
Access to all articles, new health classes, discounts in our store, and more!
Diet and Sulcus Depth
Published in The New York State Dental Journal, Vol. 30, No. 1, pp. 3-8, January 1964.
* * *
Introduction
It is generally held that physiologic sulcus depth is one to two millimeters.1-4
This study is designed for a twofold purpose: (1) to consider the epidemiology of gingival sulcus depth in a group of presumably healthy young men, and (2) to examine the effect of three dietary programs upon gingival sulcus depth.
Review of the literature
Recent clinical investigations indicate that a relatively low-refined-carbohydrate high-protein diet5-7 and a protein-supplemented diet8 exert a favorable influence on the human periodontium. Clinical improvement was evidenced by a reduction in sulcus depth,5 gingivitis,6,8 and clinical tooth mobility.7 Recently, it has been suggested that greater reduction in tooth mobility may be obtained by combining systemic nutritional therapy with local treatment measures.9
In lower animal experimentation a dramatic and significant reduction of soft tissue lesions of periodontal tissue occurred in rats on a carbohydrate-free diet.10,11 Also, significantly less alveolar bone loss has been noted in mice subsisting on a low-carbohydrate high-protein diet.12 The control groups in both experiments were given nutritionally complete diets containing carbohydrates. On the other hand, protein deprivation in dogs has been shown to quickly precipitate the destruction of periodontal tissues13 and, in association with a high-sucrose intake, to produce significantly smaller teeth in rats.14 Rats on a protein-free diet exhibited delayed gingival wound healing and a breakdown of partially healed wounds.15
Method of investigation
The depth of the gingival sulcus (to the nearest millimeter) was determined on the labial, lingual, mesial, and distal surfaces of the four mandibular incisor teeth in 128 junior dental students. Actually, four measurements were made on each of the four teeth in all but fifteen subjects. Missing and malposed teeth account for the 29 readings that could not be obtained. Hence, 2019 of a possible 2048 values (128 x 16 = 2048) constitute the data for this report. In general, the oral hygiene was rated as fair, and all readings were possible without having to remove calculus.
The gingival sulcus depth was measured at the midline of the respective tooth on the labial and lingual. The mesial and distal measurements were made from the labial of each tooth. A University of Alabama periodontal probe (Star Dental Manufacturing Company) was used to record the sulcus depth to the nearest millimeter. The instrument has two thin, flat calibrated spatula blades (one hoe and one hatchet arrangement) which have rounded edges to prevent cutting the epithelial attachment. The accuracy of the measuring technique was determined by making a series of 50 measurements and then repeating the series. The reproducibility is evidenced by a very significant (P < 0.001) coefficient of correlation (r = + 0.989).
The students were randomly classed into three major groups (Table 1).
Table 1
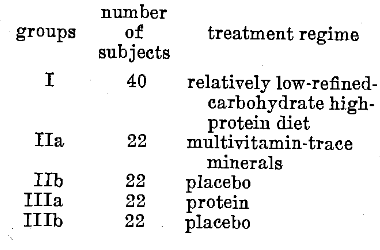
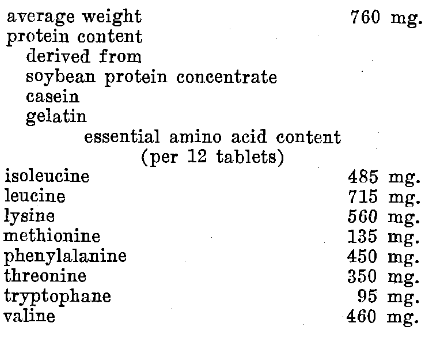
Group I, consisting of forty students, was instructed to take a relatively low-refined-carbohydrate (no sugar or white flour products) high-protein diet (increased consumption of meat, fish, fowl, eggs, nuts, and cheese) for three days. Group II (forty-four students) was randomly divided into two subcategories. Group IIa received a multivitamin-trace mineral preparation for three days (Table 2); Group Ilb was given an indistinguishable placebo for the same time period. Group III (forty-four subjects) was also randomly subdivided. Group IIIa was given forty grams daily of a protein supplement (Table 3) for three days; Group Illb was administered an indistinguishable placebo.
Three days later sulcus depth was remeasured by the same examiner with no knowledge of the initial findings nor the nature of the dietary recommendations.
Table 2–Each Capsule Contains
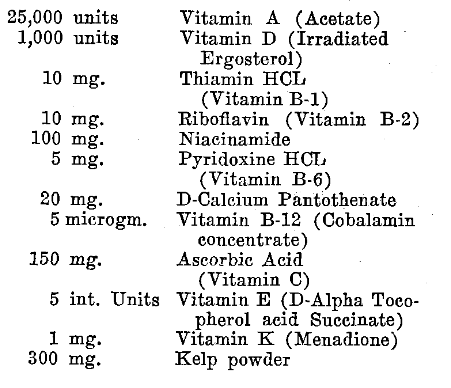
Table 3–Composition of Protein Tablets
Results
Table 4 summarizes the frequency distribution of sulcus depth at the first visit for the entire group of 128 students. Several points deserve special mention. Firstly, in not one instance, was a sulcus of zero depth observed. Secondly, the overwhelming percentage of sulci (67.5 percent) were two millimeters. Thirdly, if one to two millimeters is to be regarded as physiologic for mandibular incisors in the 20-30 year age group, then 22.5 percent of the sulci may be considered pathologic since they are three, four, and even five millimeters deep.
Table 4–Frequency Distribution of Sulcus Depth
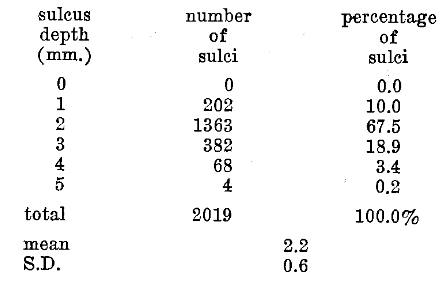
Table 5 outlines the initial and final values for sulcus depth in connection with the relatively low-refined-carbohydrate high-protein diet (Group I). Five points warrant special attention. Firstly, the greatest number of sulci (66.9 percent) is two millimeters. This fraction is consistent with the observations for the entire group (Table 4). Secondly, 22 percent of the group at the initial examination demonstrated sulci greater than two millimeters. This figure also compares favorably with the earlier reported observations (Table 4). Thirdly, following the diet, the number of one millimeter sulci rose almost two and one-half fold (from 11.1 to 26.1 percent). Fourthly, the number of two millimeter sulci remained essentially the same (66.9 to 62.1 percent). Lastly, the frequency of greater than two millimeter sulci decreased almost one half (from 22.0 to 11.8 percent).
Table 5–Effect of Relatively Low-Refined-Carbohydrate High-Protein Diet Upon Sulcus Depth (Group I)
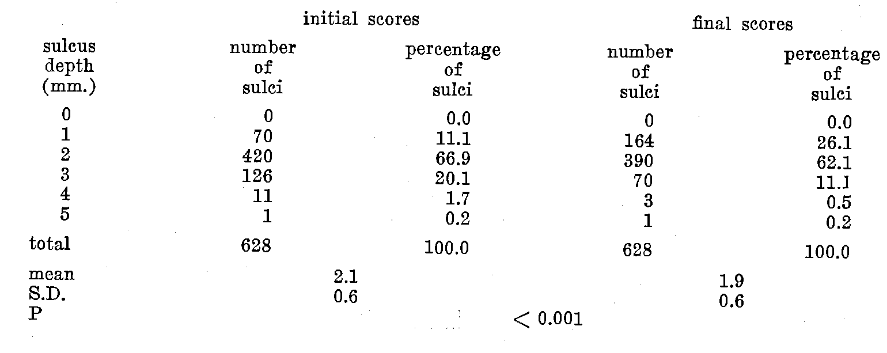
Table 6 summarizes the initial and final scores for sulcus depth for the groups supplied a three-day multivitamin-trace mineral versus placebo supplement. Five items deserve special consideration. Firstly, the greatest number of sulci (65.0 and 66.9 percent) were of the two millimeter depth. This finding is consistent with those earlier reported for the entire sample (Table 4) and Group I (Table 5). Secondly, 24.1 and 17.0 percent of the group at the start had sulci greater than two millimeters. These figures compare favorably with those previously reported (Tables 4 and 5). Thirdly, after multivitamin-trace mineral supplementation, the number of one millimeter sulci doubled (10.9 to 20.9 percent) while there was no appreciable change in the placebo-treated group (16.1 to 14.7 percent). Thirdly, in both Groups IIa and IIb the number of two millimeter sulci remained essentially the same. In Group IIa the initial and final values are 65.0 and 63.2 percent; in Group IIb 66.9 versus 67. 8 percent. Lastly, sulci greater than two millimeters decreased from 24.1 to 15.9 percent after multivitamin-trace mineral therapy; in the placebo group the values are 17.0 and 17.5 percent.
Table 6–Effect of Multivitamin-Trace Mineral Versus Placebo Supplementation Upon Sulcus Depth (Group II)
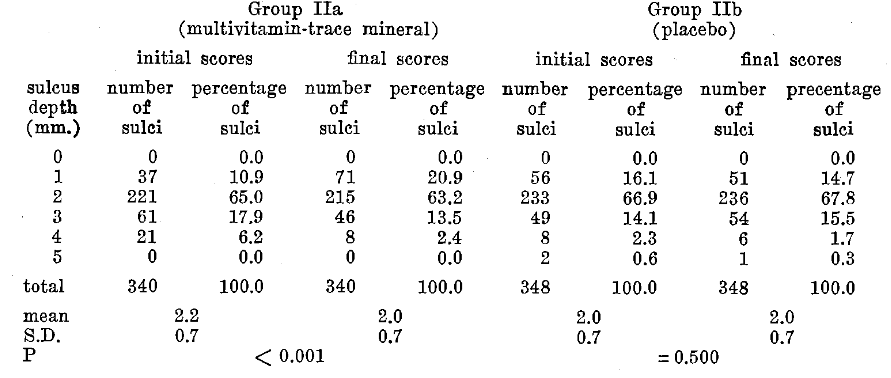
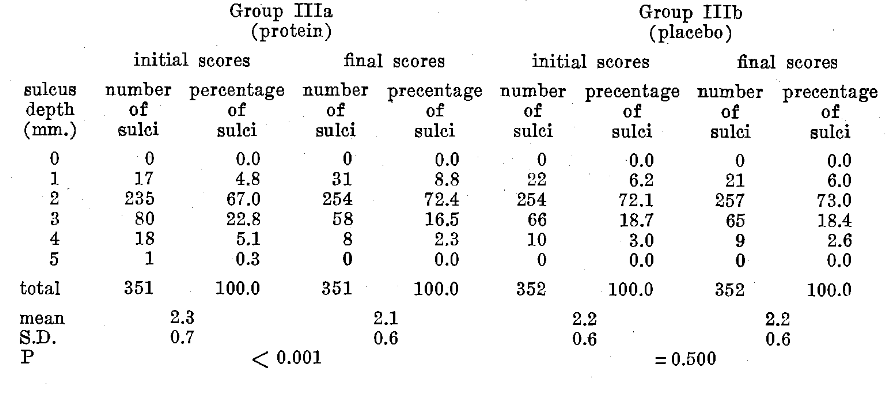
Table 7 describes the initial and final scores for sulcus depth with protein versus placebo supplementation for three days. Five points are noteworthy. Firstly, the greatest number of sulci initially were of two millimeters in depth in both the protein and placebo groups. These figures are surprisingly similar to those described in connection with Group I (Table 5), Groups IIa and IIb (Table 6), and the entire sample (Table 4). Secondly, 28.2 percent (Group IIIa) and 21.7 percent (Group IIIb) had sulci greater than two millimeters at the start of the study. These values closely parallel the observations in the other groups. Thirdly, after protein, the number of one millimeter sulci almost doubled (from 4.8 to 8.8 percent); the scores remained the same (6.2 to 6.0 percent) in the placebo-treated category. Fourthly, in both groups the number of two millimeter sulci remained essentially the same (in Group IIIa 67.0 to 72.4 percent; in Group IlIb 72.1 to 73.0 percent). Lastly, sulci greater than two millimeters decreased from 28.2 to 18.8 percent with protein; with the placebo the scores were 21.7 to 21.0 percent.
Table 7–Effect of Protein Versus Placebo Supplementation Upon Sulcus Depth (Group III)
Discussion
Firstly, in the light of conventional standards, it seems fair to conclude that pathologic sulcus depth is fairly common in a group of presumably healthy young men.
The unsupervised recommendation of a diet (Group I) seems to have yielded a significant reduction in sulcus depth from 2.1 ± 0.6 millimeters to 1.9 ± 0.6 millimeters (P < 0.001). However, it is difficult to draw many other conclusions since no control group was included, and two variables, refined carbohydrates and protein, had been altered. For this reason, it is well to turn attention to Groups II and III where controls are included, one variable is operative, and the factors are those which are part of the diet recommended to Group I.
The evidence from Table 6 suggests that a significant reduction in mean sulcus depth occurred with multivitamin-trace mineral supplementation (P < 0.001); no such change occurred with the placebo (P = 0.500). Aside from the very obvious point that there is a significant difference in the groups, there is another point which should be mentioned. It is now generally recognized that the ingestion of refined carbohydrates carries with it the possibility of developing a multivitamin deficiency. Hence, the observations in Group II suggest that the findings in Group I may be more significant than earlier pointed out.
It should be recalled that one of the recommendations to the participants in Group I was to increase protein intake in an unsupervised fashion. Group III provides the opportunity to study the effect of protein under more carefully controlled conditions. It is clear (Table 7) that a significant decrease in sulcus depth occurred with protein (P < 0.001) while no change followed the placebo (P = 0.500).
There is one other question which it would be nice to answer if at all possible. It would be helpful to try to determine the relative efficacy of the various therapeutic regimens employed in this project. A study of the data indicates that sulci greater than two millimeters decreased by 10.2 percent in Group I, 9.4 percent in Group IIIa, 8.2 percent in Group IIa; 0.7 percent in Group IIIb, and increased by 0.5 percent in Group IIb. Thus, within the limits of this study, it appears that the greatest sulcus depth reduction occurred with the elimination of refined carbohydrates and addition of protein. The second greatest reduction was associated with a protein supplement, and the least decrease in sulcus depth seemed to accompany the introduction of a multivitamin-trace mineral preparation.
The decrease in sulcus depth in each instance was mediated chiefly through a reduction in marginal inflammation and edema. These were most probably in response to systemic alterations since the dietary consistency was not altered.
It must be admitted that the method utilized in this report to measure sulcus depth leaves much to be desired. Nonetheless, the findings are highly interesting in view of the fact that the two placebo groups demonstrated only minimal changes.
Summary
Within the limits of this study and, on the assumption that sulcus depth greater than two millimeters is pathologic, one may conclude that approximately 22 percent of the sulci of a group of presumably healthy students are pathologic.
The evidence suggests that, in decreasing order, the introduction of a relatively low-refined-carbohydrate high-protein diet, a protein supplement, and a multivitamin-trace mineral preparation exerted a beneficial effect (reduction in sulcus depth). In contrast, no significant changes were noted with placebo treatment.
It is well to underscore the fact that the subjects for this study were presumably healthy students. It is also noteworthy that the changes reported here occurred from Monday to Friday of the same week.
References Cited:
- Glickman, I.: Clinical periodontology. Philadelphia, W. B. Saunders Company, p. 12, 1958.
- Goldman, H. M.: Periodontia. St. Louis, The C. V. Mosby Company, p. 66, 1953.
- Orban, B.: Periodontics. St. Louis, The C. V. Mosby Company, p. 19, 1958.
- Sorrin, S.: The practice of periodontia. New York, The Blakiston Division, McGraw-Hill Book Company, p. 21, 1960.
- Ringsdorf, W. M., Jr. and Cheraskin, E: “Periodontal pathosis in man: I. Effect of relatively high-protein low-refined-carbohydrate diet upon sulcus depth.” J. Periodont. 33: 341-343. 1962.
- Ringsdorf, W. M., Jr. and Cheraksin, E.: “Periodontal pathosis in man: II. Effect of relatively high-protein low-refined-carbohydrate diet upon gingivitis.” N. Y. State D. J. 28: 244-247, 1962.
- Cheraskin, E. and Ringsdorf, W. M., Jr.: “Periodontal pathosis in man: III. Effect of relatively high-protein low-refined-carbohydrate diet upon clinical tooth mobility.” Ann. Dent. 22: 13- 18, 1963.
- Ringsdorf, W. M., Jr and Cheraskin, E.: “Periodontal pathosis in man: IV. Effect of protein versus placebo supplementation upon gingivitis.” J. Dent. Med. 18: 92-94, 1963.
- Clark, J. W.: “Systemic factors in abnormal tooth mobility.” J. Dent. Med. 17: 16-20, 1962.
- Auskaps, A. M., Gutpa, O. P., and Shaw, J. H.: “Periodontal disease in the rice rat. III. Survey of dietary influences.” J. Nutrit. 63: 325- 343, 1957.
- Baer, P. N. and White, C. L.: “Studies on periodontal diseases in the mouse. IV. The effects of a high protein low carbohydrate diet.” J. Periodont. 32: 328-330. 1961.
- Shaw, J. H. and Griffiths, D.: “Relation of protein, carbohydrate and fat intake to the periodontal syndrome.” J. Dent. Res. 40: 614-621, 1961.
- Ruben, M. P., McCoy, J., Person, P., and Cohen, D. W.: “Effects of soft dietary consistency and protein deprivation on the periodontium of the dog.” Oral Surg., Oral Med., and Oral Path. 15: 1061-1070, 1962.
- Holloway, P. J., Shaw, J. H., and Sweeney, E. A.: “Effects of various sucrose: casein ratios in purified diets in the teeth and supporting structures of rats.” Arch. Oral Biol. 3: 185-200, 1961.
- Stahl, S. S.: “Effect of a protein-free diet on the healing of gingival wounds in rats.” Arch. Oral Biol. 7: 551-556, 1962.