
Access to all articles, new health classes, discounts in our store, and more!
Infection in Filled, Vital, Roentgenographically Negative Teeth
Published in the Cincinnati Journal of Medicine, pp. 329-339, October 1944.
* * *
The importance of infected teeth as a cause of systemic disease may be considered as established. Pulpless teeth, irrespective of whether they gave roentgenographic evidence of changes, have been proved to harbor specific types of streptococci. These streptococci on injection into animals, tend to localize and produce disease resembling that of the patient from whom the teeth were removed.2,4,6,9,10,11,14,15 Intact vital teeth, free from caries or fillings, which had been removed in a sterile manner, have been shown to be essentially sterile.1,5,16 The removal of pulpless teeth often results in improvement of patients ill with systemic diseases due to streptococci,13,14 but unfortunately this does not occur invariably. Some patients who had not been benefited by removal of pulpless teeth and other foci of infection have improved after removal of roentgenographically negative teeth that contained large restorations and that responded to vitality tests.3,7,8,13
The results obtained from a recent bacteriologic and histologic study of seven vital teeth with fillings and of diseased bone in which some of the teeth were embedded are so striking it was felt that a brief report should be made in the literature to stimulate others to use the technic here employed.
Report of Case
The patient, a physician, sixty-eight years of age, had had repeated attacks of neuromyositis, bursitis and mild arthritis at widely separated intervals for many years, but otherwise had remained in excellent health. After removal of one or two pulpless teeth from which streptococci were isolated, these recurring attacks disappeared promptly and remained absent for years.
During the past two years there was a mild recurrence of similar symptoms associated with a lack of endurance, increasing tremor of one hand, a persistent foul breath and dull aching pain in the mandible, especially surrounding teeth containing large restorations, to which bridges were attached. There were no pulpless teeth. All upper teeth had been removed some years before and a well-fitting denture functioned satisfactorily. The tonsils had been cleanly removed many years before. There was no evidence of sinusitis or prostatitis.
Roentgenograms of the upper jaw (fig. 1) showed no residual areas of infection. The mucous membrane over the alveolar process appeared normal and there was no tenderness on palpation. Five of the lower teeth had been removed, four of them about six years before. One, the right lower second bicuspid which had contained a deep gold inlay (fig. 1) and supported the anterior end of a bridge containing three teeth, was removed seven months before, twelve hours after several sharp twinges of pain suggestive of acute pulpitis had occurred during an attack of neuromuscular pain. After its aseptic removal, the tooth was split in a rigid vise with sterile technic, and the apex and the pulp, which were found severely congested, were cultured. A pure culture of streptococci was isolated in dextrose-brain broth and dextrose-brain agar. The dextrose-brain agar showed many colonies. In serial dilution cultures,12 growth occurred in extremely high dilutions of the suspension of the crushed apex. Two rabbits were inoculated, one intracerebrally with 0.1 c.c. of a 1:10,000 dilution of the culture from the pulp and the other intravenously with 10 c.c. of the undiluted primary dextrose-brain broth culture from the apex. Lesions of muscles, fascia and periarticular structures developed in both animals.
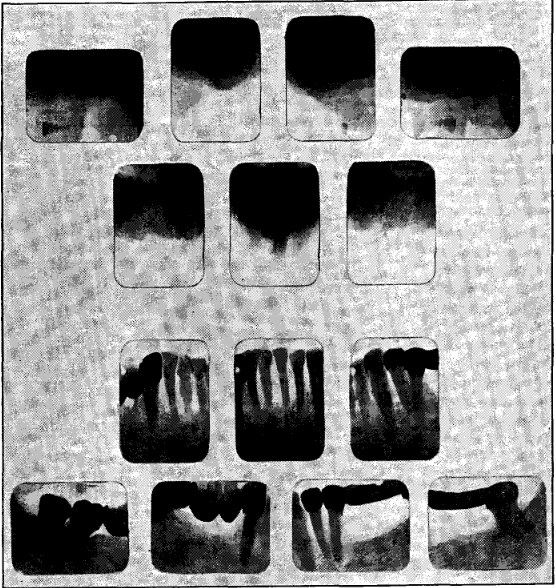
Fig. 1. Roentgenograms of the edentulous maxilla and of the teeth in the mandible or the patient concerned in this report. The pictures were taken one year before this study was made.
Following extraction of this roentgenographically negative tooth, an exacerbation of neuromuscular pain occurred but except for a second mild attack two weeks later there was relative freedom from symptoms for several months. Then similar attacks associated with undue fatigability again occurred.
Examination of the eleven remaining teeth in the lower jaw revealed that five of the anterior teeth were free from fillings, whereas all of the other six teeth contained from small to large gold fillings (fig. 1). Two of the teeth, the left lower second bicuspid and the second molar, harbored deep gold inlays to which a contact bridge containing two teeth was attached. The left third molar was capped with a large, shallow gold inlay. The left lower cuspid contained a small gold filling near the margin of the gum. The right lower second bicuspid harbored an anteroposterior gold inlay and the crown of the right lower third molar was largely replaced by a gold inlay to which the three-tooth bridge had been attached for many years, until seven months previously. Aside from moderate recession of the alveolar process under the bridge adjacent to the left lower second bicuspid and molar, roentgenograms were considered negative (fig. 1). All of the eleven teeth responded to vitality tests and in consequence were considered normal by the best dentists and exodontists, and as having nothing to do with the recurring symptoms of which the patient complained. The dull pain in the jaw was considered as being due to trauma from an unusually powerful bite. The foul breath, which could not be dispelled by most thorough brushing of teeth, was attributed to coating of the tongue and to advancing age.
Despite diminution in the amount of work and abundant rest, the episodes of neuromuscular pains and fatigability increased in severity. Sensitiveness to cold developed in several teeth and was associated with twinges of sharp pain.
It was during this time, at the advice of Dr. Martin H. Fischer and Dr. Maynard Murray of Cincinnati and several of their colleagues, that the patient consented to removal of the six filled teeth and surrounding diseased bone. This was done at one sitting by Dr. Murray under local block anesthesia. Two abscesses containing foul smelling pus were found under the bridge and one was found at the lingual side of the roots of the third right molar, so situated that roentgenograms could not reveal its presence. The bone surrounding these abscesses was badly and deeply infected. This bone and the alveolar processes surrounding the remaining teeth were removed surgically.7,8 Under the expert aftercare administered by Dr. Fischer, in which healing from the bottom was assured,3 without pocketing of infection, recovery from the operation was uneventful. Exacerbation of constitutional symptoms did not occur soon after operation nor has it occurred in the four months since the operation. The recurring attacks of dull pain in the lower jaw, the twinges of pain followed by neuromuscular pains, the foul breath and the undue fatigability have disappeared. A lower partial plate and a new upper denture to match have been made and already function satisfactorily.
Methods of Study
The six extracted teeth and pieces of diseased bone which were removed were wrapped in sterile gauze and dispatched by air mail to my laboratory in Rochester, Minnesota. On their receipt the following morning, the teeth were first washed in sterile saline solution. The apices then were severed, placed in a sterile mortar and crushed and a small amount of dextrose-brain broth was added. Cultures of the fragments and of the suspension were made in tall columns of dextrose-brain broth, by the serial dilution method in tall columns of dextrose-brain agar (0.2 per cent dextrose and 0.2 per cent agar) and on blood-agar plates. The teeth then were placed in 10 per cent formalin for one week. The pulps then were removed after splitting the teeth in a large rigid vise; care was taken not to crush the pulp. Three pulps that showed gross hemorrhages were photographed (fig. 2) and then placed in 10 per cent formalin and sectioned. Sections were stained with hematoxylin and eosin for lesions and by the Brown and modified Gram methods for micro-organisms. The modification of the Gram method consisted of deep staining of sections with gentian violet and then decolorizing to a fair blue with alcohol instead of to the end point as is usually done. Pieces of diseased bone and the fragments of the roots were placed in 10 per cent formalin, decalcified and embedded in paraffin. Sections were made and similarly stained for changes and for micro-organisms.
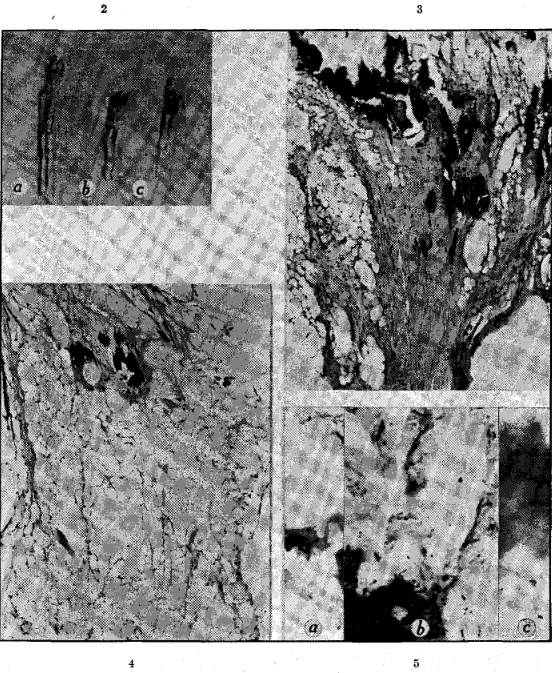
Fig. 2. Pulps of three extracted vital teeth: a, from the left lower cuspid which had only a small gold filling near the margin of the gum; b, from the left lower second molar; c, from the right lower third molar. The last two teeth had deep gold restorations. Hemorrhage may be noted near the apical end of a, in the middle portion of b and three hemorrhages in the body of the pulp in c (unstained x2).
Fig. 3. Pulp shown in figure 2c. Extreme calcareous and fatty degeneration and slight cellular infiltration may be noted (hematoxylin and eosin stain x85).
Fig. 4. Pulp from the left lower molar shown in figure 2b showing calcareous, hyaline and fatty degeneration with only slight or no cellular infiltration (hematoxylin and eosin stain x85).
Fig. 5a and c. Diplococci; b, pleomorphic diplostreptococci and fusiform bacilli. All were found adjacent to regions of calcareous degeneration in the pulp shown in figures 2c and 3 (Gram stain x1,000).
Results
A pure, or nearly pure, culture of green-producing streptococci was obtained in dextrose-brain broth and in dextrose-brain agar in serial dilution cultures from the suspension of the crushed apices of each of the six teeth, whereas cultures on blood agar remained sterile. The number of colonies of streptococci that grew in the first tube of dextrose-brain agar varied from nineteen in the culture from the left lower cuspid, to 1,600 in the material from the right lower third molar, and to 2,800 in the material from the left lower second bicuspid. Serial dilution cultures were made with the same pipet, by increasing the dilution of inoculum a hundredfold at every step. No growth occurred in the second tube in serial dilution cultures of the four teeth from which only a few colonies grew in the first tube. Growth occurred in the third tube, representing a dilution of 1:10,000, in the material from the right lower third molar, and in the fourth tube, representing a dilution of 1:1,000,000, in material from the left lower second bicuspid.
Four rabbits were inoculated with a mixture of five-hour dextrose-brain broth cultures of the streptococci obtained from the end point of growth in the serial dilution cultures from four of the teeth. Three rabbits were given 10 c.c. intravenously of the undiluted culture and one was inoculated intracerebrally with 0.1 c.c. of a 1:10,000 dilution made immediately before inoculation in sterile dextrose-brain broth. All of the three that received the intravenous injection became muscle-sore within four days at which time they were killed. Immediate examination revealed moderate to large numbers of necrotic, whitish streaks in muscles, chiefly in the flat muscles of the chest and abdomen and in tendinous ends of muscles of the extremities. Hemorrhages were found in the fascia, periarticular structures, muscles surrounding the exit of spinal nerves, periosteum and, in one instance, in the periosteum opposite the apices of hemorrhagic pulps of lower incisors. In one rabbit a few small hemorrhages were found in the tricuspid valve. The fluid from the knee of one animal was slightly cloudy. There were no lesions of lungs, stomach, duodenum, adrenal glands, kidneys, gallbladder, urinary bladder or myocardium. Cultures made of synovial fluid and blood of the three rabbits were negative. Cultures from the brain of one and from tissue from knee joints of two revealed streptococci. Mild symptoms of encephalitis followed by characteristic spasmodic torticollis developed in the rabbit that was inoculated intracerebrally. It was killed ten days after inoculation. No lesions of muscles, joints or viscera were found. Cultures in dextrose-brain broth of pipettings from the brain yielded streptococci.
Four mice also were inoculated; two intraperitoneally, each with 1.2 c.c. of the undiluted mixture of cultures from the four teeth, and two intracerebrally, each with 0.03 c.c. of a 1:100 dilution. One of the mice that was inoculated intraperitoneally died on the second day. On examination a large amount of pleural fluid was found, from which streptococci were isolated in dextrose-brain broth. There was no gross peritonitis. The remaining three mice remained well.
The symptoms and gross lesions of inoculated rabbits and the results of cultures indicated that three types of streptococci (neurotropic, arthromyotropic and pneumotropic) were isolated from the apices of the teeth, corresponding, in general, to two types of symptoms which the patient had had —tremors, fatigability and pains in joints and muscles— and to a seasonal type of pneumotropic infection against which the patient had been vaccinated.
These findings were so definite that a serologic study was made of the streptococci isolated. The following serums were used in fivefold dilutions (1:2 to 1:1,250) in agglutination tests: antistreptococcic serums prepared in horses with the respective streptococci isolated in studies of encephalitis, arthritis, and colds and influenza; the patient’s serum obtained on the eleventh day after operation; the serum of a rabbit in which mild symptoms of encephalitis and spasmodic torticollis had developed, that was obtained ten days after intracerebral inoculation with the strain of the streptococcus that had been obtained from the patient’s teeth; and as controls, normal human serum, normal rabbit serum and normal horse serum. Five strains of streptococci from five teeth, two strains from brain and two from joint tissue of inoculated rabbits, and two from the pleural fluid of inoculated mice were used in the agglutination tests.
Three of the five strains of streptococci obtained in cultures from the teeth (a mixture of these had been inoculated in animals) were agglutinated maximally by the encephalitis antistreptococcic serum, one by the cold and influenza antistreptococcic serum and one by the arthritis antistreptococcic serum. None was agglutinated by normal horse serum. The strains from the brains of inoculated rabbits were agglutinated specifically by the encephalitis antistreptococcic serum (neurotropic), those from the joint tissues of rabbits were agglutinated specifically by the arthritis antistreptococcic serum (arthrotropic) and those from the pleural fluid of mice were agglutinated specifically by the cold and influenza antistreptococcic serum (pneumotropic). The patient’s serum agglutinated to a greater degree than did normal human serum each of the three types of streptococci. The serum from the rabbit, in which mild symptoms of encephalitis and then of spasmodic torticollis had developed, agglutinated to a greater degree than did the normal rabbit serum the strains isolated from the brains of inoculated rabbits.
Gross examination of the pulps after the teeth had been in 10 per cent formalin revealed hemorrhages in three (fig. 2) and a large pulp stone enmeshed in the pulp of the right lower third molar.
The results of microscopic examination of sections of the pulps and infected bone are well illustrated in figures 3 to 9. The chief histologic changes (figs. 3 and 4) consisted of fatty, hyaline and calcareous degeneration with little or no cellular infiltration, which were roughly proportional to the size of the restoration. Streptococci were demonstrated in the pulps of all six teeth; the number was roughly proportional to the degree of changes in the pulp and to the size of the gold restorations (figs. 5 and 6). They were not demonstrable in the regions of calcareous degeneration but were found most readily and in greatest number immediately surrounding such degeneration (figs. 5 and 6a and b). Especially noteworthy was the presence of a mural thrombus, rich in leukocytes, in which large numbers of diplococci were found, in a blood vessel in the pulp of the left lower cuspid (fig. 6c). A small gold filling had been placed in this tooth near the margin of the gum many years before. Bacteria were not demonstrable in the dense portion of decalcified roots but were found in the superficial layers toward the apical end.
The results of examination of the decalcified bone and of search for bacteria are well illustrated in figures 7, 8 and 9. Bacteria were found in large numbers in the walls of the abscesses and tissues showing cellular infiltration far remote from the abscesses (figs. 8 and 9), but were not demonstrable in the dense areas of condensing osteitis nor free in the cysts.
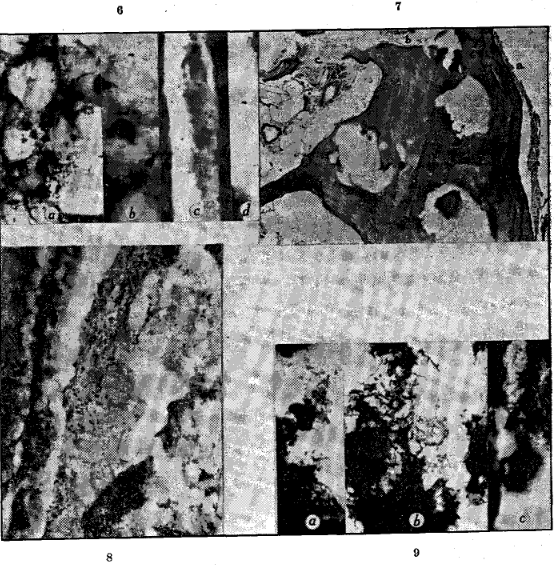
Fig. 6. Pleomorphic diplococci; a and b, in the pulp from the left lower second molar surrounding regions of calcareous degeneration shown in figure 4; c, in a mural thrombus of a blood vessel in the pulp of left lower cuspid shown in figure 2a and d, in the degenerating pulp of the left lower second bicuspid to which a contact bridge was attached (Gram stain x1,000).
Fig. 7. Bone which surrounded the abscess adjacent to the left lower second bicuspid to which the contact bridge was attached anteriorly. Areas of necrosis and dense cellular infiltration (a, b and c). The cystic degeneration and the condensing osteitis should be noted (hematoxylin and eosin stain x100).
Fig. 8. Innumerable diplococci, sometimes in short chains, in area of infiltration in region marked “a” in figure 7 (Gram stain xl,000).
Fig. 9. Fusiform bacilli, pleomorphic diplococci and streptococci; a and b region of infiltration at b and c in figure 6; c in region of necrosis of bone adjacent to left lower second molar to which the saddle bridge was attached posteriorly (Gram stain x1,000).
Comment
By the use of special methods, the apices and pulps of filled, roentgenographically negative vital teeth that were considered to be free from infection were found to be infected by streptococci having specific virulence and serologic properties. The bone in which the infected teeth were embedded showed condensing osteitis, cystic degeneration, localized regions of necrosis and leukocytic infiltration in which large numbers of streptococci and fusiform bacilli were found. Since the streptococci that grew in the brain-containing mediums had specific localizing power and they did not grow on blood agar, and since they were agglutinated specifically by the patient’s convalescent serum, it may be concluded that the streptococci isolated were not contaminants.
The symptoms of the patient disappeared promptly after removal of these teeth and surrounding bone and agglutination tests showed an increase in specific antibody titer of his serum for the streptococci isolated which indicate that in this case x-ray negative, vital teeth having large restorations were a local and systemic source or focus of infection.
References Cited:
- Austin, L. T. and Cook, T. J.: Bacteriologic study of normal vital teeth. J. Am. Dent. A. 16:894-896 (May) 1929.
- Cook, T. J.: Focal infection of the teeth and elective localization in the experimental production of ulcerative colitis. J. Am. Dent. A. 18:2290-2301 (Dec.) 1931.
- Fischer, M. H.: Death and dentistry. Springfield, Illinois, Charles C Thomas, 1940, chap. 8, pp. 115-140; chap. 9, pp. 141-196.
- Haden. R. L.: Dental infection and systemic disease. Philadelphia, Lea & Febiger. 1928, 165 pp.
- Henrici, A. T. and Hartzell, T. B.: Bacteriology of vital pulps. J. Dent. Research. 1:419-422 (Dec.) 1919.
- Meisser, J. G. and Gardner, B. S.: Elective localization of bacteria isolated from infected teeth. J. Nat. Dent. A. 19:578-592, 1922.
- Murray, Maynard: Relation of foci of infection to some allergic states. Cincinnati J. Med. 23:211-214 (July) 1942.
- Murray, M. and Papesch, W. C.: The relation of dental disease to sinusitis. Laryngoscope. 53:366-369 (May) 1943.
- Nickel, A. C. and Hufford, A. R.: Elective localization of streptococci isolated from cases of peptic ulcer. Arch. Int. Med. 41:210-230 (Feb.) 1928.
- Rhoads, P. S. and Dick, G. F.: Roentgenographically negative pulpless teeth as foci of infection; results of quantitative cultures. J. Am. Dent. A. 19:1844-1593 (Nov:) 1932.
- Rosenow, E. C.: Studies on elective localization; focal infection with special reference to oral sepsis. J. Dent. Research. 1:205-249 (Sept.) 1919.
- Rosenow, E. C.: Isolation of bacteria from virus and phage by a serial dilution method. Arch. Path. 26:70-76 (July) 1938.
- Rosenow, E. C.: Focal infection and elective localization in relation to systemic disease: a review and results of further studies. Proc. Dent. Centenary Celebration. (Mar.) 1940, pp. 261-282.
- Rosenow, E. C. and Meisser, J. G.: The production of urinary calculi by the devitalization and infection of teeth in dogs with streptococci from cases of nephrolithiasis. Arch. Int. Med. 31:806-829 (June) 1923.
- Swanson, W. F. and Van Kirk, L. E.: Results of culturing 1800 pulpless teeth. J. Dent. Research. 15:315 (Sept.) 1936.
- Tunnicliff, Ruth and Hammond, Carolyn: Presence of bacteria in pulps of intact teeth. J. Am. Dent. & Dent. Cosmos. 24:1663-1666 (Oct.) 1937.