
Access to all articles, new health classes, discounts in our store, and more!
Clinical Aspects of Abdominal Pain
Read before the Section on Gastro-Enterology and Proctology at the Eighty-Fourth Annual Session of the American Medical Association, Milwaukee, June 16, 1933. Published in The Journal of the American Medical Association, February 3, 1934, Vol. 102, pp. 341-344.
* * *
Pain is a necessary part of the animal’s mechanism of defense. Exaggeration of a sensory stimulus, whether it is transmitted centrad over cranial or spinal afferent nerves from the skeletal structures or over the afferent systems that accompany the sympathetics and parasympathetics to the internal viscera, may lead to discomfort or pain. Pain is the automatic danger signal that tells the individual to beware, for the normal mechanism is irritated in an abnormal manner, or even its integrity may be threatened.
In considering pain, it is necessary for the clinician to remember that the perception of painful stimuli is bound up with the patient’s physiologic stability and that the complaint of sensory changes will differ greatly in different individuals. What may be a painful stimulus to one person may not be to another.
The Visceral Nervous System
The sympathetic or thoracicolumbar and the parasympathetic or craniosacral components that make up the vegetative or autonomic nervous system form a correlating mechanism which in conditions of health brings the action of all the viscera into harmony and, further, in conjunction with the voluntary nervous system, brings visceral and skeletal activity into harmony. In conditions of disease, these nerves furnish the mechanism for creating disharmony.
Every secreting gland and every bit of smooth muscle is supplied by neurons belonging to one or both of these systems. Each of these systems consists of efferent neurons, which transmit stimuli to and produce action in structures, and afferent neurons, which pick up stimuli that originate in the various structures and carry them centrad, where they transmit them to efferent neurons and thereby translate them into action in the same organ or in other organs or parts. If the stimuli are of normal strength they are spent without disturbing physiologic function, but if of extraordinary strength they produce abnormal effects which result in either increased glandular secretion or increased muscular activity and not infrequently altered sensibility, which may be discussed for clinical convenience as a sensory reflex.
Nature of Visceral Pain
There has been a great deal of discussion concerning the nature of visceral pain, largely because of a lack of knowledge of the visceral nervous system.
Early in the investigation of visceral pain, Lennander and Mackenzie showed that the viscera do not respond to the same character of stimuli that cause pain in somatic structures. They showed that the viscera may be cut, pinched and burned without causing pain. This necessitated that some theory be advanced to explain this difference.
Not only were clinicians surprised to learn that viscera do not contain nerves that have the property of showing the same acute pain when injured as do skeletal structures, but they have been slow to accept it, because they have been familiar with many forms of acute visceral pain in their clinical practice.
Visceral pain, as studied in the parietal pleura and parietal peritoneum, has been long known to be acute in character and further to be expressed immediately over the areas of inflammation. Certain inflammations of abdominal viscera, too, have been known to show acute pain on deep pressure over the organ.
These facts seemed to justify clinicians, in the absence of accurate knowledge of visceral neurology, in assuming that the viscera and skeletal structures show pain in the same manner, both at the point of injury. This opinion prevailed, regardless of the fact that it was well known that the heart refers its pain regularly to the left arm and upper portion of the chest wall and that the diaphragm refers its pain to the shoulder. Later, I pointed out that the lung expresses what discomfort there is accompanying inflammation of its tissues in the somatic areas supplied by spinal nerves that arise from the midcervical segments of the cord, producing changes in sensibility in areas sometimes over the area of inflammation and sometimes removed from it, and even removed from the lung itself, as in the neck over the sternocleidomastoid and trapezius muscles.
Thus it has become evident that there is a type of visceral pain which is expressed wholly, neither in nor over the pathologic process nor even in the diseased viscus itself, but at a distance, in definite areas on the surface of the body, to which it is referred. Study showed that these areas are supplied by neurons which are closely associated in the central nervous systems with the neurons which supply the viscus in question and that there is great regularity in the localization. This type of pain was therefore designated as referred pain, being referred from the visceral neuron to the skeletal neuron for its expression. It was later proved that this referred pain is segmental in nature and that it follows certain definite laws as to its localization.
Pulmonary pain is not of an acute character. Neither is pain arising in the liver, the cortex of the kidney or the spleen. In fact, the usual pain in any solid viscus, so long as the inflammation is confined to the parenchyma of the organ, is not acute. A large area of a lung may be involved in a destructive process, and, unless the overlying pleura takes part in the inflammation, the patient may be wholly unaware of its presence, as far as sensation is concerned. So may destruction occur in the cortex of the kidney and the parenchyma of the liver without causing a disturbance in sensibility commensurate with the destruction. This is an important fact in the argument that has been advanced to explain the nature of visceral pain. There is some factor connected with hollow viscera, on the other hand, which causes them to respond with a greater degree of sensitiveness than the solid organs, when injured. The facts of contractibility and distensibility have been considered to be the most probable cause of this difference. The intestine, the ureter or the common bile duct, which under usual conditions of physiologic activity give their possessors no evidence of their existence, under spasm or distention may cause acute pain. This fact may be interpreted as indicating that referred visceral pain, as compared with referred visceral discomfort, depends first on the character of the organ in which the stimulus arises and secondly on the severity of the stimulus. This is modified always by the particular sensitivity of the patient.
Head interpreted his classic studies on pain as indicating that the afferent nerves of the viscera are the same as those which furnish skeletal tissues with deep and protopathic sensibility and, further, as showing that visceral pain is produced by a mechanism similar in nature to that which causes the less acute sensations found in the skeletal structures. This view is accepted by many but is rejected by others.
The visceral sensory system, like the sensory system of the deep skeletal structures, is not able to express discriminating sensibility. Under ordinary circumstances it is assumed that the afferent visceral neurons are subject to an inhibition from higher centers, which prevents the impulses from reaching the perceptive centers in the brain and, instead, are held to lower levels in the central nervous system, where they are regularly transformed into reflex effects without the individual’s knowledge. Under circumstances of unusual stimulation, however, the inhibition may be overcome and the impulse transmitted to the thalamus and cortex. In case it should reach the higher centers, the pain is not ascribed wholly to the viscus in which the impulses arise but is referred partly to the surface of the body. That deep pressure over inflamed visceral tissues can also produce pain which is felt in the viscus is accepted as a fact by many.
Head, recognizing the segmental nature of referred pain, suggested in explanation of it what has come to be known as Head’s law:
When a painful stimulus is applied to a part of low sensibility in close central connection with a part of much greater sensibility, the pain produced is felt in the part of higher sensibility rather than in the part of lower sensibility to which the stimulus was actually applied.
In other words, visceral stimuli are transmitted centrad over neurons that belong to the deep or the protopathic systems–neurons of the same order as those found in the deeper skeletal tissues. Should the patient’s threshold for stimuli be below normal, or should these stimuli become abnormally severe, as under conditions of undue irritation or disease, they may produce pain.
Segmental Nature of Visceral Pain
An important factor in visceral pain is its regular localization in definite somatic areas.
It is a physiologic axiom that each part adapts itself to its particular environment and develops whatever conditions are adequate for normal physiologic action in that environment. Since the more acute types of sensibility (pain) carry with them the more ready protective reaction, and since quick protective response is not regularly needed by the internal viscera, visceral pain is not developed to the same degree of acuteness as that in the skeletal structures. Under unusual circumstances, however, such as those which produce excessive irritation or injury, the structures are not left without defense, for a pain mechanism sufficient for the emergency is called into play.
When painful visceral stimuli reach the perceptive centers in the brain, the effect is regularly redistributed segmentally with the same degree of definiteness of localization as the visceral, motor and trophic reflexes that are mediated in the cord; if the effect is expressed in adjacent segments, this too follows the law that governs the spread of reflexes.
Thus visceral pain may be either narrowly localized or widely spread but always follows definite physiologic laws. In the former case it may be confined to those segments which receive the major portion of the afferent impulses from the viscus; in the latter, it may be distributed through intersegmental neurons to either higher or lower cord levels. While each viscus receives its sympathetic nerve supply from several segments of the cord, there are usually two or three segments that may be looked on as being the chief centers of supply. The latter proves to be the principal center for the mediation of reflexes. Thus the heart receives its sympathetic supply from the upper five, six or seven thoracic segments, yet cardiac pain is most commonly expressed over neurons from the first, second and third segments.
Difficulty of Comprehending Reflex Effects
Among the difficulties that are encountered in attempts to study visceral pain clinically are (1) the individual variation in reaction of different persons to stimuli of the same degree of strength, (2) the patient’s inability to describe his sensations accurately, and (3) the physician’s inability to comprehend and interpret properly the patient’s descriptions.
The same difficulty is encountered in interpreting reflex secretory and motor effects in organs because, except in cases of a low degree of physiologic stability, only major disturbances are noted and complained of by the patient. Increased tension in the skeletal muscles, which is commonly present when viscera are inflamed, too, is often neither perceived by the patient nor recognized by the examiner.
Reflex effects may be slight or severe, and of short or long duration, according to the reacting powers of the patient and the character of the visceral lesion that causes them. When visceral inflammation is of long duration, degeneration takes place in those skeletal tissues which take part in the reflex and may be detected either on inspection or palpation, or both. It does not seem illogical to assume that degeneration may also result in those visceral tissues which are affected reflexly by chronic inflammation. Clinical experience would indicate this, for it often shows a permanent functional disturbance in those viscera which are in close reflex relationship with organs that are chronically inflamed; for example, the stomach in case of disease of the gallbladder. I have found this also to be the case in chronic inflammation of the lungs, pleura, peritoneum, kidney and intestine. In the case of the lungs, I have been able to establish beyond question that reflex trophic changes may be produced not only through the sympathetic afferents and spinal nerves but also through vagus afferents and the mediating cranial nerves, particularly those supplying the facial muscles, the tongue and the mucous membranes of the nose, pharynx and larynx. Paths similar to those from the lung are open for other viscera, and chronic inflammation in them is probably followed by the same effects.
Difference in Acute and Chronic Pain
Chronicity and previous disease in the viscera are often followed by altered visceral sensibility. Visceral pain may be caused by active inflammation at any time and may recur after all evidence of active inflammation in the viscus has long disappeared. This is particularly to be expected in patients of the hypersensitive class, although it is frequently met in the hyposensitive, too. This chronic pain is explicable on the basis of a permanent lowering of the threshold for stimuli or even a permanent injury to the sensory neurons, which causes them to show pain on a minimal stimulation, even though the stimulus is such that it would not be noticed were the neuron normal. This recurrent pain is not sufficiently appreciated by clinicians and is often misinterpreted as meaning active disease, when in reality it is an expression of permanent injury to the sensory neurons which causes them to respond unphysiologically.
The recurrent pain that comes on without recurrent visceral inflammation is rather a discomfort than a pain. It may appear at any time after a given viscus has been diseased.
Recurrent pain may occur in the neurons associated with any viscus that has been the seat of prolonged inflammation and possibly prolonged irritation without inflammation. It has the same segmental characteristic as the more acute pain and is sometimes difficult to differentiate from it. I have found it in those who have previously suffered from disease of the lungs, pleura, gallbladder, ulcer of the stomach and duodenum, tuberculous peritonitis, tuberculosis of the intestine e, diverticulitis (personal experience), tuberculosis of the kidney and disease of the uterus and adnexa. It is also fairly well recognized in arthritis.
It seems that there is an inability on the part of these injured neurons to adapt themselves to unusual requirements of physiologic adjustment, whether originating in the external or in the internal environment. The change in sensibility is manifest under many conditions, such as changes in the weather, seasonal changes, tiring, such depressive emotions as worry, discontent and unhappiness, and during menstruation. While these factors differ widely in their nature, it is evident that each one calls for an unusual physiologic adjustment on the part of the patient; it will be further noticed that the individual fails to react normally only in those particular neurons which are segmentally connected with organs that were formerly diseased. Thus the patient who has had or who at the time is suffering from chronic lung trouble experiences discomfort in the segments innervated particularly by the third, fourth and fifth cervical nerves; the man who formerly had ulcer of the stomach may note pain in the skeletal areas supplied by the sixth and seventh thoracic segments to the left of the median line, while the woman with past or chronic pelvic inflammation feels the pain in the lower lumbar and sacral regions. It is a further fact that the degree of discomfort varies greatly according to the physiologic stability of the patient, being most severe in the most unstable. This type of pain is inadequately appreciated. It causes both physicians and patients much needless anxiety and results in operations when no serious danger exists.
Usual Location of Pain for the Principal Abdominal Viscera
Since the cell bodies of the afferent neurons that supply a given viscus are located in the same segments of the cord as the efferent neurons going to the viscus, and since the cell bodies of the somatic, motor and sensory nerves, which express reflex action and referred visceral pain, are located in the same segments, by knowing the connector nerve supply of an organ one also may know the skeletal nerves through which, and the tissues in which, reflexes from that organ will be most apt to be expressed. In case reflex effects and referred pain spread, they are most apt to be expressed by neurons arising either above or below in segments adjacent to those which the afferent impulse enters.
In figure 1 is shown the connector neurons which bring into connection with the cord those sympathetic cells which lie in peripheral ganglions and give origin to the nerve fibers that supply each of the more important viscera. In figure 2 is shown the arrangement of the somatic segments from which one may see the location of the pain from the viscus, with corresponding segmental innervation. It will be noted that in their sympathetic nerve supply the organs may be arranged in groups and that there is some overlapping in the distribution of the neurons to the groups themselves and also in the various organs of the groups; but, regardless of this fact, the main supply to the various organs may be arranged in a definite progressive order from the upper segments to the lower, and the somatic segments showing referred pain follow a similar progressive order. This schema can be only approximately correct with present knowledge, because the exact innervation of some of the organs is still undetermined; for example, innervation of the heart is usually given as arising in the upper five or six thoracic segments, yet operations for angina have shown that even the seventh thoracic connector neuron carries painful impulses.
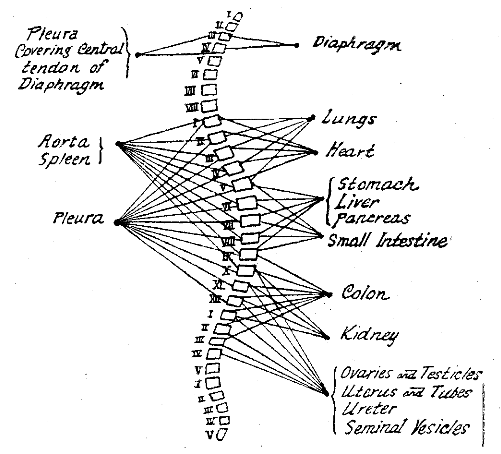
Fig. 1–The connector neurons for the important thoracic, abdominal and pelvic viscera. The connecting neurons are those which belong to the thoracolumbar outflow except those going to the diaphragm and pleura, which are spinal nerves. The motor cells for the viscera are found in the various collateral ganglions. This shows that the innervation of the various viscera may be divided into groups. The heart and lungs are innervated from practically the same segments, the upper first to the sixth thoracic. The stomach, liver and pancreas from the same segments, fifth to the ninth thoracic. The colon, kidney and pelvic viscera from practically the same segments, ninth and tenth thoracic to the third and fourth lumbar. In spite of this grouping in innervation, each organ is brought in reflex connection with efferent neurons, both sensory and motor, which are more or less definite, in such a way that the motor and sensory reflexes do not overlap as much as might be indicated
The first to the sixth dorsal segment give origin to connector neurons to the heart and lungs. The lungs, however, following their developmental relationships, express their somatic reflexes through cervical spinal neurons, particularly the third, fourth and fifth, while the heart joins with the corresponding thoracic nerves, showing reflex effects most commonly through the first, second and third thoracics. The major portion of the aorta, too, is supplied from the upper five or six thoracic segments and reflects through the same neurons as the heart.
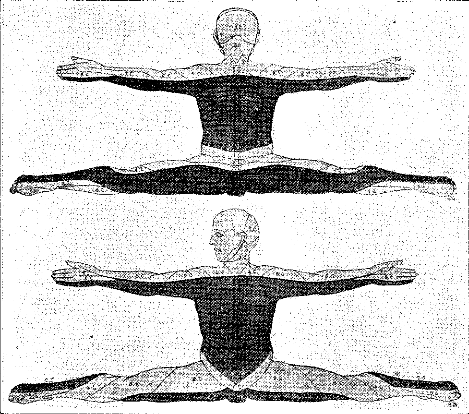
Fig. 2–Metameric distribution or transverse segmentation of cutaneous areas of sensibility of the human body, drawn with the limbs in the position of their embryonic growth. The series of dermatomes, which successively correspond to the cervical, lumbar and sacral routes, is indicated by different degrees of shading, and the different segments are numbered according to the spinal nerve supplying them. The location of the principal sensory disturbances from internal viscera can be determined from this diagram. (Constructed by Luciani from Bolk’s data.)
Following the lungs, heart and aorta caudad in the cord, the stomach, liver, gallbladder, pancreas and small intestine are innervated from the fifth to the ninth thoracic segment, but the skeletal area in which individual organs regularly express reflexes and referred pain is more or less distinct for each organ. The stomach expresses its pain most readily in the epigastrium in the median line and on the left side in areas supplied by the sixth and seventh thoracic spinal nerves, the liver and gallbladder in the median line, and on the right side. Posteriorly, the pain may be expressed in the interscapular region through the fifth to the ninth dorsal spinal nerve, on the left side from the stomach and on the right from the liver and gallbladder. The small intestine refers its pain most readily to the median line in areas supplied by spinal sensory nerves from the eighth, ninth and tenth thoracic segments.
The colon, kidney, ureter and bladder follow next in order, being supplied by neurons arising in spinal segments from the ninth thoracic to the third lumbar. Pain from the colon is expressed most commonly through the eleventh and twelfth thoracic nerves over the lower part of the abdomen, although pain may also be expressed in the first, second and third sacral segments. Kidney pain is reflected through the tenth, eleventh and twelfth dorsal nerves and the first lumbar nerve, both anteriorly over the abdomen and thigh and posteriorly in the lumbar regions. Ureteral pain is expressed both posteriorly and anteriorly.
Bladder pain is usualIy expressed through the eleventh and twelfth thoracic and from the first to the third lumbar segments, although it too may refer its pain through sacral nerves. This brings it low down in the abdomen anteriorly, as expressed through thoracic nerves, and in the peritoneum and down over the leg through the sacral nerves.
It must also be remembered that all the viscera with vagal supply may transfer stimuli to the fifth cranial nerve and express pain in some of its peripheral branches.