
Access to all articles, new health classes, discounts in our store, and more!
Is Dental Disease Predictable?
Published in Journal of Applied Nutrition, Vol. 19, Nos. 1 & 2, 1966-1967, pp. 14-36.
* * *
“Predictive medicine”–an unfamiliar term a few months ago,21–is rapidly becoming commonplace in the vocabulary of laymen and doctors, alike. The recent development of automated medical equipment is making possible undreamed of screening of individuals for many characteristics–biochemical, physiological, behavioral, etc.–a sort of fingerprinting of the whole person, by means of which on-coming disease can be predicted and perhaps, prevented.
Predictor of Dental Disease par Excellence
In 1960 it was estimated that the 180,000,000 Americans then living in the United States had accumulated 700,000,000 unfilled cavities in their teeth. The sheer magnitude of our dental problems is overwhelming, notwithstanding the billions of dollars spent on dental care and research, fluoridated water, tooth cleansers and health education. Decayed teeth are “handwriting in the mouth”1 which may be seen and warn of inner disturbances in the body chemistry, our “chief medical adversary,” according to Tom Spies, M.D., the late famed nutritionist.
As a guest speaker at the Centennial Meeting of the New York Dental Society in 1934, the writer reported a diet “predicator” (Chart I) she had discovered, by means of which the incidence of dental caries in a number of diet-teeth studies reported irr the literature was foretold with a surprising degree of accuracy.
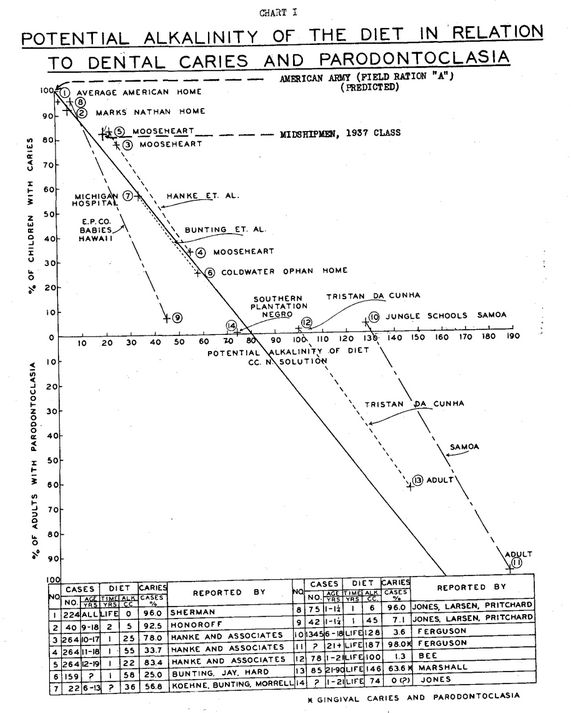
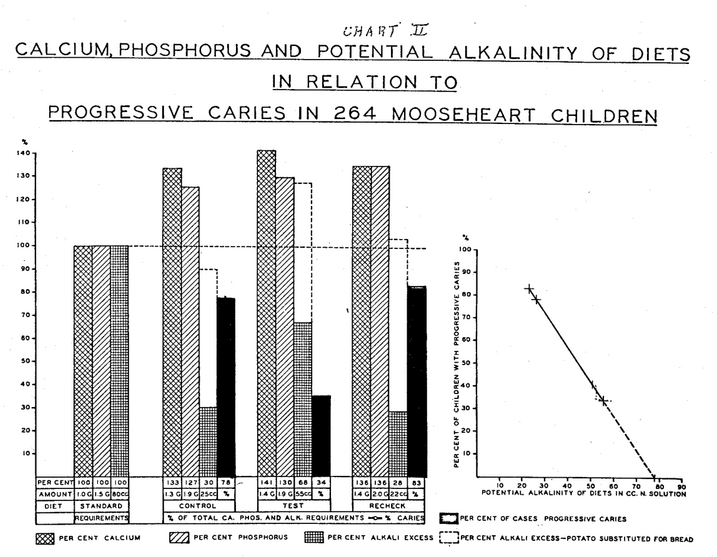
A “thumb rule” for diet balancing was suggested.2 The diet “predictor” was discovered through the analyses of the three diets–in effect one year each–reported in the diet-teeth study conducted by the Research Group of the Chicago Dental Society (Hanke and Associates) in 1933-32 (Chart II) from the standpoint of acid-base balance. As the potential alkalinity of the diets–well constituted in respect to all known diet essentials–increased from 22 to 55 cc N. alkali, with negligible changes in their calcium-phosphorus values or ratios, the incidence of caries in the 264 Mooseheart children decreased from 83 to 34 per cent (Chart II). The graph indicates that had the potential alkalinity of the diet been further increased to 78 cc N. alkali, the incidence of caries would have dropped to zero. It shows, also, that the simplest substitution of alkaline-ash potato for an equivalent amount of acid-ash bread in the three diets would have raised the potential alkalinity of each of them to near or above the optimal level, as indicated. Unfortunately, this was not done.
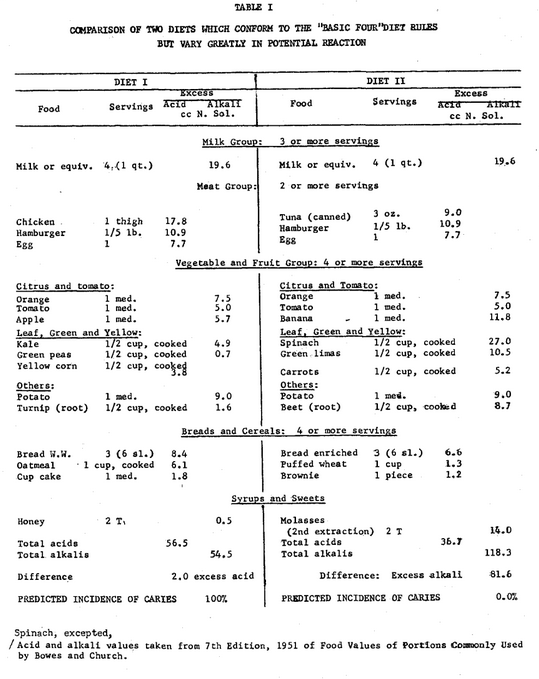
The excess of fixed alkalis or acids of any diet consisting of ordinary foodstuffs can be regulated, at will, in various ways: 1) by the exchange of alkali-poor fruits and vegetables for alkali-rich varieties; 2) by the exchange of acid-forming or alkali-poor syrups for alkali-rich ones; or 3) by increasing or decreasing the acid-forming meat, egg, grain component in proportion to the alkaline-ash fruits, vegetables and grasses (sugar cane and sorghum juices, principally), etc. How variable one’s diet may be in respect to its acid-base balance is shown in Table I. Both Diets I and II conform to the “Basic Four” diet plan generally advocated and have comparable calorie, protein and vitamin values. Diet I contains an excess of 2 cc. N. acid; Diet II, an excess of 81.6 N. alkali. According to the “Predictor,” the incidence of caries on Diet I would be 100 per cent, on Diet II, zero.
If the acid-base balance of a well constituted diet plays the important role in metabolism indicated here, the disregard for this balance shown by nutrition authorities in their dietary descriptions explains the discordant results and confusion in the literature concerning diet in relation to dental disease and related ills. Alterations in the mineral balance in one’s blood plasma affect every tissue and every cell in the body complex and undoubtedly have a bearing on the concentrations of other constituents in blood plasma, nullifying the significance of many tests now made.
Because the tissues have the ability to release ammonia (volatile alkali) from waste urea when fixed alkalis (sodium, potassium, calcium, magnesium, iron) from food are in short measure, and are thus equipped with buffers and other mechanisms for maintaining neutrality, certain nutrition authorities discount the importance of the acid-alkali content of the diet as a nutritional factor. Potential reaction values–excess acid and alkali–are not included in the Composition of Foods, Agriculture Handbook No. 8, United States Department of Agriculture; nor are they considered in the “Basic Seven” or “Basic Four” food groups advocated by the Bureau of Human Nutrition and Home Economics of the United States Department of Agriculture. Notwithstanding, D. Breese Jones, Principal Chemist in charge of the Protein and Nutrition Division of the Bureau of Chemistry and Soils, United States Department of Agriculture, in a publication titled Acid-Forming and Alkali-Forming Foods, May, 1930, states: “A satisfactory diet should contain enough of the alkaline-ash foods to balance the acid-ash foods. In health, the body is always slightly alkaline. If the blood and tissue fluids become even slightly acid, death occurs…When foods yielding an acid ash largely predominate in the diet, a condition of acidosis may result unless the resulting ash constituents are promptly neutralized and eliminated by the kidneys.”
Any metabolic process that is continually overtaxed will ultimately break down. A disturbance anywhere in the body complex might start a chain reaction which could extend throughout the entire system. It is logical to assume that changes in blood chemistry and alterations in the interrelationships of constituents would cause DROP-OUTS–cholesterol, lipids, minerals, etc. normally held in solution–which would interfere with circulation. Inevitably, cell function would become impaired; blood vessels might become encrusted with scale; resistance to infection lowered; and the stage set for the onset of disease and possibly disaster.
The normal ratio of alkalis to acids in blood plasma is reported to be approximately 4:1. The excess of alkalis over acids is called the alkali reserve–a certain level of which is essential for life. The importance of so large a reserve is understandable when one realizes that this is being continually drawn upon by the end products of metabolism and life processes: beating of the heart, breathing, contraction and tonus of muscles, etc. whether one is asleep or awake–with greatly increased withdrawals during periods of strenuous exercise, spurts in growth and development, over-exposure to ultraviolet radiation, emotional stress, acid-forming diet, etc. The ONLY source of fixed alkali for the maintenance of reserves consists of foods (and water, perhaps) that contain an excess. Such foods are fruits, vegetables and grasses (principally sugar cane and sorghum juices, as mentioned earlier) which vary tremendously in their excess alkali content. Thin green leaves (turnip, beet tops, spinach, etc.) and grasses are man’s most potent health protective foods and highest in potential alkalinity. If one wishes to get the amount of excess alkali contained in a 4 oz. serving of cooked spinach in the form of green peas, one must eat 4.8 quarts; or in the form of string beans–1.7 quarts; or in the form of shredded cabbage–1.5 quarts. This explains why one can eat pounds of fruits and vegetables which supply vitamins and other essential nutrients in adequate amount, without obtaining enough fixed alkali to keep the blood plasma reserves at a “safe” level.
Childhood Dental Troubles
The writer’s researches in nutritional diseases were prompted by her own physical-dental disabilities as a child. All six of her brothers and sisters enjoyed good health and freedom from dental troubles. The family dining table fairly groaned under its load of premium quality food–home grown for the most part, under the direction of her lawyer father, whose hobby was growing things better. There were always unlimited amounts of milk, butter and cream from pasture-fed Jersey cows; fertile eggs from thoroughbred chickens; organically grown fruits and vegetables in great quantity and variety–vine ripened and harvested fresh daily at the break of day. Apples were bought by the barrel and bananas by the bunch for between meal “snacks,” when home grown fruits were not in season.
Notwithstanding the large assortment of foods available at all times, the writer had strong likes and dislikes. She LIKED milk, meat, eggs and breads and DISLIKED vegetables in general and “greens” and sugar cane syrup (grass) in particular. Pampered by an adoring “Black Mammy” and an overly-anxious mother, she was allowed to eat what she wanted, when she wanted it. She didn’t like water and drank raw milk, instead, between meals, as well as at mealtime. She liked to gather eggs–sometimes from protesting hens. Her Mammy was ever ready to cook them for her, on order–usually hard boiled and mashed with lots of butter. At the dining table she ate meat and bread, principally. The other members of the family ate everything, usually “topping off” each meal with hot bread (five kinds served daily) liberally spread with butter and “long sweetening” (sugar cane syrup).
Year by year the writer grew taller, but her physical-dental state worsened. “Colds,” throat and ear infections succeeded one another in never ending succession. Teeth seemed to melt away. By the age of eight she was almost edentulous–all temporary teeth having been extracted and most of her newly erupted permanent ones. Broad dental arches were shrinking unevenly and new teeth erupting in wrong places. The roof of the mouth had become narrow and vaulted. Head and facial bones were getting out of alignment. A pretty, outgoing child was becoming homely, self-conscious and withdrawn. Doctors, dentist and parents were distraught. No one had the slightest idea what to do about it. Her state of health was so precarious that schooling was discouraged, and she attended classes only when the weather was good (sun shining) and she felt disposed to do so. High school finished, she decided to study her own problems, and to this end, acquired three academic degrees–including a Ph.D. in physiological chemistry at Yale in 1920. The problems remained unsolved, but the “tools” for research by means of which they were later solved were acquired.
Research
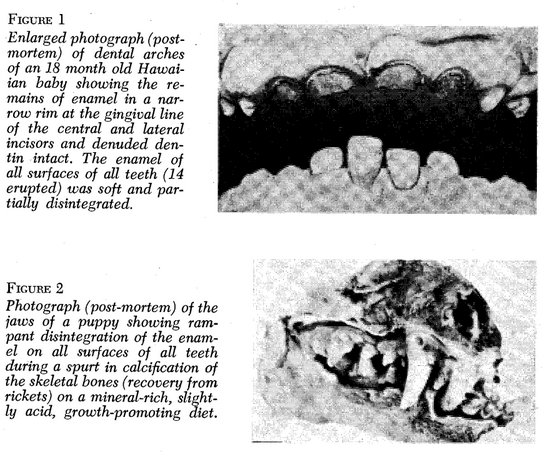
After joining the research staff of the University of California Medical School, San Francisco, in 1920, the writer started a feeding experiment on a litter of healthy, newly weaned puppies in the Department of Pediatrics. The diet consisted of bread, meat and skimmed pasteurized milk supplemented with butter fat, orange juice and a salt mixture based on the ash analysis of milk. By accident, TOO MUCH bicarbonate of soda got into the salt mixture. The puppies ate well and grew fast. Rickets-like changes in their skeletal bones began to appear. Simultaneously, metabolic studies revealed that they were excreting more calcium and phosphorus than they were ingesting. Progressive loss of bone was confirmed by x-ray. At nine months of age their bones were so decalcified that the puppies were unable to stand without support and were sacrificed. The ash content of the bones was found to be about half that of normal newborn puppies. The teeth looked normal but were found to be rootless enamel shells lightly attached to the gum (Plate I, Fig. 4).
Plate I, Figure 3–Photograph (post-mortem) of a dissected canine tooth of a dog showing enamel ravaged by decay and root (cementum and dentin) intact.
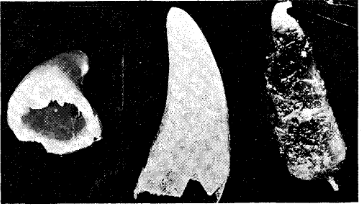
Plate I, Figure 4–Photograph (post-mortem) of a rootless canine tooth of a dog that was lightly attached to the gum of a 9 month old puppy whose skeletal and alveolar bones and roots of teeth (cementum and dentin) were DECALCIFIED on a mineral-rich, growth-promoting diet in which fixed alkalis were in excess. Note the excellence of the enamel cap.
A comparable litter of puppies was fed as nearly identically as possible, except that the excess alkali in the salt mixture was neutralized with hydrochloric acid. The results were diametrically opposite–normal bones and tooth roots but the enamel of newly erupted permanent teeth was ravaged by decay in a large percent of cases. The type of decay differed from classical caries in that it affected all surfaces of all the teeth and was called ODONTOCLASIA.13
Feeding Experiments with Adult Dogs
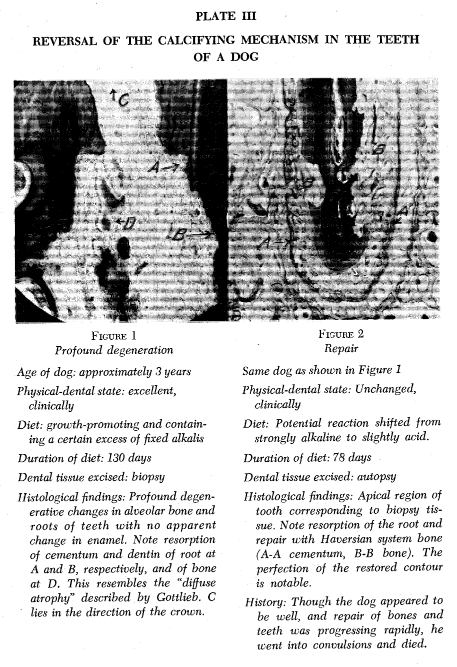
After three years of work with the puppies, the writer became a member of the California Stomatological Research Group then engaged in the study of pyorrhea; and in collaboration with its Chairman, F. Vance Simonton, D.D.S., Professor of Operative Dentistry, University of California Dental College, San Francisco, she repeated the puppy experiments on adult dogs. Biopsy tissue for histological study was taken from each animal when the potential reaction of the diet was shifted from acid to alkaline or vice versa. Findings in the puppies were duplicated in the adult dogs.3 Invariably, too high a degree of potential alkalinity in the diet caused profound degenerative changes in skeletal bones and roots of teeth (cementum and dentin) which have the same embryonic origins and react in the same way to nutritional faults; while the enamel of the teeth which has a different embryonic origin, remained intact. Conversely, the same diet made slightly acid stopped the destruction of bone and tooth roots, promoted calcification–repairing destroyed areas in the roots of the teeth with Haversian bone–and increased the liability of enamel to decay. (Plate III)
Both TOO MUCH alkali and TOO MUCH acid in the diet caused disturbances in the mineral constituents of blood plasma characterized, in part, by a low total base (alkali) content and CO2 combining power (alkali reserve). TOO MANY shifts in the acid-base balance of the diet (each period being three months) INVARIABLY resulted in convulsions and death,4 though previous to the onset of the convulsions, no clinical symptoms were apparent. At autopsy, all tissues were found to be extensively involved.
Vital Nutritional Factor
The above findings put the acid-base balance of the diet in the category of a vital nutritional factor equal in importance to protein, vitamins, trace elements or other essential nutrients. The author believes that disregard for acid-base balance in diets of today–well constituted or not–is a major factor in the physical-dental deterioration of our own nation and that of much of the civilized world. Regard for this balance as well as for the QUALITY of foods comprising the writer’s own diet solved her nutritional problems and those of hundreds of children in Hawaii and elsewhere.
Findings in the U.S.A.
We are a sick people–propaganda to the contrary. Examination of 600 supposedly healthy executives revealed 59.9 per cent of them had significant diseases of which they were not aware and only 7.7 per cent were graded as “healthy.” Among 14,132 public school children, 29.7 per cent had “hidden” diseases which were unknown previously, and only 36.3 per cent were graded “healthy.”6 The infant death rate is regarded as the most accurate indicator of a nation’s health. That of the United States is higher than the rate of nine other “advanced” nations. Our incidences of dental, respiratory and circulatory diseases are practically universal. With the progressive advance of degenerative diseases afflicting our people, one wonders what the increase in the estimated 700,000,000 unfilled cavities in the teeth of the 180,000,000 American people in 1960 might be today, and how soon we will become an edentulous nation. Said President Johnson in 1964, on appointing a 28 man commission to do something about our worsening national health: “If we do not do better, two of every three Americans now living will have or die of cancer, heart disease or stroke. I expect you to do something about it.”
During our “police” action in Korea, autopsy findings on 300 American and 300 Korean casualties were compared. The average age of the Americans was 22 years; that of the Koreans, unknown. Advanced blood vessel disease was found in 77 per cent of the Americans; NONE in the Koreans. In the Vietnam casualties today, the incidence of blood vessel disease is reported to be higher and more advanced. Indeed, autopsy findings indicate that its incidence is practically universal at the age of fifteen, and 50 per cent at ten. It has even been reported in the newborn.
Cancer was a medical rarity in children fifty years ago. In our vital statistics last year it was listed as the principal killer of children between two and fourteen years of age.
Average American Diet
The average American diet as reported by Sherman in 19327 was analysed by the writer2 from the standpoint of acid-base balance. It was practically neutral in potential reaction. On that basis, the incidence of caries was PREDICTED as 100 per cent. It was reported as 96 per cent. Although the consumption of milk, fruits and vegetables in the United States is high, the PREFERENCE of today’s generation for acid-forming corn, plums, prunes and cranberries and alkali-poor vegetables such as green peas, asparagus, string beans, head lettuce and cabbage, together with a DISLIKE for alkali-rich thin green leaves (turnip and beet tops, spinach, etc.) and grasses (concentrated juices of sugar and sorghum canes) creates a diet that may be rich in vitamins, minerals and other essential nutrients, but near neutral or acid in potential reaction.
This is strikingly illustrated in the two menus patterned on typical diets employed in northern and southern states, both of which measure up to the yardstick of good nutrition as recommended by the Food and Nutrition Board of the National Research Council. Details of the two menus were published in the 14th edition (1963) of Nutrition in Health and Disease by Cooper, et al.20 They are as follows:
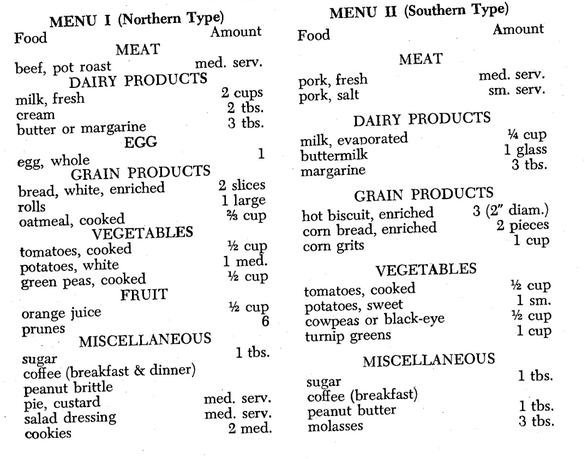
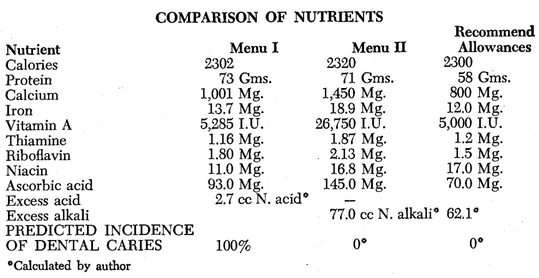
The extraordinarily high values for iron, calcium, vitamins A and C and excess alkali in Menu II (southern type) are due to turnip greens, sweet potato and molasses. They lend confirmation to the claim that greens and grasses are man’s most potent health protective foods.
As previously pointed out, one may eat pounds of fruits and vegetables of premium quality, and drink quantities of certified raw milk from pasture-fed cows and still not get enough fixed alkali to keep the reserve in the blood plasma at a safe level. Yet, no consideration is being given this aspect of our nutritional problems. After studying some of the histologic sections of dog tissues mentioned heretofore, the famed nutritionist, E. V. McCollum, Ph.D. of The Johns Hopkins University wrote the President of the Carnegie Corporation (which was supporting the Stomatological study at the University of California): “…It was very interesting to me, therefore, to learn that the work of the Stomatological Research Group has shown the possibility of producing experimentally a non-inflammatory type of paradontoclasia in the dog by a diet in which the basic ions were in excess. By modifying the inorganic relationships in the food, reconstructive changes could be induced in bones and tissues. This observation appears to be of capital importance as a starting point for further research.”15
The inorganic relationships in the food were modified by shifting potential reaction from alkaline to acid, or vice versa, and bone tissue was calcified and decalcified, at will (Plate III).
Potassium-Sodium Balance
Especially important among the interrelationships of the inorganic constituents of the blood is that of potassium and sodium, it appears. TOO LITTLE potassium, and, usually, TOO MUCH sodium have been implicated in the overproduction of the hormone aldosterone by the adrenal glands, which, in turn, is a contributing factor to high blood pressure, faulty carbohydrate metabolism and pseudo diabetes in many cases, according to Dr. Jerome W. Conn of the University of Michigan.16
It has long been known that a potassium deficiency causes microscopic lesions in muscle. The prevention of coronary thrombosis in infarct susceptible rats under stress by the administration of potassium salts as recently reported by the late Dr. Hans Selye, M.D., famed authority on stress, was dramatic–100% of the rats receiving potassium salts by stomach tube readily survived the stress, while 100% of the controls died.17
Potassium deficiency in the diet was implicated in the development of cancer more than 50 years ago by the British surgeon and cancer specialist, Forbes-Ross, who claimed that the administration of potassium salts was 100% effective in preventing cancer among his patients. He attributed the immunity of the natives in the West Indies to cancer to the high potassium content of sugar cane, which, he said, they “chewed prodigiously.”18
Potassium salts, in the form of enteric-coated tablets until recently prescribed for infarct-susceptible persons, were found to produce intestinal ulcers. Safety seems to lie in the consumption of more potassium-rich foods–greens and grasses, specifically–which are also highest in potential alkalinity and a more potent inhibitor of disease in warm blooded animals, including man.19
Findings in Pre-Civil War Days
In pioneer days and on the plantations in the “deep South” steaming dishes of “greens” and potatoes were diet staples, and a syrup stand filled with concentrated sugar cane or sorghum cane juices was an item of standard equipment on the family dining table for white and black alike. Medical and dental care were conspicuous by their absence. The plantation Negro was famed for his glistening, white, decay-free teeth. His fondness for his “mess-o-greens” and “long sweet’nen” (sugar cane syrup) was proverbial.
Though his diet–high in carbohydrate, soft in consistency, cooked in grease and sugar coated–was all WRONG as scored by today’s standards. However, when analysed from the standpoint of essential nutrients and potential reaction, it was adequate in all respects. According to the “Predictor,” its high degree of potential alkalinity assured freedom from tooth decay in practically 100 per cent of cases.
Findings at Annapolis
The writer, in collaboration with Captain H. E. Harvey, D.D.S., Senior Dental Officer in the United States Navy and Assistant to the Surgeon General, undertook a diet-teeth study of the 1937 class of midshipmen. Detailed dental examinations were made on the men at the beginning and at the end of the study period by specially appointed dental officers under the direction of Captain Harvey. The writer tested specimens of blood, urine and saliva from the 20 men who suffered the most active tooth decay; and analysed their diets, details of which were provided by the commissary officer.
The Academy had its own dairy and the men were allowed to drink milk, ad lib. The diet conformed in detail to the “Basic Seven” diet plan formulated by the Bureau of Human Nutrition and Home Economics, U.S. Department of Agriculture. It contained:
41.2 oz. whole milk or equivalent
15.0 oz. fresh or canned meat
1½ eggs
10.8 oz. citrus fruit and tomato
10.9 oz. other fresh and canned fruits
10.1 oz. leaf, green and yellow vegetables
18.5 oz. other fresh, canned and dried vegetables
11.7 oz. grain products
3.5 oz. butter
7.0 oz. sugar, syrups and preserves
This diet was exceptionally rich in protein, vitamins, calcium, phosphorus and iron and contained 7 cc N. alkali per 1000 calories. According to the “Predictor,” 80 per cent of the men would develop new caries. Actually, 81.1 per cent of them did, with the involvement of three times as many tooth areas as was reported in a comparable group of civilians. The high rate of tooth decay in the midshipmen was attributed to the combined effects of their low alkaline-ash ration and other factors incident to military training (stress, strenuous exercise, etc.) which tend to lower the body’s alkali reserve. Analysis of Army Field Ration “A” showed that it also conformed to the “Basic Seven” diet plan. It was adequate in all known essential nutrients and yielded an excess of 0.5 cc N. acid per 1000 calories. On that basis, it was PREDICTED that in case of war, if Army Field Ration “A” were used, the incidence of dental caries in our fighting forces would be 100 per cent, and that of related ills, increased.8 Autopsy findings on American GIs in Korea and Vietnam seem to substantiate the prediction.
Findings in Hawaii
The number of Polynesians resident in Hawaii in 1778 was estimated to be between 300,000 and 400,000. They were large in stature, had near perfect physiques, great physical strength and endurance, broad dental arches and beautiful, decay-free teeth–facts attested to by dental-skeletal remains. Their diet consisted of tropical vegetation–taro (root and leaf), sweet potato, a variety of “greens” and sugar cane, principally–and fish. It was high in carbohydrate and potential alkalinity, and undoubtedly adequate in all essential nutrients. With the influx of visitors to the islands and importation of grains and refined sugar, these foods gradually replaced native roots, tubers and sugar cane in the diet. Though the change did not materially affect the carbohydrate content of the diet, it shifted its potential reaction from strongly alkaline to acid. Disease and dental decay increased, apace. By 1928, the population of 300,000-400,000 people, who, for centuries, had enjoyed a state of physical-dental excellence said to be second to none the world had ever known, had dwindled to 20,000. Among the survivors (purebred) the differences in dentition in the children, especially, between those whose principal carbohydrate foods were taro and sweet potato and those whose carbohydrates came largely from grains, were striking.9,10,14 (see also Plate I, Fig. 1)
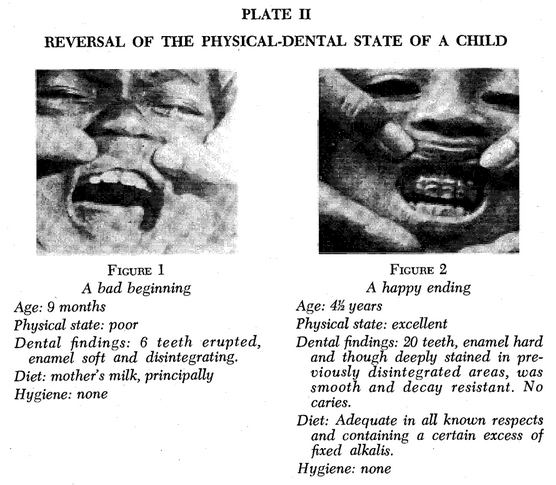
By 1928 Hawaii’s sugar cane and pineapple fields were being tilled by laborers from many lands, who also had adopted the “American style diet.” In their homelands dental troubles were unknown, many claimed. Some still enjoyed full complements of decay-free teeth, though tooth brushes were a luxury. Among the Hawaiian-born children tooth decay was rampant. Respiratory ills were universal and blood vessel disease common in elementary grade school children.11 The infant death rate was staggering. Babies were born with teeth so defective that they often disintegrated as they erupted, sometimes before the child had tasted food other than mother’s milk. (Plate II)
Blood Findings
Analyses of the blood plasma of expectant mothers and so-called “normal” young adults on the community diet: high carbohydrate, acid-forming though adequate for reproduction, lactation and growth, invariably revealed a low total base content and low alkali reserve–the same type of chemical imbalance found in the blood plasma of the dogs. Urine reactions were strongly acid.14:IV
Demonstration Infant Feeding Clinic
The similarity between the puppies in California and the preschool children in Hawaii in respect to diet and teeth, was so striking it was concluded that the causes were probably the same. (Plate I, Figures 1 and 2) That being true, all that was necessary to solve the distressing dental-health problems of the children, it appeared, was to put back native food: taro, sweet potato and whole sugar cane juice, principally, into the diet. This would not materially affect the carbohydrate content of the diet but would tremendously increase its potential alkalinity, a relatively large excess of which was apparently needed, to neutralize the acidifying effects of a tropical environment.
Plate I–Unlike Responses of Enamel and Dentin-Cementum to Nutritional Faults
To test this thesis, an infant feeding clinic was attempted in an isolated village of Filipino laborers and their families, on a sugar plantation. Though the adults were newcomers to Hawaii and many still had full complements of sound teeth–usually encrusted with food debris–the teeth of the children were obviously deteriorating. One in three babies born in the village died before its first birthday. Two months of hard work netted a single enrollee in the clinic–a pathetic nine month old boy whose newly erupting teeth were already disintegrating, though he was still breast-fed. (Plate II, Fig. 1) Four older brothers and sisters had died before attaining their first birthdays. Fear of also losing this baby prompted the mother to feed him the food that was prepared for him–gratis–at the clinic. The results were spectacular. Soon, all 33 babies under two years of age in the village were enrolled in the clinic. Health and teeth improved spectacularly as in the first child. NONE DIED. Morale in the village reached an all-time high. Warring neighbors became friends and community problems–heretofore settled with cane knives–were settled by discussion at the clinic. The dramatic success of the clinic prompted financial support and its extension to the entire pre-school population of the plantation.12 Results were duplicated. At its peak, 500 children from birth to 6 years of age were enrolled and fed in whole or in part by the clinic. A “flu” epidemic which prostrated the adult population by-passed clinic-fed children. The program accomplished the “impossible,” and attracted visitors from far and near. Application of these teachings on other plantations was instrumental in reducing their combined infant death rates from the highest to the lowest in the United States.
“Thumb Rule” for Diet Balancing
As indicated in Table I, whether one chooses an apple in preference to a banana; a serving of green peas rather than a serving of green lima beans; yellow corn on the cob rather than a dish of carrots; turnip root rather than beet root; kale rather than spinach; honey rather than sugar cane syrup, the calorie, protein and vitamin values of the diet will not be materially affected, but its potential alkalinity will be. If all the alkali-poor foods mentioned were chosen, the excess alkali contributed to the diet would amount to approximately 13 cc N. alkali. If the alkali-rich foods were chosen, they would provide approximately 77 cc N. alkali. Assuming that the remainder of the diet–milk, meat, egg, grain products, etc.–yielded a neutral ash, the graph indicates that the incidence of tooth decay in a group eating the alkali poor foods–regardless of their excellence in other respects–would be approximately 84 per cent while nearly 100 per cent of those eating the same types (leaf, green, yellow, etc.) but alkali-rich varieties would be caries free.
This points up the importance of a working knowledge of the fixed acid-alkali contents of one’s diet, and explains the varying results one may get on diets consisting of premium quality foods chosen in accordance with the “Basic Seven” or “Basic Four” Diet plan.
It emphasizes the role one’s food likes and dislikes play in physical well being. Most DISLIKED, probably, today, are man’s most potent health protective potassium, alkali-rich foods–thin green leaves (turnip and beets tops, mustard greens, spinach, etc.) and grasses (sugar cane and sorghum cane juices). Diet staples of uncounted millions of people throughout the centuries, as well as of our own pioneer ancestors, are conspicuous by their absence in today’s diet. That their restoration to it would be a contribution of the first magnitude to our national health, there can be no doubt.
“Thumb Rule” for Balancing the Diet
- More fruits and vegetables in summer than in winter seasons, and more in hot climates than in cold; that is, the more vitamin D from the sun, the more the alkali-ash foods, and vice versa.
- Proportionately more fruits and vegetables in the diet of the child than in that of the adult.
- In general, two servings of fruits and vegetables for every serving of meat, fish, egg or cereal for the growing child in temperate climates. Let one of every five servings of vegetable or fruit be the alkali-rich thin green leaf variety of vegetable or grass (sugar cane or sorghum cane syrups).
Is Dental Disease Predictable?
The evidence presented says YES! Furthermore, it emphasizes the importance of an understanding of the interrelationships of both organic and inorganic constituents of one’s blood as affected by the acid-base balance of the diet. The association of an alkali deficiency in one’s diet with an alkali deficiency in blood plasma, rampant tooth decay and high susceptibility to respiratory and other diseases in all the studies cited, forces the conclusion that this type of chemical imbalance in blood plasma may be the starting point of many of today’s diseases of obscure origin. This conclusion is strengthened by the arrest of tooth decay and spectacular improvement in the physical well-being of the plantation children when the potential reaction of their diet was shifted from acid to alkaline by the replacement of high carbohydrate acid-forming grains and refined sugar, with high-carbohydrate alkaline-ash roots, tubers and sugar cane juice. (Plate VI)
Plate VI–Try This With Your Own Babe
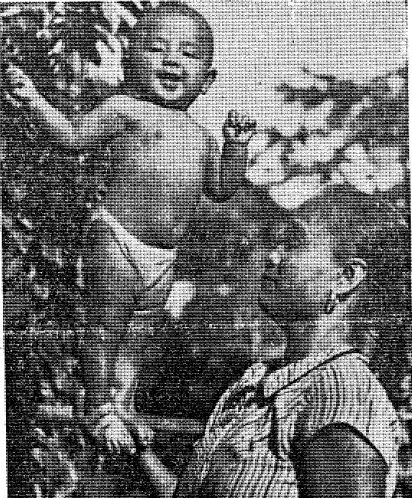
There’s no fake about this. Beatrice Calivo, whose father is a laborer on the Ewa plantation, at the age of 3½ months learned how to balance upright on her mother’s hand, a believe it or not achievement that aroused the greatest interest at the plantation clinic under whose supervision Beatrice is reared. This photograph showing sturdy Beatrice and her mother was taken when Beatrice was 4½ months young. Since birth she has thrived on a balanced diet recommended by the clinic’s director, Dr. Martha Jones. A feature of the diet is a new food, a composition of sugar juice and pei, which is prepared at the clinic and used with whole milk. Beatrice today is the pride of the famed clinic.–Star-Bulletin photo.
Diets consisting of premium quality foods as advocated in the “Basic Four” food groups, and chosen so as to ensure a certain excess of fixed alkalis (potassium, particularly) in accordance with individual needs (age, activity, climate, emotional state, stress, etc.) would alleviate much suffering, increase resistance to dental and related diseases and undoubtedly add many years of useful life to uncounted millions, and life to their years, as well. To this, the writer’s personal experiences attest.
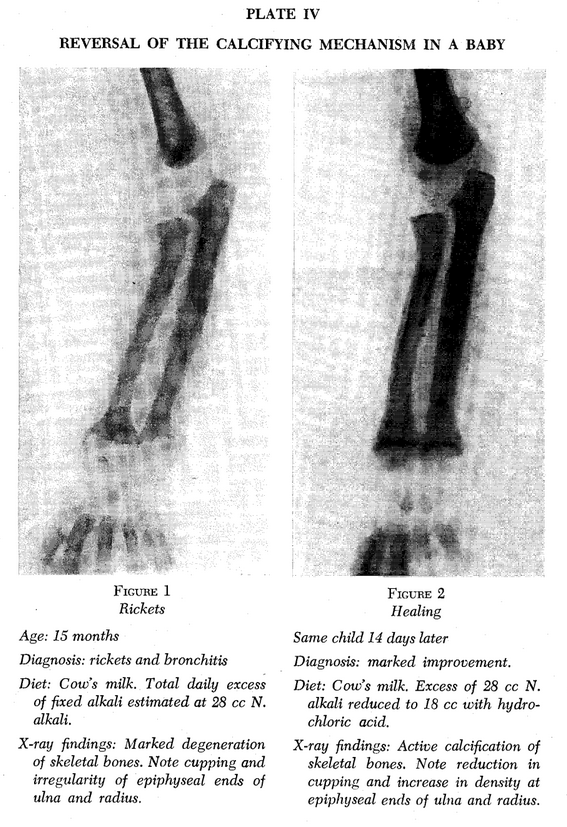
Plate V–Effect of Starvation Acidosis on the Unerupted Teeth of a Four Month Old Baby
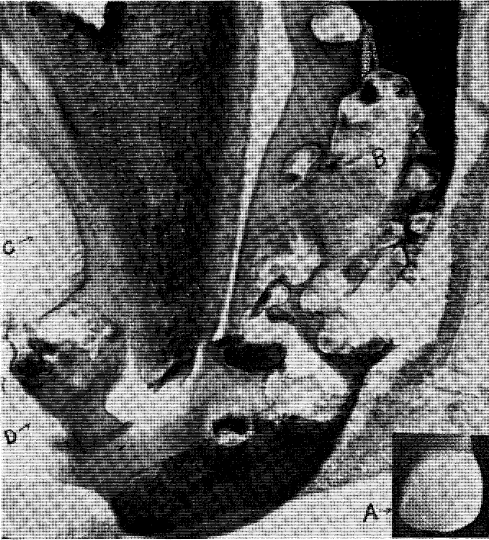
Enlarged photomicrograph of incisal tip of the right central incisor sectioned longitudinally, labio-lingually, through the middle lobe. A photograph of the dissected companion tooth is shown in the inset at “A”. The darkened area in Fig. “A” is probably more of the same kind of enamel disintegration shown in the photomicrograph.
The specimen was torn in sectioning, but no teeth were erupted, and there was no evidence, anywhere, of bacterial activity in the tooth crypts. Note the large oval at “B”. It appears to have been formed by the coalescence of numerous disintegrating areas in the enamel in which islands of matrix are still present. On the lingual side at “C”, only a fringe of enamel remnants remain. Cellular tissue has grown into the matrix at “D”. The dentin layer throughout–”E”–was intact and surprisingly well formed.
History: The baby was a full term, apparently normal infant born to an unwed Japanese teenager and was sold to an old, childless, Chinese couple. Fearing the authorities would not allow them to keep the baby, they kept it hidden, and fed it “rice-water” until it died at the age of four months.
Martha Richardson Jones is a native of Tennessee, and a lineal descendant of Richard Lee, first attorney general of the American Colonies. She received the Bachelor of Science and Master of Arts degrees from Peabody College. This was followed by three years of study at Vanderbilt University. From Yale University she received the degree of Doctor of Philosophy.
Dr. Jones has devoted her professional life to research in nutritional diseases. Among her professional assignments are the following :
Assistant, Department of Physiological Chemistry (first woman), Yale, 1918-20.
Research Associate, Department of Pediatrics at the University of California
Medical School, 1920-1928.
Research Associate, The Queen’s Hospital, Honolulu, Hawaii, 1928-36.
Organizer and director of the Ewa Plantation Health Project, Hawaii, 1929-36.
Director, “Diet and Teeth” research, Pan Pacific Women’s Association, 1928-36.
Associate with Captain H. E. Harvey, U.S.N., diet and teeth study of midshipmen, U.S. Naval Academy, Annapolis, 1936-37.
Dr. Jones is also Founder-Director of THE MARTHA R. JONES FOUNDATION for
Health Education; associated with Asbury Theological Seminary; Wilmore, Kentucky.
She has contributed to leading medical, dental and scientific journals.
Editor’s note: Since the era in which this article was written, society’s understanding of respectful terminology when referring to ethnic and cultural groups has evolved, and some readers may be offended by references to “Negro” people and other out-of-date terminology. However, this article has been archived as a historical document, and so we have chosen to use Jones’ exact words in the interest of authenticity. No disrespect to any cultural or ethnic group is intended.
References Cited:
- Jones, Martha R.: “Dental caries, the ‘handwriting’ in the mouth,” Journal of Dental Research. 22:2 (June) 1943.
- Jones, Martha R.: “Our changing concept of an ‘adequate’ diet in relation to dental disease.” Dental Cosmos: June, July, August, 1935.
- Jones, Martha R., and Simonton, F. V.: “Mineral metabolism in relation to alveolar atrophy in dogs.” Journal of American Dental Assn. May, 1928.
- Jones, Martha R.: “Studies on inorganic salt metabolism. II. The effect of the sudden alteration of the acid-base balance of the diet in dogs.” Proceedings of the Society for Experimental Biology and Medicine, XXIII. pp. 578-561, 1926.
- Thompson, C. E. and Staack, H. F.: “Executive health–diagnostic study of 600 executives.” Industrial Medicine and Surgery. 25:#4, April, 1950.
- Culbert, R. W., and Jacobziner, H.: “What does the school physician see?” American Journal of Public Health. 40:#5, May, 1950.
- Sherman, H. C.: Chemistry of Food and Nutrition. MacMillan Co., 1932.
- Jones, Martha R.: “The soldier’s mess in relation to dental caries.” Journal of Dental Research. 22:#3, June, 1943.
- Jones, Martha R., Larsen, N. P., and Pritchard, G. P.: “Taro and sweet potato versus grain foods in relation to health and dental decay in Hawaii.” Dental Cosmos. April, 1934.
- Larsen, N. P.: “Teeth.” Plantation Health Bulletin. July, 1937.
- Jones, Martha R.: Unpublished Health Survey, Ewa Plantation Elementary School.
- Jones, Martha R.: “Report of dietary observations carried on at Ewa Plantation 1932-33.” Bulletin No. 1, Hawaiian Sugar Planters Assn.
- Simonton, F. V., and Jones, Martha R.: “Odontoclasia.” Journal of the American Dental Association. June, 1927.
- Jones, Martha R., Larsen, N. P., and Pritchard, G. P.: Dental disease in Hawaii:
- A clinically unrecognized form of tooth decay in the pre-school child of Honolulu. Dental Cosmos. May, 1930.
- Dental findings in pre-school Polynesian, Japanese and Filipino children in rural districts of the Island of Oahu. Dental Cosmos. June, 1930.
- Factors in dental decay in pre-school children of certain races resident in Honolulu and rural Oahu. Dental Cosmos. July, 1930.
- The acid-base balance of the blood in relation to dental decay and alveolar atrophy. Dental Cosmos, August, 1930.
- “Can unerupted teeth decay?” Journal American Medical Assn. Nov. 26, 1932.
- “The relationship between bone and tooth development in infants.” American Journal Diseases of Children. April, 1933.
- Simonton; F. V.: “The Carnegie research group and forty years of periodontology.” Journal California State Dental Assn. and Nevada Dental Society, Oct.-Nov. 1959.
- Conn, Jerome W.: “Diabetes and blood pressure.” Lecture, New England Diabetes Assn. Time: Dec. 3, 1965.
- Selye, Hans: The Chemical Prevention of Cardiac Necrosis. New York Ronald Press Co., 1958.
- Ross, F. W. Forbes: Cancer, The Problem of Its Genesis and Treatment. Methune and Co., Ltd., London, England. 1912.
- Boley, S. J. et al: “Potassium-induced lesions of the small bowel.” Journal American Medical Assn. Sept. 20, 1965.
- Cooper, L. F., Barber, E. M., Mitchell, H. S., Rynberger, H. J., Greene, J. C.: Nutrition in Health and Disease. 14th edition, 1963. Lippincott Co., Philadelphia.
- Weber, Thos. B. et al: Instrumentation Methods for Predictive Medicine, Instrument Society of America, Pittsburgh, Penn., first edition 1966.
- Hawkins, Harold F.: Applied Nutrition, Lee Foundation, Milwaukee, Wisconsin, first edition 1947.