
Access to all articles, new health classes, discounts in our store, and more!
Bacteriological Studies on the Etiology and Chlorpromazine Treatment of Schizophrenia and Related Mental Disorders
Published in Journal of Nervous and Mental Diseases, Vol. 122, No. 4, pp. 321-331, October 1955.
* * *
In the extended studies on the etiology of diverse diseases, it was found that non-hemolytic or alpha streptococci as isolated from the end point growth of serial dilution cultures in dextrose-brain broth of nasopharyngeal swabbings, of apices of pulpless teeth, and sometimes from the blood of persons having diverse diseases localized electively on intravenous injection in the organ or organs of experimental animals corresponding to those involved in the patient from whom isolated. This occurred in high incidence even in studies of diverse diseases of the nervous system, such as peripheral neuritis, herpes zoster, intercostal neuralgia, dental neuritis and myositis, epidemic and persistent post-operative hiccup, “ether convulsions”, epidemic poliomyelitis and encephalitis, Sydenham’s Chorea, spasmodic torticollis, respiratory arrhythmia following influenza and epilepsy.1
In studies on the etiology of schizophrenia, a non-hemolytic streptococcus of low, general virulence was isolated consistently from the end point of growth in serial dilution cultures of dextrose brain broth from nasopharyngeal swabbings and in significant incidence from the blood which localized electively on intravenous injection in the brain of rabbits, monkeys and mice and on intracerebral inoculation produced symptoms simulating those in the respective patients from whom isolated.1 Furthermore, the streptococci, which localized electively in the brain of animals on intravenous injection, were agglutinated, and extracts of antigen of the streptococci were precipitated specifically by the serum of persons ill.2
Moreover, the euglobulin fraction of the serum of horses that had been immunized with respective specific types of the streptococcus and “thermal antibody” prepared from the streptococci on autoclaving of NaCl solution suspensions for 96 hours were found to elicit a similar immediate erythematous cutaneous reaction at the site of intradermal injection, indicating specific circulating streptococcal antigen. Intradermal injection of the respective streptococcal antigens elicited an immediate erythematous reaction, indicating specific circulating antibody.3,4,5
It is the purpose of this treatise to describe the methods used and to report the results obtained in a further study on the relation of a specific type of non-hemolytic streptococcus to schizophrenia and related mental disorders and the immunological action of chlorpromazine in the treatment of schizophrenia.
Methods
In order to determine the localizing properties of the streptococcus, one ml. of the culture that grew at the end point of growth of serial dilution cultures in dextrose brain broth from nasopharyngeal swabbings, of persons having schizophrenia or related mental conditions, usually at 10-6 and sometimes at 10-10 was injected routinely into a tail vein of mice. The streptococcus for the preparation of thermal antibody and other studies was isolated either from the end point of growth in the serial dilution cultures of nasopharyngeal swabbings or from the brain of mice etherized 24 hours after intravenous injection of such cultures. The pure culture of the streptococcus from the end point of growth of serial dilution cultures in destrose brain broth was inoculated into either 200 ml. or 3,500 ml. lots of 0.2 per cent dextrose broth prepared from ‘”Difco” peptone and yeast extract. The streptococci that grew in 18 to 24 hours at 35°C. in the smaller lots of dextrose broth were sedimented in a cup centrifuge, and those that grew in gallon lots were harvested in the revolving bowl of a Sharples’ supercentrifuge. The streptococci thus obtained were suspended routinely in dense, an estimated 2,000 billion organisms per ml. Of chemically pure glycerol, 2 parts, and saturated NaCl solution, 1 part, and stored in the dark at 10°C.
Streptococcal thermal antibody solutions and vaccines were prepared routinely from the streptococci in the dense glycerol saturated NaCl solution suspensions. THe vaccine represented suspensions in NaCl solution of 2 billion streptococci per ml. and heated al 70°C for one hour. Some of the streptococci partially dehydrated in the dense glycerol-NaCl solution suspensions remained viable for months, and antigenic specificity was thus maintained for several years. The highly specific results obtained with vaccines and thermal antibody in cutaneous, agglutinative test and in animal experiments are attributable in large part to the preservation of viability and antigenic specificity of the streptococci in the dense glycerol-NaCl solution suspensions. Readings of agglutinations were made and recorded as “unknowns”.
Streptococcal thermal antibody for cutaneous reactions indicating circulating antigen was prepared by autoclaving suspensions in NaCl solution containing 20 billion streptococci per ml. for 96 hours and diluting the supernatant with an equal volume of NaCl solution (+2 per cent phenol) and injecting approximately 0.03 ml. into the skin of the volar aspect of the forearm. The tests for circulating antibody were made by injecting intradermally .03 ml. of the supernatant of respective streptococci in NaCl solution containing 10 billion per ml. that had been heated at 70°C for one hour. The diagnostic erythematous reactions if positive occurred almost immediately. The maximal erythema was outlined with pen and ink, and the size of reactions was determined in sq. c.m. by matching circles of known sizes on a transparent sheet of cellophane 4 x 6″.
The agglutinative titers of the respective serums, spinal fluids and urines of persons stricken, shown in the tables, were determined as unknowns and were recorded in per cent. A four plus agglutination at each of four five-fold dilutions of the serum of 1-5 to 1-625 and for streptococci thermal antibody at four or five tenfold dilutions of 1-10 to 1-10,000, or 1-10 to 1-100,000 at each of the dilution is considered as 100 per cent, a one plus or 1/16 as 6 per cent.
Results of Cutaneous Tests in Schizophrenics Not Receiving Chlorpromazine
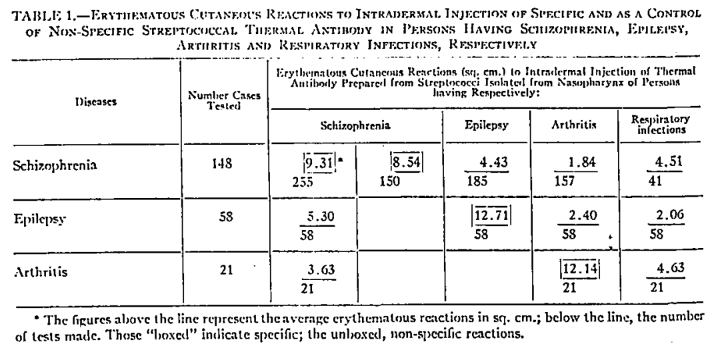
Sperilicily of non-hemolytic or alpha type streptococci as isolated in studies of schizophrenia, epilepsy and arthritis, respectively, is strikingly shown in table 1. It will be seen that the immediate erythematous reaction which followed the intradermal injection of the respective streptococcal thermal antibody solutions was maximal or specific for schizophrenia, epilepsy and arthritis and minimal to comparable injection of streptococcal antibody prepared from streptococci isolated in studies of respiratory infection.
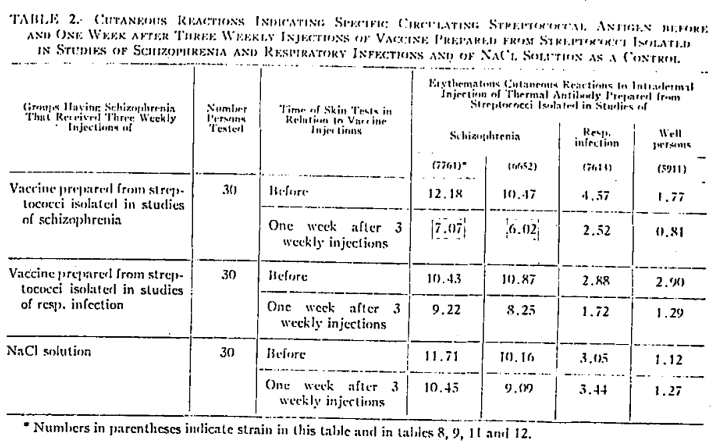
The cutaneous reactions in groups of persons having schizophrenia following the giving of subcutaneous injections, of specific and nonspecific streptococcal vaccine and of NaCl solution as a control as revealed by immediate erythematous reactions following intradermal injection of thermal antibody before and one week after three weekly immunizing subcutaneous injections of vaccine prepared from streptococci isolated in studies of schizophrenia, respiratory infection and well persons, respectively, are shown in table 2. The reactions to repeat intradermal injections of schizophrenic streptococcal thermal antibody which is taken to indicate circulating schizophrenic streptococcal antigen were maximal before giving schizophrenic streptococcal vaccine, far less following immunization with vaccine prepared from streptococci isolated in studies of schizophrenia, somewhat less following the giving of respiratory streptococcal vaccine, and negligible following comparable injections of NaCl solution. Clinical improvement occurred in significant incidence in persons receiving the vaccine prepared from the homologous streptococci.
The Agglutinative Titer of the Blood Serum of Schizophrenics for the Streptococcus
Streptococci isolated from the nasopharynx of persons suffering from diverse, especially chronic, diseases of the nervous system are so much alike that a precise classification on the basis of size, staining reactions and cultural characteristics is not possible. However, differentiation has been found readily possible on intravenous injection of rabbits and mice of the freshly isolated strains. The streptococci localized electively in the tissues or organs of injected animals corresponding to the ones affected in the spontaneously occurring disease.6,7 Moreover, streptococci that localized electively were agglutinated differentially by serum of respective persons ill and by thermal antibody prepared from freshly isolated strains of streptococci apparently causative of different diseases.8
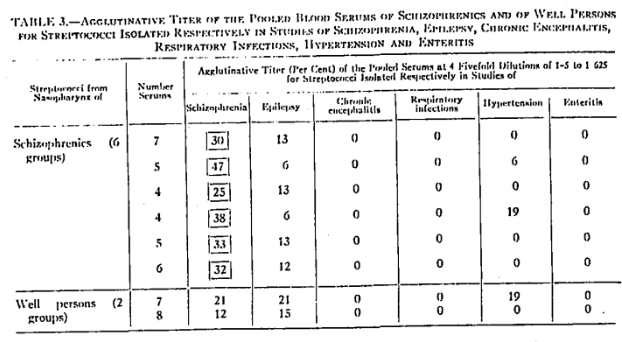
Evidence indicating serologic specificity of streptococci isolated in studies of schizophrenia is strikingly shown in table 3. The agglutination titer of the serum of persons having schizophrenia was highly specific, being far greater than by serum of well persons; than for morphologically similar non-hemolytic streptococci isolated in studies of epilepsy; than by negligible or no agglutination of streptococci similarly isolated in studies of chronic encephalitis, respiratory infections, hypertension and enteritis.
The results of the agglutinative action of the serum of persons having abnormal mental symptoms, of well non-contact controls for two composite suspensions of streptococci isolated in studies of schizophrenia, and for one composite suspension each of streptococci isolated in studies of respiratory infections and enteritis, respectively, are shown in table 4. The agglutinative titers of the serum of persons having schizophrenia and the respective groups of persons having related mental conditions for two suspensions of streptococci isolated in studies of schizophrenia were comparable and in all instances far greater than the agglutinative titer of the respective serums of well non-contact persons. The agglutinative titer for streptococci isolated from persons having chronic brain syndromes due to syphilis on contact with schizophrenia was far less than in the schizophrenia and other groups. Agglutination by the respective serums of persons having diverse mental conditions, including schizophrenia, for streptococci isolated in studies of respiratory infections approximated one-third to one-half that of the streptococci isolated in studies of schizophrenia, and agglutination of streptococci isolated in studies of enteritis was negligible.

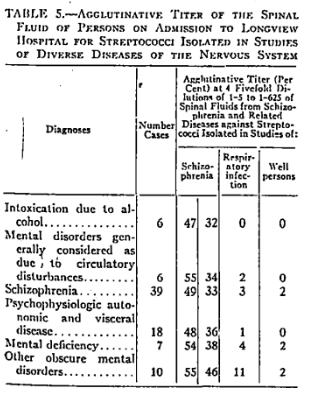
The agglutinative titers of the spinal fluid of persons having schizophrenia and of five other groups having related mental disorders for streptococci isolated in studies of schizophrenia, respiratory infection and well persons are shown in table 5. The average agglutinative titer of the spinal fluids from the five groups of persons having mental disorders not considered as schizophrenia and designated by respective diagnoses was similar to that obtained in the group of 39 persons having schizophrenia, and negligible for streptococci isolated in studies of persons having respiratory infection and of well persons.
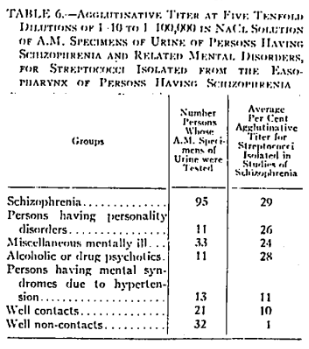
The agglutinative titers of A.M. specimens of urine at pH 7.0, respectively, of persons having schizophrenia and of related mentally ill persons, of well contacts and non-contacts for streptococci isolated from persons having schizophrenia are summarized in table 6. The agglutinative titer of the respective urines for streptococci isolated in studies of schizophrenia, other personality disorders, miscellaneous mentally ill, and alcoholic or drug psychotics was far greater than for streptococci similarly isolated from persons having mental syndromes due to hypertension and from well contacts, and was negligible for streptococci isolated from well non-contacts.
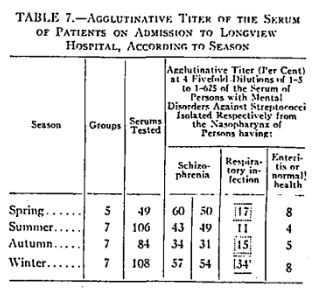
In previous studies it was found that non-hemolytic or alpha type streptococci in nature and in the throats of human beings tend to acquire “neurotropic” properties in summer and “pneumotropic” virulence in winter in temperate climates, and seemingly in consequence, epidemics of poliomyelitis and encephalitis occur predominantly in summer and respiratory infections in winter.9,10,11 On the basis of these results, the agglutinative titer of the serum of persons admitted to Longview Hospital was determined according to season. The scope of study and results obtained are shown in table 7. The agglutinative titer of the serum of persons on admission, chiefly schizophrenics, for streptococci isolated in studies of schizophrenia was least pronounced in autumn, slightly higher in summer, and highest in winter and spring. The agglutinative titer of the serum of patients on admission for streptococci isolated in studies of respiratory infection paralleled roughly the general seasonal incidence of respiratory infections, being least pronounced in summer, somewhat higher in spring and autumn, and highest in winter. Agglutinative titers for streptococci isolated in studies of enteritis and persons in normal health were negligible.
Immunological Studies of Schizophrenia Receiving Chlorpromazine Orally in Treatment
Since chlorpromazine appears to have highly beneficial effects in the treatment of schizophrenia, it was thought that this might be due to its bactericidal action on the streptococcus. Experiments in vitro and in vivo in mice were performed, and it was found that chlorpromazine had no bactericidal action on the streptococcus isolated in schizophrenia and related mental conditions.
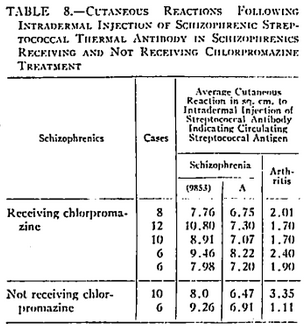
The average size of the erythematous cutaneous reactions to intradermal injection of thermal antibody indicating circulating streptococcal antigen in persons having schizophrenia was comparable in groups of schizophrenics receiving and not receiving chlorpromazine and negligible to injections of antibody prepared from streptococci isolated in studies of arthritis (table 8).
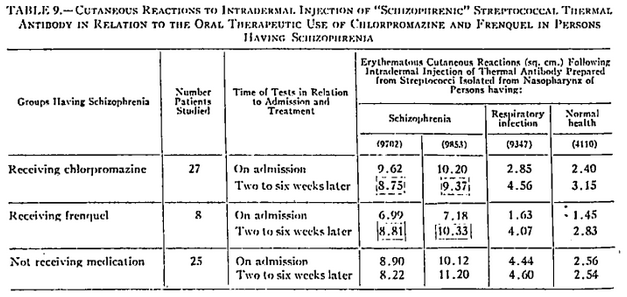
The size of the cutaneous reaction indicating circulating schizophrenic streptococcal antigen from the therapeutic use of chlorpromazine and of frenquel is shown in table 9. The titer indicating circulating streptococcal antigen in schizophrenics that received chlorpromazine was only slightly less following two to six weeks of chlorpromazine medication, and patients receiving frenquel, the antigen titer instead was significantly increased. The cutaneous reactions to intradermal injection of respiratory and “normal” streptococcal thermal antibody indicating antigen were moderately increased in persons receiving chlorpromazine or frenquel. Reactions indicating circulating schizophrenic, respiratory and “normal” streptococcal antigen in the control group not receiving medication were comparable on admission and two to six weeks later. There was no significant change in repeat tests made two to six weeks later in the control group not receiving medication.
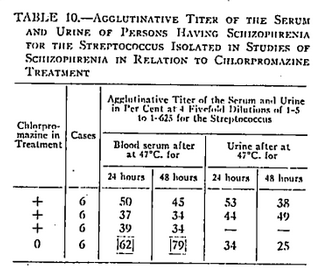
The agglutinative titer of the blood serum of schizophrenics for the streptococcus isolated in studies of schizophrenia (table 10) was found far less in each of three groups of schizophrenics receiving chlorpromazine than in the serum of a comparable group not receiving chlorpromazine. In sharp contrast, the agglutinative liter for the streptococcus in the urine at pH 7.0 of persons receiving chlorpromazine was significantly greater than in the group not receiving chlorpromazine, indicating that the diminished agglutinative titer of the serum in schizophrenics receiving chlorpromazine is due to excessive excretion of antibody in the urine rather than to a diminished synthesis.
The agglutinative titer (table 11) of the blood serum of schizophrenics receiving and not receiving chlorpromazine for the unwashed streptococci isolated from the nasopharynx of schizophrenics receiving chlorpromazine was slightly less (33 per cent) than by the serum of person not receiving chlorpromazine (36 per cent) and far less (42, 53, 49, 56 and 56 per cent), respectively, than for corresponding streptococci isolated from schizophrenics not receiving chlorpromazine (75, 75, 88, 88 per cent). The agglutinative titer of the serum of schizophrenics receiving chlorpromazine for streptococci from schizophrenics not receiving chlorpromazine was significantly less, averaging 54 per cent for the streptococcus 9853 and 70 per cent for the streptococcus 616, than by the serum of persons not receiving chlorpromazine, 64 per cent and 75 per cent, respectively. Moreover, the administration of chlorpromazine caused the streptococcus of schizophrenia to become resistant to the agglutinative action of the blood serum of schizophrenics (55 per cent) as compared with the agglutinative titer (79 per cent) of the serum for the streptococcus as isolated from persons not receiving chlorpromazine.
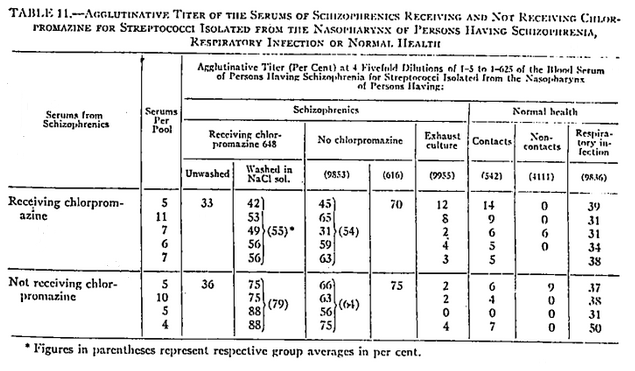
The agglutinative titer of the serum of persons receiving and not receiving chlorpromazine for streptococci isolated in studies of schizophrenia after passage through three exhaust cultures in dextrose broth (9955), for streptococci from contact persons in normal health (542), and well non-contacts (4111) was minimal and not differential. The titer for streptococci isolated in studies of respiratory infection (9836) ranged from one-half to two-fold less than that for strains of streptococci isolated in studies of schizophrenia.
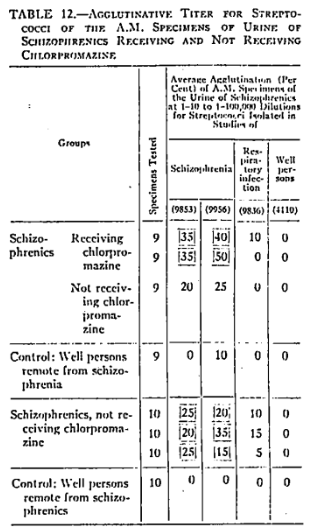
Experiments on the agglutinative titer of A. M. specimens of urine brought to pH 7.0 of schizophrenics receiving and not receiving chlorpromazine for streptococci isolated in studies of schizophrenia, respiratory infections and well persons are summarized in table 12. The agglutinative titer of the urine at pH 7.0 from schizophrenics for streptococci isolated in studies of schizophrenia was significantly higher, indicating excretion of antibody in both of two groups of persons receiving chlorpromazine, than in comparable groups of schizophrenics not receiving chlorpromazine. Agglutination by the A. M. urine of well persons remote from schizophrenics for streptococci isolated in studies of schizophrenia and by the A. M. urine of schizophrenics for streptococci isolated in studies of respiratory infection and well persons was negligible.
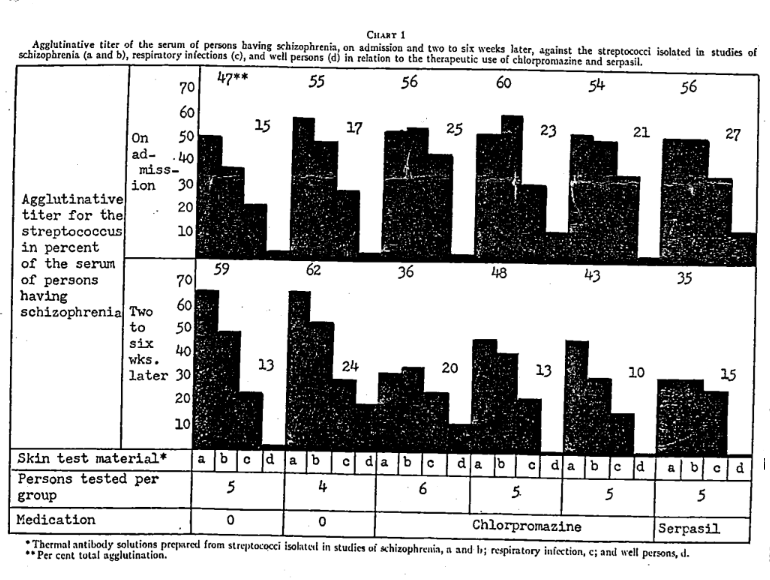
The results of the agglutinative titer of the serum of schizophrenics on admission to the hospital and two to six weeks later, for streptococci isolated in studies of schizophrenia, respiratory infection and in two groups of well persons not receiving medication, in three comparable groups receiving chlorpromazine and one group receiving serpasil are shown graphically in chart 1. The agglutinative titer for streptococci isolated in studies of schizophrenia in the two groups not receiving medication increased moderately during the two to six weeks period, whereas the agglutinative titer in the three groups receiving chlorpromazine and one group receiving serpasil decreased markedly. The agglutinative titer of the serum of persons having schizophrenia for streptococci isolated in studies of respiratory infection not receiving medication did not change while in the three groups receiving chlorpromazine and the one group receiving serpasil, there was a moderate decrease in the agglutinative titer for streptococci isolated in studies of respiratory infection.
Summary and Conclusions
Erythematous cutaneous reactions to intradermal injection of thermal antibody solutions prepared from streptococci, as isolated in studies of schizophrenia, indicating specific circulating streptococcal antigen, have been found highly specific (table 1), and they diminish in size on repeat tests as symptoms abate during immunization with homologous streptococcal vaccine (table 2).
The non-hemolytic or alpha type streptococcus isolated from the end point of growth of nasopharyngeal swabbings of serial dilution cultures in dextrose brain broth and sometimes from the blood in schizophrenia was agglutinated specifically in far higher titer by the blood serum, spinal fluid and urine of persons having schizophrenia or related mental disorders than by the blood serum of well schizophrenic contacts and of persons having mental syndromes due to hypertension (tables 3, 4, 5, 6).
The agglutinative titer of the serum of persons having schizophrenia for the streptococcus isolated from the nasopharynx of schizophrenics did not change seasonally. In sharp contrast, agglutination by the serum of schizophrenics of streptococci isolated in studies of respiratory infection varied seasonally and was maximal in winter months in accord with the general prevalence of respiratory infections (table 1).
The results of previous bacteriological and immunological studies on the etiology of schizophrenia and related mental disorders1,2,3,4 have been corroborated and extended in this further study, indicating that these conditions are due to a specific type of non-hemolytic, neurotropic streptococcal infection or intoxication.
The question remains obscure as to the source of the specific type of neurotropic, toxicogenic streptococcus of schizophrenia whether from extraneous sources, such as milk, water, or air, from contact infection or whether through inherited or inherent conditions in person stricken which supply the very conditions on which the streptococci normally present in the nasopharynx or other foci of infection in human beings acquire specific neurotropic properties.
The streptococcus of schizophrenia has a low, general virulence but is highly neurotropic in that it localizes electively in the brain of persons stricken and in animals on intravenous injection. In keeping with this low, general virulence, the general health is maintained, and stimulation of the formation of antibody is minimal; hence the disease process tends to continue unabated.
The administration of chlorpromazine in chemically effective dosage has little or no effect on the size of the cutaneous reactions to intradermal injection of streptococcal thermal antibody indicating specific circulating antigen while in person receiving frenquel, such reactions are significantly increased (tables 8 and 9).
The agglutinative titer for the streptococcus of the blood serum of schizophrenics receiving chlorpromazine unfortunately has been found far lower and of the urine significantly greater than in comparable schizophrenics not receiving chlorpromazine (tables 10 and 11).
The agglutinative titer of the urine indicating excretion of streptococcal antibody in persons receiving chlorpromazine was far greater than in comparable groups not receiving chlorpromazine and than in well persons remote from schizophrenia (table 12).
The administration of chlorpromazine and serpasil in the treatment of schizophrenics was found to cause a reduction instead of a hoped for increase in the agglutinative titer of the serum of schizophrenics for the streptococcus isolated in studies of schizophrenia (chart 1). The serum of persons receiving such medication had no demonstrable bactericidal action.
The favorable clinical effects from the administration of chlorpromazine in the treatment of schizophrenia and related mental disorders as observed in hospital wards, while sometimes truly remarkable, are sometimes associated with the occurrence of symptoms resembling Parkinson’s disease and leukemia.
It was hoped that the striking beneficial clinical effects might be shown to be due to the elimination of the underlying cause, the toxicogenic neurotropic streptococcus1,2,3,4 rather than to the sedative or tranquilizing action of this new drug chlorpromazine, but this was not realized. In fact, from the immunological standpoint, it is contraindicated, for it does not eliminate the basic cause, the specific neurotropic streptococcus, nor does it neutralize the specific toxicogenic streptococcal antigen. Further attempts to combat schizophrenia and related mental conditions specifically with streptococcal vaccine and thermal antibody are contemplated, and results obtained will be reported in due course.
It is realized how contrary to current psychiatric tenets the concept that schizophrenia and related mental disorders can possibly be due to an infectious process, but the results of bacteriological studies by the special methods used indicate that such is nevertheless the case.
Grateful acknowledgement for the cooperation of Dr. Earl A. Baber, Superintendent, and the Medical Staff of Longview Hospital is hereby made.
References Cited:
- Rosenow, E. C.: “Bacteriologic, etiologic and serologic studies in epilepsy and schizophrenia. II. Effects in animals following inoculation of alpha streptococci.” Postgraduate Med., 3: 124-236, 1948.
- Rosenow, E. C.: “Bacteriologic, etiologic and serologic studies in epilepsy and schizophrenia. I.” Postgraduate Med., 2: 346-357, 1947.
- Rosenow, E. C.: “Bacteriologic, etiologic and serologic studies in epilepsy and schizophrenia. III. Cutaneous reactions to intradermal injection of streptococcal antibody and antigen.” Postgraduate Med., 3: 367-376, 1948.
- Rosenow, E. C.: “Bacteriological studies in idiopathic epilepsy and schizophrenia.” South Dakota J. Med. & Pharm., 5: 243-248, 262-272, 1953.
- Rosenow, E. C.: “Diagnostic cutaneous reactions to intradermal injection of natural and artificial antibody and of antigen prepared from streptococci isolated in studies of diverse diseases.” Ann. Allergy, 6: 485-496, 1948.
- Rosenow, E. C.: “Elective localization of streptococci.” J. A. M. A., 65: 1087-1091, 1913.
- Rosenow, E. C.: “Elective localization of bacteria in diseases of the nervous system.” J. A. M. A., 67: 662-665, 1916.
- Rosenow, E. C.: “Focal infections and elective localization in relation to systemic disease: A review and results of further studies.” Proc. Dental Centenary Celebration, pp. 261-282, March, 1940.
- Rosenow, E. C.: “Seasonal changes in the cataphoretic velocity and virulence of streptococci, as isolated from well persons, and persons having epidemic or other diseases, and from raw milk.” J. Infect. Dis., 53: 1-11, 1933.
- Rosenow, E. C.: “Seasonal changes of streptococci isolated in studies of poliomyelitis, encephalitis and respiratory infection.” Postgraduate Med., 7: 117-123, 1950.
- Rosenow, E. C.: “Radiant energy as a probable cause of seasonal changes in specificity of non-hemolytic streptococci. Preliminary report.” Postgraduate Med., 8: 290-292, 1950.