
Access to all articles, new health classes, discounts in our store, and more!
Fabric Of Man
Published in Journal of the American Society for Preventive Dentistry, 1975
* * *
Introduction
The one incontestable feature of periodontal disease is that it begins early in life and, with advancing age, there is an increase in its frequency and severity. This is pictorially portrayed in Figure 1 with age on the abscissa and periodontal pathosis on the ordinate. The line marked natural course describes the introductory statement. The other item not mentioned as often is that the variance also enlarges with time as shown by the widening gray zone (Figure 1). This graphically supports the well-recognized observation that some old people have less periodontal disease than other young people.
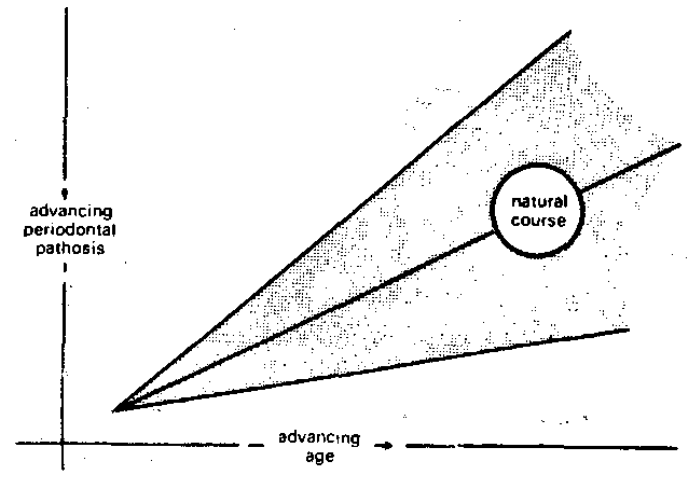
Figure 1
The therapeutic armamentaria presently available to the practitioner accomplishes, primarily, a slowing of periodontal destruction. In some instances the process may be arrested and occasionally some degree of reversal may take place (Figure 2). These three end-results collectively may be considered secondary prevention (prevention of recurrence). If this therapeutic knowledge were applied earlier in life, it would actually serve to prevent periodontal disease. The latter is properly designated primary prevention (prevention of occurrence). Prevention of periodontal disease, however defined, is only possible through an understanding of the etiology of the syndrome.
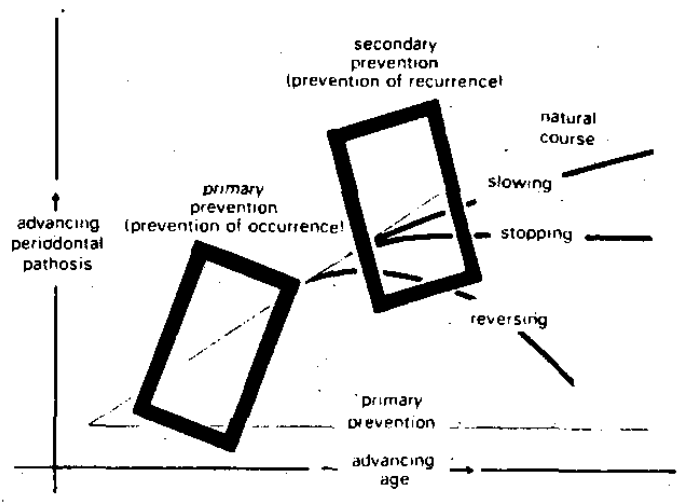
Figure 2
Etiology of Periodontal Disease
“Periodontal disease can be considered as the morbid response of the periodontal tissues to extrinsic local irritants. This response, in turn, is modified by intrinsic-systemic conditions operative within the host. Periodontal disease, therefore, represents the interaction of a variety of etiologic factors which differ in degree of significance at every pathologic site in every patient.”
This citation1 serves as an excellent working hypothesis to develop an approach to the prevention of periodontal pathosis. The intent of this report is to crystallize a practical technique for the abolition, to the extent possible, of periodontoclasia.
From the equation, it is clear that two therapeutic avenues are available (Figure 3). The first approach is to reduce the local-extrinsic irritants to zero (Figure 4) with no attention accorded the intrinsic-systemic variables. If this can be done, then no periodontal pathosis can occur since any value for the host state multiplied by zero must net zero. The second possibility is to erase all host factors (Figure 5) with no attention given to the local environment. At least, on a mathematic basis, no periodontal disease could ensue. Finally, if the two earlier approaches, while hypothetically ideal, are singly impractical, then minimizing both the local and host factors may conceivably yield the best possible practical end-result.
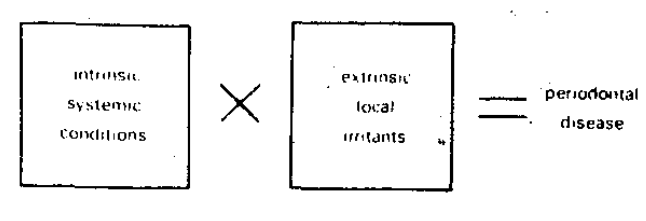
Figure 3

Figure 4
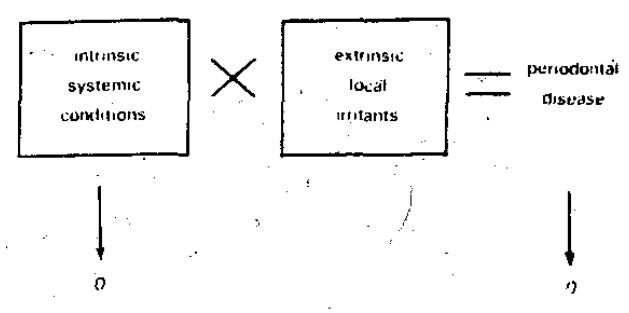
Figure 5
Method of Investigation
The human organism can be employed as a realistic experimental model to ascertain the relative effects upon periodontal pathosis when the host and the environment are modified singly and in combination. For example, in one group of subjects, prophylaxis can be performed in one-half of the mouth. A before-and-after appraisal would thus allow an evaluation of the effect of removing debris on any one of a number of parameters of periodontal state (e.g., gingival inflammation, sulcus depth, tooth mobility). Additionally, by this technique, it is possible to estimate the recorder’s reliability since one-half of the mouth is not scaled.
It is also possible to modify host state in several different ways (e.g: nutrients, hormones) along with prophylaxis in one-half of the mouth. A before-and after examination would ascertain the relative effects upon one or another periodontal parameter (e.g. gingival inflammation) of a vitamin, for example, with and without prophylaxis.
Thus, by this technique, a reasonably well-controlled study in man can be developed to show the relative effects of: (1) nothing, meaning no prophylaxis and no host change, (2) scaling with no host alteration, (31 host influences with and environmental change, and (4) combined host and local influences.
Secondary Prevention
Consideration will first be accorded secondary prevention because (1) it is the area most commonly discussed, (2) it is the subject which has been most investigated, (3) it is the zone in which the most dramatic changes have been discovered, and (4) because secondary prevention and prevention are frequently held to be synonymous.
Utilizing the experimental model previously outlined, it is a relatively simple matter to demonstrate the pattern of secondary prevention. For example, one study2 compared the effect of prophylaxis versus no prophylaxis in 25 presumably healthy subjects given a placebo with prophylaxis versus no prophylaxis in a like group of 25 subjects provided with a natural vitamin C with bioflavonoid supplements. Figure 6 shows no significant change (-10%) following no prophylaxis with placebo; in contrast, a statistically significant 30 per cent improvement with prophylaxis and placebo. Figure 6 also demonstrates that the greatest improvement (71 per cent reduction) followed the combined local and host treatment. Figures 7 and 8 demonstrate essentially the same trends with regard to sulcus depth3 and clinical tooth mobility4, respectively.
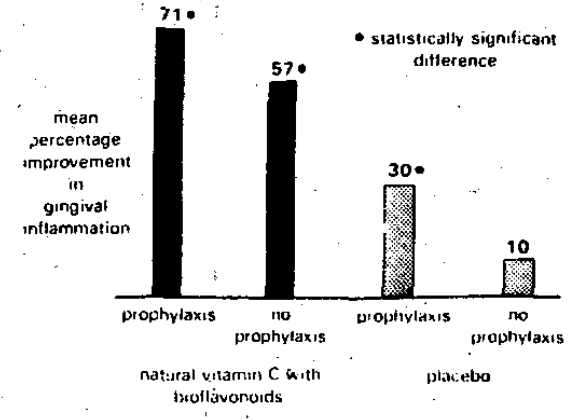
Figure 6
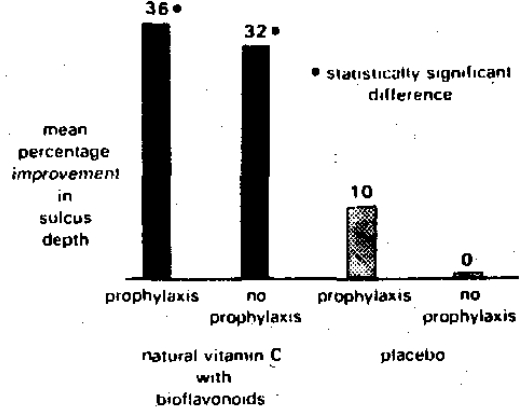
Figure 7
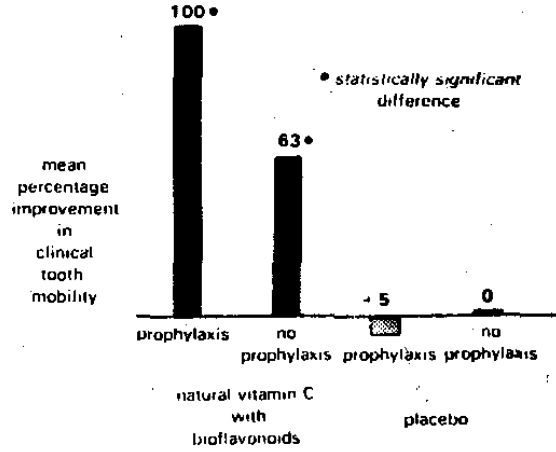
Figure 8
The point of the story is that the usual sequence of events (Figure 2) can be slowed, stopped, or reversed by means of local therapy, usually in the form of reducing the local-extrinsic irritants. The evidence from these limited studies show that the same slowing, stopping or reversal can be accomplished by host therapy without any attention to the local irritants. Most important is the observation that the slowing, or stopping, or reversal seem more sharply defined when combined local and host therapy are instituted.
Primary Prevention
While secondary prevention (prevention of recurrence) is to be lauded, obviously primary prevention (prevention of occurrence) is to be desired. Clearly, primary prevention must begin very early in life before the teeth erupt and possibly even before they are formed. Attention, therefore, should be directed to what is known about prenatal influences in general, more especially in stomatology, and most particularly with regard to periodontal pathosis.
Prenatal Influences and Medical Problems: The literature is replete with reports showing the effect of prenatal life upon the future of man.5,6 Current medical opinion is captured in the following statements:5
“As recognized by an old Japanese custom that reckons a baby as a year old on the day of its birth, when the umbilical cord is severed much has already happened in the life of the individual. Maternal disease, trauma, radiation, drugs, metabolic disturbances, and even emotional reactions occurring during the pregnancy may so alter the fetus’ environment as to interfere with its normal growth and development. Thus, at birth, far from being a tabula rasa, a clean slate where nothing has yet been written, the infant brings into the world its prenatal experiences of which some may be grossly carved as congenital anomalies while others may take a subtler form, perhaps as ‘imprintings’ at the core of the first reaction patterns and personality characteristics.”
An examination of the literature shows that every cellular component, every tissue, and every organ is capable of being altered prenatally by any one of a number of physical, chemical, microbial and/or psychic challenges.
Prenatal Influences and Oral Problems: As one might expect, much less has been published regarding prenatal influences and oral disease versus general disorders. Additionally, of the paucity of stomatologic data, the overwhelming percentage deals with dental caries. The following quotation7 summarizes the present state of affairs:
“Rats, hamsters, and monkeys fed diets very high in sugar content do not develop caries appreciably if they were fed natural diets during the time their teeth were developing. If, however, they received the purified high sugar diet during this time, their teeth do develop caries when the high sugar diet is continued in later life.
“Studies of the teeth of European children during and after the war indicate that, at least in the countries of Northern Europe, the observed reduction in caries does not exactly parallel the period of reduced sugar consumption. Rather, the younger children, whose teeth developed during the period of low sugar intake, show a caries reduction in the postwar period, when sugar consumption is again high. Their caries experience is closer to that of ancient and medieval skulls which have been studied. The reduction is not due to fluorides included in the diet during the developmental period.
“Thus, all the evidence presented suggests that the structure of the teeth themselves is very important in determining the subsequent caries experience. As yet, no specific substance has been shown to be responsible for the formation of caries-resistant teeth.”
Figure 9 is one example of the effect of pre-eruption influences upon subsequent dental caries. This is a study of the percentage of seven-year-old German children with caries in the permanent dentition (shown by the interrupted line). Figure 9 shows that, during World War I (1914 to 1918), caries declined in these youngsters. Superimposed (Figure 9) is the sugar consumption in pounds per person per year (continuous line).It is noteworthy that, during the 1914-1918 period in Germany, sugar consumption declined. Moreover, the sugar intake decrement and caries decline are in parallel. This correlation fits nicely with the current concept of the local action of refined carbohydrate foods upon the tooth enamel. However, Figure 9 also shows that, with the end of World War I, sugar intake increased but dental decay continued to decline for about six or seven years. Only in 1924 did dental decay and sugar intake once again correlate. This observation suggests that children reared in a relatively low-sugar environment during the tooth development and prior to tooth eruption develop resistance to a subsequent cariogenic milieu. Clearly, these types of data suggest that the end-result (dental caries) is in part a function of host state irrespective of the local environment.
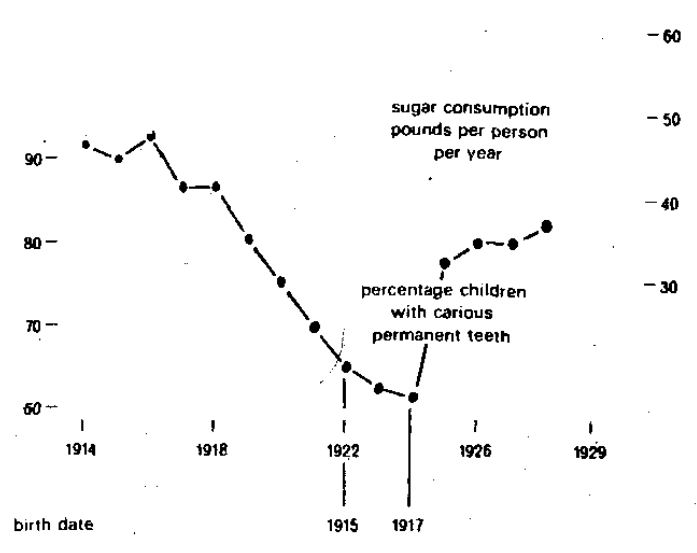
Figure 9
Unfortunately, there are no human studies in periodontology which can be likened to the observations just described in cariology. There are, however, isolated data from lower animal experimentation relevant to this discussion.
Baer and White8 studied calculus deposition and the Periodontal Index (PI) in the rat with a constant postweanling diet but different prenatal and preweanling diets. Figure 10 shows the calculus differences. It is evident that the amount of calculus deposition is clearly a function of early nutritional state. Figure 11 graphically portrays the periodontal state in terms of the same postweanling but different prenatal and preweanling diets. Once again, it is evident that periodontal health and disease is, in part, a function of early nutritional habits. In the words of the authors:8
“Thus, for the first time it has been shown that the severity of periodontal disease can be affected by prenatal and preweanling influences.”
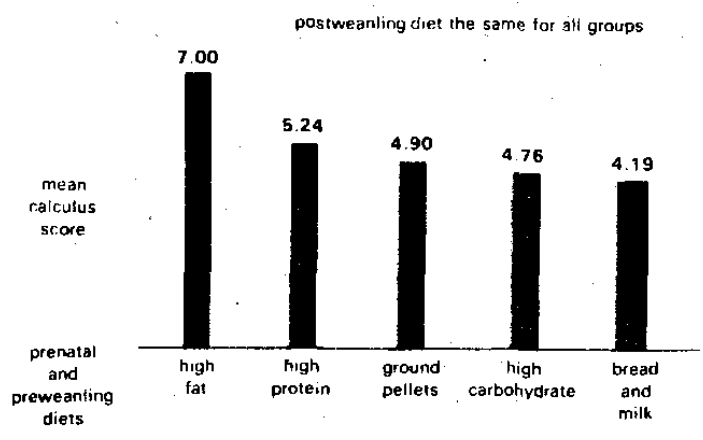
Figure 10
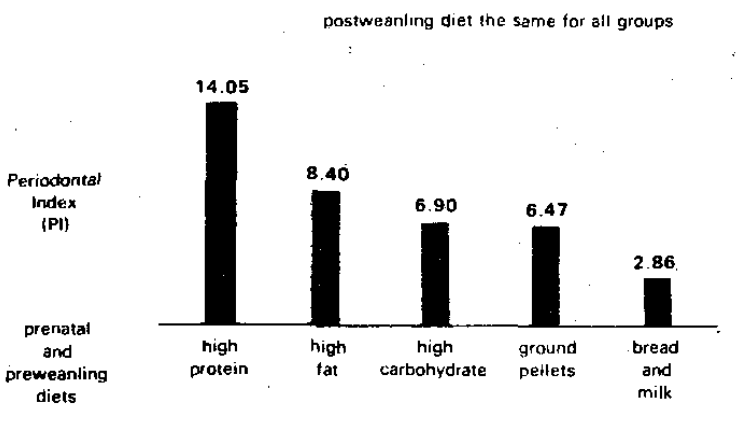
Figure 11
Summary
It is generally agreed that periodontal pathosis is a function of a constellation of local irritants modified by a pattern of extrinsic or host influences.
The literature is replete with evidence to show that the removal of local irritants, without regard to host state, is followed by improvement in periodontal state. However, the literature also clearly shows that the correlation between local irritants and periodontal pathosis is not perfect before or after local therapy.
There are some data to suggest that periodontal state can be altered by modifying the host with no attention directed to local factors. These reports have been analyzed in a recently published text.9 It must be granted that these data are more limited. Whether this is so due to the fact that host factors are less important than local irritants in the genesis of periodontal pathosis or whether the paucity of data is due to less investigation remains to be clarified.
There is little information to indicate that combined therapy (local and host treatment) nets greater results than local or host therapy singly.
In the final analysis, three avenues are available to the practitioner. For purposes of secondary prevention (prevention of recurrence), therapy can take the form of local and host treatment singly or in combination.
Primary prevention (prevention of occurrence) must originate early in life. There is abundant data to show that prenatal and early postnatal life can be so altered as to modify the remaining three score and ten with regard to general health.
There is more limited information to suggest that dental caries can be influenced in lower animals and in the human during the pre-eruption period. Even very isolated evidence suggests that prenatal and preweanling habits may affect the periodontium later in life. Obviously, the changes cannot be ascribed to changes in local irritants but rather because of alterations in host state.
More information regarding the possibility of primary prevention (prevention of occurrence) of periodontal pathosis could be obtained through a study of the relationships of the habits of the pregnant woman and the periodontal state of the offspring.
Precisely what course should be followed for the prevention of periodontal disease is a function of the philosophy of health and disease one accepts. One approach, not often enough considered in stomatology, is eloquently expressed in the following citation:10
“It is as though I had on a table three dolls, one of glass, another of celluloid, and a third of steel, and I chose to hit the three dolls with a hammer, using equal strength. The first doll would break, the. second would scar and the third would emit a pleasant musical sound.”
The suggestion is respectfully made that more consideration be given to the fabric of man (e.g., those of steel versus celluloid and glass) as it relates to his future periodontal course.
References Cited:
- Stahl, S. S. “The etiology of periodontal disease–review of the literature.” World Workshop in Periodontics. Ann Arbor, University of Michigan, 1966, p. 129.
- EI-Ashiry, G. M., Ringsdorf, W. M., Jr., and Cheraskin, E. “Local and systemic influences in periodontal disease: II. Effect of prophy/axis and natural versus synthetic vitamin C upon gingivitis.” Periodont. 35: 58 May-June, 1964.
- EI-Ashiry, G. M., Ringsdorf, W. M., Jr., and Cheraskin, E. “Local and systemic influences in periodontal disease: III. Effect of prophylaxis and natural versus synthetic vitamin C upon sulcus depth.” New York J. Dent. 34: 254 Aug.-Sept., 1964.
- EI-Ashiry, G. M., Ringsdorf, W. M., Jr., and Cheraskin, E. “Local and systemic influences in periodontal disease: lV. Effect of prophylaxis and natural versus synthetic vitamin C upon clinical tooth mobility.” J. Vit. Res.34:202,1964.
- Ferreira, A. J. Prenatal environment. Springfield, Charles C. Thomas, 1969, p. xiii.
- Montagu, M. F. A. Prenatal influences. Springfield, Charles C. Thomas, 1962.
- Sognnaes, A. P. “Is the susceptibility to dental caries influenced by factors operating during the period of tooth development?” California St. Dent. Assn. 26: 37 May-June, 1950.
- Baer, P. N. and White. C. L. “Studies on experimental calculus formation in the rat: XIV. Effect of prenatal and preweanling diets.” Periodont.-Periodontics 40: 641, Nov., 1969.
- Clark, J. W., Cheraskin, E. and Ringsdorf, W. M., Jr.: Diet and the periodontal patient. Springfield, Charles C. Thomas, 1970.
- May, J. M. “The ecology of human disease.” New York Acad. Sc. 84: 789, 1960.