
Access to all articles, new health classes, discounts in our store, and more!
Are Endamebae Important Factors in the Etiology of Pyorrhea Alveolaris?
Published in Journal of the National Dental Association, May 1915, Vol. 2, No. 2.
* * *
As directed, by the Scientific Foundation and Research Commission, this department has been making special investigations to establish methods for the identification and differentiation of pathogenic and non-pathogenic organisms of the mouth and its lesions. This is a preliminary and partial report, made at this time to assist those who are with difficulty, taking up the study of endamebae, to outline some of the as yet unanswered problems relating thereto and to suggest some lines of parallel work for the co-operation of those of the profession who may be in a position to assist in their solution.
The problem that is most vitally concerning the dental profession at this moment is, apparently, the relation of endamebic infection to so called pyorrhea alveolaris and the possibility of its cure with emetine. (1) The microscopic study is one essential line of approach and in order to provide a correct conception of what may be seen in the microscopic field, we will first review the characteristics of the living organisms. We should see and study reproductions of them which reveal their normal individualities, including not only their physical forms but also, their natural movements in life’s processes. There is as much difference in the appearance of some organisms, when living normally and when dried and stained, as in the swimming swan or the bounding deer when seen at home in their haunts or when their skins are hanging in a tannery. We can learn to identify the swan or the deer by their skins in the tannery or the organisms of the mouth in the stained slide, but we have not learned to know them and their individualities, manners and habits until we have become familiar with them in their natural environments. We have found the motion pictures to be by far the best means for studying the habits of mouth organisms, for by this method we can make them do the same act over and over, with normal rapidity or with any desired slowness. While our studies have included various organisms of the mouth, we will present here chiefly studies of the normal vital motions of the endamebae and their relations to pyorrhea alveolaris. Unfortunately, it is impossible to adequately illustrate in still pictures what is shown in motion pictures, however, a good idea can be gotten by taking out pictures from the series at definite intervals. As indicated, nearly all of these shown are selected at one-half second intervals of time, where the pictures are taken 16 to 20 per minute. In these shown, however, we have enlarged the organisms to nearly fill the field, especially to illustrate their physical characteristics and their successive rhythmic, modulating variations which as seen, are very different with different types and species of endamebae. We find that the species predominating may vary with the location and the time of the year, in the same month under certain conditions, as indicated later. Fig. 1 shows a typical endameba (1) buccalis of Prowazek (1904) (2) which is probably the same as endameba buccalis of Sternberg (1862), (3) the ameba dentalis of Grasse (1879), (4) ameba gingivallis of Gros (1849), (5) and the ameba of Flexner (1892) (6). Chiavaro (7) was the first to recognize its encysted or spore forms. It is present in varying forms in the human mouth under varying conditions referred to later. Its size varies from 6 to 30 microns (one four thousandth to one eight hundredth of an inch in diameter.) When active it throws out a few lobose pseudopods, which have a definite independent tho consecutive movement which is clearly shown in these unstained illustrations from life. This Fig. 1 shows the successive changes that have occurred at the end of each half second for twelve consecutive seconds. Seven pictures have been cut out between each of these. In the upper row of six views you will note that the lower outline remains practically constant, while successive thrusts are made with the wall of the ectosarc first to the left and then upward towards the two erythrocytes. In the second row the upper border shows practically constant, while the thrusts are downward, first toward the right and then toward the left. In the third row the upper border has changed but little, but the thrust is farther towards the left and in the fourth row, while the lower border remains about constant, the motion has been exerted again successively more and more in an upward direction. During this time, the endosarc, including the granular mass within, has changed relatively little as shown by the location of its nuclei and ingested material. The red blood corpuscles shown in the three upper rows give a good conception of the relative size of the endameba. With this species the pseudopod is seldom more pointed than shown at A in Fig. 1.
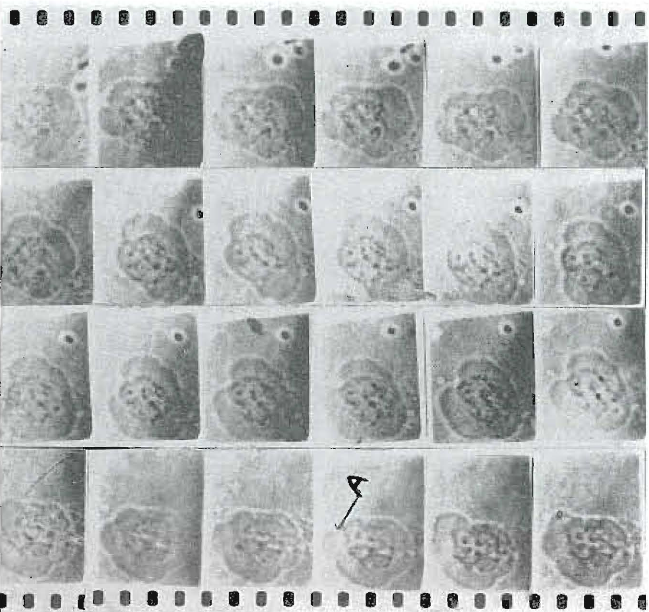
Fig. 1. Endameba buccalis. Unstained living organism, showing its motility and progressive changes of pseudopods as recorded at half second periods for twelve seconds. (See text.)
It is suggested by many that the endamebae have a definite phagocytic action and take up bacteria. It is difficult to state what all the ingested matter consists of and also difficult to differentiate it from certain structural parts such as nuclei, which are at times even as large as a leukocyte. Fig. 2 illustrates the appearance of this material especially well. Letter B indicates the stiff short blunt pseudopod with its limiting membrane, and letter A, its glassy hyaline ectoplasm. They have a slightly yellowish tint, giving a color between that of a leukocyte and a red blood cell. Frequently in extra good specimens the ectosarc with its contained protoplasm seems to be relatively large in proportion to its contained granular endosarc and gives the appearance that the latter is floating within it. In these specimens there are usually several very large blunt pseudopods present at once, tho note, as previously stated, only one is motile at a time. These characteristics are shown especially well in Fig. 3.
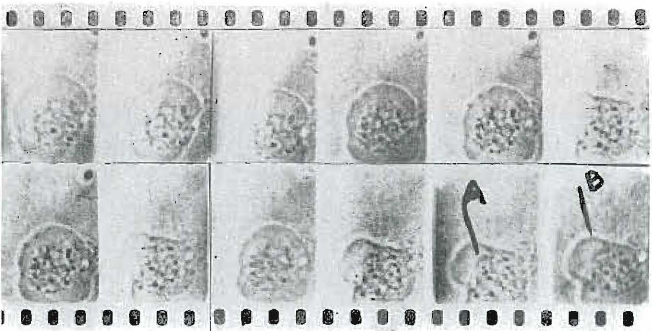
Fig. 2. Endameba buccalis. Illustrating nuclei, ingested matter and bacteria, also at A and B the ectoplasm and ectosare. Half second intervals.
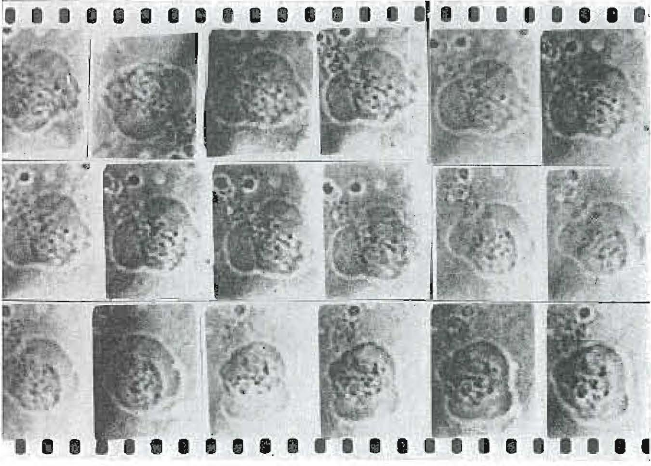
Fig. 3. Endameba buccalis. Showing differentiation of endosare and successive, but single projectious of pseudopods. Half second intervals.
It frequently occurs that it is exceedingly difficult to differentiate external foreign matter from the structural parts of the endamebae. because of their being superimposed. This is particularly well illustrated in Fig. 4 where, by knowing that this species, endameba buccalis, does not extend long pseudopods, as this view would seem to indicate we would recognize that the apparent pseudopod is an erythrocyte and some adjoining foreign material. The apparent effect of this is that of a slowly extending pseudopod.
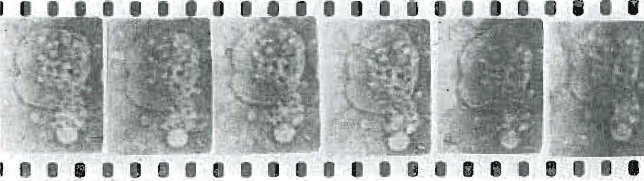
Fig. 4. Endameba buccalis. Showing relative size to a red blood cell, also a superimposition with foreign material giving the false appearance of a pseudopod. Half second intervals.
The other common species is known as endameba Kartulisi, discovered by Kartulis (8) in Egypt, the morphology of which is distinctly different from the preceding when seen in its natural state, but which, according to the manner of its dying, may take on forms quite unnatural to it in life and which more closely resemble the endameba buccalis. Its form may vary from a narrow worm-like structure to nearly or actually round, according to the conditions. When motile it projects a pseudopod in the direction it desires to move and gradually extends this until its ectosarc is in the form of a long loop with its refract tile protoplasm practically all in advance of the granular mass.
Figure 5 shows an endameba of this species, starting out on a journey, as seen in the first picture in the upper left. You will note that the condition just spoken of clearly obtains. In the second picture, one-half second later, we see the granular mass flowing within the pseudopod. Unlike the species buccalis, just described, this variety continues its projection almost entirely in one direction, which gives us the effect of a repeatedly extended single pseudopod. It will be noted that at the time the granular mass is moving within the ectosarc, there is no motion of the latter and when, as shown in pictures 3 and 4, the pseudopod is moving forward again there is practically no motion of the endosarc and its granular contents. In this variety it is very much more difficult to differentiate the endosare from the ectosarc, partly because of the migratory nature and habit of the organism. Pictures 4 and 5 illustrate how the least advanced end of the organism has scarcely started to move or change its content until the mass of the organisms has been moved forward; in other words, it has remained as an anchor to push the other forward. After the organism gets under way, as shown in the second row, particularly in the last two pictures, representing a total of six seconds, it has elongated until it has become a narrow worm-like structure and has practically doubled in length. It should be noted that the organism covers nearly twice the square surface in the last of this series as in the first. This may be due, in a large part, to a thinning of its depth in the plane of the field, but careful observation has often suggested that the organism actually takes in fluid, thereby distending its ectosarc, or outer limiting membrane, to enable its less plastic endosarc to be more easily moved within it. This species usually has two nuclei, varying in size, besides varying quantities of granular material, which may be bacteria and ingested material, according to the circumstances. It is not definitely known how endameba reproduce, but it is generally supposed that it is by transverse division and by some it is contended that they do so by means of division between the double nuclei. (9) It is significant to note from these illustrations, as shown particularly in figure 6, the clearly defined double nuclei, which clearly differentiates this species from the histolytica found in the colon, which multiplies by fragmentation of the chromatin, the remnant of the nuclei itself being expelled from the cyst. Figure 6 also shows very beautifully, and which often cannot be seen in stained specimens, that the double nuclei are not contained in a constricted limiting sheath. In the first picture they are seen close together and in the second one, one-half second later, one nucleus has moved forward to a new position, leaving the other in its original location. By one and one-half seconds later, as shown in the 5th picture, the second nucleus has moved up to the location of the first and the rapidity of this motion is clearly indicated by the fact that in the 4th picture they are at about their maximum distance apart and the 5th, one-half second later, they are close together.
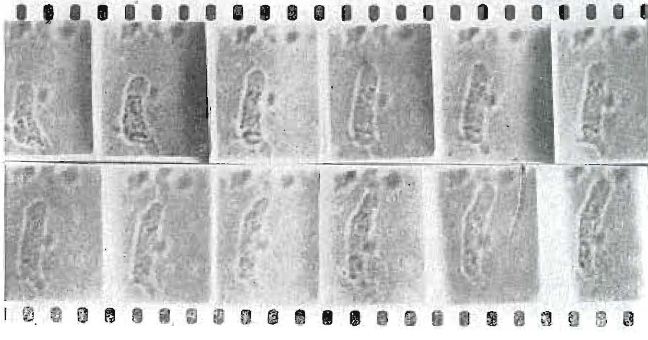
Fig. 5. Endameba Kartulisi. Showing organism starting on a journey and its progress in six seconds. Half second intervals
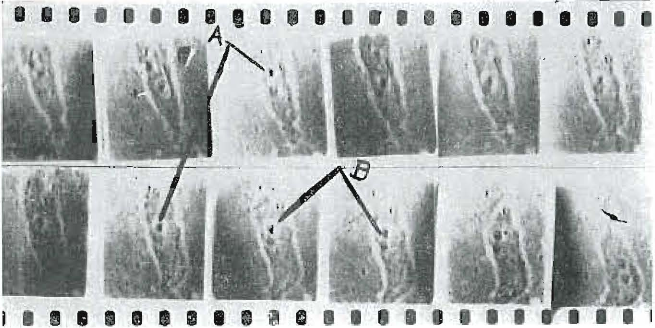
Fig. 6. Endameba Kartulisi. Showing nuclei and surrounding nourishing vacuoles A and B. See text. Half second intervals.
This motion is very spectacular when seen in the motion pictures, for in each of these series the intervening steps, covered by seven pictures, have been left out. Figure 6 also illustrates the cumbersomeness of the organism, as shown by the difficulty it has in changing its course. In the last picture of the upper row it has decided to change its direction and it moves the mass of its body much as a company of soldiers would be marched around a corner, seldom cutting the corners. The halo surrounding these nuclei, shown with particular clearness in letters A and B, are supposed, by some, to be nourishing vacuoles for the nuclei. We have never seen any contractile vacuoles in any species. It is very significant that, in the fixed slides that have come to us from various parts of the country, to be spoken of later, we have seen very few, if any, illustrations of these progressive phenomena, as there seems to be a relaxing of the organism to quite a universal state with death. It is a very frequent experience that when this type of organism is first observed on the slide that it is club shaped in form, especially so if seen very quickly after mounting, which suggests that this is a normal poise and one it takes in its natural nourishing process in its habitat. When warmed on the artificial stage it frequently occurs that the organism becomes quite rapidly motile and will quite rapidly migrate across the field. This is particularly well illustrated in figure 7, in the first of which it has that characteristic club shape appearance and in six seconds has gotten under way and has migrated a considerable distance, as measured by the dimension of Its own body. In other words, with a combination of lenses giving about 600 magnifications, the organism will cross the field in about three minutes. This figure also shows the migratory movement of the nuclei, spoken of in connection with the previous figure. Figure 8 shows an exceptionally rapid motility, in which in six seconds the organism has moved, virtually, half its own length. This is an unusual motility for this organism. We are all familiar with the fact that the root of a tree, as of a willow, can pass thru an exceedingly fine and torturous opening in a clay tile and expand on the other side to ultimately block the sewer, forming a veritable network. This property of making its cross section exceedingly narrow and of projecting and dragging itself thru exceedingly fine and torturous openings within the mass of a material, is particularly characteristic of this species, for we have seen it come to an apparently impenetrable blockade and force a hairlike figure into the mass slowly, but forcibly projecting the figure until it has extended a long distance into it, and finally by enlarging the end of the finger and using it as an anchor to slowly, but surely, drag its body into the meshes, and even tho it has been compelled to elongate itself in almost hairlike structure, it would finally emerge on the other side and assume its original form and proceed on its journey. This is a good illustration of how this organism may enter into and between the cells of living tissues and migrate to various parts of the body, as indicated by the case we speak of later, in which we have actually found it within the human tissue. It is exceedingly interesting that this species seems to dislike greatly to have death overtake it in the open and seems invariably to make for the debris, which may account for many people not finding it in their stained slides. It is also exceedingly interesting to note the great power of this little organism, for we have observed it as it would push itself into a mass of debris and crowd larger bulks of material out of its way. This is also particularly interesting as seen in the motion pictures. It has been quite significant to us that the presence of leptothrix in the patient’s mouth is very often an index of the probability of finding the endameba. The reason, however, is not known to us. The association of endameba with leptothrix has also been mentioned by Barrett. (10) It frequently happens that a stained specimen will reveal that the organism has but one nucleus when, in fact, there are two, but they are superimposed. This could not be demonstrated ordinarily but is clearly illustrated in figure 9, in which, in the first picture, we see clearly two distinct nuclei. In the second picture they are becoming superimposed and in the third, fourth and fifth they are superimposed, and had we only the latter we could easily be misled. This figure also shows clearly the apparent ability of the organism to take in fluid and enlarge its mass for its extending ectosarc, before the beginning of movement of the endosarc or diminution of its size, has presented an increase in volume that it is difficult to account for in any other way. This figure always shows clearly the rate of projection of the pseudopod, the total change here representing three seconds. It should be noted that the nuclei were generally much larger in the encysted or spore forms than in the motile varieties. The rate of motility of this species, the endameba Kartulisi, corresponds very closely to that of the common garden snail in proportion to its size.
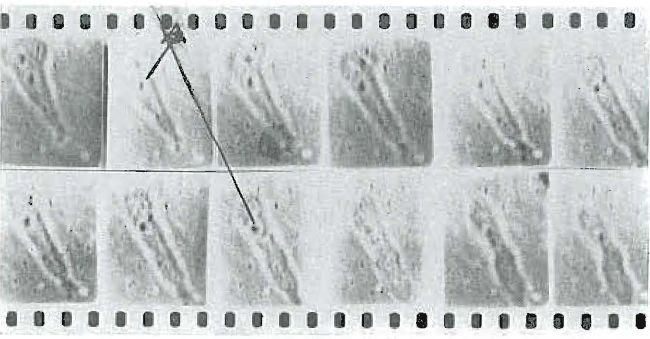
Fig 7. Endameba Kartulisi. Showing rate of migration. Total time six seconds. Half second intervals.
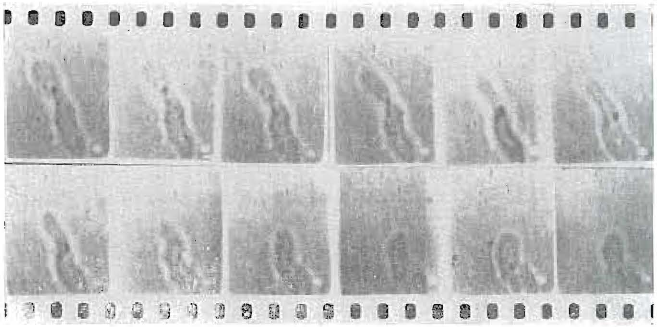
Fig. 8. – Endameba Kartulisi. Showing unusually rapid migration. Total time six seconds.
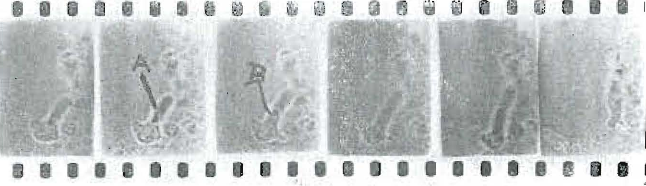
Fig. 9. – Endameba Kartulisi. Showing two nuclei becoming superimposed and plowing into pseudopod. Also apparent extension of ectosarc.
There are motile bacteria and protozoa of the mouth, mostly of the small varieties, that have a speed of locomotion, which, in proportion to their size, would compare with that of the hummingbird or the honey bee. We have found an organism in some mouths, the morphology and pathogenicity, of which we have not found in any of the literature, which has a size between that of the erythrocytes or red blood corpuscles and the endamebae and has a motility so great that it can only be kept on the microscopic field by using low powers, by the constant adjustment of the mechanical stage, and it is so transparent as to be scarcely visible with the higher powers. It has a speed of motion probably one hundred times as great as that of the most motile endamebae. Figure 10 shows motion pictures of it, taken at the rate of one per twentieth of a second, there being no pictures cut out as in the former illustrations. In the picture in the upper left hand corner the organism is marked as A and its position is indicated at each succeeding twentieth of a second, and in six-twentieths it has passed entirely off this part of the field. This is shown here under a low power, approximately 400 diameters. A relative conception of its motility, in proportion to its size, can be obtained by comparing it to the speed of a dog, or equivalent to that of a man running at the rate of 12 to 15 miles an hour. This organism has cilia and a contractile vacuole and is probably a paramecium. It is spoken of later in this paper in connection with a practical case. We have only found this organism in mouths with a prolific growth of motile mouth flora. It must be seen either in the microscopic field or in motion pictures to be appreciated.
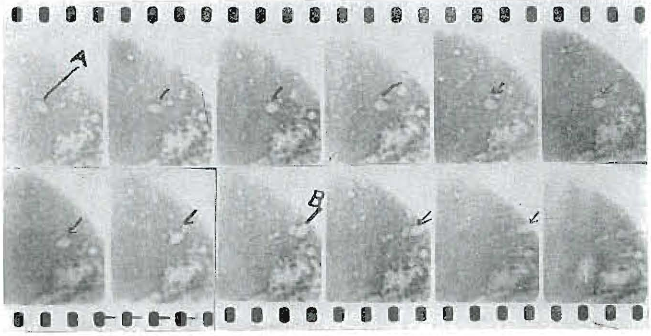
Fig. 10. A Ciliated Protozoan. Recently observed. Showing its extreme motility, which is probably 100 times that of the endameba. Intervals between views, one-twentieth of a second. Total time crossing this field, twelve twentieths of a second. It is usually larger than a leucocyte.
Some Important Conditions in the Endameba and Emetine Problems that Are Not As Yet Satisfied
Are endamebae directly related as a causative factor in so called pyorrhea alveolaris, and will emetine treatment cure the disease? There are many evidences to indicate that the answer should be affirmative, among them the following:
Favorable evidence:
- The statements made by skilled bacteriologists (11) of known exceptional ability and world reputation.
- The history of certain varieties of endameba and their known relation to other lesions, (12) as for example, endamebic dysentery (13) of warm climates and its cure with emetine treatment.
- Their frequent presence in pyorrhea alveolaris pockets. (7) At this point we wish to state that in order to enlarge the field of clinical observation we have been in correspondence with the Presidents of the various state societies of the United States and with prominent dental pathologists of the United States, Canada, Mexico, Cuba and Puerto Rico, and have had smears made and fixt on slides furnished by us, in these various localities and have stained them here under uniform conditions. We have also had the presidents of the various state societies select for us a half a dozen of the dental pathologists of their state to co-operate with us in making observations. Correspondence with these two groups of men and the study of their slides indicate that, in the type of cases that have been selected by them for the smears, the presence of the endameba is almost universal at the time of and the conditions under which the observations were made. There are, apparently, few exceptions, which will be taken up later under the evidence against the endamebic etiology of pyorrhea.
- Many observers in various parts of the country report that the use of emetine, as an amebicide, has either greatly improved or, according to their standards, has cured the pyorrhea alveolaris. (14) As an illustration of some of the correspondence, I quote from three of the letters. (a) “I have been using this treatment (emetine) now for two weeks or more, having treated about sixteen cases, and have gotten excellent results. Among this number I have absolutely cured five cases. The balance are still under treatment.” (b) “I have been using the emetine since September last and would say that with one exception I have had the best results. I have used it by the stomach, subcutaneously, and by flooding the pockets, and have had gratifying results in all but one case, but in many of them I have had to be very persistent when, no doubt, others would have given up hope, etc.” (c) “In regard to the results of the emetine treatment would say that with but one exception I have had very gratifying outcomes. Some cases, of course, yielded more than others and some are, apparently, entirely well. The case that refused to yield was one on which I have also used autogenous vaccine with negative results.” Several of the other correspondents state that the emetine treatment is frequently, or generally, successful in improving, either in part or very materially, the condition, tho very few refer to them as being cured.
- The authors of this report have found an endameba on the apex of a root that had been extracted where the pyorrhea pockets of the mouth did not show endameba, and while it is possible that the sterilization about the teeth was not perfect enough to prevent the contamination of the root end at the time of its withdrawal thru the tissue, the fact that sterilization was used and that the root apex was very conical and that the smear was taken from the very tip, strongly suggests that the organism was an inhabitant of the tissue about the apex.
- The authors have also found three very motile endamebae of the Kartulisi variety in the blood of an extirpated pulp, which operation was done under novocain. The pulp was exposed mechanically, accidentally, after the removal of a poorly fitting gold crown. The exposure was covered with calxine cement for one week. We believe there was no possibility of the organism entering the tooth thru the artificial opening made into the pulp chamber unless it passed thru the cement. This patient is suffering from an obscure irritation of an old heart lesion. This is a very significant finding and, so far as we know, the first time an endameba has been found in the tissues of the mouth, and suggests pathogenic nature of the Kartulisi variety.
- It is possible that there is some metabolic that is produced by the endameba, which exerts an enzymic action.
Evidences against the endamebic etiology of pyorrhea and the treatment of the disease with emetine:
1. The statements of skilled bacteriologists, mostly specializing in dental pathology, are that, while they find the endameba present, they do not consider it an important causative factor. (15).
2. The correspondence (16) with selected observers from different parts of the country shows the majority of them to be very conservative and reluctant to claim much benefit from the emetine treatment and some are strongly negative. I quote the following: (a) “My clinical experiments show that the treatment by emetine is not what it is ‘cracked up’ to be. I have tried it in every way possible in all kinds of cases and my experience is the same as in autogenous vaccination, that is that it does no good unless thoro instrumentation has first been accomplished and then it is not necessary. Proper surgical work is what does the work and is a great deal better than the emetine treatment, etc.” (b) “You ask for general observations as to the endameba. I will say that in the mouths I have found them I do not find them after I have carried out my thoro pyorrhea and prophylactic work, and this without the use of any drugs, whatever. I have used the emetine religiously and have found no results from its use in addition to results I obtained without it.” We would also refer you to another paper published in this department of the Journal, which directly discusses this question. In the correspondence received 11% have been positively against the use of emetine, 47% conservative and noncommittal, in other words still earnestly studying its effects, and 42% are favorable to its use, generally in conjunction with thoro instrumentation.
3. A few observers, including ourselves, have not found the ameba present in certain cases before treatment with emetine and have found it in those same cases shortly after treatment. This we will discuss later.
4. Many observers, including ourselves, have found many cases of typical so-called pyorrhea alveolaris lesions which, during the period in which the observations were made, did not, at any time, show endameba. If they were present they could not be found. In one very typical case, in a mouth where several of the teeth had been lost by this disease and where another was badly affected and loose, also to be sacrificed, exhaustive studies were made to locate at least one endameba or spore. Numerous slides were made on each of seven days during November, five days during December and four days during January, in all at least one hundred slides, both by examining directly and by staining, and in no case could the organism be found. The badly infected tooth was then extracted. Emetine treatment was used in the mouth wash during February and March and on April 1st the patient was again examined and, altho her mouth was in excellent condition, endamebae were found in the first slide and in other slides made from different parts of her mouth. Another patient was examined for endameba about the pyorrhetic teeth, some of which could be nearly removed with the fingers, several times during each November, December, January and February, and they were not found. In March the organisms were found even after the several badly affected teeth had been extracted, and the mouth put in good condition. These cases are typical of a number that were examined during both the Winter and Spring months, and which did not reveal the endameba during the Winter except at certain brief periods, if at all, until the spring days. This strongly suggested the relation of temperature or water supply to the varying presence of the organism. It is significant that a large proportion of the cases of true pyorrhea alveolaris do not have even a visible amount of pus present, which is one of the reasons that our profession has been striving, so diligently for decades, to find a name that was adaptable to the disease in its various stages and conditions. I am advised that about twenty different names have been presented as being adequate to correctly identify this lesion. It has been the experience of the authors that during the months of November, December and January, particularly the latter two, the cases showing endameba were, almost universally, those with a liberal amount of pus present, while those of February, March and April, particularly the latter periods, showed the organism in a great majority of cases, whether an abundance of pus was present or not. We have examined approximately fifteen hundred slides of our own, besides approximately one hundred and fifty furnished by the presidents of the various state societies of the Union and by dental pathologists in various cities, and have carefully tabulated the data. Unfortunately, no slides have been furnished us that were made earlier than the latter part of February, most of them during March and, consequently, they do not check against our data going back into previous months. For another reason they are not comparable, namely, that they presumedly have been almost all made from those cases of pyorrhea that had a liberal amount of pus flowing; in fact, the case reports, kindly provided with the slides, stated this fact in nearly all instances. We have made into a chart form (See figure 11) some of the data revealed by this large series of records and related them to the average temperatures for January, February, March and to April 7th. The heavy, straight, horizontal base line represents zero temperature, with the dates recorded below it, and the elevation represents temperature, Fahrenheit, shown by the zigzag curve. It is exceedingly interesting to note that the points marked A, B, C, D, F, and the ascending line thru J represents the increasing frequency of the endameba in pyorrhetic people, and from No. 1 to and thru J, where the time is marked continuously on the ascension, a large number of people who have no pyorrhetic lesions have the endameba present. In several cases children with splendid healthy mouths are showing them. The points A and B in January and C, D and F in February are particularly instructive, for at these times there was a sudden sharp increase in the presence of endamebic infections, and it will be noted that these correspond to periods immediately following, by a few days, a rise of temperature. At these periods there was a decrease in the number of spores with an increase in the number of motile endameba, suggesting a period of incubation following the rise of temperature. Circumstances prevented us from making observations at the dates corresponding to E, which is the only break in the record. It is also significant that cultures we had planted to receive and grow air ameba during the winter did not show them until the ameba line was well in ascent about the first of March, tho the condition have remained constant even as to the temperature of the inside room the culture medias were exposed to the air. It was particularly interesting to note, in this connection, that when we wrote to one of our friends, a skilled observer of mouth conditions, requesting that he observe whether or not in his locality there was the same relation of endameba to temperature changes that he replied, “I was amused at your enquiry regarding the greater prevalence of endameba in our cases of pyorrhea since the change in weather, because of the fact that for the past three weeks practically every case of pyorrhea that we had, seems to show more or less abundance of endameba. I had not attributed it to the weather so much as I had to the fortuity of the cases which where we happened to see, etc.” It was known to the writer that this observer had not found them so prevalent in the mid-winter months as in the Fall. We will be very glad to know the experience of other observers who have been looking for the endameba during the Fall, Winter and Spring and, if possible, to have the accompanying data of the relation of these conditions to the average temperatures preceding. It is not clear what the causative factor is since the temperature of the mouth must remain about constant, irrespective of the climatic conditions, nor is it clear where the organisms are sojourning in the interims when they seem to be absent from these particular cases. The correspondence with the large number of observers indicates that they probably are not related to the water supply, altho at one time in January all of the cases of the authors in which they were found to be present were using water from springs outside the city. It should be stated, in this connection, that the only slides we have received from the various observers in the different parts of the country, who prepared them for us according to our directions, which did not show endameba were made in the northern part of the country the latter part of February. An important fact obtained with regard to the presence or non-presence of the endamebic infections in the cases, herewith cited, in relation to temperature changes, namely, that there was no apparent difference in the nature or systemic effect, by any means that we could determine, when the organisms were abundantly present or were not present in the same mouth, tho the variation ranged from zero to a prolific number.
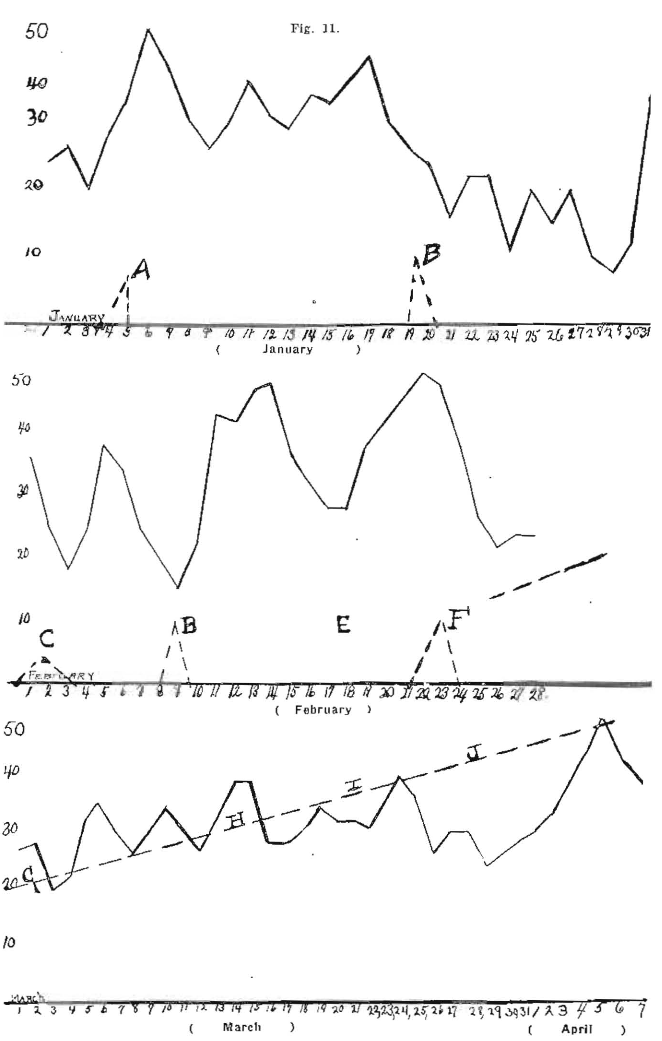
Fig. 11. Curves showing relation of varying presence of endameba to mean atmospheric temperature. (See text.)
5. Another argument against the endamebic origin of this infection is the relation of systemic disturbances to the presence of the organisms. During these months we have studied cases of the most profound systemic expression, and in which the general symptoms responded to treatment or pyorrhea, but in which cases no endamebae were found before and during the period of treatment, while the patient was suffering systematically, and yet after a thoro treatment and after subsidence of the symptoms, the endameba appeared without any return of the symptoms. These were chiefly nonsuppurative cases of pyorrhea and in all probability would have been overlooked by all except very observing dental pathologists. The mouth lesions were relatively very insignificant.
6. The effect of emetine on other microorganisms. Emetine Hydrochlorid has a profound action on other microorganisms, including the various varieties found in the mouth, which effect is almost as striking in many instances as its action on the endamebae; and granting, as there is abundance of evidence, that, in many cases, the emetine has positive beneficial effects, both on the local and the systemic conditions, whether injected intravenously, subcutaneously, or in the pyorrhea pockets, it is not established that its beneficial effects are, in a part or whole, not due to its action on these other organisms rather than the endameba. It is particularly to be regretted that this point has been almost entirely overlooked in the writing of the literature that has been published relative to the endamebic infections. There are exceptions, however, namely the discussion of Curet of New Orleans, (17) in which he says “that 1-10 per cent solution of emetine hinders perceptibly, in thirty minutes, the growth of a 24 hour culture of diphtheria and streptococcus mucosus. In one hour’s time it lessens considerably the growth of streptococcus pyogenes, and in 12 hour’s time that of staphylococcus citreus. It kills B. diphtheriae and streptococcus mucous in one hour and staphylococcus citreus in 12 hours’ time.” Wherry, (18) of Cincinnati Hospital, who has found that emetine one to 50 thousand killed ameba and one to 100 thousand paramaecium and balantidium. De-emethized ipecac failed to kill one to 5 thousand. Veder, who found when two per cent of liquid extract of ipecac was mixt with agar, it exerted marked inhibitive and germicidal action on B. typhosus, B. paratyphosus, B dysenteriae, and staphylococcus pyogenes…This is important when one considers the like role played by symbiotic bacteria in amebic lesions. The researches of the authors on this point to determine the germicidal and inhibitive action of ipecac and its products, emetine and cephaline, have demonstrated that the organisms taken from pyorrhea pockets are very directly influenced by these drugs, particularly the emetine. Ipecac, from which these two alkaloids have been extracted, has very little, if any, germicidal action. Emetine in solutions up to one to 10 thousand inhibits the growth of these organisms, besides having marked germicidal action upon them. Cephaline has also marked germicidal and amebicidal properties, but not to the extent that emetine has. An interesting experiment that any one can make very easily is to expose various culture media to the air contamination. So small an amount of emetine as a loop full to 5 C. C. of media will have the effect of preventing the growth of these organisms for 24 hours, at which time the controls will have a profuse growth.
There is much clinical evidence to indicate that the beneficial influence of emetine is due to its effect on other micro-organisms than the endameba. We cite one of several cases in detail. A man of good habits and good history, about forty years of age, had suffered for months with recurring extreme headaches lasting from two to three days and so severe as to put him to bed. His vision was disturbed with what he called liver spots. These attacks recurred at varying intervals at from two to three weeks and were getting slowly, but progressively, worse. All conceivable means had been resorted to in good medical practise, without more than temporary relief. Accompanying these attacks there was considerable distress in the liver and a digestive disturbance. Frequent examinations of his mouth during November, December, January and February for endameba were negative, altho a great many sides were made. Careful examination of the gingival tissues showed a couple of small pyorrhea pockets and the lingual root of the upper right first molar was almost entirely denuded of its attachment. We could not, at that time, get the slightest showing of pus. The cultures from the pockets showed a prolific growth of an organism which, for the present we will call X. Since the attachment of the other two roots of this tooth were excellent, the lingual root was amputated close to the crown, but before doing so animals were inoculated with the cultures aspirated from this pocket. We were able to recover the organism in question daily for several days from the blood of the tail of a rat inoculated. Within a month the rat died with multiple miliary abscesses of the liver, both macroscopic and microscopic. These abscesses produced a pure culture of the organism, which only lived 24 hours in artificial media. This organism would not grow at any time in artificial media. Other animals inoculated with the same culture, directly from this rat, died with similar lesions. Immediately following the amputation of this root the patient had an attack of his recurrent headache and digestive disturbance, which, however, was slightly different from former attacks, particularly in the rapidity and extent of his recovery. A thoro instrumentation was done on all his teeth. About three weeks later, January 8th, after he had had a recurring attack of his original disturbing symptoms, we started the emetine treatment, which consisted of injecting a small quantity of emetine into the pockets and into the tissue surrounding the socket where we had amputated the root. On January 13th we made the following record in our notes. “Since last appearance (January 8) patient has had recurrence of old symptoms without liver spots in eyes. Extreme pain like neuralgia started in the temple and extended successively thru the area supplied by the trifacial until it involved all its branches. The pain was so severe that a physician was called and gave him sedatives. The attack started mildly on Friday evening, the day of our injection with emetine, and became gradually worse, reaching the climax on Monday morning, January 11th. His recovery was very rapid, so much so as to greatly impress him and when seen on this Wednesday, the 13th, he is feeling unusually well.” This clinical picture and reaction was repeated with diminishing intensity after each treatment, with emetine, whether by flushing the pockets or by subcutaneous injection into the arm, and with such regularity that the patient dreaded the treatments because of their after effects. On February 9th the treatment was made into the pockets with flavored normal salt solution, unknown to the patient, and he waited in dread for the oncoming reaction, which, he cheerfully reported by phone on the following morning, had not materialized. The bacterial growth in the pockets was greatly modified by emetine treatments. Suddenly the patient ceased to have any reaction after the emetine injection, since which time he has been receiving one injection each week or two. Since the emetine ceased to cause reaction, he has not had a single recurrence of his digestive or neuralgia and headache troubles. He washes the pockets daily with a syringe, using 1-10 per cent solution of emetine. He has gained in weight and is feeling better than any time for a year. Let me recall that during November, December, January and February, diligent search did not reveal either the endameba or spores. In four days during March, and one already in April, he has been examined for the presence of endameba, and on every occasion but one, both spores and actively motile endameba have been found. The organism we have referred to as X has almost disappeared from these pockets. If space permitted we would present two other case histories, which are quite as striking as the above in illustration of the fact that emetine does have an effect in certain cases and, apparently, there has not been found endameba. One of these patients is now attending business eight hours daily, and had not previously more than a couple of hours a day, if at all, for six months and tho in the prime of life was completely discouraged. It should be stated in this connection that our experience in injecting emetine subcutaneously into healthy people is that it produces no reaction except a local soreness in the doses used in the above cases.
7. The special work of Noguchi (22) on the spirochaeta, treponema mucosum strongly suggests its relation to the pathogenic processes involved in pyorrhea alveolaris.
8. The progressive pathology of the lesion, known as pyorrhea alveolaris, as it is understood by our most competent students, is one of the strongest arguments against the proposition that the lesion has, as its chief etiological factor, an endamebic infection or that the disease can be cured by injections of emetine. It is an exceedingly significant circumstance that the dental pathologists, who have been spending decades, or the most of a lifetime, in the study of the pathology and etiology of this lesion, are practically unanimous in the belief that the disease will not be cured by the injection of any medicament, nor do they consider the fact of stopping the flow of pus as being in any sense a cure for the disease, since many procedures have been known to be competent to accomplish that change in the expression of the disease, but always with the tendency to recurrence but never with the complete obliteration of the lesion itself. The very form of nature’s method of attachment to the root wall is dependent upon a vital cementoblast with its normal vital attachment to the cementum. When these cementoblasts have lost their life the possibility of a reattachment seems to be so remote, according to many of our best authorities, as to be considered practically an impossibility. The treatment that has given most uniform good results has had, as its basis. the surgical treatment of an infected wound and the stimulation of the circulation with protection from a reinfection. One of the authors of this paper has searched diligently for 20 years to find a single instance where a definitely developed pyorrhea pocket with destruction of the alveolar wall had actually produced a reattachment to the tooth wall, and in that time has seen but one case and in that case the onset of the disease was very acute and sudden. The necrotic bone was cut with a bur from the necrotic alveolus and, as nearly as possible a surgical condition observed, with the result that there seems to have been a perfect reattachment and in this case it is probable that the cementoblasts had not yet died but were still vital. We have seen other cases where the alveolus had grown so tightly around the root that it seemed to be ankylosed but we could not convince ourselves it was anything more than a close adaptation of the new bone to the tooth root.
An important phase of pyorrhea alveolaris lesions is the systemic involvement and it is a matter of extreme importance that exhaustive researches should he made to determine whether or not the systemic expressions, as illustrated in the case sighted above, are the direct effects of toxins produced by the organisms or the irritations of proteins of bacterial origin that have been set free either by medication of instrumentation. Also, whether the bacterial protein or toxin, if such are producing the lesions, are set free from the bacteria by the action of the endameba. In support of this latter we have the splendid work of Evans, Middleton and Smith. (19) They explain the local reaction following the emetine injection as an index of a point of saturation when, with the death of numerous endameba, the lethal point of emetine has been reached and a great amount of bacteria, and possibly amebic toxin, is liberated. Smith, Middleton and Barrett, (20) in their splendid work on amebic infections of tonsils and their systemic conditions, suggest that the bacterial phagocytic action of the ameba probably set free in the system various endotoxins depending upon the kinds of ingested bacteria. It probably is not generally known, to those of other lines of practise and study than the treatment of teeth, that many patients are so sensitive to the indirect effects of instrumentation of pyorrhetic pockets that but a few teeth can be treated at a time without profound reaction, resembling, in many cases, a protein poisoning. This is illustrated by the following case. A young married woman, otherwise physically strong, suffered from extreme depression and lassitude with digestive disturbance and headache, and worthy efforts were made to relieve these with good medical procedure. The mouth showed non-suppurative, shallow pyorrhetic pockets with very slight local irritation and causing no personal discomfort. Recognizing the clinical picture, which is quite frequent, in the hands of all who are specializing in the treatment of this disease, we advised that only a small part of the instrumentation of removing the infecting and culturing masses and irritating deposits be undertaken at the first sitting. She was advised to watch for a reaction and report the next day by phone. The next day her symptoms were so extremely aggravated that she stayed in bed, and altho the phone was but a few feet from her she undertook to reach it and carry out her instructions to report, but she fell back wearily, stating, “Oh well, he knows I am sick, for he told me I would be, and what is the use of reporting.” This reaction recurred after each successive instrumentation, but with diminishing severity, and with no other treatment she is relieved of all her unfavorable symptoms and is, apparently, in perfect health again. Had emetine been used, it surely would have gotten the credit but nothing was done but the removal of the irritants and the culturing deposits about the teeth. Data of treatment and history of this type of case, of which there are many, should be carefully collected since they strongly indicate a bacterial protein poisoning. Beside the usual bacterial mouth organisms, consisting largely of spirochaeta, there was found in this mouth an organism similar to that shown in figure No. 10, which, as described, is probably 100 times more motile than the endamebae; in fact it is so motile that it is difficult to keep it on the field with powers high enough to study it well. It is not an endameba but is probably a ciliated protozeat, a paramaecium about the size of a leukocyte. We have only found this organism in a small per cent of the cases.
9. Another argument against the conclusion that endamebae are the causative factor in the production of the lesions we know as pyorrhea alveolaris is found in the following:
Emetine has a well established effect on some special lesions of the body that have not been suggested as being caused by endemic infection. The illustration of this is found in the fact that quite accidently it has been discovered by two different dentists that one of the most difficult of all known diseases of the skin to cure, namely, psoriasis, has been found to disappear, and the skin to return to an apparently quite normal condition as an incidental effect of the use of emetine in the treatment of pyorrhea. So far as we know, no work has been done as yet to determine whether or not patients suffering from this disease have endamebic infection of their mouths. This should be done. One of these cases is reported in detail by Wm. R. Chaplin, D.D.S., Savannah, Georgia, in the February number of the Dental Cosmos (Volume 57, No. 2, page 289). In his case the patient had suffered for fifteen years from psoriasis. He says, “The backs of both hands were completely covered with most repulsive looking inflamed, somewhat corrugated, scaly surfaces. This condition was also found in large patches on both arms and on some parts of the body. The disorder has been many times diagnosed psoriasis.” He treated the patient with emetine hydrochlorid according to the method as advocated by the Drs. Barrett and Smith, including instrumentation. After describing the case in detail, he states, “At the present time six treatments have been given–and it now being two weeks since last treatment every symptom of psoriasis has entirely disappeared.
Another report of a similar case has just come to us in a letter from Dr. J. W. Smoots, President South Dakota State Dental Society, Spearfish, South Dakota, in which he gives in parts the description of an experience he has had.
Referring to his patient, he says: “She had one finger of one hand particularly in bad shape from psoriasis, and as I had just received some P. D. & Co.’s Emetine Hydrochlorid and the physician had called me in, I advised the use of the above treatment. She has had four treatments in the last ten days and yesterday her hands seemed to be nearly normal but could not report her case cured until she has been under observation longer.”
This is of very great significance, not only because of the discovery of this new treatment for this painful and humiliating affliction, which has seemed to be practically incurable, but it suggests strongly a larger application for emetine than that of an amebicide, the inference of which can be that the beneficial effect, of emetine in the treatment of pyorrhea is due rather to its effect on other organisms than on endameba.
10. Another argument against the endamebic cause of pyorrhea is the important recent discovery that succinimide of mercury seems to have not only a specific action on the treponema pallidium, the specific organism of syphilis, but also quite as striking a curative effect on pyorrhea alveolaris as emetine. This has been discovered and emphasized by White and Wright. (20)
It has not been suggested that this drug is in any way specific for endameba, and it will seem very possible that its beneficial effect on pyorrhea could be explained on the assumption that the causative factor is a spirochaeta or some other vegetative organism. This conception is further supported by the fact that Noguchi has emphasized the possibility that pyorrhea alveolaris is caused by tbe spirochaeta, treponema mucosum, which has already been referred to in another part of this paper. (21)
The possibility of injury to the patient from hypodermic injection. We must recognize that there is a constant danger in breaking Nature’s seal of our own bodies and of causing the entrance into the body of infections. This includes not only the dangers from pathogenic bacteria but the sensitizing of the body to proteins and the distressing effects of later introductions of that same protein. whether carried in solution by the medicament or its effect on bacterial growth. An additional danger seems to have arisen by the causing of a more or less serious paralysis. We have just been informed of a case, where emetine was injected into the shoulder with the result of producing a partial paralysis of the arm lasting two days. We have not as yet received the full particulars. The authors have also seen a case of local necrosis of the alveolus from the injection of a few minims of a ½ of a 1% emetine hydrochlorid solution in the gums around a pyorrhea pocket.
Conclusions
Owing to the fact that the evidence is largely circumstantial, which has indicated that endamebae are the chief causative factor in pyorrhea alveolaris, based, in a great part, on the known bad reputation of its cousin’s species, the endameba histolytica of amebic dysentery, and since the evidence against this conclusion is in great part incomplete, we strongly urge the withholding of judgment until further researches shall have established sufficient of the following data.
- The successful production of the lesions of pyorrhea alveolaris by inoculation with endameba, according to Koch’s law, namely, (a) an organism, if it causes the disease, must be present in all cases, (b) the organism shall be isolated in pure culture, (c) a pure culture, if inoculated into a susceptible animal, must produce the disease, (d) the chemical products must produce the same alterations.
- Or, the successful production of the lesions by inoculation with some other organism, or organisms, or by some other means.
- Or, the demonstration that the endamebae of the mouth are non-pathogenic and are incidental or helpful inhabitants of the oral cavity as scavengers; not only harmless of themselves, but not producing either toxins or harmful enzymes.
- If the endameha buccalis is the chief causative factor in pyorrhea alveolaris why is the endameba Kartulisi found alone is so many of the typical cases?
- The establishment of the role of emetine, including a close differentiation between its amebicidal and its bactericidal actions.
- A determination as to whether the beneficial action of emetine is that of an amboceptor, acting upon the bacteria or protozoa with their protein and toxin contents (the toxiphor group) thru the agency of the complement, and also whether the action of emetine is that of a complement as in the case of lecithin with snake venom. (22)
- A determination as to what is involved in so-called bacteremia, which is clinically so common as a result of instrumentation and of certain medications and is this action bacteremic, septicemic or toxemic.
- The establishment of the precise local tissue changes involved in the development of the lesion of pyorrhea alveolaris and of the successive processes constituting its repair.
- The establishment of the precise role served by instrumentation in the process of repair of pyorrhetic lesions and the significance in this process of the removal of foreign material, bacterial plaques and degenerating tissue, also of polished surfaces, local stimulation of circulation by frequent massage, etc.
- The development of a means for the reattachment of vital tissue to dead and denuded cemental surfaces of roots.
- The establishment of the role of pyorrhea alveolaris pockets as culturing places for pathogenic organisms, as those of the streptococcus-pneumococcus group, which from this lesion as a primary focus, affect other organs and tissues of the body, and the establishment of the symbiotic effects of the organisms on each other.