
Access to all articles, new health classes, discounts in our store, and more!
Bacteriologic Studies by New Methods of a Major Epidemic of Poliomyelitis, 1947
Presented at a meeting of the Ohio Branch of the Society of American Bacteriologists, Columbus, Ohio, October 25, 1947. Published in The Journal-Lancet, Minneapolis, February, 1949, Vol. LXIX, No. 2, pp. 47-55.
* * *
The epidemic of poliomyelitis studied occurred during the summer of 1947, and it was the fourth annual epidemic in a large city in the Midwestern section of the United States. Two hundred and forty-six frank cases, and a much larger number of suspected cases, occurred among the population of more than 350,000 inhabitants in 1947; fifty-nine cases in 1946, forty cases in 1945 and one hundred and twenty-three cases in 1944. The 1947 epidemic was one of only three sizeable outbreaks in the United States one year after the severe and extremely widespread epidemic of poliomyelitis of 1946. The reasons for this abnormal incidence of poliomyelitis had remained obscure. Various possible causes, such as flies and mosquitoes, sewage, the polluted water of an abandoned canal, swimming pools and the “smudged” atmosphere, were considered. The water and milk supplies were rigidly tested and found satisfactory, according to present day standards. The epidemic was characterized by a high incidence among the general population, especially among children, of a peculiar, relatively mild infection of the throat associated with fever for several days. The symptoms referable to the upper respiratory tract and to the central nervous system were similar among all persons ill, regardless of whether typical poliomyelitis did or did not develop. There was a high incidence of abortive or nonparalytic cases. The mortality rate was low, despite a high incidence of the bulbar type of the disease. The range in age incidence was wide; infants, young and older children and adults being affected. The range of involvement of muscles in different persons also was wide but, in agreement with the low mortality rate, complete paralysis of muscle groups was uncommon.a
From epidemiologic considerations,1 this epidemic should not have occurred because of the previous high annual incidence of the disease. A special reason, therefore, seemed to be operative. By the use of special and new methods I attempted to determine the reason for this abnormally high incidence of poliomyelitis.
Methods of Study
Serial dilution cultures2 were made in freshly prepared dextrose-brain broth, of nasopharyngeal swabbings and of the water and milk supplies. The dextrose-brain broth, as used, was prepared by adding pieces of fresh calf brain, approximately one part by volume, to six or seven parts of 0.2 per cent dextrose broth before autoclaving. The finished medium was placed in 15 ml. amounts in test tubes (6″ x 5/8″). Blood-agar plates were inoculated with nasopharyngeal swabbings and with the milk. Nasopharyngeal swabbings were made from behind and above the soft palate, without touching the tongue, using cotton wrapped aluminum wire bent to a suitable angle. The adherent material on the swabs was washed off in 2 ml. of solution of sodium chloride. Of this washing, 0.15 ml. was inoculated into the first tube of a series of five tubes of dextrose-brain broth; 1.5 ml. of water containing the sedimented organisms from 15 ml. of centrifuged water representing samplings of water supplies, and 1.5 ml. of each sample of milk were likewise added to the first tube in each series of five tubes of dextrose-brain broth. The samples of milk had been kept well refrigerated with ice until the cultures were made, which was usually within twenty-four hours after pasteurization. After thorough mixing with a sterile 1 ml. pipette, 0.15 ml. was transferred from tube to tube in each series. One pipette was used in each series to mix and transfer the respective materials from tube to tube. The dilutions of the nasopharyngeal washings ranged from 1:100 to 1:10,000,000,000; the dilutions of the milk ranged from 1:10 to 1:1,000,000,000 and of the water from 1:1 to 1:100,000,000. In making serial dilutions of sodium chloride solution suspensions or broth cultures containing specifically virulent streptococci, without changing pipettes, it was found that dilution of viable organisms often was far less than that of the liquid menstruum and that serial dilutions in the highly favorable medium, dextrose-brain broth, served to separate the pathogens from saprophytes, just as if the pathogens adhered to the surfaces of the pipette and the saprophytes did not.
The streptococcus used for inoculation of animals, for preparation of very dense suspensions of partially dehydrated streptococci in glycerol (2 parts) and saturated sodium chloride solution (1 part) for agglutination and precipitation studies and for the preparation of thermal antibody and of antigen, were obtained either from the end point of growth, usually in the third, fourth or fifth serial dilution, or from the first, second or third rapidly repeated subculture in dextrose-brain broth.
Young white mice of the Swiss type, weighing 15 to 18 gms., were inoculated routinely, under ether anesthesia, intracerebrally with 0.03 ml. or intraperitoneally with 1 ml., of 10:1 suspensions in solution of sodium chloride of the streptococcus from the nasopharynges of persons ill and from the milk, before and after from one to four pasteurizations in milk and after one or two animal passages.
The resistance to heat of the streptococcus isolated from nasopharynx and from the pasteurized milk and other sources was determined by subjecting suspensions of the respective streptococci in autoclaved milk contained in 15 ml. amounts in rubbed capped bottles, to 145° F. or 158° F. for 30 minutes. The temperature inside of control vials containing milk was checked with certified thermometers. Sterility cultures were made in dextrose-brain broth.
The agglutinating action of normal and convalescent serum was determined in three five-fold dilutions of 1:10 to 1:250. That of “natural” antibody present in the serum of immunized horses and of thermal antibody prepared in vitro with streptococci isolated, respectively, in studies of poliomyelitis, arthritis and epilepsy was determined at four five-fold dilutions of 1:10 to 1:1,250. Two-tenths ml. of the respective dilutions of serums or thermal antibody, and 0.2 ml. of the respective suspensions containing approximately 6,000,000,000 streptococci per ml. were added to test tubes measuring 3″x3/8″. The mixtures were thoroughly shaken and then incubated at 45 to 48° C. for eighteen hours. Readings were made under the edge of a shaded 100-watt light bulb against a non-reflecting black velvet cloth in a dark room. For the sake of brevity and clarity, the agglutinative titers in tables and text are given in per cent of the total possible. Maximal agglutination of 4 plus for each dilution was considered 100 per cent. The percentage was obtained by dividing the observed degree of agglutination by the total possible (12 for the three dilutions and 16 for the four five-fold dilutions).
In studies on the production of streptococcal antibodies in vitro, it has been found that as the bacteria disintegrate in sodium chloride solution suspensions, on application of heat in the autoclave, toxic components are destroyed, the remnants of organisms become sharply agglutinated and brownish in color and substances resembling antibodies suitable for diagnostic tests of specific antigen in skin or blood become demonstrable in the supernatant of the suspension.3,4
Sodium chloride solution suspensions of streptococci (10,000,000,000 organisms per ml.) which had been isolated in studies of poliomyelitis, and other diseases, were autoclaved for ninety-six hours and heated at 65° C. for one hour, respectively. To these suspensions phenol was added to equal 0.2 per cent. The bacteria-free supernatant of the autoclaved and heated suspensions represented antibody and antigen, respectively, and were injected intradermally for the detection of specific antigen and antibody in the skin or blood of persons ill, of well contacts and of noncontacts. Solutions similarly prepared from streptococci unrelated to poliomyelitis and NaCl solution containing 0.2 per cent phenol were injected as controls. Immediate erythematous reactions occurred after intradermal injection of 0.03 ml. of the supernatant solution containing antibody, provided antigen specifically related to the streptococcus from which the antibody was prepared was present in skin or blood. A similar, although usually a less intensive, erythema occurred immediately surrounding the site of injection of the antigen, provided antibody specifically related to the streptococcus was present in the skin or blood. In studies to be reported elsewhere of persons suffering from diverse diseases associated with specific types of streptococci, including poliomyelitis, erythematous reactions, indicating streptococcal antigen in skin or blood, that occurred after intradermal injection of thermal and natural antibody ran closely parallel and reactions obtained on injection of solutions of respective antigen and specific polysaccharide also ran closely parallel.
Results of Cultures of the Water Supply
Serial dilution cultures in dextrose-brain broth were made of 10:1 suspensions of the centrifuged sediment of forty samplings of water. Fourteen of these samplings were collected for me by the Water Department from widely separated parts of the city from outlets routinely tested. Seven were collected by the Department of Health in homes where poliomyelitis had recently occurred. Four samplings were of polluted water from a canal traversing the city and samplings were obtained from four swimming pools. I collected eleven samples from water supplies of buildings equipped with flush types of toilet valves, four at the inlet and seven within the buildings. Streptococci were isolated from but one of the fourteen samples representing the city supply routinely tested. This culture proved nonvirulent, was killed by standard pasteurization in milk and was not agglutinated by convalescent serum or by the poliomyelitis antistreptococcic serum. Streptococci grew in mixture with gram-negative, gas-forming bacilli in but one of the four samples of water from the canal and in four of the seven samples from within buildings equipped with the flush type of toilets. Thus, of the forty samples cultured, a streptococcus was isolated in pure culture from but one sample. Streptococci grew in mixture with other bacteria in cultures from five and streptococci did not grow in cultures of thirty-four of the forty samplings.
Results of A Study of the Milk Supply
The results of a microscopic examination and cultural study of the milk supply by making serial dilutions in dextrose-brain broth, according to the “flash” or “holding” methods of pasteurization, and of raw milk are summarized in Table 1. It will be seen that the number of streptococci found on microscopic examination of stained films and the incidence of isolations were uniformly higher, especially isolations in pure culture, from specimens that had been pasteurized by the “flash” method than by the “holding” method. In most instances, streptococci grew at extremely high dilutions of the milk in the serial dilution cultures in dextrose-brain broth, indicating the presence of large numbers of viable streptococci. Altogether, mixed or pure cultures of the streptococci grew in serial dilution cultures in fifty-four instances and pure cultures were obtained in twenty-two instances (37 per cent) of the sixty samples of thirtytwo brands cultured, representing virtually the entire milk supply of the city. Only relatively small numbers of streptococci grew on blood-agar plates.
Table 1: Summary of a Bacteriologic Study of the Milk Supply
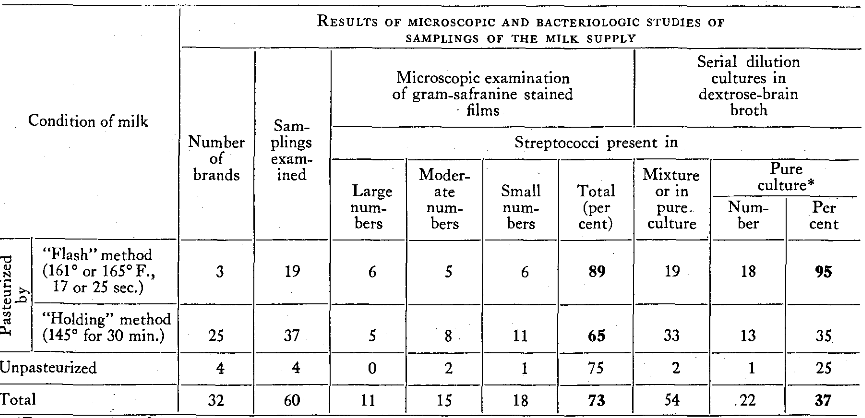
*From end point of growth.
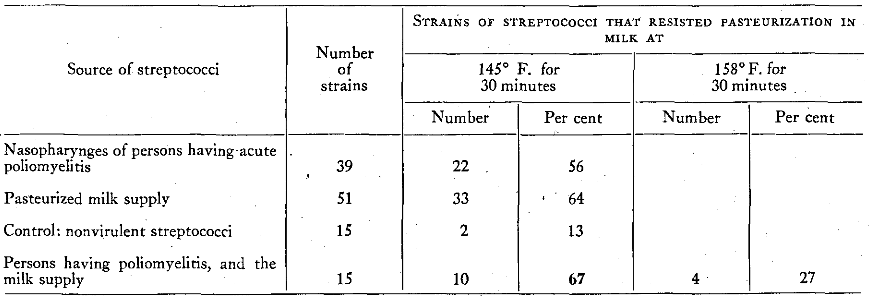
The results of a study of the heat resistance in milk of the streptococci isolated from the nasopharynges of persons having poliomyelitis and from the milk supply are summarized in Table 2. The high incidence of isolations of the streptococcus, alike from nasopharynx and from the milk supply, and the low incidence of isolations of control strains after heating to 145° F. for thirty minutes and the low incidence of isolation of the specific strains after heating to 154° F. for thirty minutes are well shown and are in accord with previous studies.5 The four of fifteen specific strains that resisted pasteurization at 154 ° F. for thirty minutes had resisted three previous pasteurizations at 145 ° F. Each of these four strains produced flaccid paralysis in mice on isolation after commercial pasteurization by the “flash” method, and all proved nonvirulent after three additional pasteurization including pasteurization at 154° F. for thirty minutes.
Table 2: Resistance of Pasteurization in Milk of Streptococci Isolated from Nasopharynges of Persons Having Poliomyelitis, and from the Milk Supply
Results of Experiments in Mice
The results following inoculation of a large number of mice with the streptococcus isolated from the nasopharynges of persons having acute poliomyelitis, from the milk supply of the epidemic under study, and from outdoor air during September and early October, 1947, representing five Middle West states, in contrast to those obtained in mice similarly inoculated with streptococci isolated from the nasopharynges of persons ill with diverse diseases remote from epidemic poliomyelitis, are summarized in Table 3. The strains isolated from persons having poliomyelitis, from the milk supply and, to a lesser but significant degree, from the outdoor air in September caused a high incidence of paralysis, usually flaccid in type, which was not the case following identical inoculations of streptococci from the control groups. In sharp contrast, streptococci isolated in studies of idiopathic epilepsy caused a very high incidence of spasms, often associated with generalized convulsions, and streptococci similarly isolated from nasopharynges of persons suffering from epidemic respiratory infections caused a high incidence of lesions of lungs. The mortality rate and isolations of streptococci from the brains of animals that succumbed, while significant, were not as distinctive as the symptoms and lesions that developed after inoculation of both the test and the control strains.
Table 3: Results in Mice Inoculated with Streptococci Isolated from the Nasopharynges of Persons Having Poliomyelitis and from the Milk Supply of a Major Epidemic, in Contrast to Results Obtained with Streptococci from Sources Other than Poliomyelitis
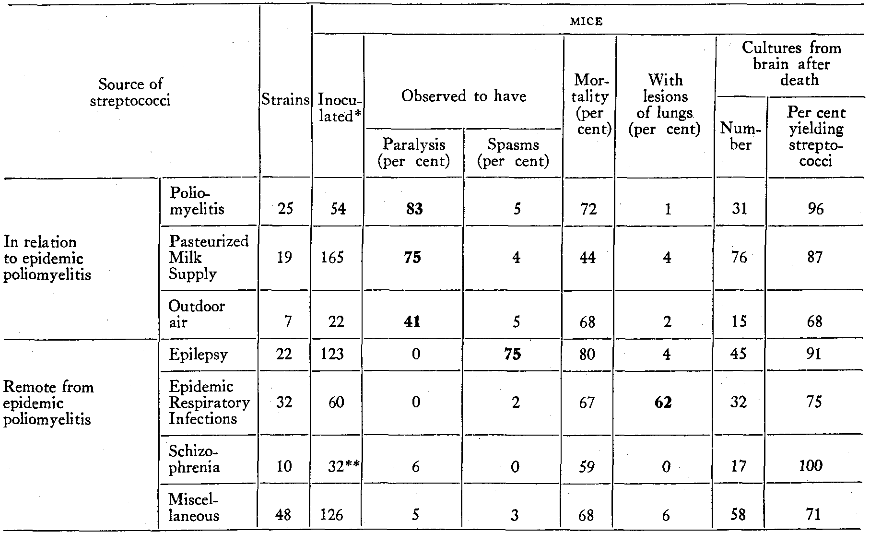
*About one-third of the animals in the first five groups were inoculated intraperitoneally. All others were inoculated intracerebrally.
**Twenty of the 32 mice became extremely excitable.
Results of Agglutination Tests
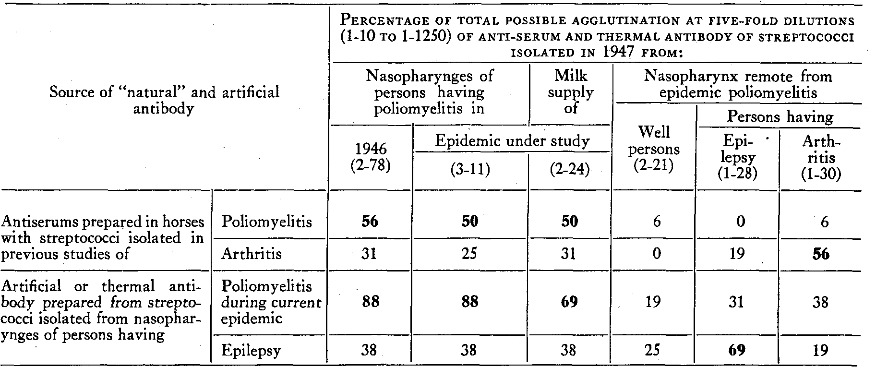
The agglutinative titer of the serum of horses prepared, respectively, with streptococci isolated in previous studies of poliomyelitis and arthritis, and that of thermal antibody prepared with streptococci isolated from the nasopharynges of persons having poliomyelitis in the epidemic under study, and of persons having epilepsy remote from poliomyelitis are summarized in Table 4. The much higher percentage of agglutination by the homologous natural and thermal antibody than that by heterologous antibody is strikingly shown.
Table 4: Agglutinative Titer of Antiserum Prepared in Horses and Thermal Antibody Prepared in Vitro with Streptococci Isolated in Studies of Poliomyelitis, Arthritis and Epilepsy for the Respective Streptococci
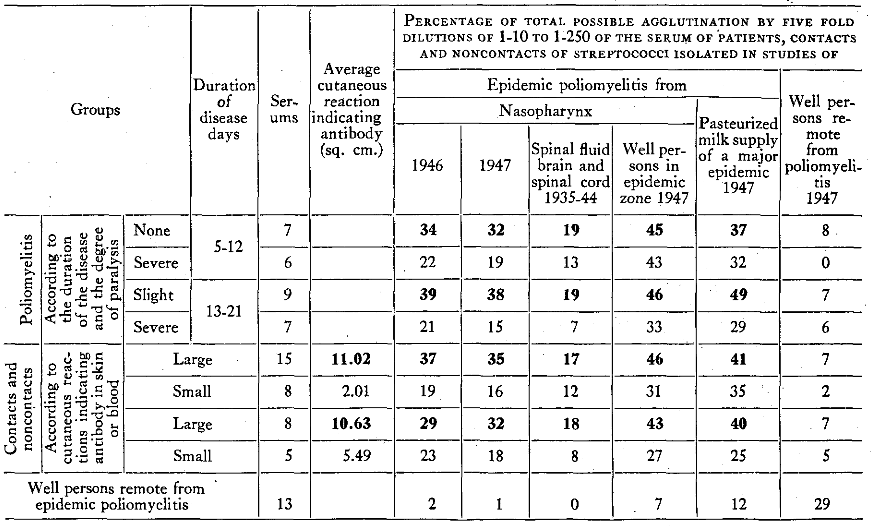
The agglutinative titer of serums from persons was determined separately. A summary of the results of the different groups is shown in Table 5. It will be seen that the average percentage of total possible agglutination by the serums from persons having nonparalytic poliomyelitis was uniformly higher, and often much higher, both at five to twelve days and thirteen to twenty-one days after onset of the disease than the serums from persons of the same age having paralytic poliomyelitis. Moreover, there was a striking parallelism between agglutinative titer of the serums and antibody titer in skin or blood as determined by intradermal injection of specific streptococcal antigen. The agglutinative titer of the serum of well persons remote from the epidemic was always much lower than that of the serum of persons convalescing from mild poliomyelitis.
Table 5: Agglutinative Titer of the Serum of Persons Suffering from Poliomyelitis for Streptococci Isolated in Studies of Poliomyelitis in Relation to the Titer of Streptococcic Antibody in Skin or Blood, Duration of the Disease and Degree of Paralysis
Results of Cutaneous Tests
The results of erythematous reactions to intradermal injection of thermal antibody and of antigen are summarized in Table 6. It will be seen that the average reactions in square centimeters and percentage of reactions 5 sq. cm. or more, indicating specific streptococcal antigen in skin or blood, was greatest among persons suffering from paralytic poliomyelitis (14.57 sq. cm.), next greatest in non-paralytics (13.90 sq. cm.); greater in persons that had not been exposed to poliomyelitis in 1946 (12.34 sq. cm. and 12.50 sq. cm.) than in persons that had been exposed in 1946 (10.08 sq. cm.) and slightly less in contacts and non-contacts (9.71 sq. cm.). In sharp contrast, reactions to antigen indicating specific streptococcal antibody in skin or blood were least among persons having paralytic poliomyelitis (4.06 sq. cm.), somewhat greater in non-paralytics (6.35 sq. cm.), still greater among well persons living in widely separated homes but not directly exposed to poliomyelitis in 1946 (8.08 sq. cm.) and well contacts and non-contacts (8.91 sq. cm.); reactions indicating antibody were greater among well physicians and nurses that had been exposed to poliomyelitis in 1946 (9.12 sq. cm.) than in those not so exposed (4.58 sq. cm.). (See also Table 7). Reactions indicating antigen and antibody were far lower for the control group than for groups living in the epidemic under study. Reactions to injections of control antibody prepared from streptococci isolated from nasopharynges of persons suffering from respiratory infections and of well persons remote from poliomyelitis were uniformly far less than to antibody prepared from streptococci isolated in studies of poliomyelitis. However, reactions of persons ill, of contacts and non-contacts and other well persons in the epidemic under study, where mild infection of the throat was common, were significantly greater to antibody prepared from streptococci isolated in studies of respiratory infection than to antibody prepared from streptococci isolated from the nasopharynges of well persons.
Table 6: Erythematous Reactions of Persons with Poliomyelitis and of Well Contacts and Noncontacts During the Epidemic of Poliomyelitis in Akron, Ohio (1947), Following Intradermal Injection of Streptococcic Thermal Antibody and Streptococcic Antigen
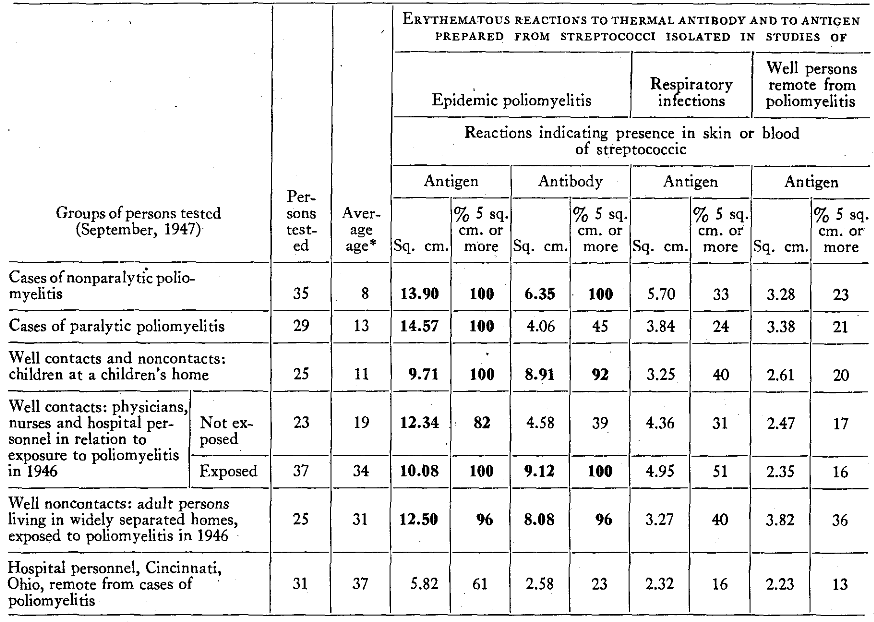
*Years
Since the streptococcus isolated from the milk supply was agglutinated in a manner similar to the streptococcus isolated from persons suffering from poliomyelitis, indicating antigenic identity, then thermal antibody prepared from it should incite cutaneous reactions similar to those that occurred after injection of antibody prepared from the streptococcus isolated from the nasopharynges of persons having acute poliomyelitis. This proved to be so, as shown in Table 7. Moreover, similar reaction to intradermal injection of antibody prepared from the streptococcus isolated from the milk supply, from the nasopharynges of persons having poliomyelitis in the epidemic under study and in an epidemic elsewhere were obtained in persons who had contracted poliomyelitis and in well contacts in other mild outbreaks. Minimal reactions among non-contacts remote from poliomyelitis, tested as controls, also ran closely parallel. It is well shown too that there was a much higher antibody titer among persons with little or no paralysis (8.01 sq. cm.) than among persons severely paralyzed (2.2 sq. cm.).
Table 7: Erythematous Reaction to Intradermal Injection of Thermal Antibody and to Antigen prepared from Streptococci Isolated from the Nasopharynges of Persons Ill with Poliomyelitis, and from the Pasteurized Milk Supply in the Epidemic of Poliomyelitis under Study
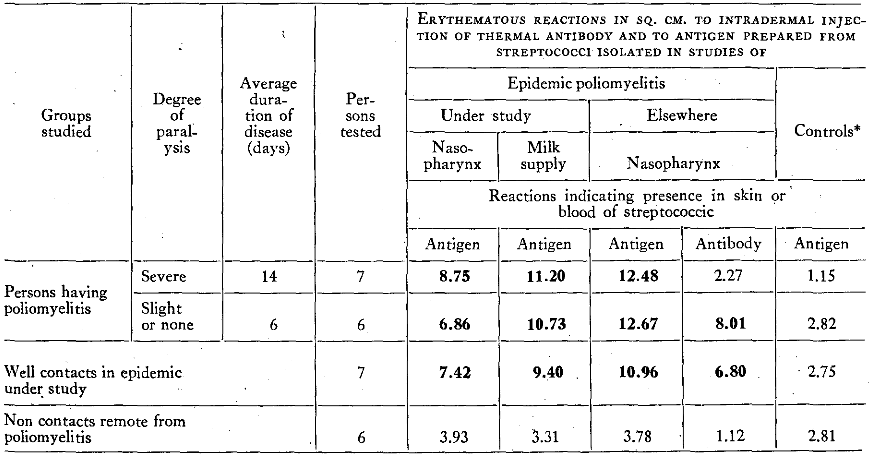
*Well persons remote from poliomyelitis
On the basis of these findings and the fact that antigen and antibody titer of skin or blood were uniformly greater among persons residing in the epidemic under study than occurred in other epidemics (in 1946 and 1947, to be reported elsewhere), it was decided to study the effect of the ingestion of the milk by well persons remote from the epidemic.
Experimental Induction of Specific Cutaneous Reactions by Ingestion of the Contaminated Milk
One of the most used brands of homogenized milk from the epidemic zone, which was pasteurized by the “flash” method and from which the specific type of streptococcus was isolated, as well as from three previous samplings, was taken properly refrigerated to Cincinnati. This milk was ingested in parallel manner with a local brand of milk pasteurized at 145° F. for thirty minutes, from which the specific type of streptococcus was not isolable, by volunteer persons who did not react positively to intradermal tests. The conditions of the tests and the results obtained are shown in Figure 1.
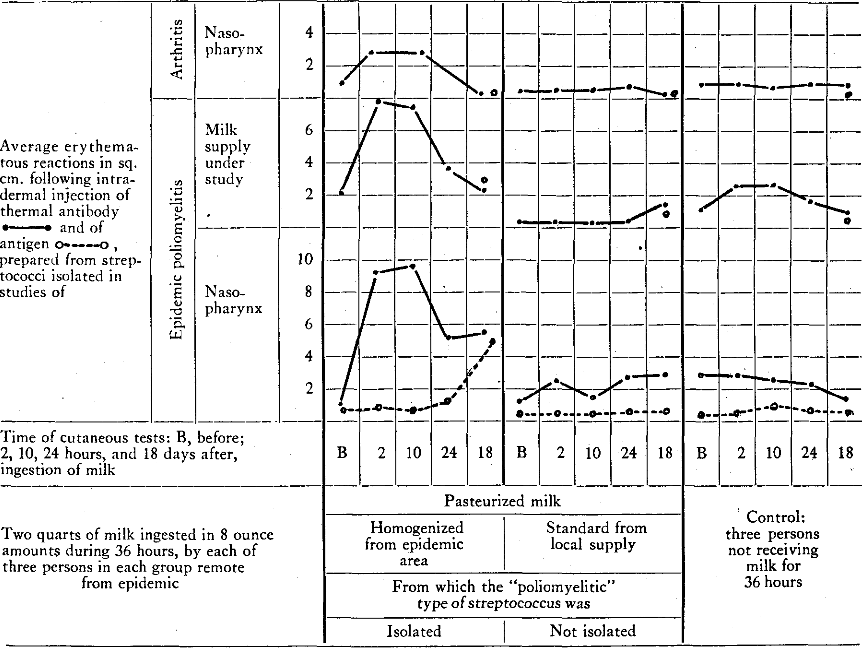
Figure 1 – Cutaneous Reactions Indicating Absence of “Poliomyelitic” Streptococcal Antigen and Antibody in Skin or Blood of Persons Before, and Their Presence After, Ingestion of Pasteurized Milk from Which the “Poliomyelitic” Streptococcus was Isolated
The cutaneous reaction to thermal antibody prepared alike from the streptococcus isolated from nasopharynges of persons suffering from poliomyelitis and from the milk supply of the epidemic under study, indicating specific streptococcic antigen in skin or blood, had increased sharply in each person in two and ten hours after ingestion of two quarts of the milk during thirty-six hours. The reaction to repeat cutaneous tests had diminished in twenty-four hours for both antibody solutions. After eighteen days, the reaction to antibody prepared from the streptococcus isolated from the milk was negative whereas that to antibody prepared from the streptococcus isolated from nasopharynx was still elevated. Antibody to both strains had developed in eighteen days. In sharp contrast, there was no significant increase in antigen or antibody, measurable by intradermal injection of antibody and antigen prepared respectively, from streptococci isolated in studies of arthritis remote from poliomyelitis, in the group which ingested the milk from the epidemic under study. Moreover, no change in “poliomyelitic” or “arthritic” antigen or antibody content of the skin or blood occurred in the control group that ingested the control pasteurized milk from which the specific type of streptococcus was not isolable, or in the additional controls tested in parallel manner who did not receive milk during thirty-six hours.
Summary and Comments
The results of a bacteriologic study, made by special and new methods, of a major epidemic, the fourth annual epidemic, of poliomyelitis in a large city are reported. A specific type of streptococcus, similar to the streptococcus isolated consistently in previous studies,6,7 was isolated from the nasopharynges of all persons studied in whom poliomyelitis had developed and from the pasteurized milk supply in high incidence. Cutaneous reactions, indicating specific streptococcal antigen and antibody in skin or blood, and hence the presence of a specific type of streptococcal infection, were demonstrated consistently among persons suffering from abortive and paralytic poliomyelitis and among well contacts and non-contacts.
The cutaneous reactions, indicating specific streptococcal antigen and antibody, of virtually all persons tested were so much greater, especially reactions indicating antibody, than those obtained in studies of other epidemics and of sporadic cases as to suggest a source, or sources, of the streptococcus and perhaps virus other than, or in addition to, contact infection. Since streptococci having certain respective specific properties had been isolated previously from persons ill6,7 and from unpotable water and from water and milk supplies5,8 during epidemics of poliomyelitis, encephalitis and respiratory infections, since the streptococci thus isolated failed to grow in the aerobic mediums now universally used for the control of the bacterial content of milk supplies, and since they often resisted pasteurization at 145° F. for thirty minutes,5 the water and milk supplies-even the pasteurized milk chiefly used-were considered as possible sources of infection. On the basis of these facts and the high incidence of the unusual type of infection of the throat in children, a bacteriologic study of the water and milk supplies was made by the special and new methods.
The specific type of streptococcus was not isolable from any of the forty samplings of water, including the drinking supply, from the polluted water of the canal and from swimming pools. Streptococci grew or were isolated from fifty-two of fifty-six samplings of pasteurized milk and from two of four samplings of raw milk. Only relatively small numbers of streptococci grew on aerobic blood-agar plates. The bacterial count of the milk supply adequately tested by the health departments using the prescribed methods was well within the prescribed limits. However, mixed and pure cultures of the streptococcus grew in high, and often in extremely high, serial dilutions in dextrose-brain broth, indicating the presence of large, and often of extremely large, numbers of viable partial tension streptococci. This was especially true of samplings from milk that had been pasteurized by the “flash” method and which constituted the major supply of the city. The streptococcus isolated from the milk resembled the streptococcus isolated from the nasopharynges of persons in whom poliomyelitis had developed in the epidemic under study and elsewhere, in cultural requirements, morphology, staining reactions, in resistance to pasteurization, in serologic properties and in virulence. Strains from both sources were agglutinated specifically by convalescent serum, by the serum of horses that had been immunized previously with the streptococcus isolated in studies of poliomyelitis, and by thermal antibody prepared from the streptococcus isolated from the nasopharynges of persons ill in the epidemic under study. The streptococcus from both nasopharynx and milk produced flaccid paralysis in high incidence in mice following intracerebral or intraperitoneal inoculation and were isolated in pure culture from the brains of mice that succumbed.
The production in mice of the all-important symptom of poliomyelitis, flaccid paralysis, associated with edema, hemorrhage and degeneration of ganglion cells in the anterior horns of the spinal cord with the streptococcus isolated from persons ill and the milk supply is considered of fundamental importance even though some of the clinical and histological findings as seen in epidemic poliomyelitis in humans and experimental “virus” poliomyelitis in monkeys were lacking.
Cutaneous reactions to thermal antibody prepared from the streptococcus isolated from the milk and from the nasopharynges of persons in whom poliomyelitis had developed ran closely parallel in persons having poliomyelitis, in contacts and in non-contacts. Ingestion of the contaminated milk caused skin test negative persons to become skin test positive to thermal antibody and to antigen, indicating respectively, the absorption of specific streptococcal antigen, the formation of specific antibody and the source of the abnormally high titer of antigen and antibody in persons ill and in well persons of the population.
The close parallelism between antibody titer in skin or blood, as determined by intradermal injection of antigen, and antibody titer in the serum as determined by agglutination tests, the presence of antigen in skin or blood in highest titer and antibody in lowest titer in paralytic poliomyelitis, and vice versa in well persons, further indicate causal relationship of the streptococcus or antigenic identity of the streptococcus and the virus.
The low antibody titer in paralytic poliomyelitis which was found in this study, and also in similar studies made elsewhere in 1947 and last year during the severe epidemic, is in striking accord with the low viral neutralizing titer in the serum of persons who had paralytic poliomyelitis, reported by Jensen.9 Whether this striking lack of antibody formation in paralytic poliomyelitis is expressive of familial or “autarceologic” susceptibility, as suggested by Aycock10 and as emphasized by Anderson,1 or whether due to a particularly severe infection by the streptococcus or virus is not clear.
The data adduced in this study indicate that the streptococcus isolated alike from the nasopharynges of persons ill and from the milk supply was causative and perhaps indirectly a source of the virus as the infection by the streptococcus occurred, and that ingestion of the milk from which the streptococcus was isolated in such high incidence and in such large numbers played an important role in pathogenesis. On the basis of these and previous studies in which the specific type of the streptococcus was isolated consistently by my methods from milk obtained in a sterile manner from cows on farms where polio occurred from composite samples of milk and cream in epidemics,5,6,7 and the fact that one epidemic traced to a milk supply came to an abrupt end by discontinuance of the use of the contaminated milk,5 it was strongly urged that the milk supply of the city be pasteurized at a temperature shown to be adequate to kill the resistant specific type of streptococcus, and that the methods herein used be adopted for the isolation of specific types of streptococci and for the bacteriologic control of milk supplies. The type of streptococcus isolated from the nasopharynges of persons and from the milk in this study has been isolated consistently in previous studies, by the special methods employed, from poliomyelitis virus, even from filtrates of the virus,2,11 from the cerebrospinal fluid in the very early stages of the spontaneous disease and as fever appears in monkeys following intracerebral inoculation of virulent virus, and from the spinal cord after death in epidemic and experimental poliomyelitis.11 Moreover, filtrable transmissible agents resembling poliomyelitic virus have been produced experimentally from neurotropic streptococci isolated in studies of poliomyelitis and from sources wholly remote from poliomyelitis.12 It is suggested that the primary infection in poliomyelitis is streptococcal and that as this occurs a virus phase of the streptococcus may develop. The streptococcus, on the basis of present knowledge, is considered to be the large, cultivable, toxigenic, highly antigenic phase of the small, filtrable, highly invasive, but relatively nonantigenic, virus.
The studies on the virus made now for nearly 40 years have been so alluring that the solution of the problem has quite naturally been sought from this standpoint, almost to the exclusion of forthright bacteriologic studies. It is hoped that the results, reported herewith, will lead to a broader approach at the solution of this problem than that hitherto employed, to a study of both the streptococcus and the virus.
Grateful acknowledgment is hereby made for the cooperation of superintendents of hospitals, nurses and children’s homes; and directors of city and county health and water departments which made this study possible.
References Cited:
- Anderson, G. W.: Epidemiology of Poliomyelitis. Journal-Lancet, Minneapolis, 67:10-13, 1947.
- Rosenow, E. C.: Isolation of Bacteria from Virus and Phage by a Serial Dilution Method. Path. 26:371-377, 1938.
- Rosenow, E. C.: Production in Vitro of Substances Resembling Antibodies from Bacteria. Infect. Dis. 76:163-178, 1945.
- Rosenow, E. C.: Studies on the Nature of Antibodies Produced in vitro from Bacteria with Hydrogen Peroxide and Heat. Immunol. 55:219-232, 1947.
- Rosenow, E. C.: Isolation from Milk Supplies of Specific Types of Green-Producing (alpha) Streptococci and Their Thermal Death Point in Milk. Med. 27:550-556, 1944.
- Rosenow, E. C.: An Institutional Outbreak of Poliomyelitis Apparently Due to a Streptococcus in Milk. Infect. Dis. 50:377-425, 1932.
- Rosenow, E. C., Rozendaal, H. M., and Thorsness, E.T.: Acute Poliomyelitis: Studies of Streptococci Isolated from Throats and Raw Milk in Relation to One Epidemic. Pediatrics 2:568-593, 1933.
- Rosenow, E. C.: Specific Types of Alpha Streptococci and Streptococcal Antigen in Unpotable Water and Water Supplies. J. Clin. Path. 15:513-528, 1945.
- Jensen, C.: The 1934 Epidemic in Denmark. Roy. Soc. Med. (Sec. Path.) 28:13-32, 1935.
- Aycock, W. L.: Nature of Autarceologic Susceptibility to Poliomyelitis. Jour. Public Health 27:575-582, 1937.
- Rosenow, E. C.: Poliomyelitis. The Relation of Neurotropic Streptococci to Epidemic and Experimental Poliomyelitis and Poliomyelitic Virus. Diagnostic Serologic Tests and Serum Treatment. The International Bulletin, New York, A-44, 1-87, 1944.
- Rosenow, E. C.: Studies on the Virus Nature of an Infectious Agent Obtained from Four Strains of “Neurotropic” Alpha Streptococci. Nerv. & Ment. Dis. 100:229-262 (Sept.), 1944.