similar facial changes occurring in even the first generation after the parents have adopted the modernized foods. The deformity patterns are not only similar in these various groups but similar to those which occur in our modern white civilizations.
If space permitted some typical illustrations of the similarity of reaction to modernization would be presented in which modern whites would be shown beside a first or second generation after modernization of a primitive racial stock. It is exceedingly strange that so important a matter as a progressive physical degeneration has been taking place in the families all about us without this fact having been recognized or become a matter of special or general information. I find no reference to it in the literature, nor had I recognized it until I found it did not obtain among primitives. Now that I have come to recognize it I find it in more than 50 per cent of the American families that I study. It is expressed as a progressive narrowing and lengthening of the face with succeeding children. The first child usually shows a much more nearly normal facial design than the later children. It is apparent from my study of primitive races that nature always makes the dental arches broad with the upper and lower dentitions interdigitating, thus providing a normal masticating mechanism and also providing, regardless of race, a facial design that is in harmony with the normal dentition. In all of these primitive races who are living on an adequate nutrition, I find all members of the family developing a facial pattern which reproduces the tribal type. At the point of contact with modern civilization, however, those children of the family born after the adoption of our modern dietary program, frequently show the progressive degeneration of the face whereas those children of the family born before, even where there are a number in the family, all have developed normal dental arches and facial form.
It is important to keep in mind that the maximum facial deformity is not seen until the permanent dentition has erupted at nine to thirteen years of age. In severe cases it involves even the temporary dentition and the childhood face.
In Figure 5 will be seen three brothers born before the government store was placed on Badu Island, north of Australia. Note their faces which are all of the same general design with typical broad dental arches. The lower picture in this illustration shows four members of a family, the oldest at the right was born before the store was placed on this island and the other three toward the left after the establishment of the store with its imported foods. Note that all of these later individuals have disturbed facial development accompanied by irregularities of the dental arches.
Unfortunately, we see so many abnormal faces that we have come to accept them as proper facial patterns. It has been very easy to account for them on the basis of mixing of ancestral stocks. This is one of the reasons why I find it necessary to go to primitive racial groups and study them where isolated and at the point of contact with the changing forces in order to eliminate this possible source of physical change due to ancestry.
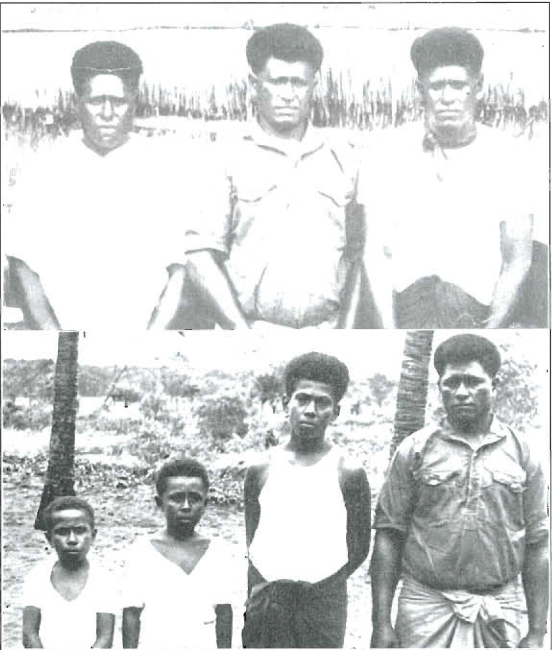
Figure 5. The three brothers above were born before the store was put on this Island and of the four below only the one to the right. The three to the left below were born after the store was established. Note the change in facial form.
This problem of progressive facial degeneration is often accompanied by a progressive physical degeneration. It is particularly significant that in these primitive groups I find the younger girls of the family, even though all have completed their growth, have narrower bodies throughout as well as a narrower face than the oldest sister, when the oldest member of the family is a girl. This will be illustrated in Figure 6 which also shows the progressive lateral narrowing and vertical lengthening of the face reading from right toward the left in the upper view. In the lower view these same two girls and their brother are shown smiling to disclose their teeth. The one to the right has the typical and normal broad dental arch convex throughout its curve. Her sister to the left has arches that are flattened on the side and with a depression and narrowing in the bicuspid and molar regions. The next younger, the brother, has had so faulty a bony development of the face that both arches are very badly constricted so much so that there is not room for the cuspids either above or below in the line of the arch. This is precisely the type of condition that is occurring in a large number of our American families and is clearly a part of the progressive physical degeneration that can be traced to a lowered capacity of the mother for reproduction.
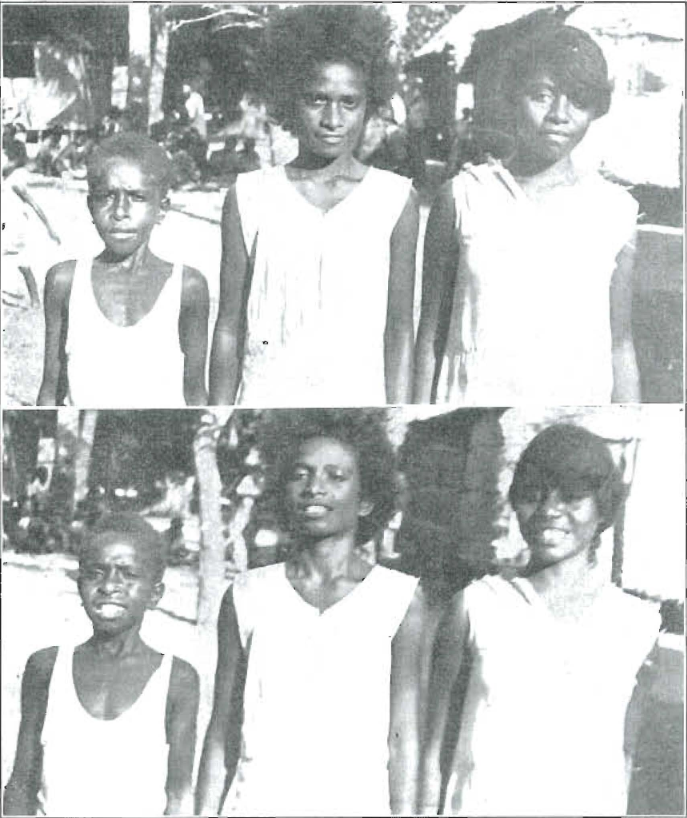
Figure 6. Note the progressive lateral narrowing and vertical lengthening of the faces in the three members of this family. Below note the narrowing of the dental arches with excessive deformity of the dental arches in the youngest member.
Since 1927 I have been carrying forward an analysis of dairy products received monthly from many places throughout the world. These have shown seasonal curves for vitamin levels17 which are directly related to plant growth and the consequent nutrition of the cattle. These in turn have been related to the level of morbidity and mortality for some of the degenerative processes and also for acute infections such as children’s diseases.18
Several research reports have appeared relating the nutrition of domestic animals to their reproductive capacity. Hale19 in discussing the relation of Vitamin A to eye development in the pig states:
“’A previous observation (see Abst. 4010, Vol. 3) is repeated in which three litters of pigs were born without eyeballs or with very serious eye defects when the mother had received a diet deficient in Vitamin A before mating and during the first thirty days of gestation.”
It is important in this connection to present data from other sources. Murphy20,21 has reported important studies relating to malformations with a period of lower reproductive activity. In concluding one of his reports on a study of statistical data on the birth records of Philadelphia, he states:
“4. Miscarriages, still-births and premature births occurred more often than would be expected by chance in the pregnancies immediately preceding and immediately following the pregnancy which resulted in the birth of the defective child, and less often than would be expected by chance in the remaining pregnancies. Miscarriage, still-birth and premature birth occurred more often in the pregnancy immediately preceding that of the defective child.
“’5. From the above observations, it is concluded that the birth of a congenitally malformed child may be only one expression of a prolonged decrease in functional reproductive activity, the other expressions having been miscarriages, stillbirths and premature births.”
Among the managers of zoological gardens it has been common knowledge that it was exceedingly difficult and nearly impossible to rear members of the cat family until recently unless the mother herself had been born in the jungle. This condition has been overcome by feeding the animals in captivity on the organs of animals such as the natural jungle mother obtains in her native environment.
In my studies of these primitive races I find many illustrations of a knowledge that the mother must be specially fed in anticipation of each pregnancy and that the pregnancies must be sufficiently spaced to permit re-establishment of an adequate factor of safety before the next occurs. This is accomplished in many of the primitive tribes by the system of plural wives in which the wife with the youngest child is protected.
We have here two distinct features of modern degeneration, the cause of which can now be traced directly to nutrition. The one, namely, dental caries which is shown to be directly related to the nutrition of the individual and the other facial deformity changes which are found to be directly related to the nutrition of the parent. We are now concerned with other expressions as having possible similar origin.
An important phase of these studies has been the accumulation of data relative to the physical characteristics of those individuals in various primitive tribes who were suffering from tuberculosis. This has been accomplished by making contact with the tubercular hospitals situated among the primitive racial stocks that were in the process of being modernized. All of the 20 boys and girls in the Juneau (Alaska) hospital suffering from pulmonary tuberculosis had gross deformities of the dental arches. Similarly, all of the 18 individuals between 12 and 40 in the Hilo sanitarium (Hawaiian Islands) suffering from pulmonary tuberculosis, had facial and dental arch deformities; and similarly all of the boys and girls in the Honolulu tuberculosis hospital suffering from pulmonary tuberculosis between 10 and 30 years of age, 19 in all, had dental arch deformities. Again in a study of the individuals in the Maori tubercular hospital situated at Pukeora, New Zealand, containing 34 individuals ranging in age between 13 and 48 years, 100 per cent of those under 21 years of age and 91.2 per cent of the adults showed marked or gross deformities of the dental arches and facial form.
This is a particularly important phase for study in connection with the general fact that in all of these primitive racial stocks there is a rapid toll being taken by tuberculosis. The reason generally ascribed is a lack of an accumulated immunity in the ancestry because of the lack of exposure. While that doubtless has been a factor it cannot account for the fact that so large a percentage of the individuals affected proved to be those who were definitely injured during the formative period. In the matter of arthritis in my studies of the Indians of the far north of Canada inside the Rocky Mountain range living in northern British Columbia and Yukon, not a single individual was found suffering severely from deforming arthritis among the isolated groups. At the point of contact, however, with our modern civilization at Telegraph Creek and vicinity where the imported foods, chiefly white flour and sugar, were being shipped in during the summer period and exchanged for furs during the winter, I found ten bedridden cripples suffering from deforming arthritis. Many of these were young people.
The problem of progressive physical degeneration in our modern civilization is probably second to none in importance, and evidence is being accumulated which relates the forces responsible directly to a lowered efficiency of the nutrition due in part to progressive soil depletion22 but largely to a departure from the accumulated wisdom of the primitive races. Much of the wisdom that I have collected has been consolidated and illustrated and is being published in book form in extended detail.
Editor’s note: Since the era in which this article was written, society’s understanding of respectful terminology when referring to ethnic and cultural groups has evolved, and some readers may be offended by references to “primitive” people and other out-of-date terminology. However, this article has been archived as a historical document, and so we have chosen to use Price’s exact words in the interest of authenticity. No disrespect to any cultural or ethnic group is intended.
References Cited:
- Dyer, T. F.: “Dental Caries in Prehistoric South Africa.” Nature, 136, 302, 1935.
- Price, Weston A.: “Why Dental Caries With Modern Civilization? (1) Field Studies in Primitive Loetschental Valley, Switzerland.” Dental Digest, March 1933.
- Price, Weston A.: “(2) Field Studies in Primitive Valais (Wallis) Districts, Switzerland.” Dental Digest, April 1933.
- Price, Weston A.: “(3) Field Studies in Modernized St Moritz, Herisau, Switzerland.” Dental Digest, May 1933.
- Price, Weston A.: “(4) Field Studies in Primitive and in Modern Outer Hebrides, Scotland.” Dental Digest, June 1933.
- Price, Weston A.: “(10) Field Studies Among Primitive and Modernized Eskimos of Alaska.” Dental Digest, 40, 120, June 1934.
- Price, Weston A.: “(9) Field Studies Among Primitive Indians in Northern Canada.” Dental Digest, 40, 130, April 1934.
- Price, Weston A.: “(8) Field Studies of Modernized Indians in Twenty Communities of the Canadian and Alaskan Pacific Coast.” Dental Digest, 40, 81, March 1934.
- Price, Weston A.: “(7) Field Studies of Modernized American Indians in Ontario, Manitoba and New York.” Dental Digest, 40, 52, February 1934.
- Price, Weston A.: “(12) Field Studies Among the Polynesians and Melanesians of the South Sea Islands.” Dental Digest, 41, 161, May 1935.
- Price, Weston A.: “(13) Field Studies Among the Polynesians and Melanesians of the South Sea Islands.” Dental Digest, 41, 191, June 1935.
- Price, Weston A.: “Studies of Relationships Between Nutritional Deficiencies and (a) Facial and Dental Arch Deformities and (b) Loss of Immunity to Dental Caries Among South Sea Islanders and Florida Indians.” Dental Cosmos, 77, 1033. Nov. 1935.
- Price, Weston A.: “(14) and (15) Field Studies in Kenya, Uganda, Belgian Congo, Sudan and Egypt.” Dental Digest, 42: 52, 89, February, March 1936.
- Price, Weston A.: “Field Studies Among Some African Tribes on the Relation of Their Nutrition to the Incidence of Dental Caries and Dental Arch Deformities.” Journal American Dental Assn., 23, 876, May 1936.
- Price, Weston A.: “Additional Light on the Etiology and Nutritional Control of Dental Caries With its Application to Each District’s Showing Immunity and Susceptibility.” Journal American Dental Assn., 20, 1648, Sept. 1933.
- Price, Weston A.: “New Light Obtained by a Study of Primitive Races on Modern Physical Degenerations, Inchding Dental Caries.” Dental Cosmos, 78, 853, August 1936.
- Price, Weston A.: “New Light on the Control of Dental Caries and the Degenerative Diseases.” Journal American Dental Assn., 18, 1189, July 1931.
- Price, Weston A.: “Some Contributing Factors to the Degenerative Diseases, With Special Consideration of the Role of Dental Focal Infections and Seasonal Tides in Defensive Vitamins.” Dental Cosmos, 72, Oct. and Nov. 1930.
- Hale, F.: “The Relation of Vitamin A to the Eye Development in the Pig.” Proc. Amer. Soc. Animal Prod. pp. 126, (Texas Exp. Station) Jan. 1935.
- Murphy, D. P., and Mazer, M.: “The Birth Order of 582 Malformed Individuals.” Jour. Am. Med. Assn., 105, 849, Sept. 14, 1935.
- Murphy, D. P., and Mazer, M.: “Reproductive Efficiency Before and After the Birth of Malformed Children.” Surgery, Gynecology and Obstetrics, 62, 585, March 1936.
- Price, Weston A.: “New Light on Some Relationships Between Soil Mineral Deficiencies, Low Vitamin Foods and Some Degenerative Diseases, Including Dental Caries with Practical Progress on Their Control.” Bull. of Indiana Dental Soc., Sept. 1932.