
Access to all articles, new health classes, discounts in our store, and more!
Diagnosis of Pigmentation of the Oral Tissues
Presented at the First Symposium on Oral Pigmentation, Veterans Administration Hospital, Tuskegee, Alabama, November 20, 1959. Published in The Journal of Periodontology, Vol. 31, pp. 375-382, October 1960.
* * *
A rational and practical knowledge of the significance of pigmentation of the oral tissues hinges upon: (1) a definition of pigmentation, (2) an appreciation of physiologic pigmentation, and (3) a logical system for considering the various pathologic factors which produce oral pigmentation.
Definition
An examination of almost any medical and lay dictionary1, 2 discloses that the term pigmentation signifies the deposition of coloring matter. It follows from this definition that there is a difference between oral pigmentation and oral color. The color of the teeth and oral mucosa is the hue which results from the deposition of various coloring matters plus the color contribution of the subjacent circulating blood in the vascular system. The yardstick to be used in this report will be based on the more restricted definition. In other words, only those conditions will be discussed which result from the deposition of coloring matter in the hard or soft tissues of the oral cavity.
Under so-called normal conditions, pigments are present in the oral tissues which contribute to physiologic pigmentation and to the different hues encountered in the mouth. The problem of physiologic pigmentation may be divided conveniently into two categories: (1) the dental tissues, and (2) the soft tissues.
Dental Tissues
Different teeth and different portions of the same tooth vary in hue because of the relative presence and absence of pigments.3For example, the maxillary central incisor is the lightest tooth in the mouth. In other words, this upper anterior tooth approaches white more closely than any of the other teeth in the arch. In addition, the incisal third of the maxillary central incisor is the lightest portion of the crown of the tooth. On the other hand, the cervical third of the tooth is darkest. In general, the maxillary lateral incisor is slightly darker than the central incisor. Also, as in the case of the central incisor, the incisal third is lightest and the cervical third darkest. As one proceeds posteriorly, the teeth become darker and the incisal or morsal third is generally the lightest portion of the crown. The same pattern exists in the lower jaw with the exception that the mandibular lateral incisor is usually slightly lighter than the central incisor. Still, the posterior progression to darkness and the darkening cervical ward on each tooth prevail.
The consensus is that the color of the natural teeth is some shade of yellow due principally to the translucency of the enamel and the pigment content of the dentin. Thus, the incisal third of the maxillary central incisor looks relatively white because there is very little subjacent dentin to contribute the yellow cast and the bulk of enamel incisally is greatest. On the other hand, the thickness of the enamel at or near the neck of the tooth is relatively narrow and there is considerable dentin beneath the thin enamel layer.
Soft Tissues
The color of the soft tissues of the mouth is the result of the product of a different set of circumstances. In the first place, the cytoarchitecture of different mucosal areas is quite distinct. In general, three different types of mucosa are present.3
Lining Mucosa: The first is strictly a lining mucosa. It is very thin, minimally hornified, and very delicate. This is the mucosa which can be observed in areas of the oral cavity which are normally under relatively little mechanical trauma. Thus, one can observe this type of lining mucosa in the buccal area, sublingual space, and the soft palate. In general, lining mucosa is more pink or red than other mucosal zones because of the thinness of the lining wall and the relative nearness of the subjacent vessels to the surface. Color, then, is a function to a large degree of the amount of reduced or oxygenated hemoglobin circulating in the subepithelial blood vessels. Since such color change is not due to the deposition of coloring matter, it will not receive attention in this report. Pigments can and do normally occur in the tissues of the lining mucosa. The most common such pigment is melanin though carotene, caretenoids, and possibly melanoids may also be present.
Masticatory Mucosa: A second type of mucosa is admirably suited to withstand considerable mechanical and chemical trauma.4 This type is observed in the gingiva and the hard palate. The tissue is characterized principally by a relatively high degree of keratinization. Thus, two points become important. First, the underlying blood vessels are not as close to the surface, hence do not contribute to redness or pinkness as much as in the lining mucosa. Secondly, the keratinization is due to production of eleidin which, in itself, yields a yellow cast. However, pigments can be demonstrated in these tissues. The most common pigment is melanin though carotene, caretenoids, and possibly melanoids may also be present to contribute to physiologic pigmentation.
Specialized Mucosa: The tongue structure is distinctive and quite different from the lining and masticatory mucosae described. Here one encounters on the dorsum of the tongue an area peppered with different types of papillae. The filiform papillae are long and narrow. A large portion of a filiform papilla is taken up by epithelium. Thus, the filiform papillae yield a yellow cast because of the presence of eleidin. In contrast, the second most common projection from the surface of the tongue is the fungiform papilla. This organ is not as heavily keratinized. Therefore, the yellow cast is not as obvious. In addition, because of the relative lack of keratinization, the subjacent blood vessels are apparent. The end result is a projection which appears pink to red in part because of the absence of pigment (eleidin) and partly because of the relatively greater vascular supply. Because of the fewness and posterior position of the circumvallate papilla, they are not significant in any consideration of lingual pigmentation.
One other point must be mentioned with regard to pigmentation and specialized mucosal tissue. The distribution of papillae on the dorsum of the tongue allows the entrapment of foreign bodies in the interpapillary spaces. This becomes important because of the greater possibility of pigmentary deposition on the dorsum of the tongue as against similar pigmentary incarceration on the lining and masticatory mucosae.
Pathologic Pigmentation
The diagnosis of pathologic pigmentation hinges upon an understanding of: (1) the etiologic factor or factors, and (2) the method by which the pigment reaches the oral tissues.
Biologic Factors
A number of microbial agents can exert an effect upon the dental or soft tissues and produce pigmentation. In addition, these microbes can attack the tissues from the outside (exogenously) or by way of the blood stream (endogenously).
Common examples of pigmentation the result of microbes operating exogenously are the very common green stain5 (Fig. 1) and orange stain6 noted in children. A relatively classic example of pigmentation the result of exogenous microbial action upon soft tissues is observed with thrush7 (Fig. 2).
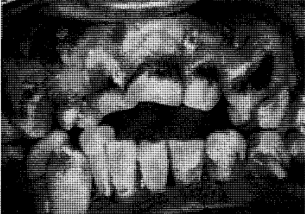
Fig. 1. Green stain due to microbial growth.
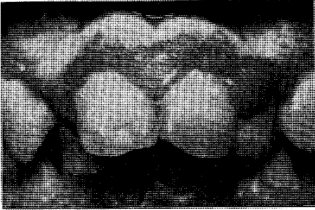
Fig. 2. Typical white color of thrush.
On the other hand, bacteria, viruses, fungi, and parasites can produce pigmentation of the dental and soft tissues by reaching these structures via the circulating blood stream. For example, the tooth may become discolored following bacterial invasion of the pulp. Thus, we have here an illustration (bacterial pulpitis8) the result of endogenous action of biologic factors upon the dental tissues (Fig. 3). In contrast, microbial factors may operate by destroying the vessel wall so that blood is permitted to lodge extravascularly. The end result of extravascular blood deposition leads to decomposition of hemoglobin and the appearance of pigment the result of iron in the tissues. This is the explanation for petechiae in infectious mononucleosis9 (Fig. 4).

Fig. 3. The darkened left central incisor is due to pulpitis secondary to microbial invasion.

Fig. 4. Typical pigmentary change (petechia) in infectious mononucleosis due to the perivascular deposit of blood.
Physical Factors
Physical factors may take one of several forms including mechanical, electrical, thermal, and radiation trauma. By far, mechanical trauma is most common. Physical trauma may act exogenously or endogenously and the effects may be directed at the dental and/or soft tissues. For example, food particles may lodge on the tooth surface or on the soft tissues and may remain for a variable period of time depending on the speed with which cleansing occurs. This type of pigmentation does not produce a diagnostic problem since the etiology is relatively clearcut and the therapy is simple and often unnecessary. On the other hand, endogenous influences may be operative so that the end result is pigmentation due to some type of physical trauma. This is well illustrated in mechanical pericementitis.10 This is a situation where a mechanical insult is brought to bear upon a tooth surface so that there is eventual pulpal death and alteration in the pulp and dentine because of the absence of nourishment to the tooth. The very simple and obvious example of the results of physical trauma upon the soft tissues is shown in the contusion (Fig. 5). Here the situation is one in which physical trauma is brought to bear upon the soft tissues so that small blood vessels are caused to rupture. The blood which lodges extravascularly then undergoes decomposition. First the area appears red, then purple, then black and blue, and finally the area clears up through a progression of color changes leading through brown and green.
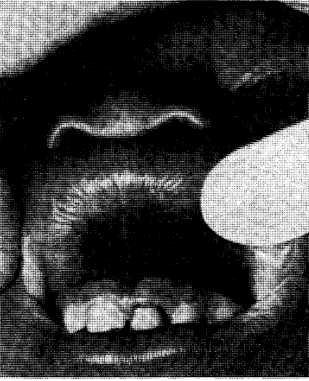
Fig. 5. Contusion to the lip causing the extravasation of blood into regional tissues and eventual decomposition of blood products.
Chemical Factors
A host of chemical substances can exert an effect upon the dental or soft tissues exogenously or endogenously and in this manner lead to pigmentation. Certainly, tobacco stain is a common illustration to show the deposition of various fractions from tobacco upon the tooth surface and the neighboring soft tissues. However, as has been previously mentioned, it is difficult to delimit exogenous or endogenous factors for, in many cases, both are operative. For example, the systemic intake of fluorides in the drinking water may produce changes in the tooth surface characterized by small chalky areas.11 However, because of the alteration in the tooth surface, exogenous materials find it more easy to lodge upon the tooth. Thus, the pigmentary changes described with fluorosis actually are the result of exogenous deposits upon a tooth surface which allows such deposits to lodge easily (Fig. 6). Occasionally foreign bodies are present in the soft tissues and, in their disintegration, color the neighboring structures. This is commonly encountered in the situation whereby a small fragment of amalgam is trapped in the oral soft tissues.

Fig. 6. The exogenous pigmentation associated with classical fluorosis made possible by the changes in the enamel surface.
On the other hand, endogenous factors may play a more dominant role than has been shown, for example, in the case of fluorosis. For instance, chemical pulpitis12 may follow pulpal death due to a silicate restoration which has been placed in a tooth without appropriate protection of the subjacent tissues. Similarly, endogenous factors may play a role in the development of pigmentation of the soft tissues. For instance, many cardiac patients are required to take mercurial diuretics. This, of course, means that mercury is circulating in the blood stream. In areas of inflammation hydrogen sulfide is formed. The end result is that the mercury unites with hydrogen sulfide to produce mercuric sulfide. This condition, mercurialism,13 is commonly encountered in the free marginal gingiva (Fig. 7). This is also believed to be the explanation for the pigmentary changes in the gingiva in patients with plumbism.14
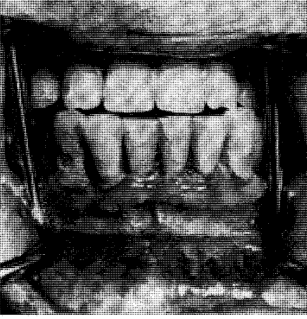
Fig. 7. Mercurialism with metallic gingival pigmentation.
Hormonal Factors
Mention has already been made that each group of factors may operate exogenously and endogenously. It would, therefore, seem that these two routes must be operative in the case of hormonal imbalance. However, little study has been directed to the effect of exogenous hormonal factors upon dental and soft tissues. Certainly, the effect is clearcut that there is deepening of color of the skin and mucosae in patients with hyperpituitarism15 and hypoadrenalism.15 The classical descriptions of so-called bronzing of the skin are described with Addison’s disease (Fig. 8).
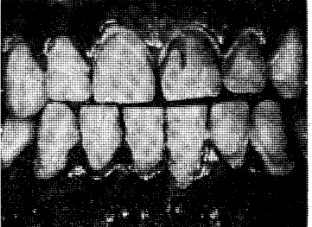
Fig. 8. Brown pigmentation of the oral mucosa (melanosis) due to hypoadrenalism.
Developmental Factors
Developmental factors are conditions in which alterations occur in the oral tissues either because of an inheritable factor or because of changes in the developing fetus during intrauterine maturation. Developmental disorders may be accompanied by oral pigmentation for two reasons. In the first place, the oral tissues may be malformed in such a way as to produce abnormal pigmentary patterns. This is well illustrated by the hereditary opalescent dentin16 with or without osteogenesis imperfecta (Fig. 9). In this instance, the chemistry of the dentin is so altered that, in combination with the usual translucency of enamel, the dental tissues appear opalescent. Amelogenesis imperfecta17 of the enamel hypoplasia type also produces an unusual pigmentation of the teeth. In this instance, it is due to the inadequate production of enamel so that the underlying dentinal color is more apparent. Consequently, persons with this problem show unusually yellow teeth (Fig. 10). An example of soft tissue pigmentation of developmental origin is well illustrated in intestinal polyposis18 (Fig. 11). Here one encounters macular lesions in the oral cavity which actually represent discrete depositions of melanin.

Fig. 9. Hereditary opalescent dentin in a 19 year old boy with osteogenesis imperfecta. The crowns are disproportionately large for the roots and the pulp chambers and canals are obliterated.


Fig. 10. The teeth in amelogenesis imperfecta (enamel hypoplasia type) are yellow because of the relative absence of enamel. Shown in the roentgenograms is the absence of enamel roentgenopacity.

Fig. 11. Melanin spots characteristic of intestinal polyposis.
On the other hand, the developmental factor may so alter the hard or soft tissues of the oral cavity so as to invite exogenous stains to deposit more easily. This is illustrated in amelogenesis imperfecta17 (Fig. 12) of the enamel hypocalcification type. Here the problem is not one of adequate enamel matrix formation but one of imperfect calcification. Consequently, the enamel is soft and is lost from the tooth very easily. The end result is a roughened surface which invites the deposition of outside stains.
Fig. 12. Amelogenesis imperfecta (enamel hypocalcification type). The pigment is exogenous.
Nutritional Factors
Nutritional imbalance is apt to be associated with pigmentary alterations of the soft tissues for two reasons. In the first place, the absence of certain nutrients from the dental tissues may so alter the chemistry of the enamel and dentine as to yield a tooth of unusual color. Also, vascular fragility and permeability are very much dependent upon nutritional factors such as ascorbic acid19 (Fig. 13). Consequently, with increased vascular fragility and permeability the extravascular appearance of blood is very possible. The end results are petechiae and/or ecchymoses.
Fig. 13. Petechiae in the palate due to increased capillary fragility and permeability secondary to Vitamin C deficiency.
Nutritional factors play an important role in normal maturation of oral tissues. Consequently, with nutritional imbalance during the formative years of dental development the end result may lead to hypoplasias. These roughened surfaces permit the more ready deposition of exogenous pigment. This is demonstrated in rickets20 (Fig. 14).

Fig. 14. Rachetic teeth. The exogenous pigmentation is possible because of the roughened tooth surface.
Stress Disorders
Every local stimulus is accompanied by a local response. However; every local excitatory force is also associated with a generalized reaction.21 This systemic response is important to the organism encountering the local stressor. Should the generalized reaction not occur, then serious complications may ensue. Thus, more correctly, stress disorders are really disorders due to lack of adaptation. Any serious stressor during dental development may leave its mark upon the forming dental tissues. For example, high fever in a child may be recorded permanently in the dental apparatus by way of pits, fissures, or other evidences of hypoplasia. These roughened areas make it more possible for exogenous stains to attach themselves to the tooth structures. One of the most important factors in the maintenance of vascular fragility and permeability is adrenocortical balance. In disorders due to lack of adaptation to stress, hypoadrenalism is present. Thus, with reduced adrenal activity there is the possibility of increased vascular fragility and permeability. Consequently, petechiae and ecchymoses may be present.
Summary
- Strictly speaking, pigmentation signifies the deposition of coloring matter in a tissue. In contrast, hue represents the color of a tissue which is due to pigmentation and the status of the subjacent vascular supply.
- Under normal conditions, different teeth and different portions of the same tooth differ in hue because of the thickness of the enamel and the character of the subjacent dentin.
- Under physiologic conditions, different portions of the oral mucosa differ in color in part because of various pigments present in the tissues and also because of the blood supply.
- In some instances, biologic, physical, chemical, hormonal, developmental, nutritional, and stress factors may be singly responsible for the presence of pathologic pigmentation. These seven factors may operate by exogenous or endogenous mechanisms.
- In most cases, pathologic pigmentation is the result of a combination of circumstances operating both exogenously and endogenously.
References Cited:
- Dorland’s Medical Dictionary. Twenty-third Edition. 1957. Philadelphia, W. B. Saunders Company.
- Macmillan’s Modern Dictionary. 1943. New York, The Macmillan Company.
- Cheraskin, E. and Langley, L. L. Dynamics of oral diagnosis. 1956. Chicago, The Year Book Publishers.
- Glickman, I. Clinical periodontology. Second edition. 1958. Philadelphia, W. B. Saunders Company.
- Leung, S. W. “Naturally occurring stains on the teeth of children.” J.A.D.A. 41: #8, 191-197, August 1950.
- Bartels, H. A. “A note of chromogenic microorganisms from an orange colored deposit of the teeth.” Internat. Jour. Orthodont. 25: #8, 795-796, August 1939.
- Lighterman, I. “Oral moniliasis. A complication of Aureomycin therapy.” Oral Surg., Oral Med. and Oral Path. 4: #11, 1420-1426, November 1951.
- Herbert, W. E. “Correlation of clinical signs and symptoms and histological condition of the pulp of 52 teeth.” Brit. Dent. Jour. 78: #6, 161-174, March 16, 1945.
- Pader, E. and Grossman, H. “Thrombocytopenic purpura in infectious mononucleosis.” N. Y. Jour. Med. 56: #12, 1905-1910, June 15, 1956.
- Macdonald, J. B., Hare, G. C. and Wood, A. W. S. “The bacteriologic status of the pulp chambers in intact teeth found to be nonvital following trauma.” Oral Surg., Oral Med. and Oral Path. 10: #3, 318-322, March 1957.
- Bauer, W. H. “Experimental chronic fluorine intoxication. Effect on bones and teeth.” Amer. Jour. Orthodont. and Oral Surg. (Oral Surg. Sect.) 31: #12, 700-719, December 1945.
- Zander, H. A. and Pejko, I. “Protection of pulp under silicate cements with cavity varnishes and cement linings.” J.A.D.A. 34: #12, 811-819, June 15, 1947.
- Akers, L. H. “Ulcerative stomatitis following the therapeutic use of mercury and bismuth.” J.A.D.A. 23: #5, 781-785, May 1936.
- Schour, I. and Sarnat, B. G. “Oral manifestations of occupational origin.” J.A.M.A. 120: #15, 1197-1207, December 12, 1942.
- Davis, M., Boynton, J., Ferguson, J. and Rothman, S. “Studies on pigmentation of endocrine origin.” Jour. Clin. Endocrinol. 5: #3, 138-146, March 1945.
- Finn, S. B. “Hereditary opalescent dentin. I. An analysis of the literature on hereditary anomalies of tooth color.” J.A.D.A. 25: #8, 1240-1249, August 1938.
- Weinmann, J. P., Svoboda, J. F. and Woods, P. W. “Hereditary disturbances of enamel formation and calcification.” J.A.D.A. 32: #7, 397-418, April 1945.
- Jeghers, H., McKusich, F. A. and Katz, K. H. “Generalized intestinal polyposis and melanin spots of the oral mucosa, lips, and digits: a syndrome of diagnostic significance.” New England Jour. Med. 241: #25, 993-1005, December 22, 1949; #26, 1031-1036, December 29, 1949.
- Mead, S. V. “Studies of the effect of ingestion of citrus fruit upon gingival hemorrhage.” Jour. Dent. Res. 23: #1, 73-79, February 1944.
- Eggnatz, M. Rickets. “Caries, hypoplasia and malocclusion of the teeth.” Amer. Jour. Orthodont. and Oral Surg. 27: #7, 379-393, July 1941.
- Selye, H. The stress of life. 1956. New York, McGraw-Hill Book Company.