
Access to all articles, new health classes, discounts in our store, and more!
Diagnostic Cutaneous Reactions to Intradermal Injection of Natural and Artificial Antibody and of Antigen Prepared from Streptococci Isolated in Studies of Diverse Diseases
Presented at the meeting of the American College of Allergists, Atlantic City, New Jersey, June 7, 1947. Published in the Annals of Allergy, Vol. 6, No. 5, September-October 1948, pp. 485-496.
* * *
The consistent isolation by special methods of specific types of green-producing or alpha streptococci from infection atria and from tissues involved in various epidemic and nonepidemic diseases has been reported.5,7 The inherent or acquired property of streptococci to localize and produce lesions in tissue of animals, corresponding to those chiefly involved in the spontaneously occurring disease in question, was often so pronounced as to resemble the specific pharmacological action of certain drugs or chemicals.3,4 This tendency of streptococci to localize electively was shown to be due to the production, within the organisms themselves and free in broth cultures, of highly labile toxins or poisons which had predilection for, and specific damaging action on, the very tissues in which localization and growth occurred in the spontaneous and experimentally reproduced diseases. Similar original and corroborative studies on specificity of alpha streptococci have been reported by others; to which reference has been made in prior publications.
Evidence of specificity of streptococci as isolated in studies of various diseases was not limited to elective localization. The distribution curves of cataphoretic velocity of the streptococci varied according to the embryologic origin of the tissues chiefly involved and for which the streptococci had respective elective affinity.6 Moreover, the different types were agglutinated, and extracts were precipitated specifically by the respective antiserums.5,7
Each of these procedures used for demonstrating specificity of streptococci —elective localization, agglutination and precipitation reactions, and cataphoretic mobility— are cumbersome, time consuming, and difficult. Special methods for their isolation and for preservation of specificity have been found necessary, and even these do not always suffice. A search, therefore, was made for simpler methods for the detection of the presence of specific types of streptococcal infections and antibody response in persons suffering from different diseases.
In agreement with the erythematous antibody-antigen reaction discovered by Foshay1 in tularemia and with the antigen-antibody reaction described by Francis2 in pneumonia, it was found that an immediate erythematous reaction on intradermal injection of streptococcal antibody served for the detection of specific antigen, and that a similar reaction to intradermal injection of antigen served for the detection of specific antibody in skin or blood in persons suffering from the respective type of streptococcal infection. It is the purpose of this paper to describe the methods used and report the results obtained in cutaneous tests made with natural and artificial streptococcal antibody and with antigen, and the effects of therapeutic injection of artificial antibody in persons suffering from diverse diseases associated with, or due to, green-producing or alpha streptococci.
Methods Of Study
The streptococci from which natural and artificial antibody and antigen were prepared were isolated chiefly from nasopharyngeal swabbings of persons ill with diverse diseases and, as a control, from well persons remote from epidemics. For the isolation of specific types, serial dilution cultures of the NaCI-solution washings of the swabbings were made at steps of 10-2 or 10-4 in tall tubes of freshly prepared dextrose brain broth. Pure cultures of the streptococci were obtained from the end point of growth, and these were grown for only one, two, or three culture generations in this medium and then inoculated into large volumes (3,500 ml.) of freshly prepared, warm, 0.2 per cent dextrose broth. All cultures were incubated at 33° to 35° for only fourteen to twenty hours, and the growth in the large volumes of dextrose broth was harvested in the bowl of a continuous feed centrifuge. The putty-like growth was removed from the bowl with a sterile spatula and suspended in glycerol, 2 parts, and saturated NaCl-solution, 1 part, so that each ml. of this suspension contained the growth from 500 ml. of broth, or approximately 1,000 billion streptococci. The streptococci in this suspension, owing to the hygroscopic properties of the glycerol, become dehydrated. Some remained viable for a year or two and remained antigenically specific almost indefinitely. The use of the highly favorable medium, dextrose brain broth, which affords a reduced oxygen tension, the short period of growth of the organisms, and the dense suspension were found essential for the primary isolation of specific types of alpha streptococci and for maintaining their specific properties.
Appropriate dilutions of the dense suspension of the streptococci, and not the streptococci grown indefinitely on artificial mediums, were used for the immunization of horses, for the preparation of artificial antibody and of antigen as used in cutaneous tests and in treatment, for the preparation of vaccines and solutions of specific polysaccharides and extracts for precipitation tests, and for suspensions suitable for agglutination tests.
Ten per cent solutions of the euglobulin fraction of the serum of horses that had been immunized with the respective streptococci, and the bacteria-free supernatant of NaCI-solution suspensions containing 20 billion streptococci per ml., that had been autoclaved at 17 pounds pressure for ninety six hours, diluted with equal parts of NaCl-solution containing 0.4 per cent phenol, were used in cutaneous tests for the detection of specific antigen.8 The supernatant of suspensions containing 10 billion streptococci per ml., which had been heated at 70° C. for one hour, were used for the detection of specific antibody in skin or blood.
The Luer type of syringe of 0.5 ml. capacity, fitted with a 27-gauge needle, was used. Solutions of antibody and antigen considered homologous to the disease at hand in the persons to be tested, together with heterologous and control solutions, were drawn into syringes before beginning the injections. The skin was disinfected lightly with pledgets of absorbent cotton or gauze moistened with 95 per cent alcohol. Approximately 0.03 ml. of the test and control materials were injected in rapid succession, 5 cm. apart in two rows, into the skin of the volar aspect of the forearm, beginning at the bend of the elbow and proceeding towards the wrist.
The maximal area of the rapidly occurring erythema was outlined with pen and washable ink and recorded in square centimeters by superimposing circles of predetermined size on a 4 by 6 inch transparent discarded x-ray film. The solutions of antibody and antigen were kept in small rubber-capped vials, and the syringes containing the test materials were kept upright in test tubes containing enough 95 per cent alcohol to bathe the needle. They were kept in the refrigerator when not in use. The material in the syringes was not wasted after storage, but a few drops were discarded just before use to wash out any alcohol that might have diffused into the lumen of the needle. Solutions of natural and artificial antibody, when kept in the refrigerator, have been found to remain potent for as long as five and three years, respectively.
The reactions varied greatly in intensity and size, and at times were blotchy and irregular in outline. Their significance was always considered in relation to reactions or lack of reactions following injection of suitable control antibody or antigen and usually of NaCI-solution containing 0.2 per cent phenol. The erythema following injection of specific antigen occurred less often than that following injection of antibody, and was usually less intense and more transient than the reaction that followed injection of antibody. The reactions began to fade promptly. Slight edema and erythema were sometimes noted twenty-four hours later at the site of injection of the antigen. The size of reactions were usually checked by two or three observers, and large and small groups of well persons and persons suffering from different diseases were tested as unknowns. Reactions to several injections of the same test material ran closely parallel. In no instances did persons become sensitized or allergic following repeated intradermal or therapeutic injection of artificial antibody.
Artificial antibody used therapeutically was prepared by autoclaving NaCI-solution suspensions containing 10 billion streptococci per ml., by diluting the respective dense suspensions in glycerol-NaCl-solution 100 fold and autoclaving for three hours after adding 1.5 per cent H2O2.9 The slightly opalescent solution, containing the sharply agglutinated remnants of the organisms thus obtained, was brought to pH 6.8, diluted 1 to 5 with NaCI-solution, and from 2 to 10 ml. of such dilution were injected subcutaneously or intramuscularly in treatment.
Results Following Intradermal Injection of Antibody
The results following intradermal injection of natural and artificial antibody in persons suffering from influenza and other respiratory infections, influenzal pneumonia, “virus” or atypical pneumonia, epidemic and postoperative persistent hiccup, neuromyositis, and chronic infectious or rheumatoid arthritis, are summarized in Table I. The reactions were highly specific to both natural and artificial antibody.
Table I. Erythematous Reactions, in Persons Suffering from Influenza and Other Respiratory Infections, Persistent Hiccup and Arthritis, to Intradermal Injection of Natural and Artificial Antibody Prepared from Streptococci Isolated in Studies of the Respective Diseases
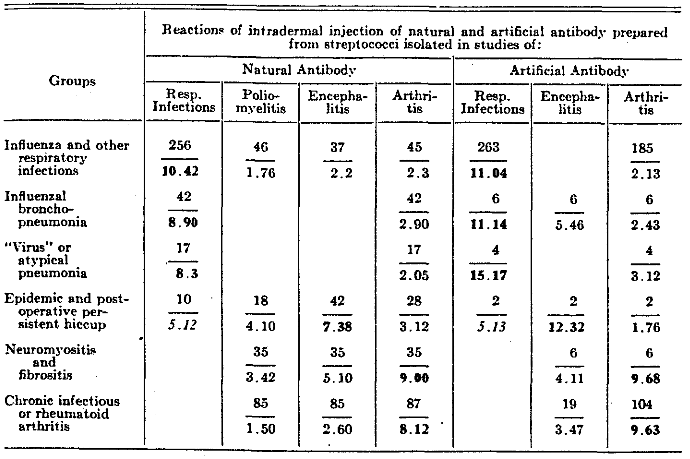
The figures above the line in each instance indicate the number of persons tested; the figures below the line indicate the average reactions in square centimeters.
The results obtained in cutaneous tests made during two institutional epidemics among persons having mild symptoms of schizophrenia, one of respiratory infection and one of enteritis, are summarized graphically in Figure 1. The reactions to the respective artificial antibodies were remarkably specific, roughly proportional to the severity of the diseases in question, and became greatly less as recovery occurred. Pronounced reactions occurred to the two respective homologous antibodies, one prepared from streptococci isolated in studies of respiratory infection and one from streptococci isolated in studies of epidemic enteritis in persons who suffered from both respiratory infection and enteritis.
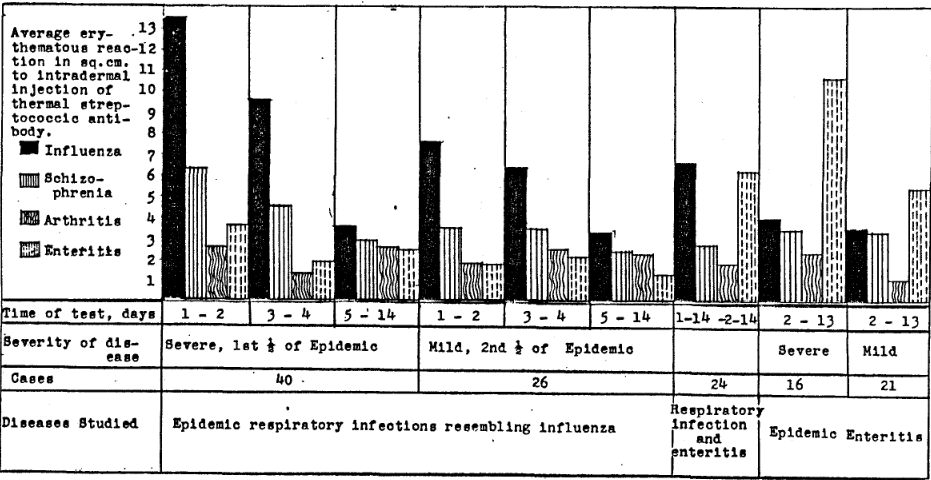
Fig. 1. Erythematous reactions to intradermal injection of thermal antibody produced from alpha streptococci isolated, respectively, in studies of epidemic respiratory infections, schizophrenia, arthritis, and epidemic enteritis.
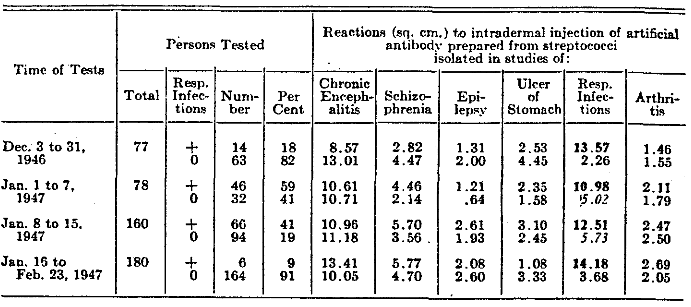
The results obtained at a penitentiary in prisoners during a sharp epidemic of respiratory infection are summarized in Table II. Each of four groups of persons, who were having respiratory infection when tested, reacted strongly to artificial antibody prepared from streptococci isolated in previous studies of respiratory infection, averaging 13.57, 10.98, 12.51, and 14.18 sq. cm. respectively. Two of four comparable groups that were free from symptoms of respiratory infection reacted significantly greater to the respiratory streptococcal antibody at the height of the epidemic (5.02 and 5.73 sq. cm.) than did two otherwise comparable groups before and after the height of the epidemic (2.26 and 3.68 sq. cm.). This increase during the height of the epidemic, indicating the carrier state, was apparently not due to contact infection.
Table II. Erythematous Reactions, in Prisoners at A Penitentiary During an Epidemic of Respiratory Infection, to Intradermal Injection of Artificial Antibody Prepared from Streptococci Isolated in Studies of Respiratory and Other Infections
The abnormally marked average reactions of this and a much larger number of prisoners to artificial antibody prepared from “neurotropic” streptococci isolated in studies of chronic encephalitis, schizophrenia, and from incorrigible prisoners, will be reported elsewhere. Suffice it to state here that intercurrent epidemic respiratory infections did not change the cutaneous reactivity to intradermal injection of two specimens of artificial antibody prepared from “neurotropic” streptococci.
The cutaneous reaction obtained following intradermal injection of natural and artificial antibody in persons suffering from epidemic poliomyelitis and encephalitis, from multiple sclerosis or ulcer of the stomach, and in well contacts and noncontacts in epidemic zones of poliomyelitis and in well persons remote from epidemics, are summarized in Table III. The average reactions to both natural and artificial antibody were uniformly much greater in persons suffering from the disease in studies of which the streptococcus was isolated and from which the reacting antibody was prepared. Moreover, the reactions in well persons to antibody prepared from streptococci isolated in studies of poliomyelitis were proportional to the degree of exposure to poliomyelitis in epidemic zones and were minimal or absent in well persons remote from poliomyelitis.
Table III. Erythematous Reactions, in Persons Suffering from Poliomyelitis, Encephalitis, Multiple Sclerosis or from Ulcer of the Stomach, to Intradermal Injection of Natural and Artificial Antibody Prepared from Streptococci Isolated in Studies of the Respective Diseases
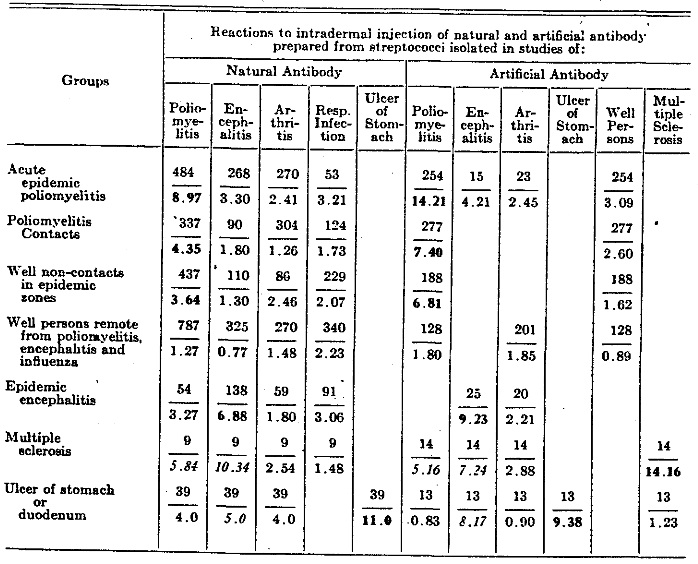
The figures above the line in each instance indicate the number of persons tested; the figures below the line indicate the average reaction in square centimeters.
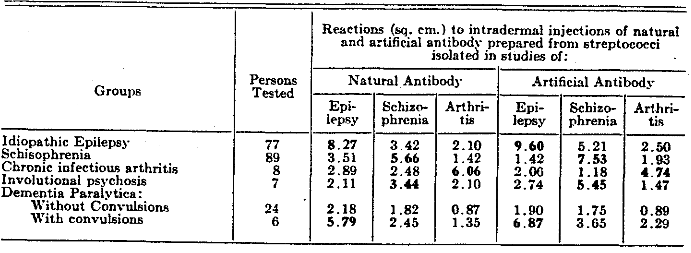
The average cutaneous reactions obtained in persons suffering from idiopathic epilepsy, schizophrenia, chronic infectious arthritis, involutional psychosis, and dementia paralytica, tested in parallel with natural and artificial antibody, are summarized in Table IV. A consistently high degree of specificity was obtained with both types of antibody, including a strikingly greater average reaction to antibody prepared from streptococci isolated in studies of epilepsy in persons suffering from dementia paralytica having convulsions, than occurred in persons having dementia paralytica without convulsions. The reactions were uniformly minimal to all antibodies in the uncomplicated group of dementia paralytica, and to heterologous antibody in the groups which reacted specifically to the homologous antibody. Moreover, cross reactions were relatively greater in persons suffering from epilepsy or schizophrenia to both types of antibody prepared, respectively, from the more closely related streptococci isolated in studies of epilepsy and schizophrenia, than to antibody prepared from the streptococci isolated in studies of arthritis.
Table IV. Erythematous Reactions, in Persons Suffering from Diseases of the Nervous System or from Arthritis, to Intradermal Injection of Natural and Artificial Antibody Prepared from Streptococci Isolated in Studies of the Respective or Related Diseases
Results Following Therapeutic Injection of Artificial Antibody
The presence of abundant specific antigen and minimal specific antibody in skin or blood of persons in the early stages of respiratory infections, the gradual diminution of antigen, and the increase of antibody with time during the natural course of the disease and as recovery ensued, are shown graphically in Figure 2.
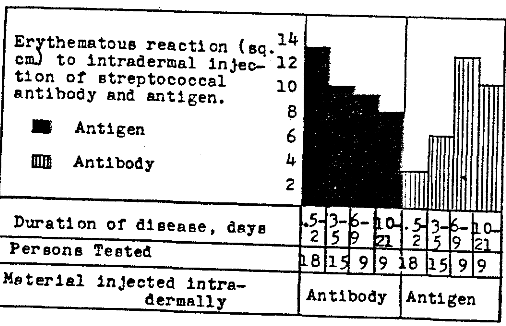
Fig. 2. Erythematous reactions, in persons suffering from epidemic respiratory infections, to intradermal injection of antibody and antigen prepared in vitro from streptococci isolated in studies of respiratory infections, according to the duration of the disease.
The effects of therapeutic injection of artificial antibody on the antigen, and antibody content of skin or blood in persons suffering from influenza or other respiratory infections are shown graphically in Figure 3. The decrease in specific antigen, as shown by intradermal injection of artificial antibody prepared from streptococci isolated in studies of influenza and other respiratory infections, and the increase in antibody, as shown on intradermal injection of the corresponding antigen following therapeutic injection of specific artificial antibody, were greater in twelve and six hours, respectively, than occurred in six to nine or more days during the natural course of the disease (Fig. 2). There was usually a corresponding improvement in symptoms, especially in the early stages of the disease as antigen was sharply reduced and antibody abruptly increased.
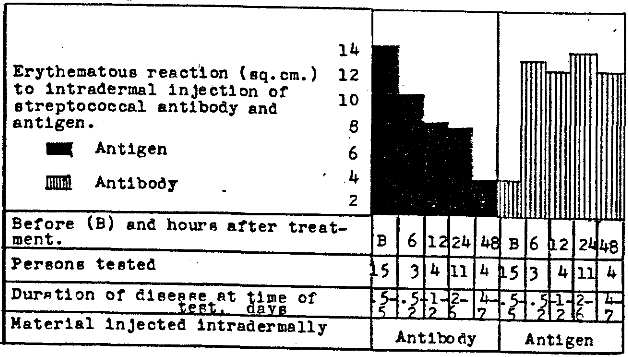
Fig. 3. Erythematous reactions, in persons suffering from influenza or other respiratory infections, to intradermal injection of antibody and antigen prepared in vitro from streptococci isolated in studies of epidemic respiratory infections, before and after therapeutic injection of homologous streptococcal antibody.
The effects of therapeutic injection of artificial antibody prepared from streptococci isolated in studies of poliomyelitis on the content of specific antigen and antibody in the skin or blood of persons suffering from epidemic poliomyelitis, are summarized graphically in Figure 4. A striking reduction in antigen and an increase in antibody occurred in three hours and persisted for forty-eight hours following one therapeutic injection per person of antibody in the group of sixteen persons in the early stages of the disease. A moderate decrease in antigen and increase in antibody occurred in the group of twelve persons in the later stages of the disease, and no change in antigen and antibody occurred in the four control persons having poliomyelitis who received “therapeutic” injections of NaCl-solution.
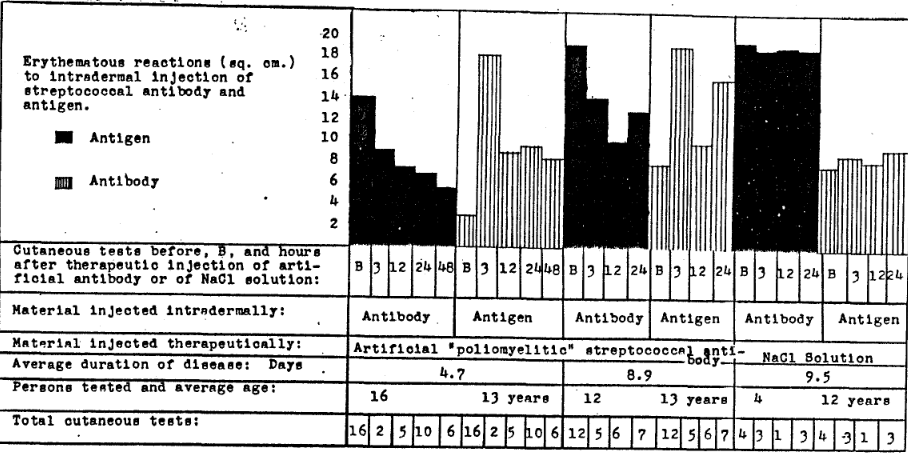
Fig. 4. Erythematous reactions, in persons suffering from epidemic poliomyelitis, to intradermal injection of antibody and antigen prepared from streptococci isolated in studies of poliomyelitis, according to the duration of the disease and therapeutic intramuscular injection of artificial antibody.
Comments and Summary
The results of cutaneous tests in persons suffering from widely different epidemic and nonepidemic diseases, made with natural and artificial antibody and with antigen prepared from green-producing or alpha streptococci isolated in studies of persons suffering from the respective diseases and of well controls remote from epidemics, are reported.
The reactions to intradermal injection of natural antibody prepared in horses and artificial antibody prepared in vitro with the respective streptococci, indicating specific antigen in skin or blood and, hence, corresponding specific types of streptococcal infections, ran closely parallel. The reactions were usually proportional to the severity of respective symptoms, fairly constant in chronic disease, greatest in the early stages of acute disease, and gradually became less pronounced and finally disappeared after recovery.
Reactions to intradermal injection of antigen, indicating specific antibody in skin or blood, were often slight or absent at the onset of acute respiratory infections and epidemic poliomyelitis, but gradually increased in size as recovery occurred, and then disappeared usually as antigen also disappeared.
There was a great difference in the length of time that specific antigen was demonstrable in skin or blood in the natural course of different acute diseases. The reaction indicating specific streptococcal antigen, in acute respiratory infections followed by a transient immunity, usually disappeared in two weeks, whereas in epidemic poliomyelitis, followed by an enduring immunity, the reaction usually persisted for six or eight weeks. The erythematous reactions are not considered diagnostic of disease but rather diagnostic of the presence in skin or blood of respective specific streptococcal antigen and antibody and, hence, of specific types of streptococcal infections.
The reactions obtained on intradermal injection of natural and artificial streptococcal, antibody or of antigen are almost certainly not allergic or urticarial in character, nor are they due to histamine. Wheal and pseudopodia formation and itching, characteristic of allergic and histaminic reactions, almost never occurred.
Reactions to antibody in persons suffering from the different diseases, and who reacted most strongly to homologous antibody, were relatively greater to antibody prepared from streptococci isolated from persons suffering from more closely related diseases than to antibody prepared from streptococci isolated from persons suffering from more distantly related diseases. Reactions in persons ill with various diseases were minimal to antibody prepared from streptococci isolated from well persons remote from epidemics. Moreover, reactions in well persons and persons ill with noninfectious diseases remote from epidemics were slight or entirely negative. Reactions to control NaCI-solution, to which 0.2 per cent phenol had been added after autoclaving, were slight or negative alike in ill and well persons.
Therapeutic injection of natural, and especially of artificial, antibody caused a greater reduction in antigen and a great increase in antibody in the course of hours than occurred in the natural course of acute disease during several to many days. With striking reduction of antigen and increase of antibody following therapeutic injection of artificial antibody, there was usually a corresponding clinical improvement and, in the very early stages of respiratory infection and poliomyelitis, abrupt disappearance of symptoms.
The cutaneous tests which have been developed and reported herewith are considered of importance because they are strictly objective, easily performed and controlled, and because the information obtained is in such strict accord with the demonstration, by animal inoculation, serologic and cataphoretic methods, of the presence of specific types of alpha streptococci in the diseases studied.
The supernatant solutions are designated as artificial or thermal antibody because they were prepared in vitro and because they agglutinated the respective streptococci in high dilution, hastened the destruction of streptococci on intraperitoneal injection in animals, caused a prompt reduction in antigen and increase in antibody on therapeutic injection, and had apparent curative action in the treatment of persons suffering from streptococcal infections homologous to the streptococcus from which the antibody injected was prepared.
Acknowledgment of the co-operation of the many attending physicians and nurses, of hospital superintendents and health officers, which made these studies possible, is hereby made.
References Cited:
- Foshay, Lee: The nature of the bacterial-specific intradermal anti-serum reaction. Infect. Dis., 59:330-339, 1936.
- Francis, T., Jr.: Value of skin test with type specific capsular polysaccharide in serum treatment of type I pneumonococcus pneumonia. Exper. Med., 57:617-631, 1933.
- Rosenow, E. C.: Elective localization of streptococci. A.M.A., 65:1687-1691, 1915.
- Rosenow, E. C.: The production of spasm of the diaphragm in animals by living cultures, filtrates, and the dead streptococcus from cases of epidemic hiccup. lnfect. Dis., 32:72-94, 1923.
- Rosenow, E. C.: Serologic specificity of streptococci having elective localizing power as isolated in the study of various diseases of man. Infect. Dis., 45:331-359, 1929.