
Access to all articles, new health classes, discounts in our store, and more!
Effect of EDTA Chelation Therapy Plus Multivitamin Trace Mineral Supplementation Upon Vascular Dynamics: Ankle Brachial Doppler Systolic Blood Pressure Ratio
Published in the Journal of Holistic Medicine, Vol. 7, No. 1, pp. 16-22, Spring/Summer 1985.
* * *
Abstract: A study of 117 lower extremities in 77 elderly patients with documented occlusive peripheral vascular stenosis, diagnosed by the Doppler systolic ankle/brachial blood pressure ratio, revealed that intravenous ethylene diamine tetraacetic acid (EDTA) chelation therapy with supportive multivitamin/trace mineral supplementation improved arterial blood flow significantly after approximately 60 days and 26 infusions (P < 0.001).
Bernstein and his contributors,1 in their monumental text, Noninvasive Diagnostic Techniques in Vascular Disease, make four cogent points. First, noninvasive diagnostic instrumentation and interpretation have now reached a state of excellence in routine clinical use. Second, some of the procedures are simple and practical enough for use in a general private practice environment. Third, of all available single noninvasive diagnostic techniques, the ankle/brachial Doppler systolic blood pressure ratio is preferred. Fourth and last, noninvasive diagnostic and predictive measurements can reliably monitor results of therapy, both surgical and nonsurgical.
This study evaluates measurements of ankle/brachial Doppler systolic blood pressure ratios in a general private practice, before and after a course of intravenous EDTA chelation therapy, in conjunction with multivitamin and trace mineral support.
Review of the Literature
There is general agreement that the presence of significant occlusive peripheral vascular disease may be ascertained in a large percentage of patients by means of a careful medical history and physical examination, although more precise information about the location and severity of the lesion(s) may be derived from angiography. Clinical assessment is highly subjective, while angiography is invasive and incurs significant risk to the patient. The noninvasive ankle/brachial Doppler systolic blood pressure ratio can be derived easily, objectively, and with reproducible accuracy and thus provides a reliable and sensitive index of the severity of the occlusive process.
Although additional information may be obtained from segmental Doppler systolic blood pressure readings at various levels along the legs (also from plethysmography and wave form analysis), the ankle/brachial index has more commonly been used since it reflects, better than any other single reading, the overall condition of proximal vessels.2,3,4
The ankle/brachial Doppler systolic blood pressure ratio has been well studied in diagnosis and as a monitor of both medical and surgical treatment. This is believed to be the first report of a study of the effect of EDTA chelation upon vascular dynamics, as measured by this particular noninvasive technique. (Parenthetic mention is made of a previous report5 which demonstrated improvement of cerebral blood flow following EDTA chelation therapy, utilizing measurements with oculocerebrovasculometry.)
Method of Investigation
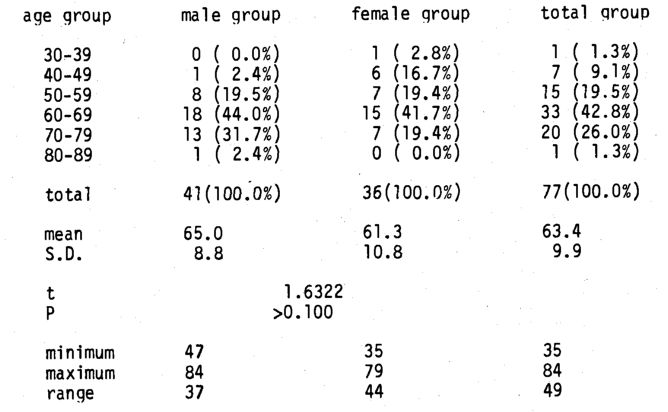
This experiment included 41 males and 36 females in whom 117 lower extremities (60 male; 57 female) were examined (Table 1). Ankle/brachial Doppler systolic blood pressure ratios were measured at the beginning and the end of the study utilizing a Parks Model 806-C Directional Doppler (Parks Electronic Laboratory, Beaverton, Oregon). Each course of treatment lasted an average of 60 days per patient. Treatment consisted of an average of 26.2 ± 8.1 infusions of 3 gm EDTA, along with supportive multivitamin/trace mineral supplementation. All subjects demonstrated an initial ankle/brachial ratio < 1.0. This cutoff point was used because it is generally accepted that the “normal” ankle/brachial ratio is 1.126 and that values lower than 0.97 should be considered abnormal.7,8,9 All patients treated during the period of the study who demonstrated initial ratios < 1.0 are included in this report.
Supportive multivitamin, mineral, trace-element supplementation was tailored to each patient’s needs, based on biochemical and clinical evaluation. Dosages for water soluble vitamins, C and B Complex, were on the order of ten times the Recommended Daily Allowance (RDA), while other vitamins, minerals, and trace elements were supplemented in approximately RDA amounts.
All measurements were performed at rest, in the supine position, because the evidence suggests that, under these conditions, Doppler systolic blood pressure measurements provide a sensitive index of arterial occlusion.10,11
Table 1–Age and Sex Distribution
Results
Line 1 of Table 2 summarizes ankle/brachial Doppler systolic blood pressure ratios at the start of the experiment. Because only those patients with a ratio < 1.0 were selected, it is evident (mean 0.77 ± 0.22) that all subjects suffered with arterial insufficiency (the range was from 0.00 to 0.99). Following EDTA chelation therapy, (line 2) the ratio increased (mean 0.94 ± 0.27, range from 0.43 to 1.59). Subsequent to an average of approximately 26 infusions of EDTA per patient, extending over approximately 60 days, the ankle/brachial index increased an average of 22%, indicating an improvement in arterial blood flow. This is highly significant statistically (t = 8.0041, P < 0.001). The significance of this result is supported by other studies which indicate that a change in the ankle/brachial index of 15% or more is significant, while a difference of 10-15% is of borderline significance.7 Of the 117 limbs studied, 95 (81%) improved, 22 (19%) worsened. Phrased another way, 95 limbs improved an average of 29% and 22 limbs worsened an average of 10%.
Considering the wide range of initial ratios, indicating that some patients were suffering with more and others less stenosis, the entire sample of 117 limbs was divided into two subgroups. One subset of 46 measured an average initial ratio of < 0.80. This is designated as the “poorer” group; the other 71 measured an initial ratio of 0.80 and is labelled the “better” group.
Table 2–Effect of EDTA Chelation Therapy with Vitamin/Mineral Supplementation Upon Ankle/Brachial Systolic Pressure
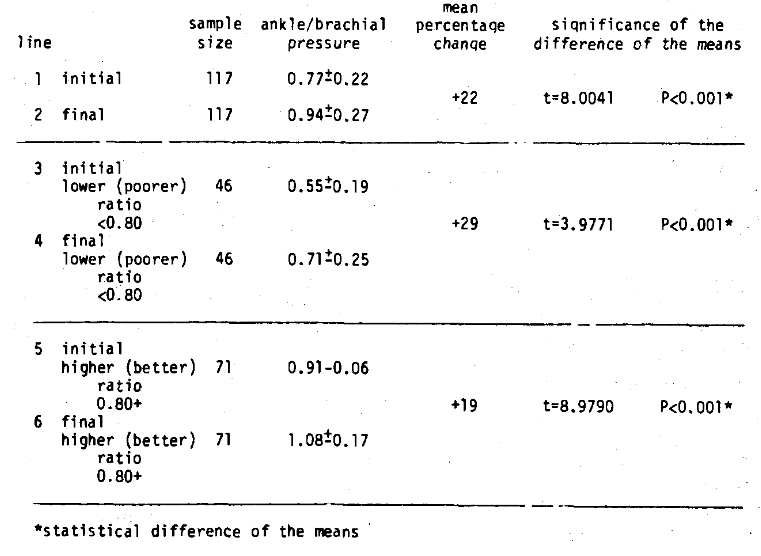
Line 3 of Table 2 summarizes the average initial scores of the poorer group (0.55 ± 0.19). Line 4 shows the final average values (0.71 ± 0.25) of that group. In those with more severe occlusion, the ankle/brachial index (reflecting arterial blood flow) improved an average of 29%, which is highly statistically significant (t = 3.997, P<0.001). To subdivide this group even further, 33 patients (71%) improved and 13 patients (29%) worsened. The 33 patients improved an average of 46% and the 13 less fortunate patients worsened by an average of 11%. Some patients had systolic ankle pressures below 50 mm Hg, the limit below which gangrene may be expected,12 and all such patients experienced clinical improvement.
In the relatively healthier group of 71 patients, the average initial index (line 5) was 0.91 ± 0.06. The final average value (line 6) was 1.08 ± 0.17. This was an average of 19% improvement, which is highly significant statistically (t = 8.9790, P<0.001). Actually, 62 of the 71 patients (87%) improved while 9 patients (3%) worsened. Put another way, 62 patients improved an average of 23% and 9 patients worsened 10%.
Discussion
A number of points deserve special mention. First, improvements in arterial blood flow to diseased legs summarized in this experiment are highly significant on statistical analysis (Table 2). This becomes even more important when it is considered that multiple serial determinations of Doppler systolic ankle blood pressure may differ from the mean of three or more readings by up to 11 mm Hg.7 Expressed as a ratio, this corresponds to only 0.09 for the ankle/brachial value. Hence, the improvement observed following treatment with intravenous EDTA is far greater than would be expected from purely technical error.
Second, while the principal therapeutic thrust for occlusive peripheral vascular disease has been surgical, there is isolated mention in the published literature to suggest that vascular insufficiency can be favorably altered by nonsurgical means such as clofibrate.13 This report is believed to be the first to report improvement from EDTA chelation plus supportive multivitamin/trace mineral supplementation.
Third, because of the leaching effect of EDTA chelation therapy, multivitamin, mineral, and trace element supplementation is important. It is also customary to administer nutritional supplements with anti-oxidant properties to enhance the benefit of EDTA in removal of metallic free radical catalysts. This then raises a question concerning the relative contributions of EDTA versus nutritional supplements. This experiment does not address itself to that question, although it would indeed be interesting, in another study, to measure the effect of a multivitamin/trace mineral supplementation versus placebo in the treatment of arterial insufficiency.
Fourth, it should be noted that those patients in the groups that worsened did so only by approximately 10%. A change of 10% is of questionable significance.
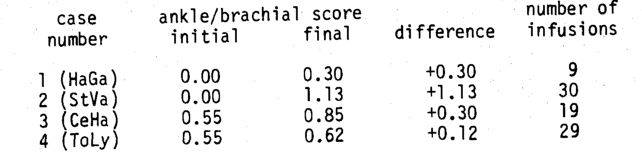
Finally, we note in this experiment that while there is evidence for a statistically significant improvement in average arterial blood flow, there are considerable differences in response between individual patients (Table 3). A comparison of Case #1 (HaGa) and Case #2 (StVa) shows an improvement of +0.30 in Case #1 following 9 infusions, while Case #2 improved by +1.13 following 30 infusions. These data would seem to indicate a linear relationship between the number of infusions and final benefit. Such, however, is not always the case. Case #3 (CeHa) experienced an improvement of only +0.30 following 19 infusions, in comparison to the same benefit from 9 infusions by Case #1, while Case #4 (ToLy) improved only slightly, +0.12, following 29 infusions.
Table 3–Individual Case Difference
In an earlier study we reported similar differences in biochemical changes between individual patients following EDTA chelation therapy. Individual differences in. patient response to EDTA were reported relative to serum cholesterol,14,15 high density lipoprotein cholesterol,16 total serum cholesterol/high density lipoprotein cholesterol ratio,17 serum creatinine,18 serum calcium,19 and blood urea nitrogen.20 Further study is planned to reexamine the biochemical and vascular data to ascertain whether those who fared best biochemically were the same individuals who showed the greatest improvement of blood flow in diseased arteries.
Although there is evidence to suggest that the ankle/brachial Doppler systolic blood pressure ratio is an excellent index of peripheral arterial status, it is not a perfect diagnostic test. This is so in part because of artifactually evaluated ankle blood pressures in patients with severely sclerotic and rigid arteries which do not compress under the cuff (especially in diabetes mellitus). A more complete peripheral arterial examination would also include measurements at the thigh, calf, ankle, foot, and toe, including plethysmography and wave form analysis.
References Cited:
- Bernstein EF: Noninvasive Diagnostic Techniques in Vascular Disease (2nd ed.), Saint Louis, CV Mosby, 1982.
- Bollinger A, Barras JP, Mahler F: “Measurement of foot artery blood pressure by micromanometry in normal subjects and in patients with arterial occlusive disease.” Circulation 1976; 53: 506-512.
- Nielsen PE, Barras, JP, Holstein P: “Systolic pressure amplification in the arteries of normal subjects.” Scand J Clin Lab Invest 1974; 33: 371-377.
- Stegall HF, Kardon MB, Kemmerer WT: “Indirect measurement of arterial blood pressure by Doppler ultrasonic sphygmomanometry.” J Appl Physiol 1968; 25: 793-798.
- McDonagh EW, Rudolph CJ, Cheraskin E: “An oculocerebrovasculometric analysis of the improvement in arterial stenosis following EDTA therapy.” J Holistic Med 1982; 4: 21-23.
- Thulesius O: “Systemic and ankle blood pressure in patients with arterial insufficiency.” Angiology 1978; 29: 374-378.
- Carter SA: “Indirect systolic pressures and pulse waves in arterial occlusive disease of the lower extremities.” Circulation 1968; 37: 624-630.
- Carter SA: “Clinical measurement of systolic pressures in limbs with arterial occlusive disease.” JAMA 1969; 207: 1869-1894.
- Yao ST, Hobbs JT, Irvine WT: “Ankle systolic pressure measurements in arterial disease affecting the lower extremities.” Brit J Surg 1969; 56: 676-679.
- Gaskell P: “The rate of blood flow in the foot and calf before and after reconstruction by arterial grafting of an occluded main artery to the lower limb.” Clin Sc 1956; 15: 259-269.
- Lewis JD, et al.: “Simultaneous blood flow and pressure measurements in intermittent claudication.” Brit J Surg 1972; 59: 418-422.
- Lassen NA, Tonnesen KH, Holstein P: “Distal blood pressure.” Scand J Clin Lab Invest 1976; 36: 705- 709.
- Postlethwaite JC, Dormandy JA: “Results of ankle systolic pressure measurements in patients with intermittent claudication being treated with clofibrate.” Ann Surg 1975; 181: 799-802.
- McDonagh EW, Rudolph CJ, Cheraskin E: “Serum cholesterol and the aging process.” Med Hypotheses 1981; 7: 685-694.
- McDonagh EW, Rudolph CJ, Cheraskin E: “The effect of intravenous disodium ethylenediaminetetraacetic acid (EDTA) upon blood cholesterol in a private practice environment.” J Int Acad Prevent Med 1982; 7: 5-12.
- McDonagh EW, Rudolph CJ, Cheraskin E: “The homeostatic effect of EDTA with supportive multivitamin-trace mineral supplementation upon high-density lipoproteins (HDL).” J Osteopath Physicians & Surg Calif 1982; 8: 34.
- McDonagh EW, Rudolph CJ, Cheraskin E: “The influence of EDTA salts plus multivitamin-trace mineral therapy upon total serum cholesterol/high-density lipoprotein cholesterol.” Med Hypotheses 1982; 9: 643-646.
- McDonagh EW, Rudolph CJ, Cheraskin E: “The effect of EDTA salts plus multivitamin-trace mineral supplementation upon renal function: A study in serum creatinine.” J Holistic Med 1982; 4: 146-151.
- McDonagh EW, Rudolph CJ, Cheraskin E: “The effect of intravenous disodium ethlenediaminetetraacetic acid (EDTA) plus supportive multivitamin-trace mineral supplementation upon fasting serum calcium.” Med Hypotheses 1983; 11: 431-438.
- McDonagh EW, Rudolph CJ, Cheraskin E: “The effect of EDTA chelation therapy plus supportive multivitamin-trace mineral supplementation upon renal function: A study in blood urea nitrogen (BUN).” J Holistic Med 1983; 5: 163-171.